

Machine Learning System for Lung Neoplasms Distinguished Based on Scleral Data
Abstract
:1. Introduction
2. Materials and Methods
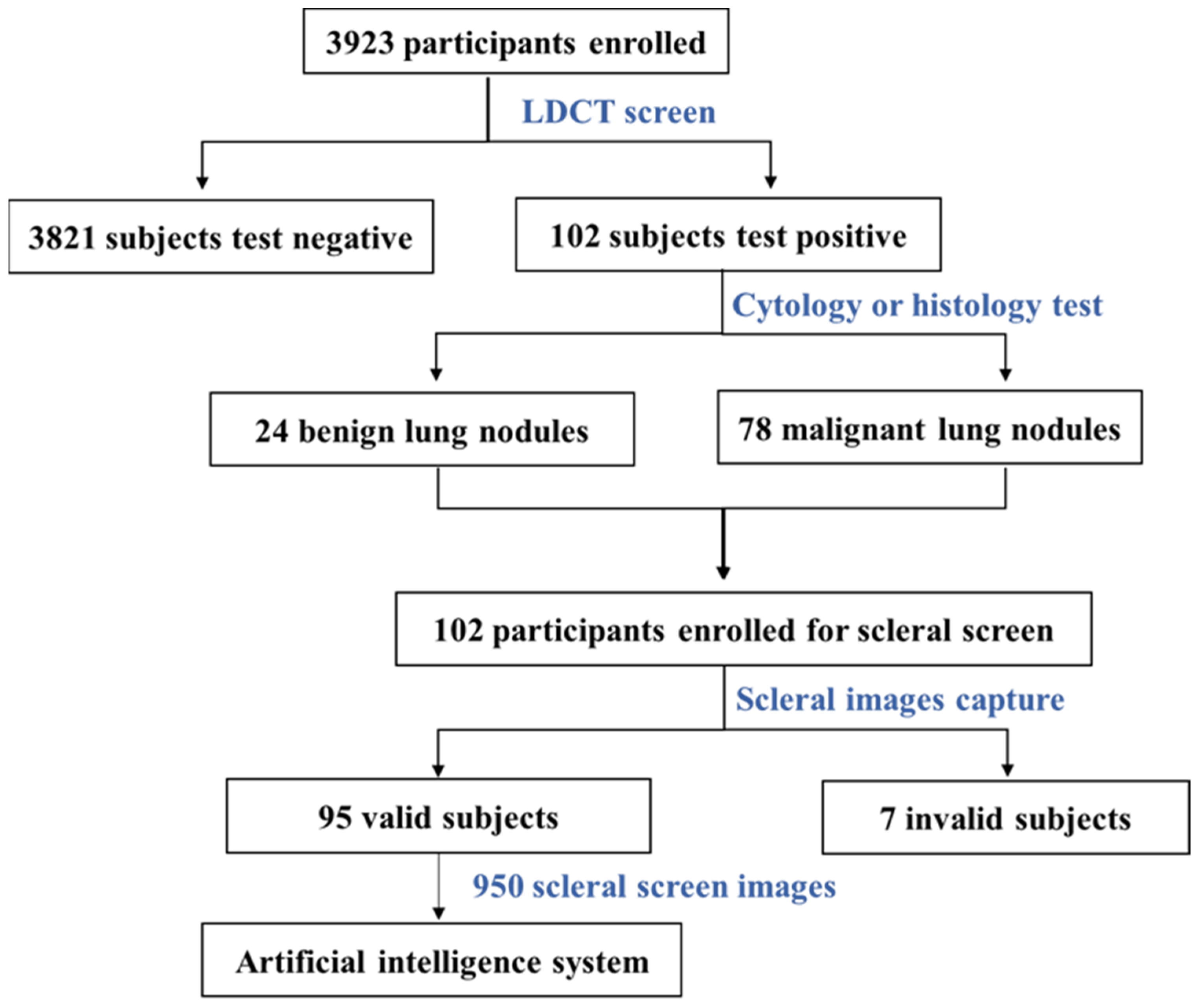
2.1. Participants
2.2. Screening Strategy
2.3. Scleral Imaging Method and Instrument
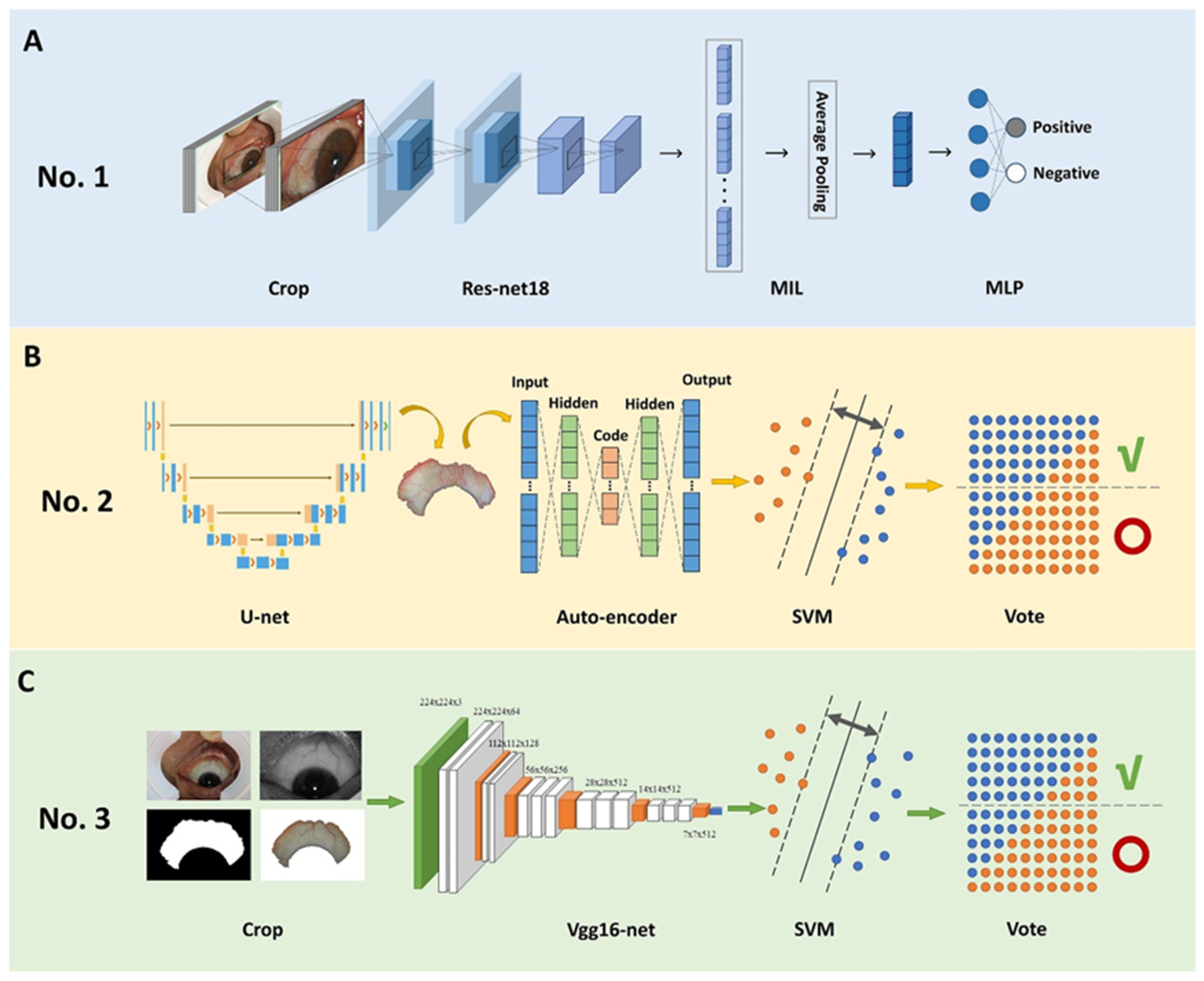
