
Challenging Patterns of Atypical Dermatofibromas and Promising Diagnostic Tools for Differential Diagnosis of Malignant Lesions
 , , ,
, , ,
Abstract
:1. Introduction
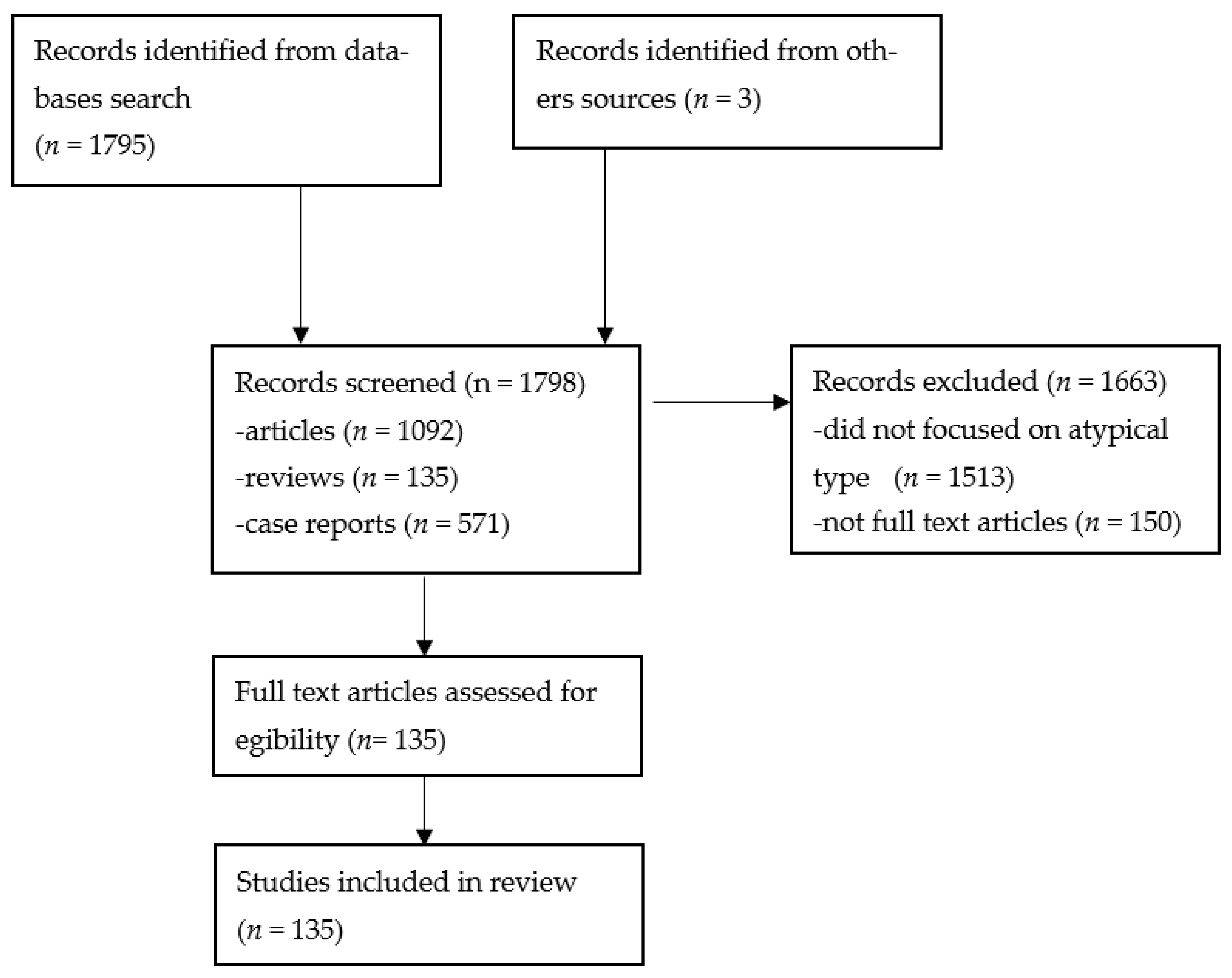
2. Materials and Methods
3. Results
3.1. Clinical Presentation
3.2. Diagnosis and Assessment
- Melanoma-like: various colors and patterns, white structureless areas, polarizing-specific white lines, pink-red or blue-gray structureless areas, dark brown thick reticular lines, peripheral black clods and eccentric distribution of straight, curved, dotted and branched vessels [75].
- Keratoacanthoma-like: central keratin area with a surrounding radial arrangement of polymorphic vessels (curved, branched and dotted) [75].
- Seborrheic keratosis-like: thick curved lines, orange, brown or white clods, brown-black crusted structures, blue-gray structureless areas and loop, dotted or coiled vessels [75].
- Xanthogranuloma-like: yellow structureless areas, coiled vessels with a peripheral reddish halo [75].
- Pyogenic granuloma-like: polymorphic vessels (curved, dotted, straight and branched) with irregular distribution, white lines and pink-red structureless areas [75].
- Spitzoid-like: pink-red structureless areas, shiny white lines, white structureless areas, light brown clods, halo phenomenon, dotted vessels [75].
3.3. Histologic Variants
3.4. Differential Diagnosis
4. Discussion
Promising Differential Diagnostic Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aytekin, S.; Kaynak, E.; Ayhan, E. Dermoscopy of dermatofibromas: A new perspective. Int. J. Clin. Pract. 2021, 75, e14547. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.V.P.; Matos, D.M.; Barreiros, H.F.; Bártolo, E.A.F.L.F. Variants of dermatofibroma-a histopathological study. An. Bras. Dermatol. 2014, 89, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Llambrich, A.; Vila, A.; Terrasa, F.; Bañuls, J.; Nadal, C.; Zaballos, P. Dermoscopy of pink nodular dermatofibromas: A study of 36 cases. Australas. J. Dermatol. 2019, 60, e357–e360. [Google Scholar] [CrossRef]
- uptodate.com. Available online: https://www.uptodate.com/contents/overview-of-benign-lesions-of-the-skin?search=dermatofibroma&source=search_result&selectedTitle=1~22&usage_type=default&display_rank=1#H1101419831 (accessed on 2 June 2022).
