
Carotid Plaque Vulnerability Diagnosis by CTA versus MRA: A Systematic Review
 , , ,
, , ,
Abstract
:1. Introduction
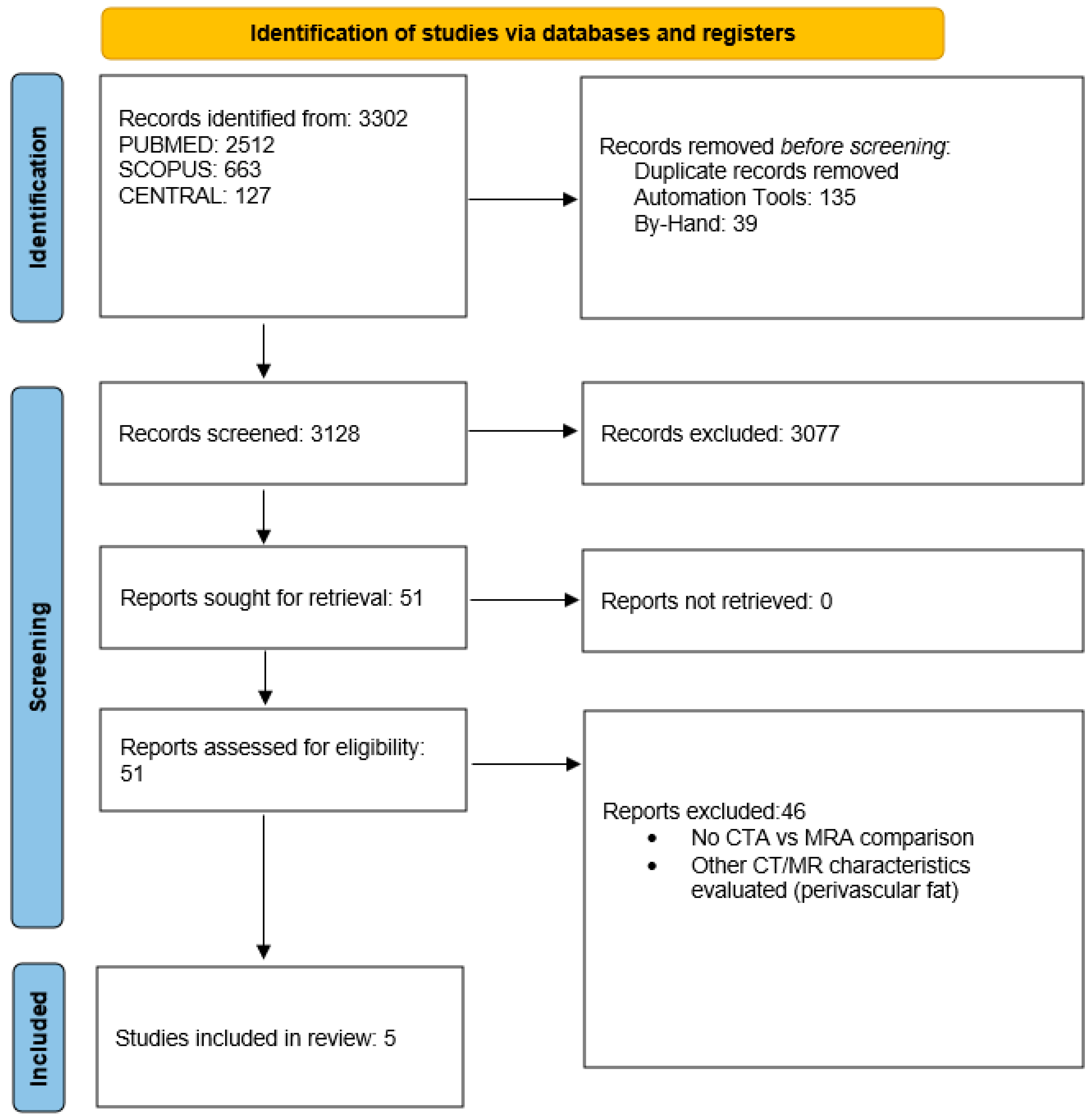
2. Methods
2.1. Review Protocol
2.2. Search Strategy
2.3. Data Extraction
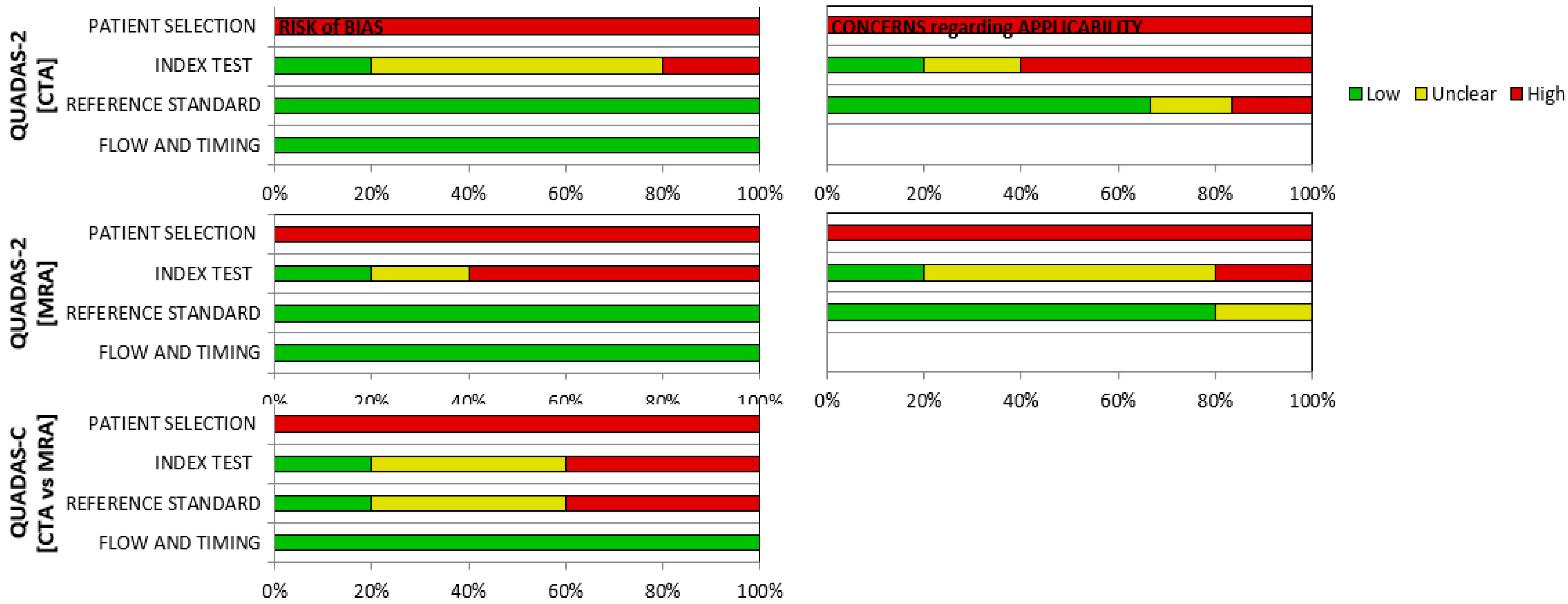
2.4. Quality Assessment
2.5. Definitions
2.6. Statistical Analysis
3. Results
3.1. Carotid Plaque Vulnerability Characteristics
3.2. Risk of Bias
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Flaherty, M.L.; Kissela, B.; Khoury, J.C.; Alwell, K.; Moomaw, C.J.; Woo, D.; Pooja, K.; Ferioli, S.; Adeoye, O.; Broderick, J.P.; et al. Carotid artery stenosis are a cause of stroke. Neuroepidemiology 2013, 40, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Abbott, A.L.; Paraskevas, K.I.; Kakkos, S.K.; Golledge, J.; Eckstein, H.-H.; Diaz-Sandoval, L.J.; Cao, L.; Fu, Q.; Wijeratne, T.; Leung, T.W.; et al. Systematic Review of Guidelines for the Management of Asymptomatic and Symptomatic Carotid Stenosis. Stroke 2015, 46, 3288–3301. [Google Scholar] [CrossRef] [PubMed]
- Hadar, N.; Raman, G.; Moorthy, D.; O’Donnell, T.F.; Thaler, D.E.; Feldmann, E.; Lau, J.; Kitsios, G.D.; Dahabreh, I.J. Asymptomatic carotid artery stenosis treated with medical therapy alone: Temporal trends and implications for risk assessment and the design of future studies. Cerebrovasc. Dis. 2014, 38, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, A.N.; Kakkos, S.K.; Kyriacou, E.; Griffin, M.; Sabetai, M.; Thomas, D.J.; Tegos, T.; Geroulakos, G.; Labropoulos, N.; Doré, C.J.; et al. Asymptomatic internal carotid artery stenosis and cerebrovascular risk stratification. J. Vasc. Surg. 2010, 52, 1486–1496.e5. [Google Scholar] [CrossRef]
- Cicha, I.; Wörner, A.; Urschel, K.; Beronov, K.; Goppelt-Struebe, M.; Veorheven, E.; Daniel, W.G.; Garlichs, C.D. Carotid plaque vulnerability: A positive feedback between hemodynamic and biochemical mechanisms. Stroke 2011, 42, 3502–3510. [Google Scholar] [CrossRef]
- Kopczak, A.; Schindler, A.; Bayer-Karpinska, A.; Koch, M.L.; Sepp, D.; Zeller, J.; Strecker, C.; Hempel, J.-M.; Yuan, C.; Malik, R.; et al. Complicated Carotid Artery Plaques as a Cause of Cryptogenic Stroke. J. Am. Coll. Cardiol. 2020, 76, 2212–2222. [Google Scholar] [CrossRef]