2.4. Development of AI Models
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Subjects Enrolled in AI Analysis
3.2. Modeling of AI Models
3.3. Performance of the Top Three AI Models
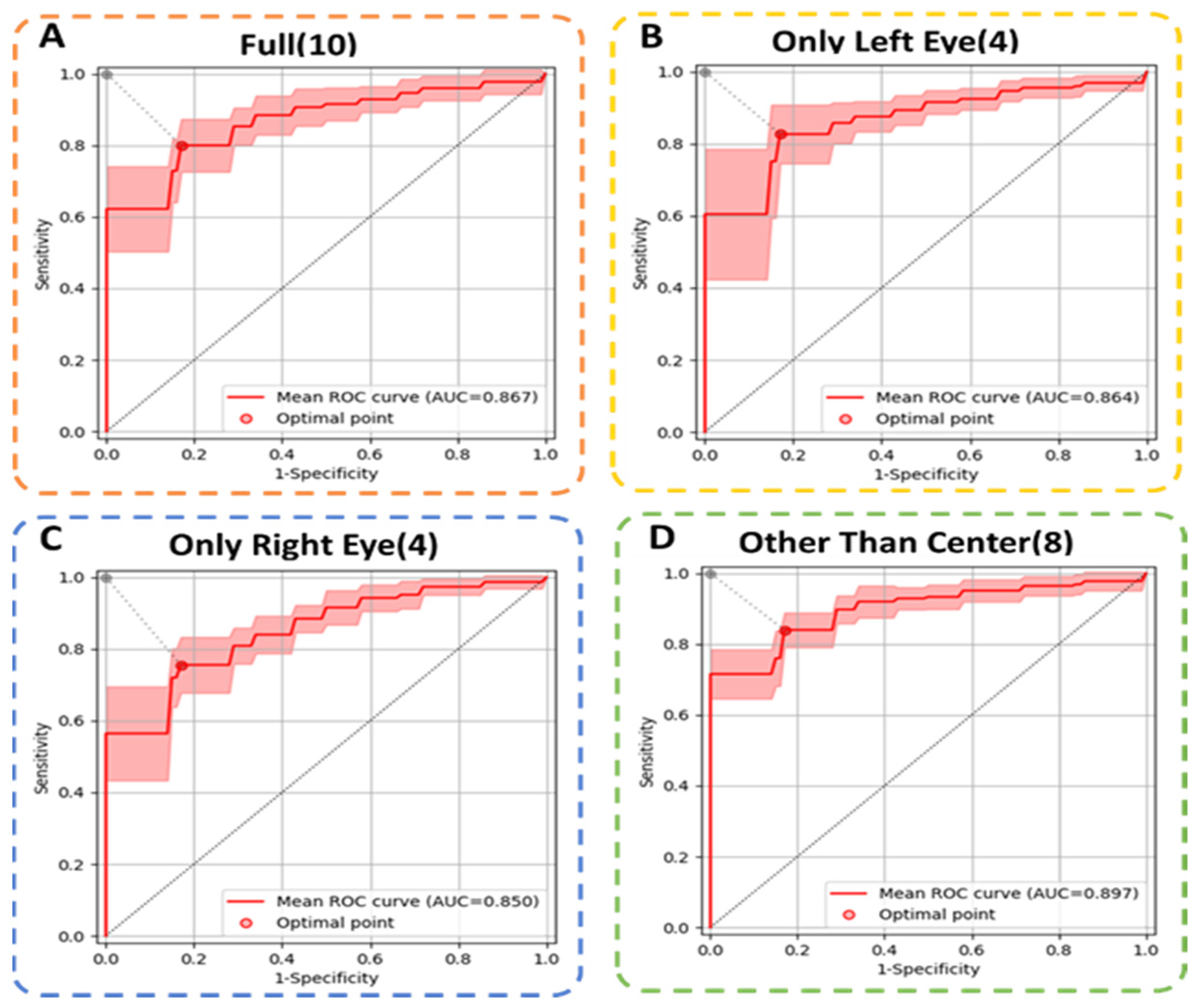
3.4. Comparison of Different Scleral Image Input Strategies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar]
- National Cancer Registration and Analysis Service, Public Health England (PHE). Cancer Survival in England for Patients Diagnosed between 2014 and 2018, and Followed up to 2019. C2022. Available online: https://www.gov.uk/government/statistics (accessed on 2 December 2022).