- Kittler, H.; Rosendahl, C.; Cameron, A.; Tschandl, P. Dermatoscopy: Pattern Analysis of Pigmented and Non-Pigmented Lesions, 2nd ed.; Facultas Verlags und Buchhandels AG: Vienna, Austria, 2016; pp. 9–52. [Google Scholar]
- Gaufin, M.; Michaelis, T.; Duffy, K. Cellular Dermatofibroma: Clinicopathologic Review of 218 Cases of Cellular Dermatofibroma to Determine the Clinical Recurrence Rate. Dermatol. Surg. 2019, 45, 1359–1364. [Google Scholar] [CrossRef]
- Berklite, L.; Ranganathan, S.; John, I.; Picarsic, J.; Santoro, L.; Alaggio, R. Fibrous histiocytoma/dermatofibroma in children: The same as adults? Hum. Pathol. 2020, 99, 107–115. [Google Scholar] [CrossRef]
- Zaballos, P.; Puig, S.; Llambrich, A.; Malvehy, J. Dermoscopy of Dermatofibromas: A prospective morphological study of 412 cases. Arch. Dermatol. 2008, 144, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Argenziano, G.; Buccini, P.; Cota, C.; Sperduti, I.; De Simone, P.; Eibenschutz, L.; Silipo, V.; Zalaudek, I.; Catricalà, C. Typical and atypical dermoscopic presentations of dermatofibroma. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 1375–1380. [Google Scholar] [CrossRef]
- Bowling, J. Diagnostic dermatology. In The Illustrated Guide, 1st ed.; Wiley-Blackell: Oxford, UK, 2012; p. 77. [Google Scholar]
- Lehmer, L.M.; Ragsdale, B.D. Digital dermatofibromas-Common lesion, uncommon location: A series of 26 cases and review of the literature. Dermatol. Online J. 2011, 17. [Google Scholar] [CrossRef]
- Kadakia, S.; Chernobilsky, B.; Iacob, C. Dermatofibroma of the Auricle. J. Drugs Dermatol. 2016, 15, 1270–1272. [Google Scholar] [PubMed]
- Kim, J.M.; Cho, H.J.; Moon, S.-H. Rare experience of keloidal dermatofibroma of forehead. Arch. Craniofacial Surg. 2018, 19, 72–74. [Google Scholar] [CrossRef] [Green Version]
- emedicine.emedscape.com. Available online: https://emedicine.medscape.com/article/1056742-overview (accessed on 20 July 2022).
- Evans, J.; Mattacks, C.; Clarke, T.; Pond, C.M. Dermatofibromas and Arthropod Bites: Is There Any Evidence to Link the Two? Lancet 1989, 334, 36–37. [Google Scholar] [CrossRef] [PubMed]
- Lobato-Berezo, A.; Churruca-Grijelmo, M.; Martínez-Pérez, M.; Imbernón-Moya, A.; Vargas-Laguna, M.E.; Fernández-Cogolludo, E.; Aguilar-Martínez, A.; Gallego-Valdés, M. Dermatofibroma Arising within a Black Tattoo. Case Rep. Dermatol. Med. 2014, 2014, 745304. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Fukuda, H.; Niiyama, S.; Oharasaki, T.; Mukai, H. Multiple dermatofibromas subsequent to folliculitis. Eur. J. Dermatol. 2013, 23, 890–891. [Google Scholar] [CrossRef]
- Nomura, E.; Yamamoto, T. Photoletter to the editor: Fibrous histiocytoma developing at the site of tuberculin skin test. J. Dermatol. Case Rep. 2012, 6, 130–131. [Google Scholar] [CrossRef] [PubMed]
- Myers, D.J.; Fillman, E.P. Dermatofibroma. In StatPearls [Internet]; StatPearls Publishing LLC: Treasure Island, FL, USA, 2022. [Google Scholar]
- Yamamoto, T.; Katayama, I.; Nishioka, K. Role of mast cells in dermatofibroma: Recent viewpoints into the pathogenesis. Eur. J. Dermatol. 2003, 13, 419–423. [Google Scholar] [PubMed]
- Kuroda, K.; Tajima, S. Proliferation of HSP47-positive skin fibroblasts in dermatofibroma. J. Cutan. Pathol. 2008, 35, 21–26. [Google Scholar] [CrossRef]
- Jin, S.Y.; Choi, J.S.; La Choi, Y.; Kim, D.H.; Lee, S.H. Identification of Leukocyte-Specific Protein 1-Positive Cells: A Clue to the Cell of Origin and a Marker for the Diagnosis of Dermatofibroma. Ann. Dermatol. 2015, 27, 157–162. [Google Scholar] [CrossRef]
- Törőcsik, D.; Bárdos, H.; Nagy, L.; Ádány, R. Identification of factor XIII-A as a marker of alternative macrophage activation. Cell Mol. Life Sci. 2005, 62, 2132–2139. [Google Scholar] [CrossRef]
- Cerio, R.; Spaull, J.; Jones, E.W. Histiocytoma cutis: A tumour of dermal dendrocytes (dermal dendrocytoma). Br. J. Dermatol. 2006, 120, 197–206. [Google Scholar] [CrossRef]
- Kubo, M.; Ihn, H.; Yamane, K.; Tamaki, K. The expression levels and the differential expression of transforming growth factor-β receptors in dermatofibroma and dermatofibrosarcoma protuberans. Br. J. Dermatol. 2006, 154, 919–925. [Google Scholar] [CrossRef]