- Porambo, M.E.; DeMarco, J.K. MR imaging of vulnerable carotid plaque. Cardiovasc. Diagn. Ther. 2020, 10, 1019–1031. [Google Scholar] [CrossRef]
- Gupta, A.; Baradaran, H.; Mtui, E.E.; Kamel, H.; Pandya, A.; Giambrone, A.; Iadecola, C.; Sanelli, P.C. Detection of Symptomatic Carotid Plaque Using Source Data from MR and CT Angiography: A Correlative Study. Cerebrovasc. Dis. 2015, 39, 151–161. [Google Scholar] [CrossRef]
- U-King-Im, J.; Fox, A.J.; Aviv, R.I.; Howard, P.; Yeung, R.; Moody, A.R.; Symons, S.P. Characterization of carotid plaque hemorrhage: A CT angiography and MR intraplaque hemorrhage study. Stroke 2010, 41, 1623–1629. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Barnett, H.J.; Taylor, D.W.; Eliasziw, M.; Fox, A.J.; Ferguson, G.G.; Haynes, R.B.; Rankin, R.N.; Clagett, G.P.; Hachinski, V.C.; Sackett, D.L.; et al. Benefit of Carotid Endarterectomy in Patients with Symptomatic Moderate or Severe Stenosis. N. Engl. J. Med. 1998, 339, 1415–1425. [Google Scholar] [CrossRef]
- Stary, H.C. Natural history and histological classification of atherosclerotic lesions: An update. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1177–1178. [Google Scholar] [CrossRef]
- Anzidei, M.; Napoli, A.; Geiger, D.; Marincola, B.C.; Zini, C.; Zaccagna, F.; Di Paolo, P.L.; Catalano, C.; Passariello, R. Preliminary experience with MRA in evaluating the degree of carotid stenosis and plaque morphology using high-resolution sequences after gadofosveset trisodium (Vasovist) administration: Comparison with CTA and DSA. La Radiol. Med. 2010, 115, 634–647. [Google Scholar] [CrossRef]
- Trelles, M.; Eberhardt, K.; Buchholz, M.; Schindler, A.; Bayer-Karpinska, A.; Dichgans, M.; Reiser, M.; Nikolaou, K.; Saam, T. CTA for Screening of Complicated Atherosclerotic Carotid Plaque—American Heart Association Type VI Lesions as Defined by MRI. Am. J. Neuroradiol. 2013, 34, 2331–2337. [Google Scholar] [CrossRef]