- Leon, M.E.; Peruga, A.; Neill, A.M.; Kralikova, E.; Guha, N.; Minozzi, S.; Espina, C.; Schuz, J. European Code against Cancer, 4th Edition: Tobacco and Cancer. Cancer Epidemiol. 2015, 39 (Suppl. S1), S20–S33. [Google Scholar]
- Oncology Committee of Chinese Medical Association, National Medical Journal of China. Guidelines for the clinical diagnosis and treatment of lung cancer from the Chinese Medical Association (2022). Natl. Med. J. China 2022, 102, 1706–1740. [Google Scholar]
- US Preventive Services Task Force; Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; et al. Screening for Lung Cancer: Us Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 962–970. [Google Scholar]
- Veronesi, G.; Baldwin, D.R.; Henschke, C.I.; Ghislandi, S.; Iavicoli, S.; Oudkerk, M.; De Koning, H.J.; Shemesh, J.; Field, J.K.; Zulueta, J.J.; et al. Recommendations for Implementing Lung Cancer Screening with Low-Dose Computed Tomography in Europe. Cancers 2020, 12, 1672. [Google Scholar]
- Tammemägi, M.C.; Church, T.R.; Hocking, W.G.; Silvestri, G.A.; Kvale, P.A.; Riley, T.L.; Commins, J.; Berg, C.D. Evaluation of the Lung Cancer Risks at Which to Screen Ever- and Never-Smokers: Screening Rules Applied to the Plco and Nlst Cohorts. PLoS Med. 2014, 11, e1001764. [Google Scholar] [CrossRef]
- Thun, M.J.; Hannan, L.M.; Adams-Campbell, L.L.; Boffetta, P.; Buring, J.E.; Feskanich, D.; Flanders, W.D.; Jee, S.H.; Katanoda, K.; Kolonel, L.N.; et al. Lung Cancer Occurrence in Never-Smokers: An Analysis of 13 Cohorts and 22 Cancer Registry Studies. PLoS Med. 2008, 5, e185. [Google Scholar] [CrossRef]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar]
- Tammemägi, M.C.; Katki, H.A.; Hocking, W.G.; Church, T.R.; Caporaso, N.; Kvale, P.A.; Chaturvedi, A.K.; Silvestri, G.A.; Riley, T.L.; Commins, J.; et al. Selection Criteria for Lung-Cancer Screening. N. Engl. J. Med. 2013, 368, 728–736. [Google Scholar]
- Wilson, D.O.; Weissfeld, J. A Simple Model for Predicting Lung Cancer Occurrence in a Lung Cancer Screening Program: The Pittsburgh Predictor. Lung Cancer 2015, 89, 31–37. [Google Scholar]
- Muller, D.C.; Johansson, M.; Brennan, P. Lung Cancer Risk Prediction Model Incorporating Lung Function: Development and Validation in the Uk Biobank Prospective Cohort Study. J. Clin. Oncol. 2017, 35, 861–869. [Google Scholar]
- Oudkerk, M.; Liu, S.Y.; Heuvelmans, M.A.; Walter, J.E.; Field, J.K. Lung Cancer Ldct Screening and Mortality Reduction-Evidence, Pitfalls and Future Perspectives. Nat. Rev. Clin. Oncol. 2021, 18, 135–151. [Google Scholar]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International Evaluation of an Ai System for Breast Cancer Screening. Nature 2020, 586, E19. [Google Scholar] [CrossRef]
