
Three-Dimensional Voxel-Wise Quantitative Assessment of Imaging Features in Hepatocellular Carcinoma
 ,
,
Abstract
:1. Introduction
Contributions and Organization
- Piece-wise smooth nonlinear registration: an iterative reweighted local cross-correlation (IRLCC) method was used to overcome the deformation caused by various reasons, and it assumes that the entire deformation is piece-wise smooth.
- Three-dimensional calculation: imaging features were quantified voxel-wise, based on registered images.
- Consistency: all 3D information of the whole lesion was used for quantitative analysis and visualization.
2. Materials and Methods
2.1. Dataset
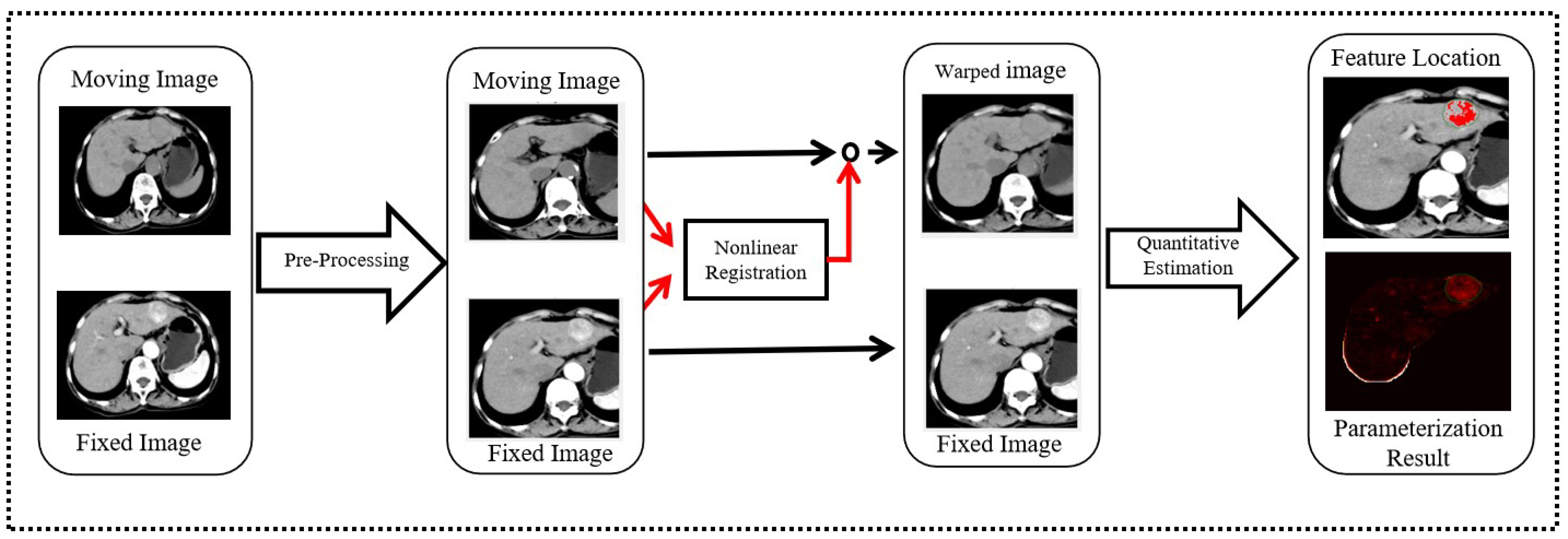