- Yamamoto, T. Dermatofibroma: A possible model of local fibrosis with epithelial/mesenchymal cell interaction. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Sellheyer, K.; Smoller, B.R. Dermatofibroma: Upregulation of Syndecan-1 Expression in Mesenchymal Tissue. Am. J. Dermatopathol. 2003, 25, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Skroza, N.; Rotolo, S.; Ceccarelli, S.; Romano, F.; Innocenzi, D.; Frati, L.; Angeloni, A.; Marchese, C. Modulation of the expression of the FGFR2-IIIb and FGFR2-IIIc molecules in dermatofibroma. J. Dermatol. Sci. 2008, 51, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Walther, C.; Hofvander, J.; Nilsson, J.; Magnusson, L.; Domanski, H.A.; Gisselsson, D.; Tayebwa, J.; Doyle, L.A.; Fletcher, C.D.M.; Mertens, F. Gene fusion detection in formalin-fixed paraffin-embedded benign fibrous histiocytomas using fluorescence in situ hybridization and RNA sequencing. Lab. Investig. 2015, 95, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulos, I.; Gorunova, L.; Bjerkehagen, B.; Lobmaier, I.; Heim, S. LAMTOR1-PRKCD and NUMA1-SFMBT1 fusion genes identified by RNA sequencing in aneurysmal benign fibrous histiocytoma with t(3;11)(p21;q13). Cancer Genet. 2015, 208, 545–551. [Google Scholar] [CrossRef]
- Doyle, L.A.; Mariño-Enriquez, A.; Fletcher, C.D.M.; Hornick, J.L. ALK rearrangement and overexpression in epithelioid fibrous histiocytoma. Mod. Pathol. 2015, 28, 904–912. [Google Scholar] [CrossRef]
- Szablewski, V.; Laurent-Roussel, S.; Rethers, L.; Rommel, A.; Vaneechout, P.; Camboni, A.; Willocz, P.; Copie-Bergman, C.; Ortonne, N. Atypical fibrous histiocytoma of the skin with CD30 and p80/ALK1 positivity and ALK gene rearrangement. J. Cutan. Pathol. 2014, 41, 715–719. [Google Scholar] [CrossRef]
- Chen, T.-C.; Kuo, T.-T.; Chan, H.-L. Dermatofibroma is a clonal proliferative disease. J. Cutan. Pathol. 2000, 27, 36–39. [Google Scholar] [CrossRef]
- Cerio, R.; Spaull, J.; Oliver, G.F.; Jones, E.W. A Study of Factor XHIa and MAC 387 Immunolabeling in Normal and Pathological Skin. Am. J. Dermatopathol. 1990, 12, 221–233. [Google Scholar] [CrossRef]
- Mentzel, T.; Wiesner, T.; Cerroni, L.; Hantschke, M.; Kutzner, H.; Rütten, A.; Häberle, M.; Bisceglia, M.; Chibon, F.; Coindre, J.-M. Malignant dermatofibroma: Clinicopathological, immunohistochemical, and molecular analysis of seven cases. Mod. Pathol. 2013, 26, 256–267. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, A.; Soyer, H.P.; Peris, K.; Argenziano, G.; Mazzocchetti, G.; Piccolo, D.; De Giorgi, V.; Chimenti, S. Central white scarlike patch: A dermatoscopic clue for the diagnosis of dermatofibroma. J. Am. Acad. Dermatol. 2000, 43, 1123–1125. [Google Scholar] [CrossRef]
- Lamgan, S.M.; Robinson, T.W.E. Cryotherapy for dermatofibromas. Clin. Exp. Dermatol. 1987, 12, 121–123. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Mentzel, T. Cutaneous mesenchymal tumours: An update. Pathology 2014, 46, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.B.; Gilchrest, B.A. Dimple Sign to Differentiate Benign from Malignant Pigmented Cutaneous Lesions. N. Engl. J. Med. 1977, 296, 1518. [Google Scholar] [CrossRef] [PubMed]
- Lookingbill, D.P. A Malignant Dimple. N. Engl. J. Med. 1977, 297, 841–842. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.A.; Fletcher, C.D. Metastasizing “Benign” Cutaneous Fibrous Histiocytoma: A clinicopathologic analysis of 16 cases. Am. J. Surg. Pathol. 2013, 37, 484–495. [Google Scholar] [CrossRef] [PubMed]
- Gershtenson, P.C.; Krunic, A.L.; Chen, H.M. Multiple clustered dermatofibroma: Case report and review of the literature. J. Cutan. Pathol. 2010, 37, e42–e45. [Google Scholar] [CrossRef] [PubMed]
- Kalsi, H.; Rahman, A.; Harbol, T.; Sidhu, J. Giant Hemosiderotic Dermatofibroma: The Largest Giant Dermatofibroma Reported to Date. Am. J. Dermatopathol. 2015, 37, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Finch, J.; Berke, A.; McCusker, M.; Chang, M.W. Congenital Multiple Clustered Dermatofibroma in a 12-Year-Old Girl. Pediatr. Dermatol. 2014, 31, 105–106. [Google Scholar] [CrossRef]
- Massone, C.; Parodi, A.; Virno, G.; Rebora, A. Multiple eruptive dermatofibromas in patients with systemic lupus erythematosus treated with prednisone. Int. J. Dermatol. 2002, 41, 279–281. [Google Scholar] [CrossRef] [PubMed]
- García-Millán, C.; Aldanondo, I.; Fernández-Lorente, M.; Carrillo, R.; Jaén, P. Multiple Eruptive Dermatofibromas in 2 Patients Infected with the Human Immunodeficiency Virus. Actas Dermosifiliogr. 2007, 98, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Marque, M.; Pallure, V.; Huet, P.; Bessis, D.; Guillot, B. Multiple familial “eruptive” dermatofibromas. Ann. Dermatol. Venereol. 2013, 140, 452–454. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.-Y.; Chu, C.-Y.; Hsiao, C.-H. Multiple eruptive dermatofibromas in a patient with dermatomyositis taking prednisolone and methotrexate. J. Am. Acad. Dermatol. 2007, 57, S81–S84. [Google Scholar] [CrossRef] [PubMed]