- Lehman, C.D.; Wellman, R.D.; Buist, D.S.; Kerlikowske, K.; Tosteson, A.N.; Miglioretti, D.L.; Breast Cancer Surveillance Consortium. Diagnostic Accuracy of Digital Screening Mammography with and without Computer-Aided Detection. JAMA Intern. Med. 2015, 175, 1828–1837. [Google Scholar]
- Wan, Y.-L.; Wu, P.W.; Huang, P.-C.; Tsay, P.-K.; Pan, K.-T.; Trang, N.N.; Chuang, W.-Y.; Wu, C.-Y.; Lo, S.B. The Use of Artificial Intelligence in the Differentiation of Malignant and Benign Lung Nodules on Computed Tomograms Proven by Surgical Pathology. Cancers 2020, 12, 2211. [Google Scholar]
- Espinoza, J.L.; Dong, L.T. Artificial Intelligence Tools for Refining Lung Cancer Screening. J. Clin. Med. 2020, 9, 3860. [Google Scholar]
- Chang, Y.-J.; Hung, K.-C.; Wang, L.-K.; Yu, C.-H.; Chen, C.-K.; Tay, H.-T.; Wang, J.-J.; Liu, C.-F. A Real-Time Artificial Intelligence-Assisted System to Predict Weaning from Ventilator Immediately after Lung Resection Surgery. Int. J. Environ. Res. Public Health 2021, 18, 2713. [Google Scholar] [CrossRef]
- Ardila, D.; Kiraly, A.P.; Bharadwaj, S.; Choi, B.; Reicher, J.J.; Peng, L.; Tse, D.; Etemadi, M.; Ye, W.; Corrado, G.; et al. End-to-End Lung Cancer Screening with Three-Dimensional Deep Learning on Low-Dose Chest Computed Tomography. Nat. Med. 2019, 25, 954–961. [Google Scholar]
- Szabó, I.V.; Simon, J.; Nardocci, C.; Kardos, A.S.; Nagy, N.; Abdelrahman, R.-H.; Zsarnóczay, E.; Fejér, B.; Futácsi, B.; Müller, V.; et al. The Predictive Role of Artificial Intelligence-Based Chest CT Quantification in Patients with COVID-19 Pneumonia. Tomography 2021, 7, 697–710. [Google Scholar] [CrossRef]
- Lu, M.T.; Raghu, V.K.; Mayrhofer, T.; Aerts, H.; Hoffmann, U. Deep Learning Using Chest Radiographs to Identify High-Risk Smokers for Lung Cancer Screening Computed Tomography: Development and Validation of a Prediction Model. Ann. Intern. Med. 2020, 173, 704–713. [Google Scholar]
- Gould, M.K.; Huang, B.Z.; Tammemagi, M.C.; Kinar, Y.; Shiff, R. Machine Learning for Early Lung Cancer Identification Using Routine Clinical and Laboratory Data. Am. J. Respir. Crit. Care Med. 2021, 204, 445–453. [Google Scholar]
- Eijnatten, M.; Rundo, L.; Batenburg, K.J.; Lucka, F.; Beddowes, E.; Caldas, C.; Gallagher, F.A.; Sala, E.; Schönlieb, C.B.; Woitek, R. 3d Deformable Registration of Longitudinal Abdominopelvic Ct Images Using Unsupervised Deep Learning. Comput. Methods Programs Biomed. 2021, 208, 106261. [Google Scholar] [CrossRef]
- Ma, L.; Zhang, D.; Li, N.M.; Cai, Y.; Zuo, W.M.; Wang, K.G. Iris-Based Medical Analysis by Geometric Deformation Features. IEEE J. Biomed. Health Inf. 2013, 17, 223–231. [Google Scholar]
- Boote, C.; Sigal, I.A.; Grytz, R.; Hua, Y.; Nguyen, T.D.; Girard, M. Scleral Structure and Biomechanics. Prog. Retin. Eye Res. 2020, 74, 100773. [Google Scholar]
