
Cell-Free DNA in Plasma and Serum Indicates Disease Severity and Prognosis in Blunt Trauma Patients
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Preanalytical and Analytical Methods
2.3. Statistics
3. Results
3.1. Data Distribution of cfDNA in Trauma Groups
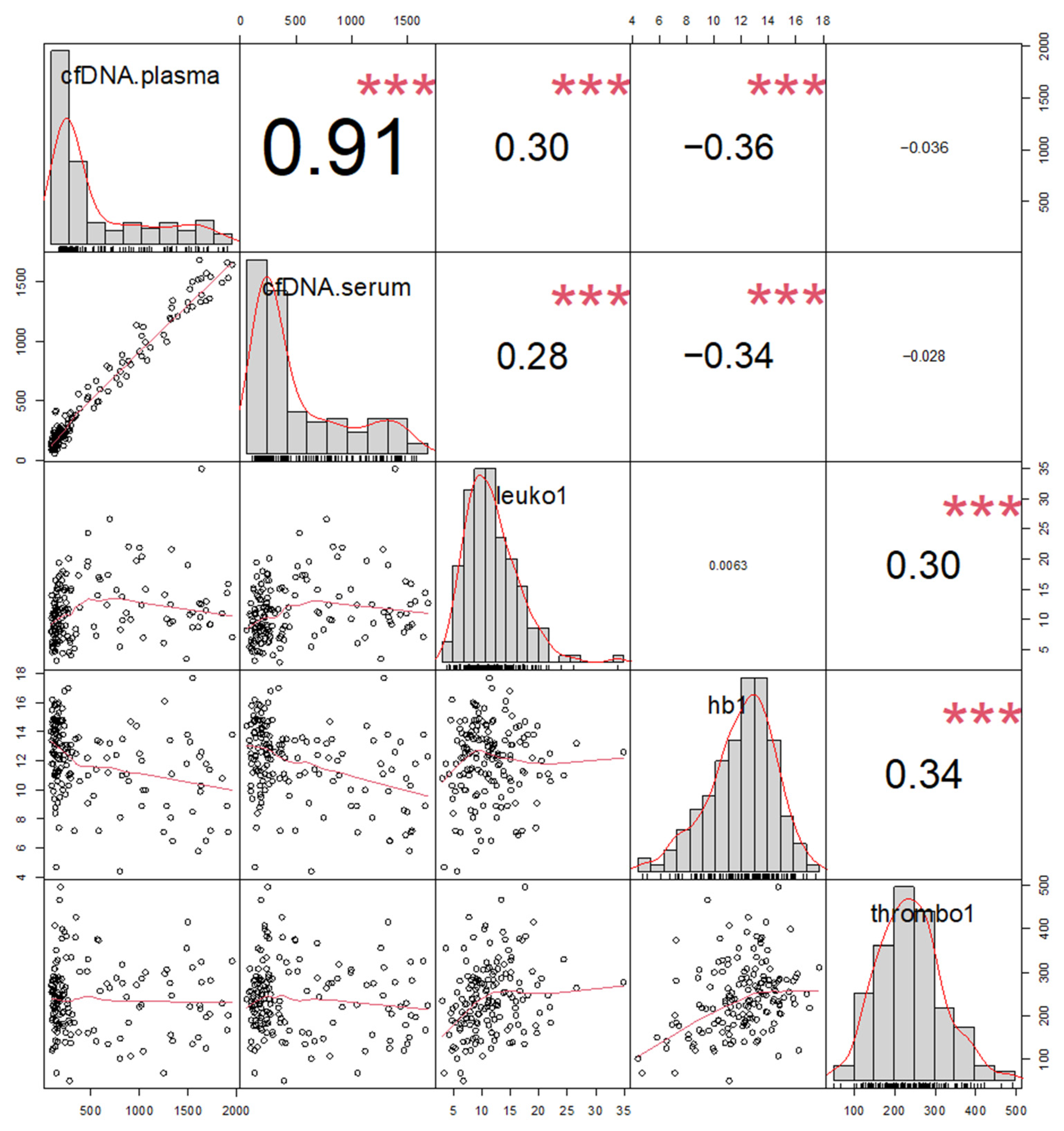
3.2. Correlations of cfDNA and Hematology in Overall Patient Group
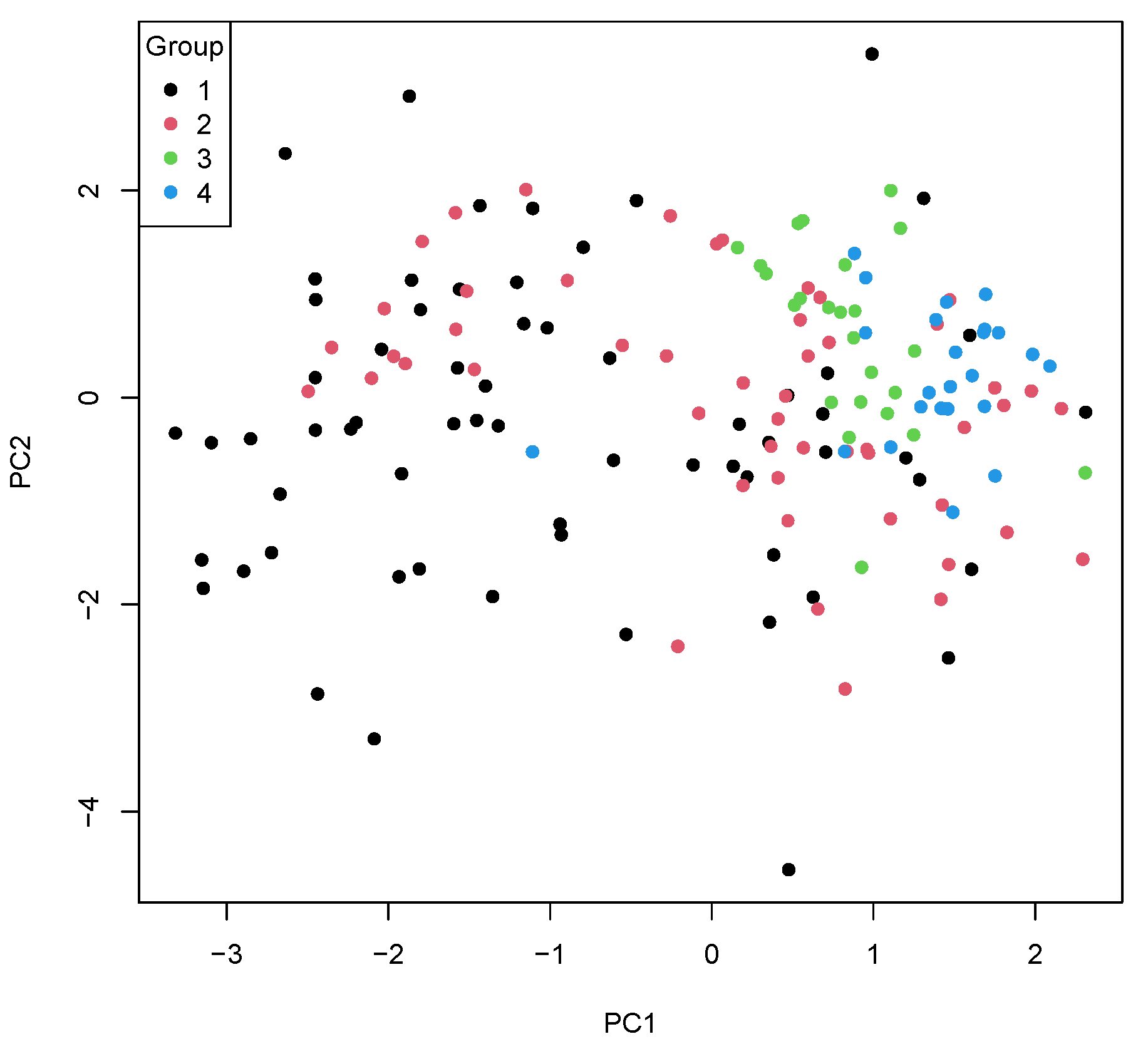
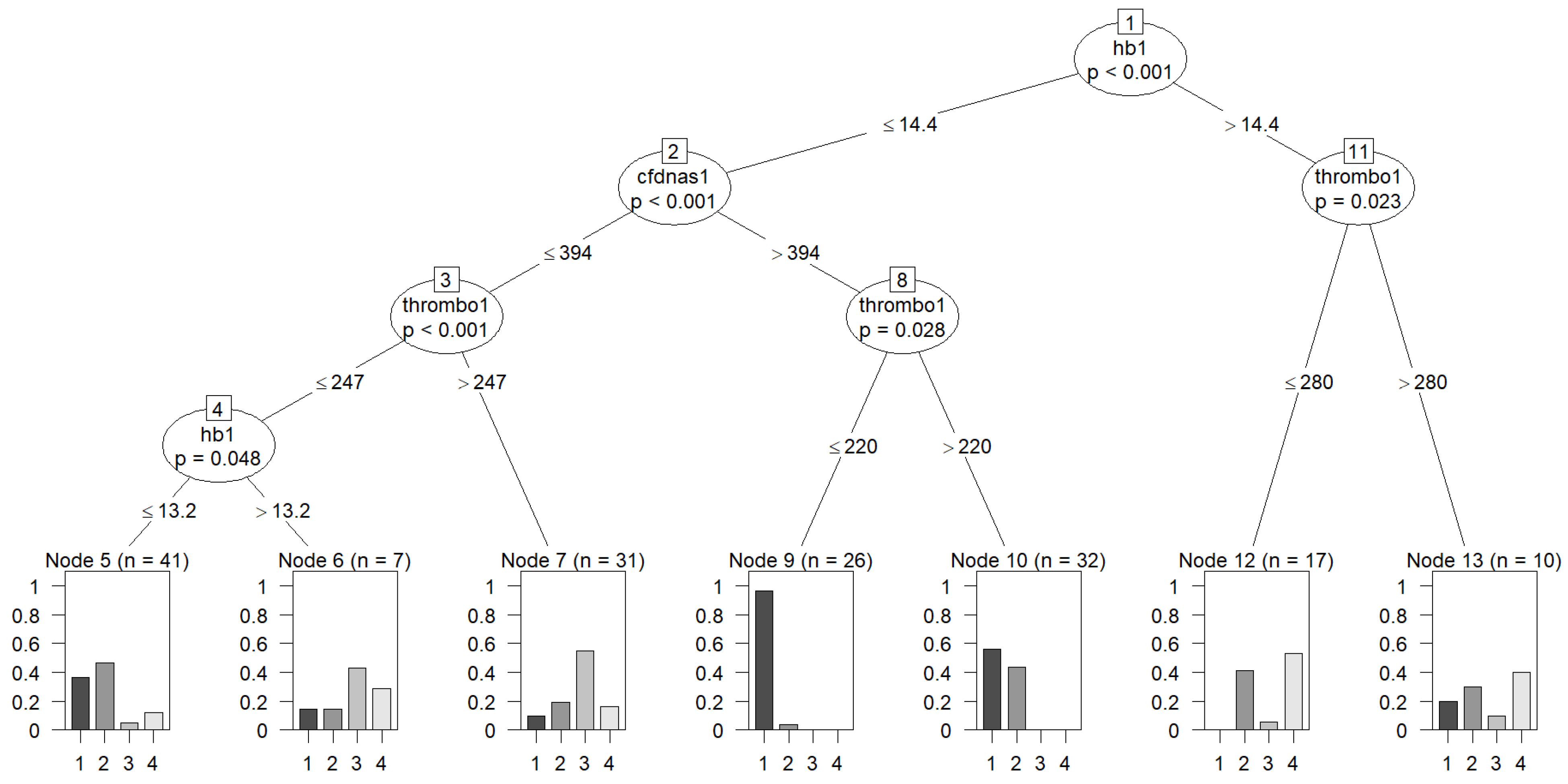