- López, N.; Fernández, A.; Bosch, R.J.; Herrera, E. Multiple eruptive dermatofibromas in a patient with Graves-Basedow disease. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 402–403. [Google Scholar] [CrossRef]
- Kimura, Y.; Kaneko, T.; Akasaka, E.; Nakajima, K.; Aizu, T.; Nakano, H.; Sawamura, D. Multiple eruptive dermatofibromas associated with Hashimoto’s thyroiditis and myasthenia gravis. Eur. J. Dermatol. 2010, 20, 538–539. [Google Scholar] [CrossRef]
- Monteagudo, B.; Suarez-Amor, O.; Cabanillas, M.; Leon-Mateos, A.; Perez-Valcarcel, J.; de las Heras, C. Down syndrome: Another cause of immunosuppression associated with multiple eruptive dermatofibromas? Dermatol. Online J. 2009, 15, 15. [Google Scholar] [CrossRef]
- Alexandrescu, D.T.; Wiernik, P.H. Multiple Eruptive Dermatofibromas Occurring in a Patient with Chronic Myelogenous Leukemia. Arch. Dermatol. 2005, 141, 397–398. [Google Scholar] [CrossRef]
- Bhattacharjee, P.; Umar, S.A.; Fatteh, S.M. Multiple Eruptive Dermatofibromas Occurring in a Patient with Myelodysplastic Syndrome. Acta Derm. Venereol. 2005, 85, 270–271. [Google Scholar] [CrossRef]
- Zaccaria, E.; Rebora, A.; Rongioletti, F. Multiple eruptive dermatofibromas and immunosuppression: Report of two cases and review of the literature. Int. J. Dermatol. 2008, 47, 723–727. [Google Scholar] [CrossRef]
- Yazici, A.C.; Baz, K.; Ikizoglu, G.; Koca, A.; Kokturk, A.; Apa, D.D. Familial eruptive dermatofibromas in atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Beyazit, Y.; Caner, S.; Kurt, M.; Kekilli, M.; Aydog, G.; Ibis, M. Dermatofibroma in a patient with Crohn’s disease: A novel clinical manifestation. J. Crohn’s Colitis 2010, 4, 490–491. [Google Scholar] [CrossRef] [PubMed]
- Hiraiwa, T.; Hanami, Y.; Yamamoto, T. Hidradenitis suppurativa and multiple dermatofibromas in a patient with ulcerative colitis. J. Dermatol. 2013, 40, 1071–1072. [Google Scholar] [CrossRef] [PubMed]
- Goldbach, H.; Wanat, K.; Rosenbach, M. Multiple eruptive dermatofibromas in a patient with sarcoidosis. Cutis 2016, 98, E15–E97. [Google Scholar] [PubMed]
- Bachmeyer, C.; Cordier, F.; Blum, L.; Cazier, A.; Vérola, O.; Aractingi, S. Multiple eruptive dermatofibromas after highly active antiretroviral therapy. Br. J. Dermatol. 2000, 143, 1336–1337. [Google Scholar] [CrossRef] [PubMed]
- Queirós, C.; Uva, L.; de Almeida, L.S.; Filipe, P. Multiple eruptive dermatofibromas associated with pregnancy—A case and literature review. Dermatol. Online J. 2019, 25, 12. [Google Scholar] [CrossRef]
- Santos-Juanes, J.; Coto-Segura, P.; Mallo, S.; Galache, C.; Soto, J. Multiple Eruptive Dermatofibromas in a Patient Receiving Efalizumab. Dermatology 2008, 216, 363. [Google Scholar] [CrossRef]
- Giavedoni, P.; Combalia, A.; Pigem, R.; Mascaró, J.M. Multiple Eruptive Dermatofibromas in a Patient Treated with Brentuximab Vedotin. Actas. Dermosifiliogr. 2019, 110, 419–420. [Google Scholar] [CrossRef]
- Caldarola, G.; Bisceglia, M.; Pellicano, R. Multiple eruptive plaque-like dermatofibromas during anti-TNFα treatment. Int. J. Dermatol. 2013, 52, 638–641. [Google Scholar] [CrossRef]
- Llamas-Velasco, M.; Fraga, J.; Solano-López, G.E.; Steegmann, J.L.; Diez, A.G.; Requena, L. Multiple eruptive dermatofibromas related to imatinib treatment. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 979–981. [Google Scholar] [CrossRef]
- Beatrous, S.V.; Riahi, R.R.; Grisoli, S.B.; Cohen, P.R. Associated conditions in patients with multiple dermatofibromas: Case reports and literature review. Dermatol. Online J. 2017, 23. [Google Scholar] [CrossRef]
- Ohnishi, T.; Sasaki, M.; Nakai, K.; Watanabe, S. Atrophic dermatofibroma. J. Eur. Acad. Dermatol. Venereol. 2004, 18, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Kai, H.; Fujita, H.; Yamamoto, M.; Asahina, A. Polypoid dermatofibroma with a slim pedicle: A case report. Dermatol. Online J. 2012, 18. [Google Scholar] [CrossRef]
- Curcó, N.; Jucgla, A.; Bordas, X.; Moreno, A. Dermatofibroma with spreading satellitosis. J. Am. Acad. Dermatol. 1992, 27, 1017–1019. [Google Scholar] [CrossRef]
- Schofield, C.; Weedon, D.; Kumar, S. Dermatofibroma and halo dermatitis. Australas. J. Dermatol. 2012, 53, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Marinescu, S.A.; Tatu, A.L.; Mihai, I.R.; Giuglea, C. Correlations between clinics, dermoscopy and histopathology in a female with two dermatofibromas-a case report. Rom. J. Morphol. Embryol. 2016, 57, 323–326. [Google Scholar] [PubMed]
- Picard, A.; Long-Mira, E.; Chuah, S.Y.; Passeron, T.; Lacour, J.-P.; Bahadoran, P. Interest of high-definition optical coherent tomography (HD-OCT) for non-invasive imaging of dermatofibroma: A pilot study. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 485–487. [Google Scholar] [CrossRef]