2.2. Image Registration Framework
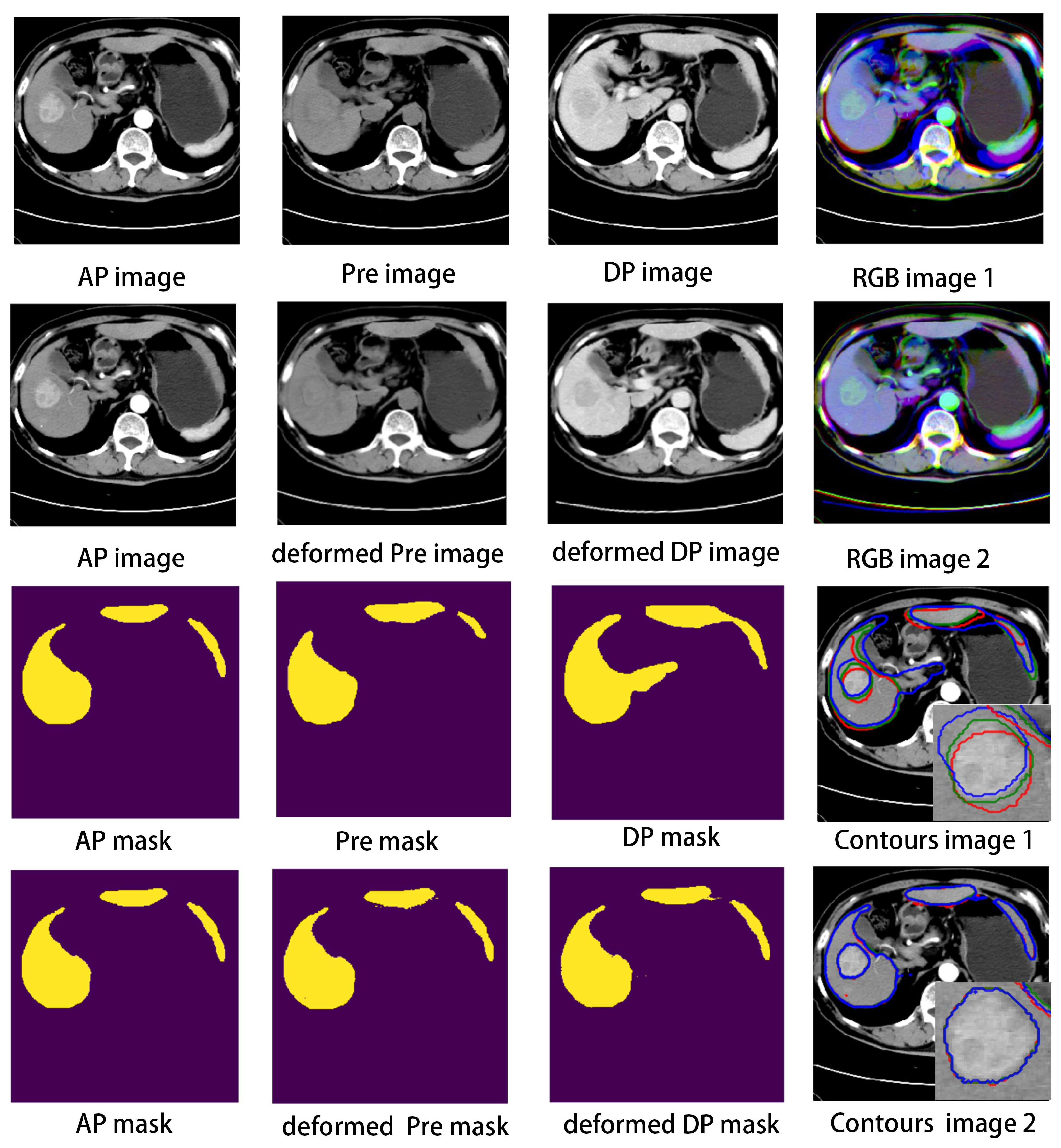
2.2.1. Image Preprocessing
2.2.2. Nonlinear Registration: The IRLCC Method
| Algorithm 1: Fixed-Point Iteration Algorithm |
Input: , l is the current level. Output: . Initialization: Upsample to the size in level l, then deform the moving image: ;  |
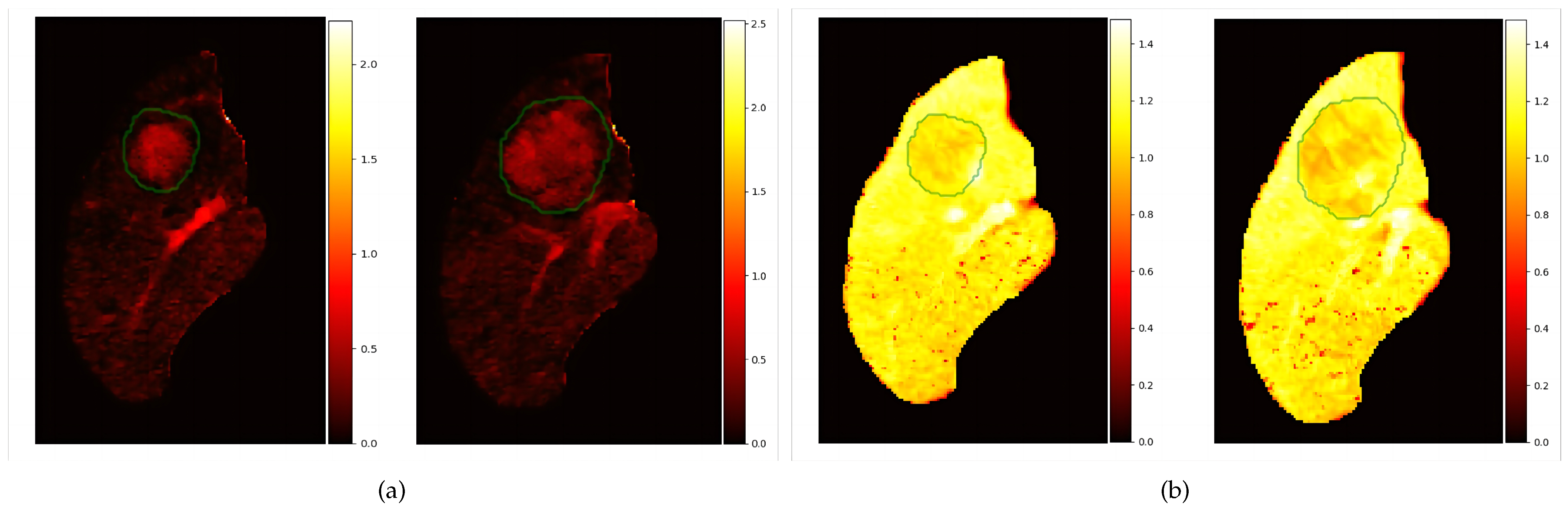
2.3. The 3D Voxel-Wise Quantitative Assessment of Imaging Features
2.3.1. Locations Extraction
2.3.2. Estimation
3. Results
3.1. Setting of Registration Parameters
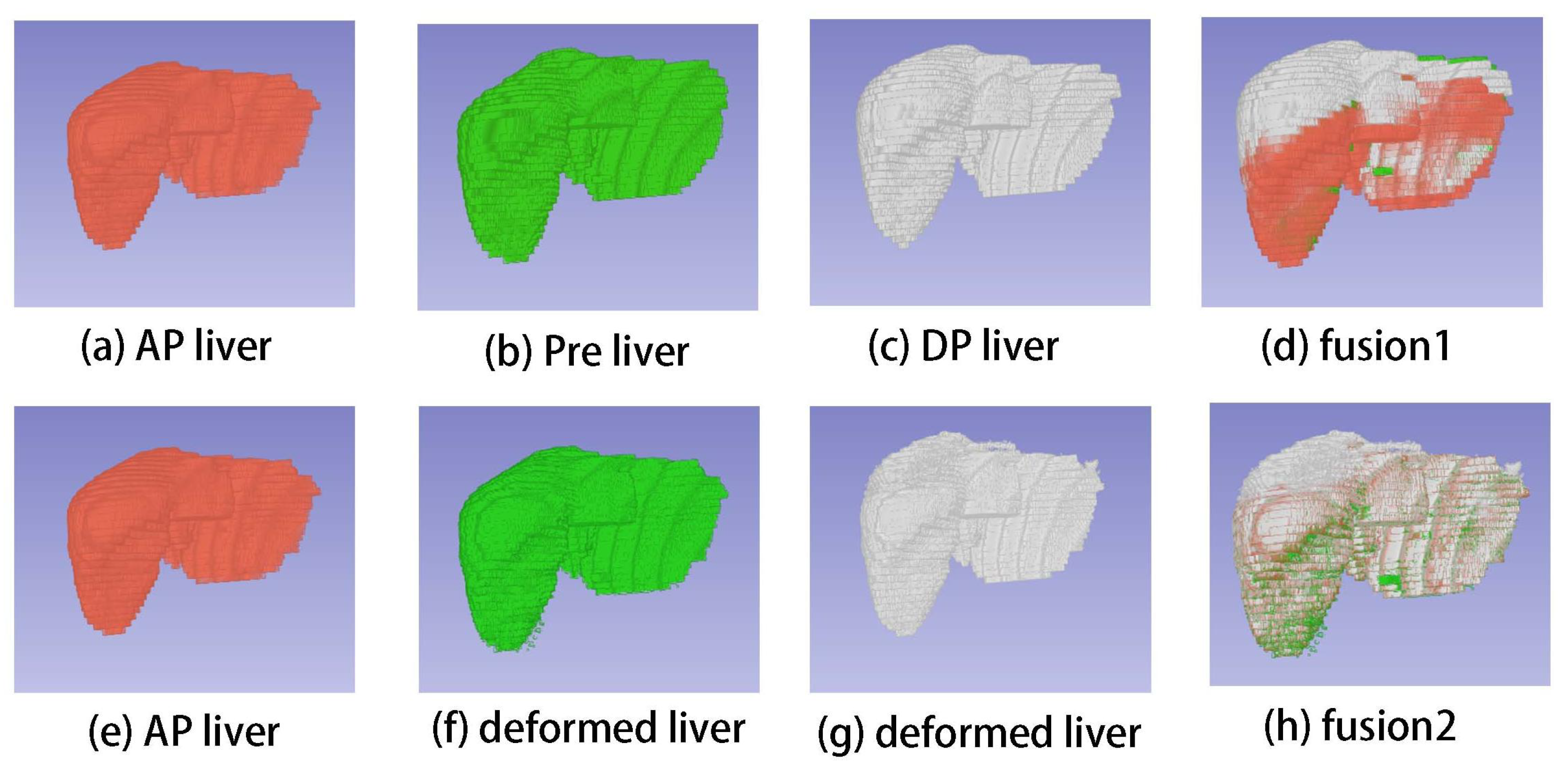
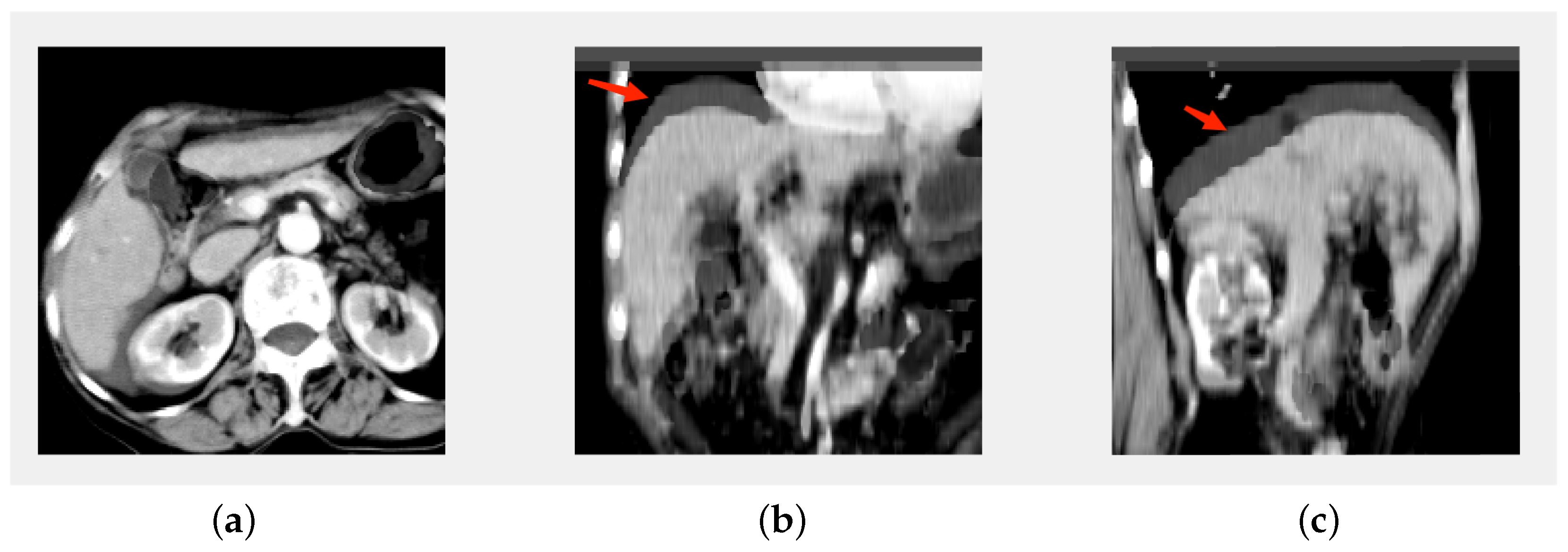
3.2. Registration Results
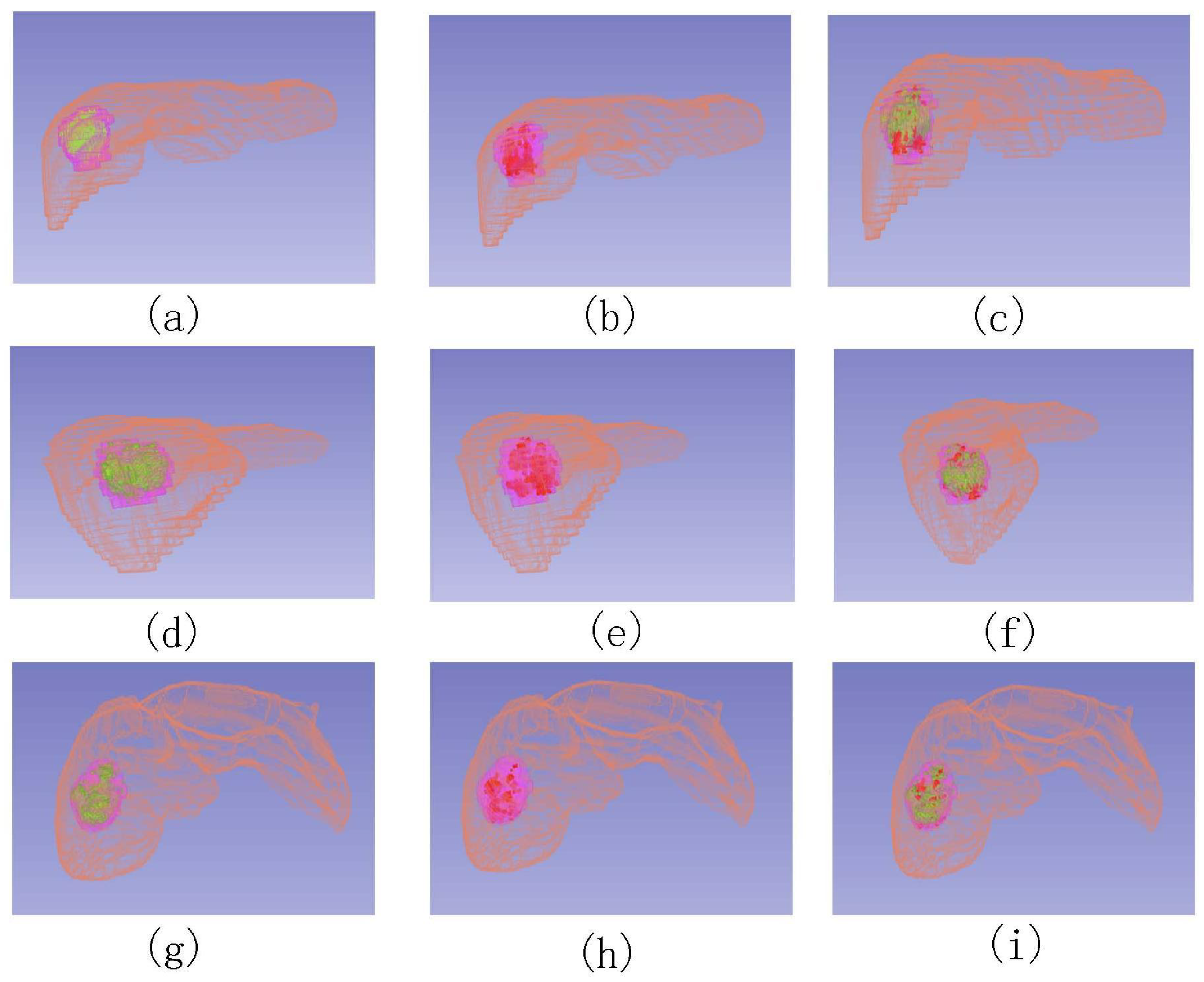