3.3. Differential Diagnosis of Severe Multiple Trauma
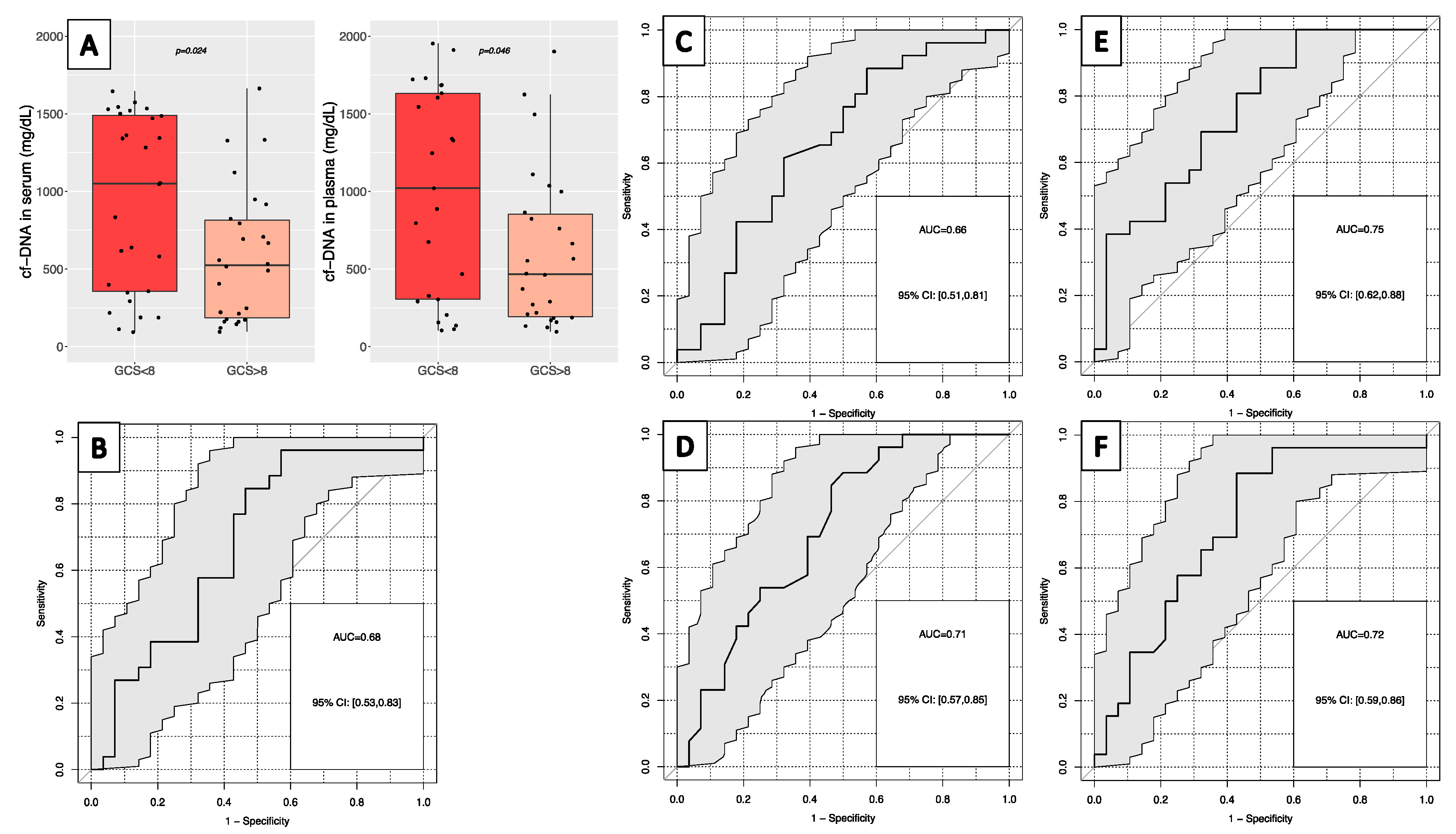
3.4. Correlation and Prognosis of cfDNA and Trauma Severity
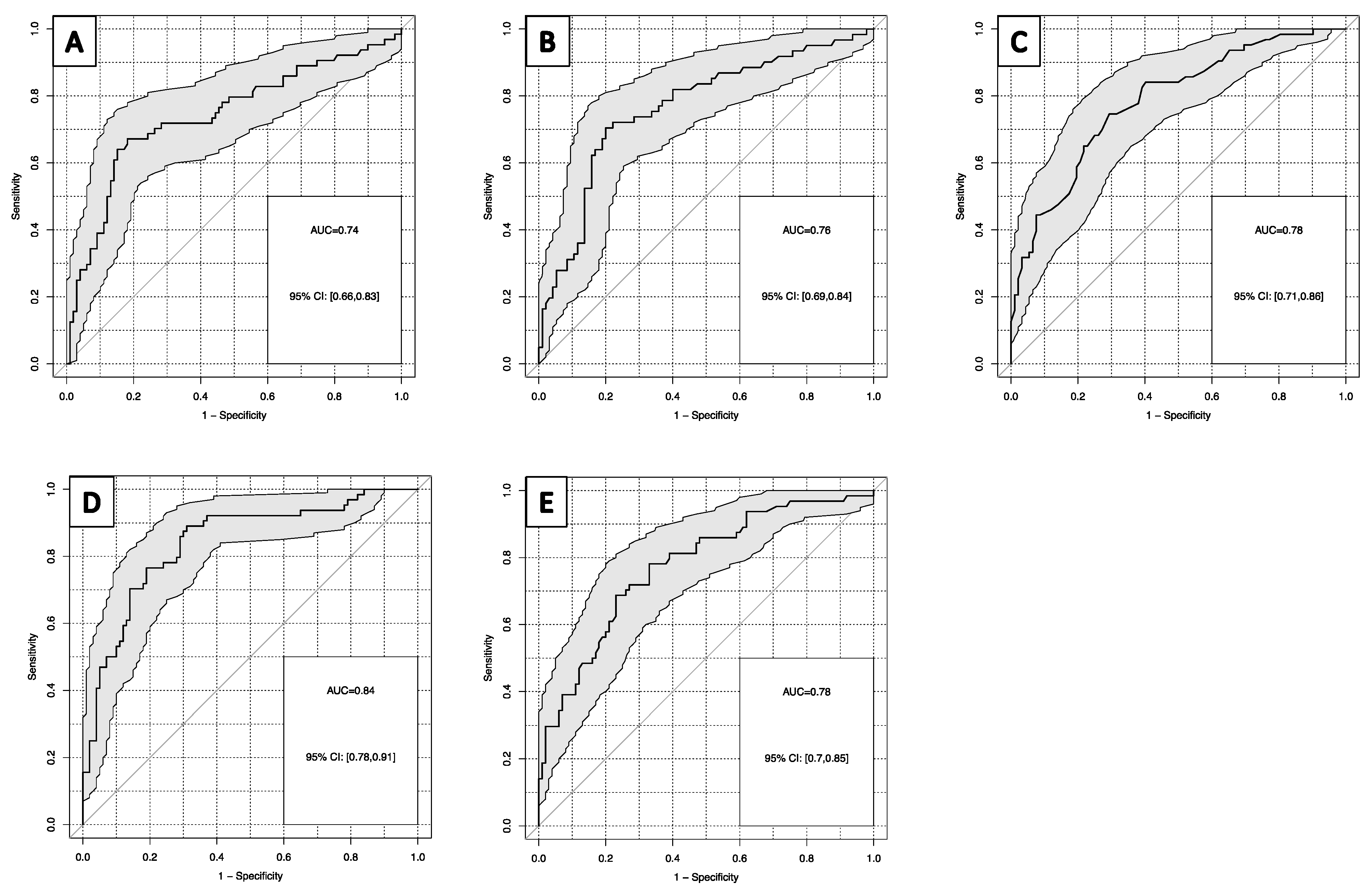
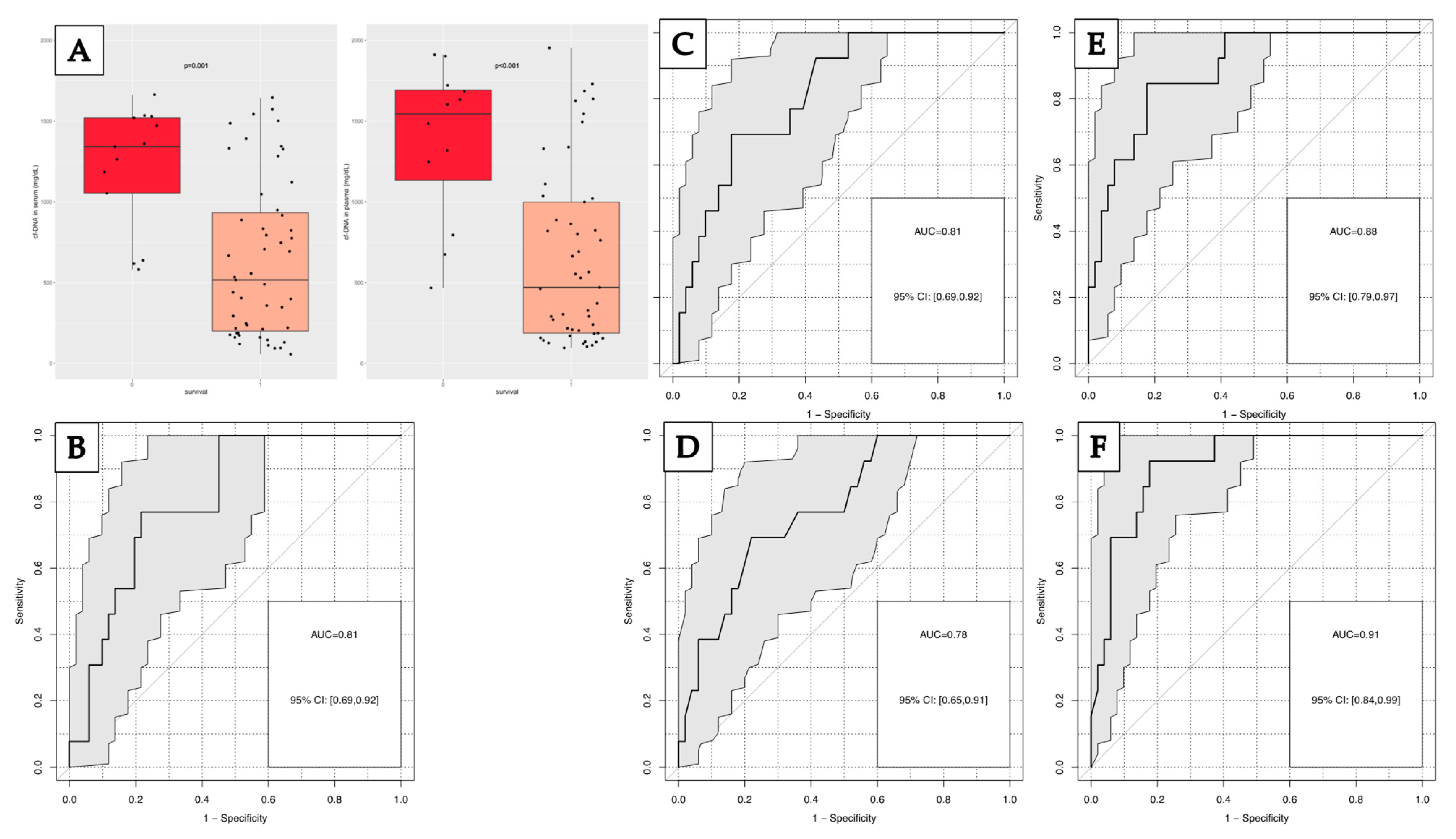
3.5. Prognosis of In-Hospital First-Week Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Health Estimates: Life Expectancy and Leading Causes of Death and Disability. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (accessed on 27 April 2022).