- Eisenmenger, L.B.; Aldred, B.W.; Kim, S.E.; Stoddard, G.J.; de Havenon, A.; Treiman, G.S.; Parker, D.L.; McNally, J.S. Prediction of Carotid Intraplaque Hemorrhage Using Adventitial Calcification and Plaque Thickness on CTA. Am. J. Neuroradiol. 2016, 37, 1496–1503. [Google Scholar] [CrossRef]
- Josephson, S.A.; Bryant, S.O.; Mak, H.K.; Johnston, S.C.; Dillon, W.P.; Smith, W.S. Evaluation of carotid stenosis using CT angiography in the initial evaluation of stroke and TIA. Neurology 2004, 63, 457–460. [Google Scholar] [CrossRef]
- Adlova, R.; Adla, T. Multimodality Imaging of Carotid Stenosis. Int. J. Angiol. 2015, 24, 179–184. [Google Scholar] [CrossRef]
- Gupta, A.; Baradaran, H.; Schweitzer, A.D.; Kamel, H.; Pandya, A.; Delgado, D.; Dunning, A.; Mushlin, A.I.; Sanelli, P.C. Carotid plaque MRI and stroke risk: A systematic review and meta-analysis. Stroke 2013, 4, 3071–3077. [Google Scholar] [CrossRef]
- Nighoghossian, N.; Derex, L.; Douek, P. The vulnerable carotid artery plaque: Current imaging methods and new perspectives. Stroke 2005, 36, 2764–2772. [Google Scholar] [CrossRef] [PubMed]
- Mura, M.; Della Schiava, N.; Long, A.; Chirico, E.N.; Pialoux, V.; Millon, A. Carotid intraplaque haemorrhage: Pathogenesis, histological classification, imaging methods and clinical value. Ann. Transl. Med. 2020, 8, 1273. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.M.; Hatsukami, T.S.; Ferguson, M.S.; Small, R.; Polissar, N.L.; Yuan, C. Classification of Human Carotid Atherosclerotic Lesions with In Vivo Multicontrast Magnetic Resonance Imaging. Circulation 2002, 106, 1368–1373. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Mitsumori, L.M.; Ferguson, M.S.; Polissar, N.L.; Echelard, D.; Ortiz, G.; Small, R.; Davies, J.W.; Kerwin, W.S.; Hatsukami, T.S. In Vivo Accuracy of Multispectral Magnetic Resonance Imaging for Identifying Lipid-Rich Necrotic Cores and Intraplaque Hemorrhage in Advanced Human Carotid Plaques. Circulation 2001, 104, 2051–2056. [Google Scholar] [CrossRef] [PubMed]
- Takaya, N.; Yuan, C.; Chu, B.; Saam, T.; Polissar, N.L.; Jarvik, G.P.; Isaac, C.; McDonough, J.; Natiello, C.; Small, R.; et al. Presence of intraplaque hemorrhage stimulates progression of carotid atherosclerotic plaques: A high-resolution magnetic resonance imaging study. Circulation 2005, 111, 2768–2775. [Google Scholar] [CrossRef]