- Demir, M.K.; Ozdemir, H.; Gençhallaç, H.; Altaner, S.; Kartal, O. Dermatofibroma mimicking malignancy on integrated F-18 fluorodeoxyglucose PET-CT. Diagn. Interv. Radiol. 2009, 15, 61–63. [Google Scholar]
- Guedes, R.V.D.A.P.; De Menezes, N.M.N.; Leite, I.B.; Baptista, M.A. Benign fibrous histiocytoma: Particular aspects on confocal laser scanning microscopy. Eur. J. Dermatol. 2012, 22, 288–289. [Google Scholar] [CrossRef]
- Genc, Y.; Akay, B.N.; Heper, A.O.; Rosendahl, C.; Erdem, C. Dermatopathological characteristics of dermatofibromas from dermatoscopic clues. Int. J. Dermatol. 2020, 59, 66–75. [Google Scholar] [CrossRef]
- Lin, M.J.; Xie, C.; Pan, Y.; Jalilian, C.; Kelly, J.W. Dermoscopy improves diagnostic accuracy for clinically amelanotic nodules. Australas. J. Dermatol. 2019, 60, 45–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Won, K.Y.; Park, S.Y.; Jin, W.; Lew, B.-L. Dermatofibroma: Sonographic findings and pathologic correlation. Acta Radiol. 2018, 59, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Kelati, A.; Aqil, N.; Baybay, H.; Gallouj, S.; Mernissi, F.Z. Beyond classic dermoscopic patterns of dermatofibromas: A prospective research study. J. Med. Case Rep. 2017, 11, 266. [Google Scholar] [CrossRef]
- Roldán-Marín, R.; Barreiro-Capurro, A.; García-Herrera, A.; Puig, S.; Alarcón-Salazar, I.; Carrera, C.; Malvehy, J. Green colour as a novel dermoscopic finding in the diagnosis of haemosiderotic dermatofibroma. Australas. J. Dermatol. 2014, 55, 196–197. [Google Scholar] [CrossRef] [PubMed]
- Arpaia, N.; Cassano, N.; Vena, G.A. Dermoscopic Patterns of Dermatofibroma. Dermatol. Surg. 2005, 31, 1336–1339. [Google Scholar] [CrossRef]
- Karaarslan, I.K.; Gencoglan, G.; Akalin, T.; Ozdemir, F. Different dermoscopic faces of dermatofibromas. J. Am. Acad. Dermatol. 2007, 57, 401–406. [Google Scholar] [CrossRef]
- Agero, A.L.C.; Taliercio, S.; Dusza, S.W.; Salaro, C.; Chu, P.; Marghoob, A.A. Conventional and Polarized Dermoscopy Features of Dermatofibroma. Arch. Dermatol. 2006, 142, 1431–1437. [Google Scholar] [CrossRef]
- Han, T.Y.; Chang, H.S.; Lee, J.H.K.; Lee, W.-M.; Son, S.-J. A Clinical and Histopathological Study of 122 Cases of Dermatofibroma (Benign Fibrous Histiocytoma). Ann. Dermatol. 2011, 23, 185–192. [Google Scholar] [CrossRef]
- Zelger, B.G.; Sidoroff, A. Combined dermatofibroma: Co-existence of two or more variant patterns in a single lesion. Histopathology 2000, 36, 529–539. [Google Scholar] [CrossRef]
- Calonje, E.; Brenn, T.; Lazar, A.; Mckee, P. McKee’s Pathology of the Skin with Clinical Correlations, 4th ed.; Elsevier Saunders: Edinburgh, UK, 2012; pp. 1643–1662. [Google Scholar]
- Zeidi, M.; North, J.P. Sebaceous induction in dermatofibroma: A common feature of dermatofibromas on the shoulder. J. Cutan. Pathol. 2015, 42, 400–405. [Google Scholar] [CrossRef]
- Cazzato, G.; Colagrande, A.; Cimmino, A.; Marrone, M.; Stellacci, A.; Arezzo, F.; Lettini, T.; Resta, L.; Ingravallo, G. Granular Cell Dermatofibroma: When Morphology Still Matters. Dermatopathology 2021, 8, 371–375. [Google Scholar] [CrossRef] [PubMed]
- LeBoit, P.E.; Barr, R.J.; Burall, S.; Metcalf, J.S.; Yen, T.S.B.; Wick, M.R. Primitive Polypoid Granular-Cell Tumor and Other Cutaneous Granular-Cell Neoplasms of Apparent Nonneural Origin. Am. J. Surg. Pathol. 1991, 15, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Lee, W.J.; Jung, J.M.; Won, C.H.; Chang, S.E.; Choi, J.H.; Moon, K.C. Clinical and histological patterns of dermatofibroma without gross skin surface change: A comparative study with conventional dermatofibroma. Indian J. Dermatol. Venereol. Leprol. 2015, 81, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Victor, T.A. Neoplasms with Follicular Differentiation, 2nd ed.; Ackerman, B., Reddy, V.B., Soyer, H.P., Eds.; Blackwell Publishing Inc.: Hoboken, NJ, USA, 2002. [Google Scholar]
- Kaddu, S.; McMenamin, M.E.; Fletcher, C.D.M. Atypical Fibrous Histiocytoma of the Skin: Clinicopathologic analysis of 59 cases with evidence of infrequent metastasis. Am. J. Surg. Pathol. 2002, 26, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Tatu, A.L. Black Nodule on the Forearm. J. Cutan. Med. Surg. 2017, 21, 157. [Google Scholar] [CrossRef]
- Agarwal, A.; Gopinath, A.; Tetzlaff, M.T.; Prieto, V.G. Phosphohistone-H3 and Ki67: Useful Markers in Differentiating Dermatofibroma from Dermatofibrosarcoma Protuberans and Atypical Fibrohistiocytic Lesions. Am. J. Dermatopathol. 2017, 39, 504–507. [Google Scholar] [CrossRef]