- Jucá Moscardi, M.F.; Meizoso, J.; Rattan, R. Trauma Epidemiology. In The Trauma Golden Hour; Nasr, A., Saavedra Tomasich, F., Collaço, I., Abreu, P., Namias, N., Marttos, A., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 5–8. ISBN 978-3-030-26442-0. [Google Scholar]
- Jahresbericht 2022—Trauma Register DGU®. Available online: https://www.traumaregister-dgu.de/fileadmin/user_upload/TR-DGU-Jahresbericht_2022.pdf (accessed on 3 February 2023).
- Baker, S.P.; O’neill, B.; Haddon, W.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma Inj. Infect. Crit. Care 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Gennarelli, T.A.; Wodzin, E. AIS 2005: A Contemporary Injury Scale. Injury 2006, 37, 1083–1091. [Google Scholar] [CrossRef]
- Zuercher, M.; Ummenhofer, W.; Baltussen, A.; Walder, B. The Use of Glasgow Coma Scale in Injury Assessment: A Critical Review. Brain Inj. 2009, 23, 371–384. [Google Scholar] [CrossRef]
- Nasr, A.; Saavedra Tomasich, F.; Collaço, I.; Abreu, P.; Namias, N.; Marttos, A. (Eds.) The Trauma Golden Hour: A Practical Guide; Springer International Publishing: Cham, Switzerland, 2020; ISBN 978-3-030-26442-0. [Google Scholar]
- Keel, M.; Trentz, O. Pathophysiology of Polytrauma. Injury 2005, 36, 691–709. [Google Scholar] [CrossRef]
- Lord, J.M.; Midwinter, M.J.; Chen, Y.-F.; Belli, A.; Brohi, K.; Kovacs, E.J.; Koenderman, L.; Kubes, P.; Lilford, R.J. The Systemic Immune Response to Trauma: An Overview of Pathophysiology and Treatment. Lancet 2014, 384, 1455–1465. [Google Scholar] [CrossRef] [Green Version]
- Stawski, R.; Stec-Martyna, E.; Chmielecki, A.; Nowak, D.; Perdas, E. Current Trends in Cell-Free DNA Applications. Scoping Review of Clinical Trials. Biology 2021, 10, 906. [Google Scholar] [CrossRef] [PubMed]
- de Miranda, F.S.; Barauna, V.G.; dos Santos, L.; Costa, G.; Vassallo, P.F.; Campos, L.C.G. Properties and Application of Cell-Free DNA as a Clinical Biomarker. Int. J. Mol. Sci. 2021, 22, 9110. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.M.D.; Corbetta, N.; Chamberlain, P.F.; Rai, V.; Sargent, I.L.; Redman, C.W.; Wainscoat, J.S. Presence of Fetal DNA in Maternal Plasma and Serum. Lancet 1997, 350, 485–487. [Google Scholar] [CrossRef]
- Andreatta, M.V.; Curty, V.M.; Coutinho, J.V.S.; Santos, M.Â.A.; Vassallo, P.F.; de Sousa, N.F.; Barauna, V.G. Cell-Free DNA as an Earlier Predictor of Exercise-Induced Performance Decrement Related to Muscle Damage. Int. J. Sports Physiol. Perform. 2018, 13, 953–956. [Google Scholar] [CrossRef] [PubMed]
- Jackson Chornenki, N.L.; Coke, R.; Kwong, A.C.; Dwivedi, D.J.; Xu, M.K.; McDonald, E.; Marshall, J.C.; Fox-Robichaud, A.E.; Charbonney, E.; Liaw, P.C. Comparison of the Source and Prognostic Utility of CfDNA in Trauma and Sepsis. Intensive Care Med. Exp. 2019, 7, 29. [Google Scholar] [CrossRef] [Green Version]
- Vajpeyee, A.; Wijatmiko, T.; Vajpeyee, M.; Taywade, O.; Pandey, S.; Chauhan, P.S. Clinical Usefulness of Cell-Free DNA as a Prognostic Marker in Acute Ischemic Stroke. Neurologist 2020, 25, 11–13. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, G.C.; Petrone, A.B.; Tennant, C.S.; Lucke-Wold, N.; Kabbani, Y.; Tarabishy, A.R.; Chantler, P.D.; Barr, T.L. Circulating Extracellular DNA Levels Are Acutely Elevated in Ischaemic Stroke and Associated with Innate Immune System Activation. Brain Inj. 2017, 31, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Kronbichler, A.; Park, D.D.-Y.; Park, Y.; Moon, H.; Kim, H.; Choi, J.H.; Choi, Y.; Shim, S.; Lyu, I.S.; et al. Neutrophil Extracellular Traps (NETs) in Autoimmune Diseases: A Comprehensive Review. Autoimmun. Rev. 2017, 16, 1160–1173. [Google Scholar] [CrossRef] [PubMed]
- Dinsdale, R.J.; Hazeldine, J.; Al Tarrah, K.; Hampson, P.; Devi, A.; Ermogenous, C.; Bamford, A.L.; Bishop, J.; Watts, S.; Kirkman, E.; et al. Dysregulation of the Actin Scavenging System and Inhibition of DNase Activity Following Severe Thermal Injury. Br. J. Surg. 2020, 107, 391–401. [Google Scholar] [CrossRef] [Green Version]
