
Can Imaging Using Radiomics and Fat Fraction Analysis Detect Early Tissue Changes on Historical CT Scans in the Regions of the Pancreas Gland That Subsequently Develop Adenocarcinoma?
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
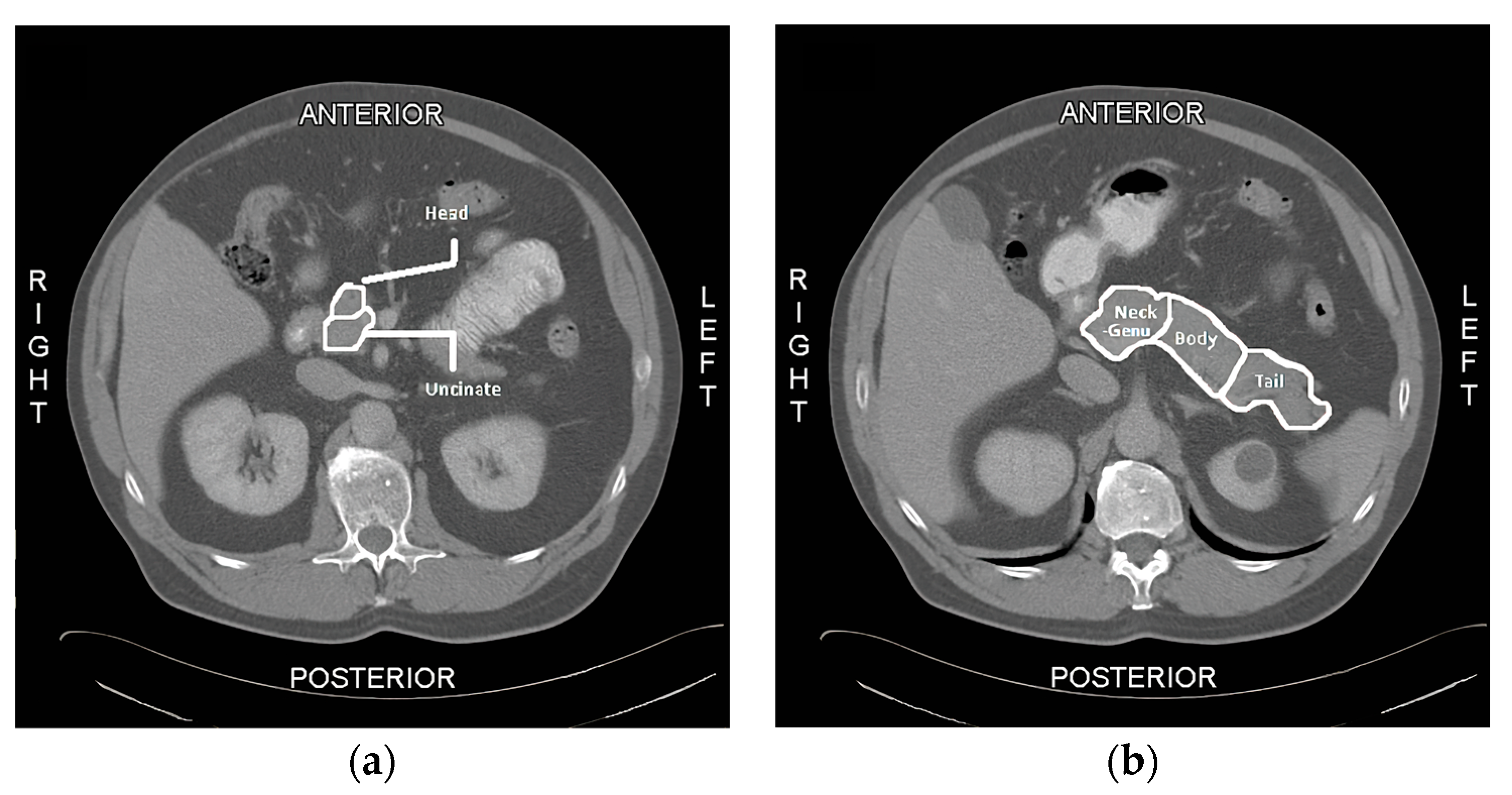