- Trøstrup, H.; Bigdeli, A.K.; Krogerus, C.; Kneser, U.; Schmidt, G.; Schmidt, V.J. A Multidisciplinary Approach to Complex Dermal Sarcomas Ensures an Optimal Clinical Outcome. Cancers 2022, 14, 1693. [Google Scholar] [CrossRef]
- Volpicelli, E.R.; Fletcher, C.D.M. Desmin and CD34 positivity in cellular fibrous histiocytoma: An immunohistochemical analysis of 100 cases. J. Cutan. Pathol. 2012, 39, 747–752. [Google Scholar] [CrossRef]
- John, A.M.; Holahan, H.H.; Singh, P.; Handler, M.Z.; Lambert, W.C. When Immunohistochemistry Deceives Us: The Pitfalls of CD34 and Factor XIIIa Stains in Dermatofibroma and Dermatofibrosarcoma Protuberans. Skinmed 2017, 15, 53–55. [Google Scholar]
- Kim, H.J.; Lee, J.Y.; Kim, S.H.; Seo, Y.J.; Lee, J.H.; Park, J.K.; Kim, M.H.; Cinn, Y.W.; Cho, K.H.; Yoon, T.Y. Stromelysin-3 expression in the differential diagnosis of dermatofibroma and dermatofibrosarcoma protuberans: Comparison with factor XIIIa and CD34. Br. J. Dermatol. 2007, 157, 319–324. [Google Scholar] [CrossRef]
- Maekawa, T.; Jinnin, M.; Ihn, H. The expression levels of thrombospondin-1 in dermatofibroma and dermatofibrosarcoma protuberans. Eur. J. Dermatol. 2011, 21, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yu, Y.; Yang, Y.; Wang, L.; Cao, J.; Liang, X.; Xiao, X.; Tu, Y.; Chen, H. IGFBP7, a novel immunohistochemical marker in differentiating dermatofibroma from dermatofibrosarcoma protuberans. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.; Misago, N.; Yamamoto, O.; Toda, S.; Narisawa, Y. Expression of nestin in dermatofibrosarcoma protuberans in comparison to dermatofibroma. J. Dermatol. 2008, 35, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xiang, Y.N.; Zhang, Y.H.; Tu, Y.T.; Chen, H.X. Collagen triple helix repeat containing-1 in the differential diagnosis of dermatofibrosarcoma protuberans and dermatofibroma. Br. J. Dermatol. 2011, 164, 135–140. [Google Scholar] [CrossRef]
- Yan, X.; Takahara, M.; Xie, L.; Tu, Y.; Furue, M. Cathepsin K expression: A useful marker for the differential diagnosis of dermatofibroma and dermatofibrosarcoma protuberans. Histopathology 2010, 57, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Toyozawa, S.; Yamamoto, Y.; Ishida, Y.; Kondo, T.; Nakamura, Y.; Furukawa, F. Immunohistochemical Analysis of CXCR4 Expression in Fibrohistiocytic Tumors. Acta Histochem. Cytochem. 2010, 43, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Ishigami, T.; Hida, Y.; Matsudate, Y.; Murao, K.; Kubo, Y. The involvement of fibroblast growth factor receptor signaling pathways in dermatofibroma and dermatofibrosarcoma protuberans. J. Med. Investig. 2013, 60, 106–113. [Google Scholar] [CrossRef]
- Kazlouskaya, V.; Malhotra, S.; Kabigting, F.D.; Lal, K.; Elston, D.M. CD99 Expression in Dermatofibrosarcoma Protuberans and Dermatofibroma. Am. J. Dermatopathol. 2014, 36, 392–396. [Google Scholar] [CrossRef]
- West, K.L.; Cardona, D.M.; Su, Z.; Puri, P.K. Immunohistochemical Markers in Fibrohistiocytic Lesions: Factor XIIIa, CD34, S-100 and p75. Am. J. Dermatopathol. 2014, 36, 414–419. [Google Scholar] [CrossRef]
- Mikoshiba, Y.; Ogawa, E.; Uchiyama, R.; Uchiyama, A.; Uhara, H.; Okuyama, R. 5-Hydroxymethylcytosine is a useful marker to differentiate between dermatofibrosarcoma protuberans and dermatofibroma. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 130–131. [Google Scholar] [CrossRef]
- Karanian, M.; Pérot, G.; Coindre, J.-M.; Chibon, F.; Pedeutour, F.; Neuville, A. Fluorescence in situ hybridization analysis is a helpful test for the diagnosis of dermatofibrosarcoma protuberans. Mod. Pathol. 2015, 28, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Kaur, H.; Kaur, J.; Gill, K.S.; Mannan, R.; Arora, S. Subcutaneous Dermatofibroma: A Rare Case Report with Review of Literature. J. Clin. Diagn. Res. 2014, 8, FD01–FD02. [Google Scholar] [CrossRef] [PubMed]
- Motegi, S.-I.; Fujiwara, C.; Sekiguchi, A.; Yamazaki, S.; Yokoyama, Y.; Yasuda, M.; Ishikawa, O. Possible contribution of PDGF-BB-induced autophagy in dermatofibrosarcoma protuberans: Autophagy marker Atg5 could be a differential marker between dermatofibrosarcoma protuberans and dermatofibroma. J. Dermatol. Sci. 2019, 93, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Lyundup, A.V.; Balyasin, M.V.; Maksimova, N.V.; Kovina, M.V.; Krasheninnikov, M.E.; Dyuzheva, T.G.; Yakovenko, S.A.; Appolonova, S.A.; Schiöth, H.B.; Klabukov, I.D. Misdiagnosis of diabetic foot ulcer in patients with undiagnosed skin malignancies. Int. Wound J. 2022, 19, 871–887. [Google Scholar] [CrossRef] [PubMed]