- Pantalone, D.; Bergamini, C.; Martellucci, J.; Alemanno, G.; Bruscino, A.; Maltinti, G.; Sheiterle, M.; Viligiardi, R.; Panconesi, R.; Guagni, T.; et al. The Role of DAMPS in Burns and Hemorrhagic Shock Immune Response: Pathophysiology and Clinical Issues. Review. Int. J. Mol. Sci. 2021, 22, 7020. [Google Scholar] [CrossRef]
- Konishi, S.; Narita, T.; Hatakeyama, S.; Yoneyama, T.; Yoneyama, M.S.; Tobisawa, Y.; Noro, D.; Sato, T.; Togashi, K.; Okamoto, T.; et al. Utility of Total Cell-Free DNA Levels for Surgical Damage Evaluation in Patients with Urological Surgeries. Sci. Rep. 2021, 11, 22103. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Hoon, D.S.B.; Pantel, K. Cell-Free Nucleic Acids as Biomarkers in Cancer Patients. Nat. Rev. Cancer 2011, 11, 426–437. [Google Scholar] [CrossRef]
- Brodbeck, K.; Kern, S.; Schick, S.; Steinbrück, A.; Schwerer, M.; Bayer, B.; Anslinger, K.; Peldschus, S. Quantitative Analysis of Individual Cell-Free DNA Concentration before and after Penetrating Trauma. Int. J. Legal Med. 2019, 133, 385–393. [Google Scholar] [CrossRef]
- Timmermans, K.; Kox, M.; Scheffer, G.J.; Pickkers, P. Danger in the Intensive Care Unit: Damps in Critically Ill Patients. Shock 2016, 45, 108–116. [Google Scholar] [CrossRef]
- Bronkhorst, A.J.; Ungerer, V.; Oberhofer, A.; Gabriel, S.; Polatoglou, E.; Randeu, H.; Uhlig, C.; Pfister, H.; Mayer, Z.; Holdenrieder, S. New Perspectives on the Importance of Cell-Free DNA Biology. Diagnostics 2022, 12, 2147. [Google Scholar] [CrossRef]
- Marcatti, M.; Saada, J.; Okereke, I.; Wade, C.E.; Bossmann, S.H.; Motamedi, M.; Szczesny, B. Quantification of Circulating Cell Free Mitochondrial DNA in Extracellular Vesicles with PicoGreenTM in Liquid Biopsies: Fast Assessment of Disease/Trauma Severity. Cells 2021, 10, 819. [Google Scholar] [CrossRef]
- Grabuschnig, S.; Bronkhorst, A.J.; Holdenrieder, S.; Rosales Rodriguez, I.; Schliep, K.P.; Schwendenwein, D.; Ungerer, V.; Sensen, C.W. Putative Origins of Cell-Free DNA in Humans: A Review of Active and Passive Nucleic Acid Release Mechanisms. Int. J. Mol. Sci. 2020, 21, 8062. [Google Scholar] [CrossRef] [PubMed]
- Bronkhorst, A.J.; Wentzel, J.F.; Aucamp, J.; van Dyk, E.; du Plessis, L.; Pretorius, P.J. Characterization of the Cell-Free DNA Released by Cultured Cancer Cells. Biochim. Biophys. Acta BBA Mol. Cell Res. 2016, 1863, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.K.; Naidu, G. The Role of Danger-Associated Molecular Patterns (DAMPs) in Trauma and Infections. J. Thorac. Dis. 2016, 8, 1406–1409. [Google Scholar] [CrossRef] [Green Version]
- Relja, B.; Land, W.G. Damage-Associated Molecular Patterns in Trauma. Eur. J. Trauma Emerg. Surg. 2020, 46, 751–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Relja, B.; Mörs, K.; Marzi, I. Danger Signals in Trauma. Eur. J. Trauma Emerg. Surg. 2018, 44, 301–316. [Google Scholar] [CrossRef] [Green Version]
- Gögenur, M.; Burcharth, J.; Gögenur, I. The Role of Total Cell-Free DNA in Predicting Outcomes among Trauma Patients in the Intensive Care Unit: A Systematic Review. Crit. Care 2017, 21, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazeldine, J.; Dinsdale, R.J.; Naumann, D.N.; Acharjee, A.; Bishop, J.R.B.; Lord, J.M.; Harrison, P. Traumatic Injury Is Associated with Reduced Deoxyribonuclease Activity and Dysregulation of the Actin Scavenging System. Burns Trauma 2021, 9, tkab001. [Google Scholar] [CrossRef] [PubMed]
- Lubkin, D.T.; Bishawi, M.; Barbas, A.S.; Brennan, T.V.; Kirk, A.D. Extracellular Mitochondrial DNA and N-Formyl Peptides in Trauma and Critical Illness: A Systematic Review. Crit. Care Med. 2018, 46, 2018–2028. [Google Scholar] [CrossRef]
- Stahl, J.B.; Hoecherl, E.F.; Durner, J.; Nagel, D.; Wolf, K.; Holdenrieder, S. HMGB1, Nucleosomes and SRAGE as New Prognostic Serum Markers after Multiple Trauma. Lab. Med. 2016, 40, 165–173. [Google Scholar] [CrossRef]