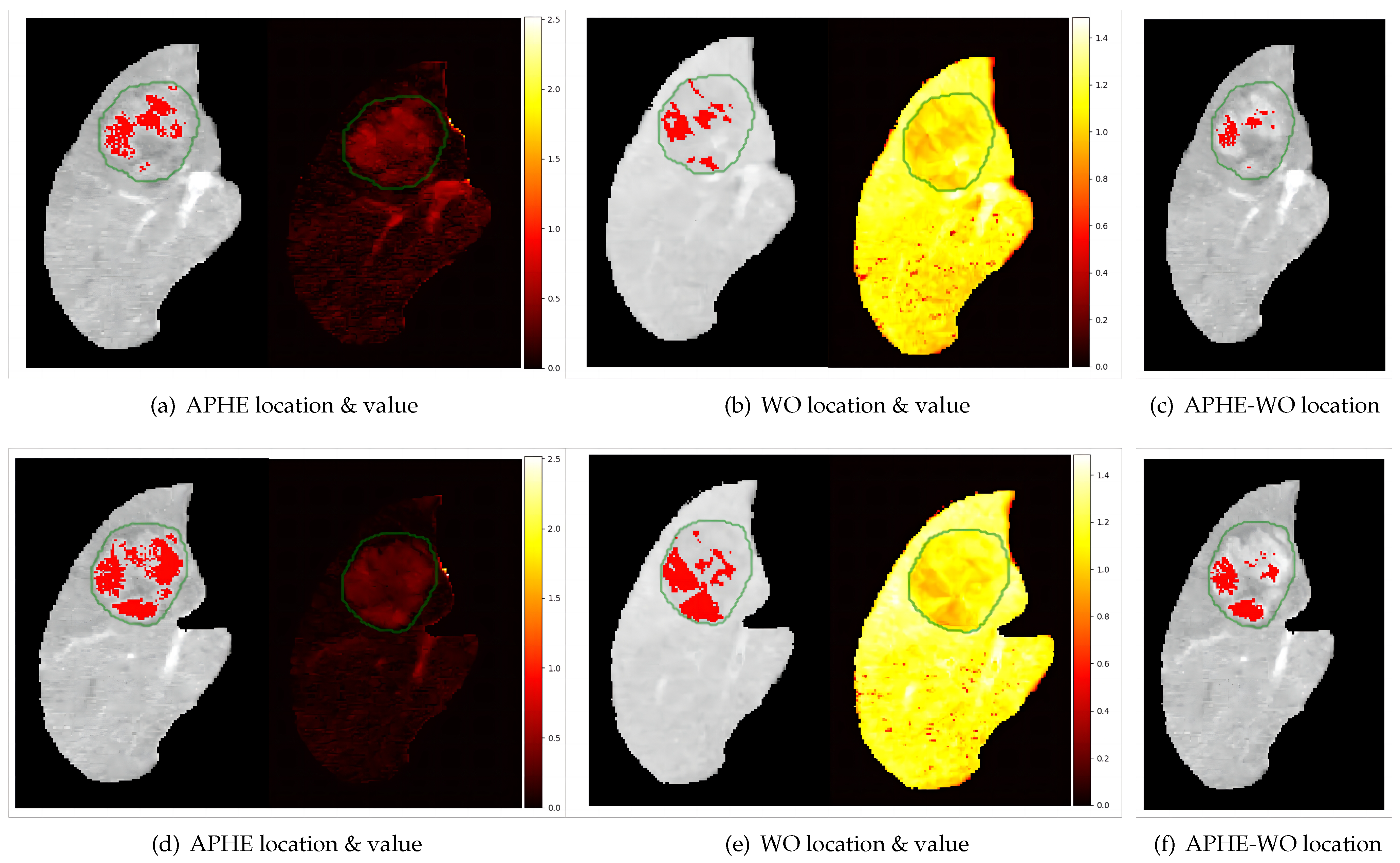
3.3. Voxel-Wise Quantitative Assessment Results and Visualization
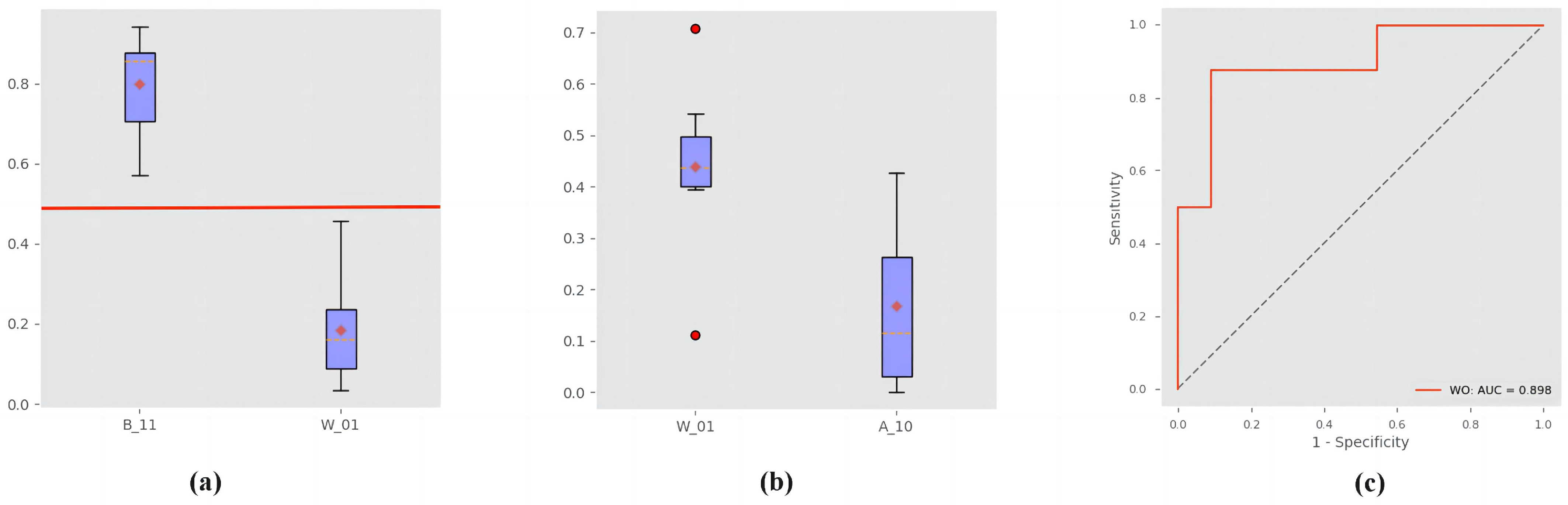
3.4. Quantitative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APHE | Arterial phase hyperenhancement |
| WO | Subsequent Washout |
| HCC | Hepatocellular carcinoma |
| AUC | Area under the curve |
| CT | Computed tomography |
| CM | Contrast media |
| MRI | Magnetic resonance imaging |
| Pre | Pre-contrast Phase |
| PAE | Percentage of arterial enhancement |
| AP | Arterial Phase |
| LI-RADS | Liver Imaging Reporting and Data System |
| PV | Portal Venous Phase |
| LLCR | Lesion-to-liver contrast ratio |
| DP | Delayed Phase |