- Giovannacci, I.; Meleti, M.; Garbarino, F.; Cesinaro, A.M.; Mataca, E.; Pedrazzi, G.; Reggiani, C.; Paganelli, A.; Truzzi, A.; Elia, F.; et al. Correlation between Autofluorescence Intensity and Histopathological Features in Non-Melanoma Skin Cancer: An Ex Vivo Study. Cancers 2021, 13, 3974. [Google Scholar] [CrossRef] [PubMed]
- Dessinioti, C.; Antoniou, C.; Stratigos, A.J. New targeted approaches for the treatment and prevention of nonmelanoma skin cancer. Expert Rev. Dermatol. 2011, 6, 625–634. [Google Scholar] [CrossRef]
- Drakaki, E.; Vergou, T.; Dessinioti, C.; Stratigos, A.J.; Salavastru, C.; Antoniou, C. Spectroscopic methods for the photodiagnosis of nonmelanoma skin cancer. J. Biomed. Opt. 2012, 18, 061221. [Google Scholar] [CrossRef]
- Seidenari, S.; Arginelli, F.; Bassoli, S.; Cautela, J.; French, P.M.W.; Guanti, M.; Guardoli, D.; König, K.; Talbot, C.; Dunsby, C. Multiphoton Laser Microscopy and Fluorescence Lifetime Imaging for the Evaluation of the Skin. Dermatol. Res. Pract. 2011, 2012, 810749. [Google Scholar] [CrossRef]
- Balaceanu, L.A. Biomarkers vs. imaging in the early detection of hepatocellular carcinoma and prognosis. World J. Clin. Cases 2019, 7, 1367–1382. [Google Scholar] [CrossRef]
- Czajkowska, J.; Juszczyk, J.; Piejko, L.; Glenc-Ambroży, M. High-Frequency Ultrasound Dataset for Deep Learning-Based Image Quality Assessment. Sensors 2022, 22, 1478. [Google Scholar] [CrossRef]
- Malciu, A.M.; Lupu, M.; Voiculescu, V.M. Artificial Intelligence-Based Approaches to Reflectance Confocal Microscopy Image Analysis in Dermatology. J. Clin. Med. 2022, 11, 429. [Google Scholar] [CrossRef] [PubMed]
- Maron, R.C.; Utikal, J.S.; Hekler, A.; Hauschild, A.; Sattler, E.; Sondermann, W.; Haferkamp, S.; Schilling, B.; Heppt, M.V.; Jansen, P.; et al. Artificial Intelligence and Its Effect on Dermatologists’ Accuracy in Dermoscopic Melanoma Image Classification: Web-Based Survey Study. J. Med. Internet Res. 2020, 22, e18091. [Google Scholar] [CrossRef]
- Tschandl, P.; Wiesner, T. Advances in the diagnosis of pigmented skin lesions. Br. J. Dermatol. 2018, 178, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Styła, M.; Giżewski, T. The Study of Usefulness of a Set of Fractal Parameters to Build Classes of Disease Units Based on Images of Pigmented Skin Lesions. Diagnostics 2021, 11, 1773. [Google Scholar] [CrossRef] [PubMed]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 5, 180161. [Google Scholar] [CrossRef]
- Felmingham, C.; MacNamara, S.; Cranwell, W.; Williams, N.; Wada, M.; Adler, N.R.; Ge, Z.; Sharfe, A.; Bowling, A.; Haskett, M.; et al. Improving Skin Cancer Management with Artificial Intelligence (SMARTI): Protocol for a preintervention/postintervention trial of an artificial intelligence system used as a diagnostic aid for skin cancer management in a specialist dermatology setting. BMJ Open 2022, 12, e050203. [Google Scholar] [CrossRef]
- Tschandl, P.; Rinner, C.; Apalla, Z.; Argenziano, G.; Codella, N.; Halpern, A.; Janda, M.; Lallas, A.; Longo, C.; Malvehy, J.; et al. Human–computer collaboration for skin cancer recognition. Nat. Med. 2020, 26, 1229–1234. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Nagendran, M.; Chen, Y.; Lovejoy, C.A.; Gordon, A.C.; Komorowski, M.; Harvey, H.; Topol, E.J.; Ioannidis, J.P.A.; Collins, G.S.; Maruthappu, M. Artificial intelligence versus clinicians: Systematic review of design, reporting standards, and claims of deep learning studies. BMJ 2020, 368, m689. [Google Scholar] [CrossRef]
- Ouellette, S.; Rao, B.K. Usefulness of Smartphones in Dermatology: A US-Based Review. Int. J. Environ. Res. Public Health 2022, 19, 3553. [Google Scholar] [CrossRef]
- Patrzyk, S.; Bielecki, W.; Woźniacka, A. A study of attitudes among Polish dermatologists and dermatology trainees regarding modern technologies in medicine. Adv. Dermatol. Allergol. 2022, 39, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Breslavets, M.; Shear, N.H.; Lapa, T.; Breslavets, D.; Breslavets, A. Validation of artificial intelligence application in clinical dermatology. J. Am. Acad. Dermatol. 2022, 86, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Koh, U.; Horsham, C.; Soyer, H.P.; Loescher, L.J.; Gillespie, N.; Vagenas, D.; Janda, M. Consumer Acceptance and Expectations of a Mobile Health Application to Photograph Skin Lesions for Early Detection of Melanoma. Dermatology 2019, 235, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Fluhr, J.W.; Gueguen, A.; Legoupil, D.; Brenaut, E.; Abasq, C.; Araújo, H.; Misery, L. Teledermatology in Times of COVID-19 Confinement: Comparing Patients’ and Physicians’ Satisfaction by the Standardized Brest Teledermatology Questionnaire. Dermatology 2021, 237, 191–196. [Google Scholar] [CrossRef]