- McIlroy, D.J.; Bigland, M.; White, A.E.; Hardy, B.M.; Lott, N.; Smith, D.W.; Balogh, Z.J. Cell Necrosis–Independent Sustained Mitochondrial and Nuclear DNA Release Following Trauma Surgery. J. Trauma Acute Care Surg. 2015, 78, 282–288. [Google Scholar] [CrossRef]
- Comish, P.B.; Carlson, D.; Kang, R.; Tang, D. Damage-Associated Molecular Patterns and the Systemic Immune Consequences of Severe Thermal Injury. J. Immunol. 2020, 205, 1189–1197. [Google Scholar] [CrossRef]
- Gu, X.; Yao, Y.; Wu, G.; Lv, T.; Luo, L.; Song, Y. The Plasma Mitochondrial DNA Is an Independent Predictor for Post-Traumatic Systemic Inflammatory Response Syndrome. PLoS ONE 2013, 8, e72834. [Google Scholar] [CrossRef]
- Margraf, S.; Lögters, T.; Reipen, J.; Altrichter, J.; Scholz, M.; Windolf, J. Neutrophil-derived circulating free DNA (cf-DNA/NETs): A potential prognostic marker for posttraumatic development of inflammatory second hit and sepsis. Shock 2008, 30, 352–358. [Google Scholar] [CrossRef]
- Manson, J.; Thiemermann, C.; Brohi, K. Trauma Alarmins as Activators of Damage-Induced Inflammation. Br. J. Surg. 2011, 99, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Pugin, J. How Tissue Injury Alarms the Immune System and Causes a Systemic Inflammatory Response Syndrome. Ann. Intensive Care 2012, 2, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Block, H.; Rossaint, J.; Zarbock, A. The Fatal Circle of NETs and NET-Associated DAMPs Contributing to Organ Dysfunction. Cells 2022, 11, 1919. [Google Scholar] [CrossRef]
- Bhagirath, V.C.; Dwivedi, D.J.; Liaw, P.C. Comparison of the Proinflammatory and Procoagulant Properties of Nuclear, Mitochondrial, and Bacterial DNA. Shock 2015, 44, 265–271. [Google Scholar] [CrossRef]
- Aswani, A.; Manson, J.; Itagaki, K.; Chiazza, F.; Collino, M.; Wupeng, W.L.; Chan, T.K.; Wong, W.S.F.; Hauser, C.J.; Thiemermann, C.; et al. Scavenging Circulating Mitochondrial DNA as a Potential Therapeutic Option for Multiple Organ Dysfunction in Trauma Hemorrhage. Front. Immunol. 2018, 9, 891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faust, H.E.; Oniyide, O.; Wang, Y.; Forker, C.M.; Dunn, T.; Yang, W.; Lanken, P.N.; Sims, C.A.; Yehya, N.; Christie, J.D.; et al. Early Plasma Nuclear DNA, Mitochondrial DNA, and Nucleosome Concentrations Are Associated With Acute Kidney Injury in Critically Ill Trauma Patients. Crit. Care Explor. 2022, 4, e0663. [Google Scholar] [CrossRef]
- Campello Yurgel, V.; Ikuta, N.; Brondani da Rocha, A.; Lunge, V.R.; Fett Schneider, R.; Kazantzi Fonseca, A.S.; Grivicich, I.; Zanoni, C.; Regner, A. Role of Plasma DNA as a Predictive Marker of Fatal Outcome Following Severe Head Injury in Males. J. Neurotrauma 2007, 24, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Wijeratne, S.; Butt, A.; Burns, S.; Sherwood, K.; Boyd, O.; Swaminathan, R. Cell-Free Plasma DNA as a Prognostic Marker in Intensive Treatment Unit Patients. Ann. N. Y. Acad. Sci. 2004, 1022, 232–238. [Google Scholar] [CrossRef]
- Lima-Oliveira, G.; Monneret, D.; Guerber, F.; Guidi, G.C. Sample Management for Clinical Biochemistry Assays: Are Serum and Plasma Interchangeable Specimens? Crit. Rev. Clin. Lab. Sci. 2018, 55, 480–500. [Google Scholar] [CrossRef] [PubMed]
- Meddeb, R.; Pisareva, E.; Thierry, A.R. Guidelines for the Preanalytical Conditions for Analyzing Circulating Cell-Free DNA. Clin. Chem. 2019, 65, 623–633. [Google Scholar] [CrossRef]
- Zinkova, A.; Brynychova, I.; Svacina, A.; Jirkovska, M.; Korabecna, M. Cell-Free DNA from Human Plasma and Serum Differs in Content of Telomeric Sequences and Its Ability to Promote Immune Response. Sci. Rep. 2017, 7, 2591. [Google Scholar] [CrossRef]
- Thurairajah, K.; Briggs, G.D.; Balogh, Z.J. The Source of Cell-Free Mitochondrial DNA in Trauma and Potential Therapeutic Strategies. Eur. J. Trauma Emerg. Surg. 2018, 44, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Pfister, H. Neutrophil Extracellular Traps and Neutrophil-Derived Extracellular Vesicles: Common Players in Neutrophil Effector Functions. Diagnostics 2022, 12, 1715. [Google Scholar] [CrossRef] [PubMed]