2.1. QTA Analysis of the Pancreas
2.2. Fat Quantification in Slice-O-Matic
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics
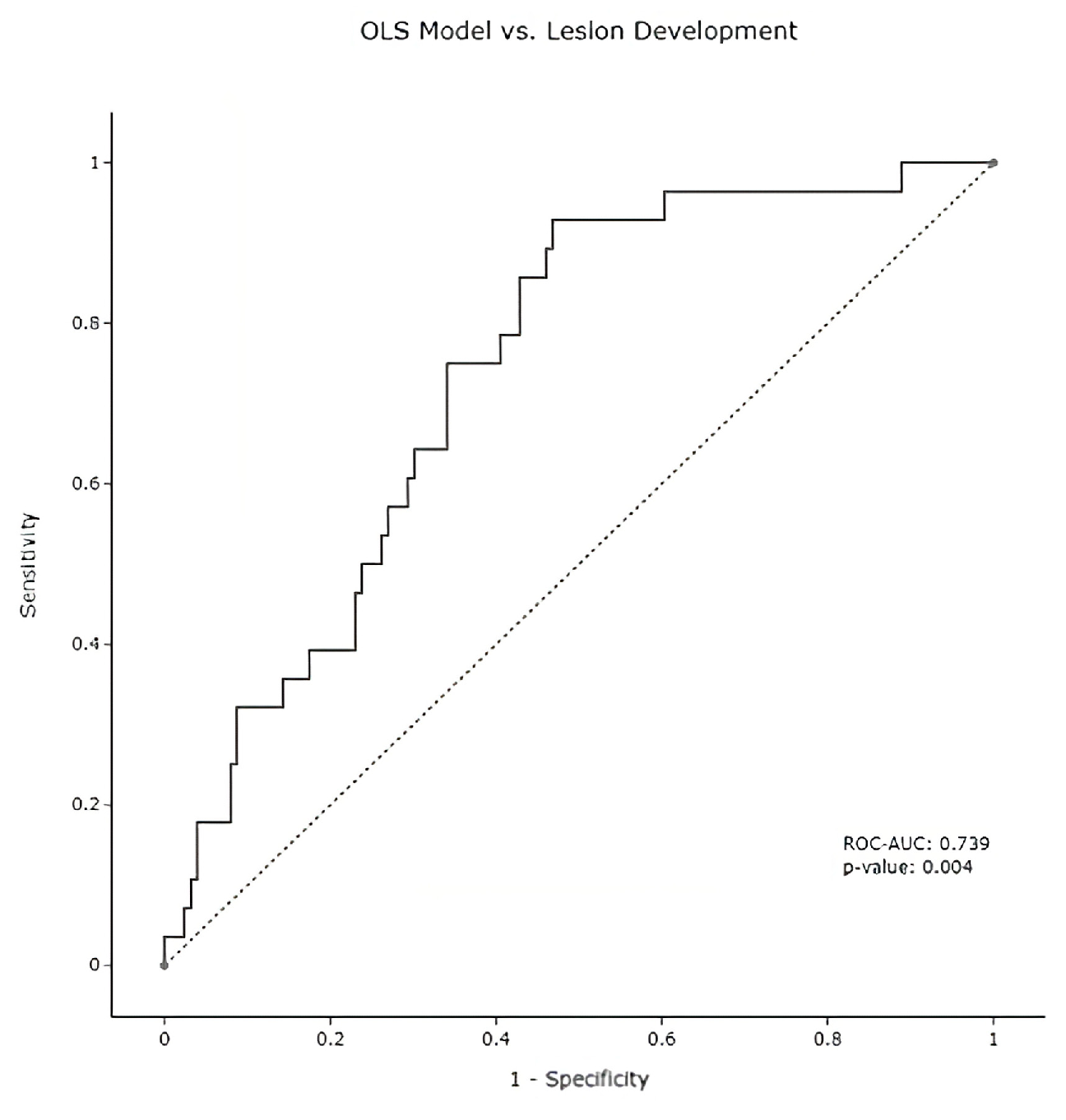
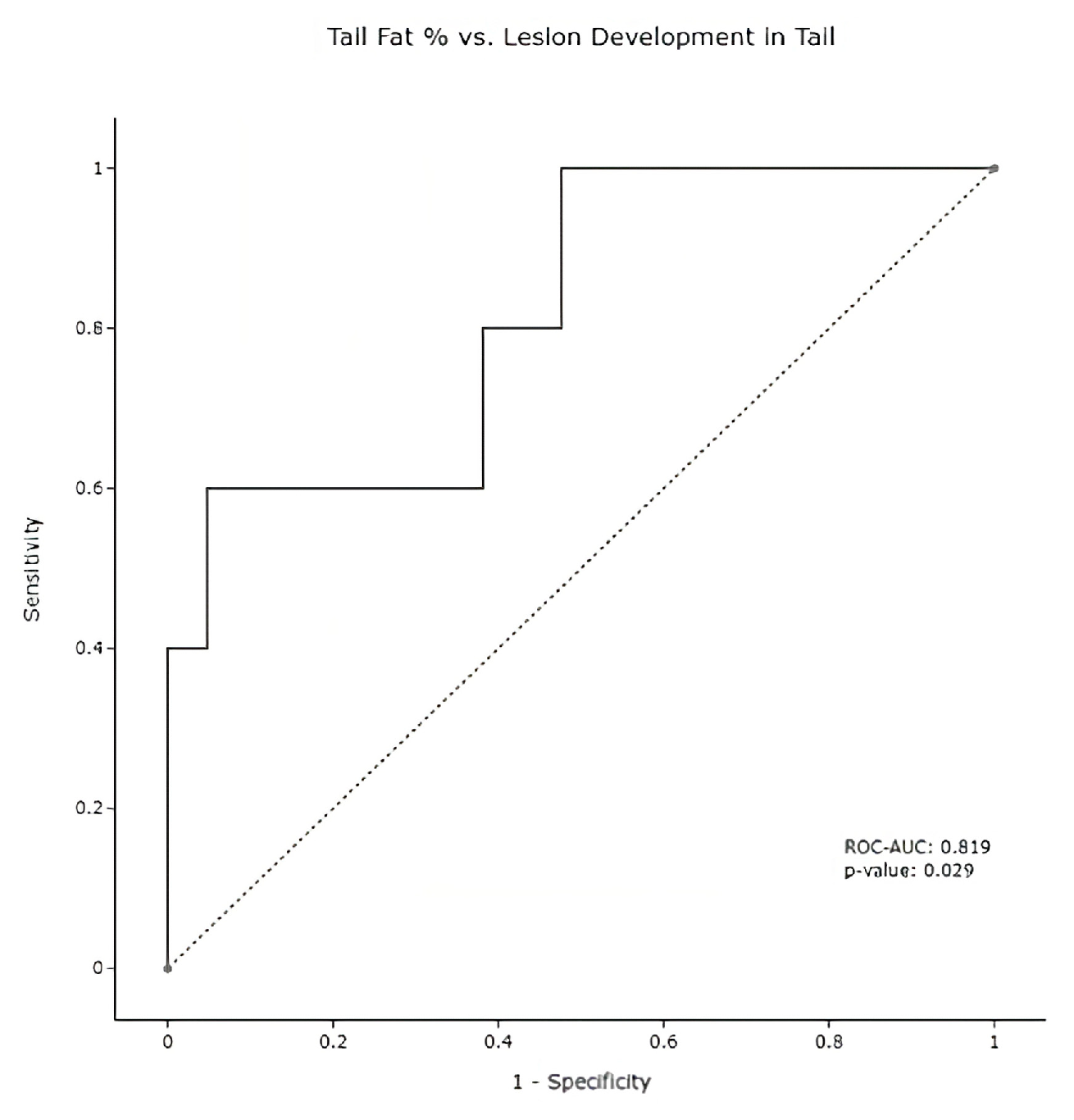
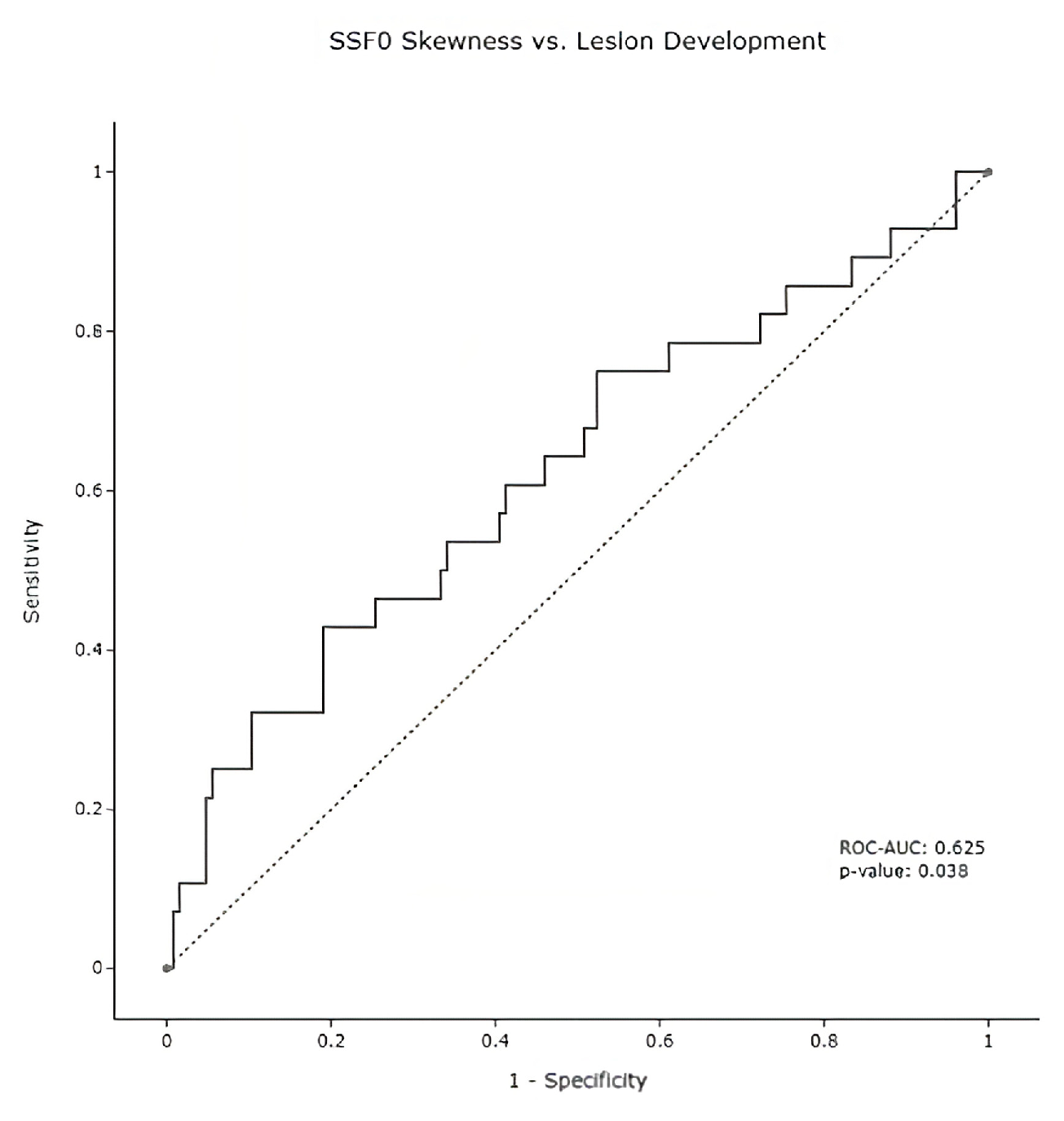
3.2. Radiomic Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, W.; Chawla, A.; O’Reilly, E. Pancreatic Cancer: A Review. JAMA 2021, 326, 851–862. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute: Cancer Stat Facts: Pancreatic Cancer. 2022. Available online: https://seer.cancer.gov/statfacts/html/pancreas.html (accessed on 30 January 2023).
- National Comprehesive Cancer Network Clinical Practice Guidelines in Oncology: Pancreatic Adenocarcinoma. Version 1. 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf (accessed on 30 January 2023).