- Judah, F. Angiogenesis: An Organizing Principle for Drug Discovery? Nat. Rev. Drug Discov. 2007, 6, 273–286. [Google Scholar]
- Countee, R.W.; Gnanadev, A.; Chavis, P. Dilated Episcleral Arteries-a Significant Physical Finding in Assessment of Patients with Cerebrovascular Insufficiency. Stroke 1978, 9, 42–45. [Google Scholar]
- Murphy, P.J.; Lau, J.; Sim, M.; Woods, R.L. How Red Is a White Eye? Clinical Grading of Normal Conjunctival Hyperaemia. Eye 2007, 21, 633–638. [Google Scholar]
- Hussain, T.; Haider, A.; Muhammad, A.M.; Agha, A.; Khan, B.; Rashid, F.; Raza, M.S.; Din, M.; Khan, M.; Ullah, S.; et al. An Iris Based Lungs Pre-Diagnostic System. In Proceedings of the 2019 2nd International Conference on Computing, Mathematics and Engineering Technologies (iCoMET), Sukkur, Pakistan, 30–31 January 2019; pp. 1–5. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Benign Group | Malignant Group |
|---|---|---|
| Age | 50.6 | 61.9 |
| Gender | ||
| Female | 10 (30.3%) | 23 (68.7%) |
| Male | 10 (16.1%) | 52 (83.9%) |
| Tumor type | ||
| Lung squamous cell carcinoma (LUSC) | 28 (37.3%) | |
| Lung metastasis | 17 (22.7%) | |
| Lung adenocarcinoma (LUAD) | 15 (20.0%) | |
| Mixed/unspecified NSCLC | 9 (12.0%) | |
| Small Cell Lung Cancer (SCLC) | 6 (8.0%) |
| Models 1 | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| No. 1 | 0.811 | 0.813 | 0.800 |
| No. 2 | 0.779 | 0.827 | 0.600 |
| No. 3 | 0.768 | 0.827 | 0.550 |
| Input Images 2 | Accuracy | Sensitivity | Specificity | Average AUC |
|---|---|---|---|---|
| Full (10) | 0.818 ± 0.043 | 0.818 ± 0.044 | 0.817 ± 0.090 | 0.867 ± 0.058 |
| Only Left Eye (4) | 0.835 ± 0.044 | 0.849 ± 0.054 | 0.786 ± 0.084 | 0.864 ± 0.063 |
| Only Right Eye (4) | 0.779 ± 0.055 | 0.778 ± 0.061 | 0.783 ± 0.051 | 0.850 ± 0.055 |
| Other Than Center (8) | 0.835 ± 0.031 | 0.836 ± 0.048 | 0.828 ± 0.095 | 0.897 ± 0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Q.; Lv, W.; Zhou, Z.; Tan, S.; Lin, X.; Bo, Z.; Fu, R.; Jin, X.; Guo, Y.; Wang, H.; et al. Machine Learning System for Lung Neoplasms Distinguished Based on Scleral Data. Diagnostics 2023, 13, 648. https://doi.org/10.3390/diagnostics13040648
Huang Q, Lv W, Zhou Z, Tan S, Lin X, Bo Z, Fu R, Jin X, Guo Y, Wang H, et al. Machine Learning System for Lung Neoplasms Distinguished Based on Scleral Data. Diagnostics. 2023; 13(4):648. https://doi.org/10.3390/diagnostics13040648
Chicago/Turabian StyleHuang, Qin, Wenqi Lv, Zhanping Zhou, Shuting Tan, Xue Lin, Zihao Bo, Rongxin Fu, Xiangyu Jin, Yuchen Guo, Hongwu Wang, and et al. 2023. "Machine Learning System for Lung Neoplasms Distinguished Based on Scleral Data" Diagnostics 13, no. 4: 648. https://doi.org/10.3390/diagnostics13040648