- Goswami, J.; MacArthur, T.; Bailey, K.; Spears, G.; Kozar, R.A.; Auton, M.; Dong, J.-F.; Key, N.S.; Heller, S.; Loomis, E.; et al. Neutrophil Extracellular Trap Formation and Syndecan-1 Shedding Are Increased after Trauma. Shock 2021, 56, 433–439. [Google Scholar] [CrossRef]
- Stortz, J.A.; Hawkins, R.B.; Holden, D.C.; Raymond, S.L.; Wang, Z.; Brakenridge, S.C.; Cuschieri, J.; Moore, F.A.; Maier, R.V.; Moldawer, L.L.; et al. Cell-Free Nuclear, but Not Mitochondrial, DNA Concentrations Correlate with the Early Host Inflammatory Response after Severe Trauma. Sci. Rep. 2019, 9, 13648. [Google Scholar] [CrossRef] [Green Version]
- Itagaki, K.; Kaczmarek, E.; Lee, Y.T.; Tang, I.T.; Isal, B.; Adibnia, Y.; Sandler, N.; Grimm, M.J.; Segal, B.H.; Otterbein, L.E.; et al. Mitochondrial DNA Released by Trauma Induces Neutrophil Extracellular Traps. PLoS ONE 2015, 10, e0120549. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.J.; Brohi, K.; Calfee, C.S.; Rahn, P.; Chesebro, B.B.; Christiaans, S.C.; Carles, M.; Howard, M.; Pittet, J.-F. Early Release of High Mobility Group Box Nuclear Protein 1 after Severe Trauma in Humans: Role of Injury Severity and Tissue Hypoperfusion. Crit. Care 2009, 13, R174. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | (%) | Age Median (Range) | |
|---|---|---|---|
| I: Patients with severe multiple trauma (SMT, ISS ≥ 16) | 64 | 43.4 (16–88) | |
| Gender | |||
| Female | 24 | 37.5% | |
| Male | 40 | 62.5% | |
| Head injury | |||
| GCS ≤ 8 | 28 | 43.8% | |
| GCS > 8 | 26 | 40.6% | |
| No GCS available | 10 | 15.6% | |
| Injured body region | |||
| Head and neck | 52 | 81.3% | |
| Chest | 45 | 70.3% | |
| Abdomen | 26 | 40.6% | |
| Face | 28 | 43.8% | |
| Extremities | 47 | 73.4% | |
| Survival of first week in hospital | |||
| Yes | 51 | 79.7% | |
| No | 13 | 20.3% | |
| II: Patients with moderate multiple trauma (MMT, ISS < 16) | 51 | 45.1 (16–93) | |
| Gender | |||
| Female | 15 | 29.4% | |
| Male | 36 | 70.6% | |
| III: Patients with femur fracture (FNF) | 24 | 71.0 (32–86) | |
| Gender | |||
| Female | 17 | 70.8% | |
| Male | 7 | 29.2% | |
| IV: Patients with ankle fracture (AF) | 25 | 50.7 (20–84) | |
| Gender | |||
| Female | 10 | 40.0% | |
| Male | 15 | 60.0% |
| N | cfDNA Serum (ng/mL) | cfDNA Plasma (ng/mL) | |||
|---|---|---|---|---|---|
| Median | Range | Median | Range | ||
| SMT | 64 | 680 | 57–1663 | 674 | 96–1953 |
| MMT | 51 | 271 | 96–1686 | 211 | 88–1849 |
| p-value | p = 0.003 | p = 0.002 | |||
| FNF | 24 | 203 | 82–387 | 172 | 97–346 |
| p-value | p < 0.001 | p < 0.001 | |||
| AF | 25 | 151 | 85–804 | 125 | 94–908 |
| p-value | p < 0.001 | p < 0.001 | |||
| TBI in SMT | |||||
| GCS ≤ 8 | 28 | 1051 | 93 -1645 | 1020 | 104–1953 |
| GCS > 8 | 26 | 525 | 95–1663 | 466 | 96–1901 |
| p-value | p = 0.024 | p = 0.046 | |||
| Survival in SMT | |||||
| yes | 51 | 516 | 57–1645 | 470 | 96 -1953 |
| no | 13 | 1341 | 581–1663 | 1484 | 467–1911 |
| p-value | p = 0.001 | p < 0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trulson, I.; Stahl, J.; Margraf, S.; Scholz, M.; Hoecherl, E.; Wolf, K.; Durner, J.; Klawonn, F.; Holdenrieder, S. Cell-Free DNA in Plasma and Serum Indicates Disease Severity and Prognosis in Blunt Trauma Patients. Diagnostics 2023, 13, 1150. https://doi.org/10.3390/diagnostics13061150
Trulson I, Stahl J, Margraf S, Scholz M, Hoecherl E, Wolf K, Durner J, Klawonn F, Holdenrieder S. Cell-Free DNA in Plasma and Serum Indicates Disease Severity and Prognosis in Blunt Trauma Patients. Diagnostics. 2023; 13(6):1150. https://doi.org/10.3390/diagnostics13061150
Chicago/Turabian StyleTrulson, Inga, Juliane Stahl, Stefan Margraf, Martin Scholz, Eduard Hoecherl, Konrad Wolf, Juergen Durner, Frank Klawonn, and Stefan Holdenrieder. 2023. "Cell-Free DNA in Plasma and Serum Indicates Disease Severity and Prognosis in Blunt Trauma Patients" Diagnostics 13, no. 6: 1150. https://doi.org/10.3390/diagnostics13061150