- Asabor, E.N.; Bunick, C.G.; Cohen, J.M.; Perkins, S.H. Patient and physician perspectives on teledermatology at an academic dermatology department amid the COVID-19 pandemic. J. Am. Acad. Dermatol. 2021, 84, 158–161. [Google Scholar] [CrossRef]
- Fijałkowska, M.; Koziej, M.; Żądzińska, E.; Antoszewski, B.; Sitek, A. Assessment of the Predictive Value of Spectrophotometric Skin Color Parameters and Environmental and Behavioral Factors in Estimating the Risk of Skin Cancer: A Case–Control Study. J. Clin. Med. 2022, 11, 2969. [Google Scholar] [CrossRef]
- Hauser, K.; Kurz, A.; Haggenmüller, S.; Maron, R.C.; von Kalle, C.; Utikal, J.S.; Meier, F.; Hobelsberger, S.; Gellrich, F.F.; Sergon, M.; et al. Explainable artificial intelligence in skin cancer recognition: A systematic review. Eur. J. Cancer 2022, 167, 54–69. [Google Scholar] [CrossRef]
- Liopyris, K.; Gregoriou, S.; Dias, J.; Stratigos, A.J. Artificial Intelligence in Dermatology: Challenges and Perspectives. Dermatol. Ther. 2022, 12, 2637–2651. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Authors | Article Type | Year of Publication | Atypical Features with High Risk | Cases (n/%) |
|---|---|---|---|---|
| Aytekin S et al. [1] | Original article | 2021 | Irregular delicate/asymmetric pigment network Peripheral proeminent pigment network Irregular proeminent pigment network Atypical pigment network Irregular white network Irregular brown areas Dotted vessels Glomerular vessels Polymorphous/atypical vessels Ulceration White radial streaks | 31 (21.8) 3 (2.1) 2 (1.4) 2 (1.4) 3 (2.1) 9 (6.3) 34 (23.9) 2 (1.4) 6 (4.2) 5 (3.5) 8 (5.6) |
| Genc Y et al. [75] | Report | 2020 | Melanoma-like BCC-like Keratoachantoma-like Spitzoid-like | 11 (19.4) 3 (4.9) 2 (2.6) 26 (19.4) |
| Llambrich A et al. [3] | Research letter | 2019 | Dotted vessels Arborizing vessels Polymorphous/atypical vessels Shiny white streaks | 18 (50) 7 (19.4) 18 (50) 16 (44.4) |
| Lin MJ et al. [76] | Original research | 2018 | Dotted/pinpoint vessels Sharply focused arborizing vessels Linear irregular vessels Glomerular vessels Polymorphous vascular pattern White lines Ulceration Blue/grey veil | 2 (22) 0 1 (11) 1 (11) 1 (11) 0 0 0 |
| Won KY et al. [77] | Original research | 2017 | Irregular shape Spiculated margins | 8 (44) 12 (67) |
| Kelati A et al. [78] | Research article | 2017 | White streaks Ulceration Brown streks Negative-network-like appearance Dotted vessels Multicomponent melanoma-like Vascular tumor-like BCC-like Collision tumor-like Peripheral diffuse pink to red to reddish violet halo White ring around an ulceration Pink bluish pigmentation with vascularization Pigment network with a ring around follicular opening | 18 (18) 6 (6) 6 (6) 3 (3) 23.3% 20 (20%) 0 0 0 7 (7%) 6 (6%) 7 (7%) 2 (2%) |
| Marinescu SA et al. [71] | Case report | 2016 | Pinky-milk areas Peripheral pigment network Polymorphous atypical vessels | |
| Roldán-Marín R et al. [79] | Case report | 2014 | Grey-green colour | |
| Ferrari A et al. [9] | Original article | 2013 | Melanoma-like Vascular tumour-like BCC-like Collision tumour-like | 21 (16.2) 6 (4.6) 5 (3.8) 3 (2.3) |
| Zaballos et al. [8] | Prospective study | 2008 | Proeminent atypical pigment network Irregular pigment network Irregular white network Irregular brown areas Dotted vessels Glomerular vessels Polymorphous/atypical vessels Ulceration | 13 (3.1) 8 (1.9) 3 (0.7) 125 (30.6) 3 (0.7) 10 (2.4) 18 (4.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orzan, O.A.; Dorobanțu, A.M.; Gurău, C.D.; Ali, S.; Mihai, M.M.; Popa, L.G.; Giurcăneanu, C.; Tudose, I.; Bălăceanu, B. Challenging Patterns of Atypical Dermatofibromas and Promising Diagnostic Tools for Differential Diagnosis of Malignant Lesions. Diagnostics 2023, 13, 671. https://doi.org/10.3390/diagnostics13040671
Orzan OA, Dorobanțu AM, Gurău CD, Ali S, Mihai MM, Popa LG, Giurcăneanu C, Tudose I, Bălăceanu B. Challenging Patterns of Atypical Dermatofibromas and Promising Diagnostic Tools for Differential Diagnosis of Malignant Lesions. Diagnostics. 2023; 13(4):671. https://doi.org/10.3390/diagnostics13040671
Chicago/Turabian StyleOrzan, Olguța Anca, Alexandra Maria Dorobanțu, Cristian Dorin Gurău, Sibel Ali, Mara Mădălina Mihai, Liliana Gabriela Popa, Călin Giurcăneanu, Irina Tudose, and Beatrice Bălăceanu. 2023. "Challenging Patterns of Atypical Dermatofibromas and Promising Diagnostic Tools for Differential Diagnosis of Malignant Lesions" Diagnostics 13, no. 4: 671. https://doi.org/10.3390/diagnostics13040671