| ROC | Receiver operating characteristics |
| ROIs | Regions of interests |
References
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennedige, T.; Venkatesh, S.K. Imaging of hepatocellular carcinoma: Diagnosis, staging and treatment monitoring. Cancer Imaging 2013, 12, 530–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bano, J.; Nicolau, S.A.E.A. Multiphase Liver Registration from Geodesic Distance Maps and Biomechanical Modelling. In Abdominal Imaging. Computation and Clinical Applications, Proceedings of the 6th International Workshop, ABDI 2014, Held in Conjunction with MICCAI, Cambridge, MA, USA, 14 September 2014; Springer: Berlin/Heidelberg, Germany, 2013; pp. 165–174. [Google Scholar]
- Hwang, G. Nodular hepatocellular cacinomas (Detection with arterial-, portal-, and delayed-phase images at spiral CT). Radiology 1997, 202, 383–388. [Google Scholar] [CrossRef]
- Kim, T.; Murakami, T.; Takahashi, S.; Tsuda, K.; Tomoda, K.; Narumi, Y.; Sakon, M.; Nakamura, H. Optimal phases of dynamic CT for detecting hepatocellular carcinoma: Evaluation of unenhanced and triple-phase images. Abdom. Imaging 1999, 24, 473–480. [Google Scholar] [CrossRef]
- Laghi, A.; Iannaccone, R.E.A. Hepatocellular carcinoma: Detection with triple-phase multi-detector row helical CT in patients with chronic hepatitis. Radiology 2003, 226, 543–549. [Google Scholar] [CrossRef]
- Kitao, A.; Zen, Y.; Matsui, O.; Gabata, T.; Nakanuma, Y. Hepatocarcinogenesis: Multistep changes of drainage vessels at CT during arterial portography and hepatic arteriography–radiologic-pathologic correlation. Radiology 2009, 252, 605–614. [Google Scholar] [CrossRef]
- Lee, Y.J.; Lee, J.M.; Lee, J.S.; Lee, H.Y.; Park, B.H.; Kim, Y.H.; Han, J.K.; Choi, B.I. Hepatocellular carcinoma: Diagnostic performance of multidetector CT and MR imaging-a systematic review and meta-analysis. Radiology 2015, 75, 97–109. [Google Scholar] [CrossRef] [Green Version]
- American College of Radiology. Liver Imaging Reporting and Data System. 2018. Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS (accessed on 2 February 2023).