- Saba, L.; Francone, M.; Bassareo, P.; Lai, L.; Sanfilippo, R.; Montisci, R.; Suri, J.; De Cecco, C.; Faa, G. CT Attenuation Analysis of Carotid Intraplaque Hemorrhage. Am. J. Neuroradiol. 2017, 39, 131–137. [Google Scholar] [CrossRef]
- Xia, J.; Yin, A.; Li, Z.; Liu, X.; Peng, X.; Xie, N. Quantitative Analysis of Lipid-Rich Necrotic Core in Carotid Atherosclerotic Plaques by In Vivo Magnetic Resonance Imaging and Clinical Outcomes. Experiment 2017, 23, 2745–2750. [Google Scholar] [CrossRef]
- Biasi, G.M.; Froio, A.; Diethrich, E.B.; Deleo, G.; Galimberti, S.; Mingazzini, P.; Nicolaides, A.N.; Griffin, M.; Raithel, D.; Reid, D.B.; et al. Carotid plaque echolucency increases the risk of stroke in carotid stenting: The Imaging in Carotid Angioplasty and Risk of Stroke (ICAROS) study. Circulation 2004, 110, 756–762. [Google Scholar] [CrossRef]
- Chai, J.T.; Biasolli, L.; Li, L.; Alkhalil, M.; Galassi, F.; Darby, C.; Halliday, A.W.; Hands, L.; Magee, T.; Perkins, J.; et al. Quantification of Lipid-Rich Core in Carotid Atherosclerosis Using Magnetic Resonance T2 Mapping: Relation to Clinical Presentation. JACC Cardiovasc. Imaging 2017, 10, 747–756. [Google Scholar] [CrossRef]
- Wintermark, M.; Jawadi, S.; Rapp, J.; Tihan, T.; Tong, E.; Glidden, D.; Abedin, S.; Schaeffer, S.; Acevedo-Bolton, G.; Boudignon, B.; et al. High-Resolution CT Imaging of Carotid Artery Atherosclerotic Plaques. Am. J. Neuroradiol. 2008, 29, 875–882. [Google Scholar] [CrossRef] [Green Version]
- Rafailidis, V.; Chryssogonidis, I.; Tegos, T.; Kouskouras, K.; Charitanti-Kouridou, A. Imaging of the ulcerated carotid atherosclerotic plaque: A review of the literature. Insights Imaging 2017, 8, 213–225. [Google Scholar] [CrossRef]
- Etesami, M.; Hoi, Y.; Steinman, D.; Gujar, S.; Nidecker, A.; Astor, B.; Portanova, A.; Qiao, Y.; Abdalla, W.; Wasserman, B. Comparison of Carotid Plaque Ulcer Detection Using Contrast-Enhanced and Time-of-Flight MRA Techniques. Am. J. Neuroradiol. 2012, 34, 177–184. [Google Scholar] [CrossRef]