- Yachida, S.; Jones, S.; Bozic, I.; Antal, T.; Leary, R.; Fu, B.; Kamiyama, M.; Hruban, R.H.; Eshleman, J.R.; Nowak, M.A.; et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature 2010, 467, 1114–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillies, R.J.; Schabath, M.B. Radiomics Improves Cancer Screening and Early Detection Radiomics of Early Detection. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2556–2567. [Google Scholar] [CrossRef] [PubMed]
- Weiss, G.J.; Ganeshan, B.; Miles, K.A.; Campbell, D.H.; Cheung, P.Y.; Frank, S.; Korn, R.L. Noninvasive image texture analysis differentiates K-ras mutation from Pan-wildtype NSCLC and is prognostic. PLoS ONE 2014, 9, e100244. [Google Scholar] [CrossRef] [PubMed]
- Sandrasegaran, K.; Lin, Y.; Asare-Sawiri, M.; Taiyini, T.; Tann, M. CT texture analysis of pancreatic cancer. Eur. Radiol. 2019, 29, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.A.; Vosough, A.; Khalvati, F.; Kiss, A.; Ganeshan, B.; Bjarnason, G.A. CT texture analysis: A potential tool for prediction of survival in patients with metastatic clear cell carcinoma treated with sunitinib. Cancer Imaging 2017, 17, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.T.; Chang, D.; Yen, H.; Liu, K.L.; Huang, S.Y.; Roth, H.; Wu, M.S.; Liao, W.C.; Wang, W. Radiomic features at CT can distinguish pancreatic cancer from noncancerous pancreas. Radiol. Imaging Cancer 2021, 3, e210010. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Oshima, K.; Schott, D.; Wu, H.; Hall, W.; Song, Y.; Tao, Y.; Li, D.; Zheng, C.; Knechtges, P.; et al. (2017). Assessment of treatment response during chemoradiation therapy for pancreatic cancer based on quantitative radiomic analysis of daily CTs: An exploratory study. PLoS ONE 2017, 12, e0178961. [Google Scholar]
- Yun, G.; Kim, Y.H.; Lee, Y.J.; Kim, B.; Hwang, J.H.; Choi, D.J. Tumor heterogeneity of pancreas head cancer assessed by CT texture analysis: Association with survival outcomes after curative resection. Sci. Rep. 2018, 8, 7226. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A.; Ganeshan, B.; Hayball, M.P. CT texture analysis using the filtration-histogram method: What do the measurements mean? Cancer Imaging 2013, 13, 400–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dbouk, M.; Katona, B.W.; Brand, R.E.; Chak, A.; Syngal, S.; Farrell, J.J.; Kastrinos, F.; Stoffel, E.M.; Blackford, A.L.; Rustgi, A.K.; et al. The Multicenter Cancer of Pancreas Screening Study: Impact on Stage and Survival. J. Clin. Oncol. 2022, 40, 3257–3266. [Google Scholar] [CrossRef] [PubMed]
- Baek, H.J.; Kim, H.S.; Kim, N.; Choi, Y.J.; Kim, Y.J. Percent change of perfusion, skewness and kurtosis: A potential imaging biomarker for early treatment response in patients with newly diagnosed glioblastomas. Radiology 2012, 264, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Yamada, D.; Eguchi, H.; Hata, T.; Iwagami, Y.; Noda, T.; Asaoka, T.; Kawamoto, K.; Gotoh, K.; Kobayashi, S.; et al. CT density in the pancreas is a promising imaging predictor for pancreatic ductal adenocarcinoma. Ann. Surg. Oncol. 2017, 24, 2762–2769. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable Name | Coefficient | Odds-Ratio | p-Value |
|---|---|---|---|
| Intercept | −1.0574 | 0.347 | 0.007 |
| Mean | −0.0338 | 0.967 | 0.005 |
| Skewness | 1.0754 | 2.931 | 0.018 |
| Kurtosis Mean Split | 0.9913 | 2.695 | 0.032 |
| Total Pancreas Fat % | −2.9476 | 0.052 | 0.172 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korn, R.L.; Burkett, A.; Geschwind, J.; Zygadlo, D.; Brodie, T.; Cridebring, D.; Von Hoff, D.D.; Demeure, M.J. Can Imaging Using Radiomics and Fat Fraction Analysis Detect Early Tissue Changes on Historical CT Scans in the Regions of the Pancreas Gland That Subsequently Develop Adenocarcinoma? Diagnostics 2023, 13, 941. https://doi.org/10.3390/diagnostics13050941
Korn RL, Burkett A, Geschwind J, Zygadlo D, Brodie T, Cridebring D, Von Hoff DD, Demeure MJ. Can Imaging Using Radiomics and Fat Fraction Analysis Detect Early Tissue Changes on Historical CT Scans in the Regions of the Pancreas Gland That Subsequently Develop Adenocarcinoma? Diagnostics. 2023; 13(5):941. https://doi.org/10.3390/diagnostics13050941
Chicago/Turabian StyleKorn, Ronald Lee, Andre Burkett, Jeff Geschwind, Dominic Zygadlo, Taylor Brodie, Derek Cridebring, Daniel D. Von Hoff, and Michael J. Demeure. 2023. "Can Imaging Using Radiomics and Fat Fraction Analysis Detect Early Tissue Changes on Historical CT Scans in the Regions of the Pancreas Gland That Subsequently Develop Adenocarcinoma?" Diagnostics 13, no. 5: 941. https://doi.org/10.3390/diagnostics13050941