- Chernyak, V.; Fowler, K.J.; Kamaya, A.; Kielar, A.Z.; Elsayes, K.M.; Bashir, M.R.; Kono, Y.; Do, R.K.; Mitchell, D.G.; Singal, A.M.; et al. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: Imaging of Hepatocellular Carcinoma in At-Risk Patients. Radiology 2018, 289, 816–830. [Google Scholar] [CrossRef]
- Elsayes, K.M.; Hooker, J.C.; Agrons, M.M.; Kielar, A.Z.; Tang, A.; Fowler, K.J.; Chernyak, V.; Bashir, M.R.; Kono, Y.; Do, R.K.; et al. 2017 Version of LI-RADS for CT and MR Imaging: An Update. Radiographics 2017, 37, 1994–2017. [Google Scholar] [CrossRef]
- Kyung Won Kim, M.; Jeong Min Lee, M.; Ernst Klotz, P.; Hee Sun Park, M.; Dong Ho Lee, M.; Ji Young Kim, M.; Soo Jin Kim, M.; Se Hyung Kim, M.; Jae Young Lee, M.; Joon Koo Han, M. Quantitative CT Color Mapping of the Arterial Enhancement Fraction of the Liver to Detect Hepatocellular Carcinoma. Radiology 2009, 250, 425–434. [Google Scholar]
- Liu, Y.I.; Shin, L.K.; Jeffrey, R.B.; Kamaya, A. Quantitatively defining washout in hepatocellular carcinoma. Am. J. Roentgenol. 2013, 200, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Grajo, J.R.; Fuentes-Orrego, J.M.; Abtahi, S.M.; Harisinghani, M.G.; Saini, S.; Hahn, P.F. Distinguishing hemangiomas from metastases on liver MRI performed with gadoxetate disodium: Value of the extended washout sign. Eur. J. Radiol. 2016, 85, 635–640. [Google Scholar] [CrossRef]
- Kloeckner, R.; dos Santos, D.P.; Kreitner, K.F.; Leicher-Duber, A.; Weinmann, A.; Mittler, J.; Duber, C. Quantitative assessment of washout in hepatocellular carcinoma using MRI. BMC Cancer 2016, 16, 758. [Google Scholar] [CrossRef] [Green Version]
- Stocker, D.; Becker, A.S.; Barth, B.K.; Skawran, S.; Kaniewska, M.; Fischer, M.A.; Donati, O.; Reiner, C.S. Does quantitative assessment of arterial phase hyperenhancement and washout improve LI-RADS v2018–based classification of liver lesions? Eur. Radiol. 2020, 30, 2922–2933. [Google Scholar] [CrossRef]
- Zhao, H.C.; Wu, R.L.; Liu, F.B.; Zhao, Y.J.; Wang, G.B.; Zhang, Z.G.; Huang, F.; Xie, K.; Geng, X.-P. A retrospective analysis of long term outcomes in patients undergoing hepatic resection for large (>5 cm) hepatocellular carcinoma. HPB 2016, 18, 943–949. [Google Scholar] [CrossRef] [Green Version]
- Jialin Peng, J.W.; Kong, D. A new convex variational model for liver segmentation. In Proceedings of the 21st International Conference on Pattern Recognition (ICPR2012), Tsukuba, Japan, 11–15 November 2012; pp. 3754–3757. [Google Scholar]
- Beare, R.; Lowekamp, B.; Yaniv, Z. Image Segmentation, Registration and Characterization in R with SimpleITK. J. Stat. Softw. 2018, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaniv, Z.; Lowekamp, B.C.; Johnson, H.J.; Beare, R. SimpleITK Image-Analysis Notebooks: A Collaborative Environment for Education and Reproducible Research. J. Digit. Imaging 2017, 31, 290–303. [Google Scholar] [CrossRef] [Green Version]
- Lowekamp, B.C.; Chen, D.T.; Ibanez, L.; Blezek, D. The Design of SimpleITK. Front. Neuroinform. 2013, 7, 45. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Qiu, C.; Peng, Z.; Yuan, J.; Kong, D. Iterative Reweighted Local Cross Correlation Method for Nonlinear Registration of Multiphase Liver CT Images. In Proceedings of the 2021 IEEE International Conference on Image Processing (ICIP), Anchorage, Alaska, 19–22 September 2021; pp. 136–140. [Google Scholar]
- Cachier, P.; Bardinet, E.; Dormont, D.; Pennec, X.; Ayache, N. Iconic Feature Based Nonrigid Registration: The PASHA Algorithm. Comput. Vis. Image Underst. 2003, 89, 272–298. [Google Scholar] [CrossRef]
- Cachier, P.; Pennec, X. 3D Non-Rigid Registration by Gradient Descent on a Gaussian-Windowed Similarity Measure using Convolutions. In Proceedings of the IEEE Workshop on Mathematical Methods in Biomedical Image Analysis, Burnaby, BC, Canada, 12–15 December 2011. [Google Scholar]
- Avants, B.B.; Epstein, C.L.; Grossman, M.; Gee, J.C. Symmetric diffeomorphic image registration with cross-correlation: Evaluating automated labeling of elderly and neurodegenerative brain. Med. Image Anal. 2008, 12, 26–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, M.J.; Anandan, P. The Robust Estimation of Multiple Motions: Parametric and Piecewise-Smooth Flow Fields. Comput. Vis. Image Underst. 1996, 63, 75–104. [Google Scholar] [CrossRef]
- Brox, T.; Bruhn, A.; Papenberg, N.; Weickert, J. High Accuracy Optical Flow Estimation Based on a Theory for Warping. In Proceedings of the Computer Vision-ECCV 2004: 8th European Conference on Computer Vision, Prague, Czech Republic, 11–14 May 2004; Volume 4, pp. 25–36. [Google Scholar]
- Ce, L. Beyond Pixels: Exploring New Representationsand Applications for Motion Analysis. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2009. [Google Scholar]
- Sun, Y.; Yuan, J.; Rajchl, M.; Qiu, W.; Romagnoli, C.; Fenster, A. Efficient convex optimization approach to 3D non-rigid MR-TRUS registration. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Nagoya, Japan, 22–26 September 2013. [Google Scholar]
- Qiu, W.; Yuan, J.; Fenster, A. 3D prostate MR-TRUS non-rigid registration using dual optimization with volume-preserving constraint. In Medical Imaging 2016: Image Processing; Styner, M.A., Angelini, E.D., Eds.; International Society for Optics and Photonics, SPIE: Bellingham, WA, USA, 2016; Volume 9784, pp. 458–463. [Google Scholar]
- Dice, L.R. Measures of the Amount of Ecologic Association Between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Heimann, T.; Van Ginneken, B.; Styner, M.A.; Arzhaeva, Y.; Aurich, V.; Bauer, C.; Beck, A.; Becker, C.; Beichel, R.; Bekes, G.; et al. Comparison and Evaluation of Methods for Liver Segmentation From CT Datasets. IEEE Trans. Med. Imaging 2009, 28, 1251–1265. [Google Scholar] [CrossRef]
- Huttenlocher, D.P.; Klanderman, G.A.; Rucklidge, W.J. Comparing Images Using the Hausdorff Distance. IEEE Trans. Pattern Anal. Mach. Intell. 1993, 15, 850–863. [Google Scholar] [CrossRef] [Green Version]
- Zhu, W. Segmentation and Registration of CT Multi-Phase Images for Abdominal Surgical Planning. Ph.D. Thesis, University of Strasbourg, Strasbourg, Germany, 2015. [Google Scholar]
- Hecht, E.M.; Israel, G.M.; Krinsky, G.A.; Hahn, W.Y.; Kim, D.C.; Belitskaya-Levy, I.; Lee, V.S. Renal masses: Quantitative analysis of enhancement with signal intensity measurements versus qualitative analysis of enhancement with image subtraction for diagnosing malignancy at MR imaging. Radiology 2004, 232, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Ho, V.B.; Allen, S.F.; Hood, M.N.; Choyke, P.L. Renal Masses: Quantitative Assessment of Enhancement with Dynamic MR Imaging. Radiology 2002, 224, 695–700. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Number of Patients | Ratio (%) | |
|---|---|---|---|
| Gender | Male | 29 | 83% |
| Female | 6 | 17% | |
| Age | ≥60 | 23 | 66% |
| <60 | 12 | 34% | |
| maximum diameter | ≥5 cm | 8 | 23% |
| 3∼5 cm | 21 | 60% | |
| <3 cm | 6 | 17% | |
| Thickness | 5 mm | ||
| Slice Resolution | 512 × 512 | ||
| Number of slice | 38∼53 slices | ||
| OutIter | InIter | SOR | Size of Coarsest Level Image | ||
|---|---|---|---|---|---|
| 0.001 | 0.001 | 5 | 1 | 20 | 32 |
| OutIter | InIter | SOR | Size of Coarsest Level Image | ||
|---|---|---|---|---|---|
| 0.00015 | 0.0001 | 3 | 1 | 20 | 32 |
| Region | Phase | Method | DSC (%) | MSD (mm) | HDD (mm) |
|---|---|---|---|---|---|
| liver | Pre–AP | N | |||
| R | |||||
| NR | 4.34 ± 1.04 | ||||
| DP–AP | N | ||||
| R | |||||
| NR | 98.1 ± 1.2 | 0.54 ± 0.38 | 6.16 ± 2.92 | ||
| lesion | Pre–AP | N | |||
| R | |||||
| NR | 98.7 ± 0.5 | 0.31 ± 0.27 | 2.24 ± 0.58 | ||
| DP–AP | N | ||||
| R | |||||
| NR | 98.3 ± 0.8 | 0.64 ± 0.72 | 2.34 ± 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.; Ying, S.; Huang, M.; Qiu, C.; Lu, F.; Peng, Z.; Kong, D. Three-Dimensional Voxel-Wise Quantitative Assessment of Imaging Features in Hepatocellular Carcinoma. Diagnostics 2023, 13, 1170. https://doi.org/10.3390/diagnostics13061170
Huang C, Ying S, Huang M, Qiu C, Lu F, Peng Z, Kong D. Three-Dimensional Voxel-Wise Quantitative Assessment of Imaging Features in Hepatocellular Carcinoma. Diagnostics. 2023; 13(6):1170. https://doi.org/10.3390/diagnostics13061170
Chicago/Turabian StyleHuang, Chongfei, Shihong Ying, Meixiang Huang, Chenhui Qiu, Fang Lu, Zhiyi Peng, and Dexing Kong. 2023. "Three-Dimensional Voxel-Wise Quantitative Assessment of Imaging Features in Hepatocellular Carcinoma" Diagnostics 13, no. 6: 1170. https://doi.org/10.3390/diagnostics13061170