- Homburg, P.J.; Rozie, S.; van Gils, M.J.; Bouwhuijsen, Q.J.V.D.; Niessen, W.J.; Dippel, D.W.; van der Lugt, A. Association Between Carotid Artery Plaque Ulceration and Plaque Composition Evaluated with Multidetector CT Angiography. Stroke 2011, 42, 367–372. [Google Scholar] [CrossRef]
- Korn, A.; Bender, B.; Thomas, C.; Danz, S.; Fenchel, M.; Nägele, T.; Heuschmid, M.; Ernemann, U.; Hauser, T. Dual energy CTA of the carotid bifurcation: Advantage of plaque subtraction for assessment of grade of the stenosis and morphology. Eur. J. Radiol. 2011, 80, e120–e125. [Google Scholar] [CrossRef]
- Baradaran, H.; Gupta, A. Carotid Vessel Wall Imaging on CTA. Am. J. Neuroradiol. 2020, 41, 380–386. [Google Scholar] [CrossRef]
- Hatsukami, T.S.; Ross, R.; Polissar, N.L.; Yuan, C. Visualization of Fibrous Cap Thickness and Rupture in Human Atherosclerotic Carotid Plaque In Vivo with High-Resolution Magnetic Resonance Imaging. Circulation 2000, 102, 959–964. [Google Scholar] [CrossRef]
- Redgrave, J.; Gallagher, P.; Lovett, J.K.; Rothwell, P.M. Critical cap thickness and rupture in symptomatic carotid plaques: The oxford plaque study. Stroke 2008, 39, 1722–1729. [Google Scholar] [CrossRef]
- Skinner, M.P.; Yuan, C.; Mitsumori, L.; Hayes, C.E.; Raines, M.P.S.E.W.; Nelson, J.A.; Ross, R. Serial magnetic resonance imaging of experimental atherosclerosis detects lesion fine structure, progression and complications in vivo. Nat. Med. 1995, 1, 69–73. [Google Scholar] [CrossRef]
- Soila, K.; Nummi, P.; Ekfors, T.; Viamonte, M.A., Jr.; Kormano, M. Proton relaxation times in arterial wall and atheromatous lesions in man. Investig. Radiol. 1986, 21, 411–415. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Year | Journal | Type of Study | Study Period | Study Type | Number of Patients | Age (Years) | Males | Females |
|---|---|---|---|---|---|---|---|---|---|
| U-Kind-Im et al. [9] | 2010 | Stroke | Retrospective of prospective data | 2003–2008 | Retrospective Observational | 167 | 69 ± 12.8 | 109 | 58 |
| Anzidei et al. [15] | 2010 | J Vasc Interv Radiol | Retrospective of prospective data | 2008 | Retrospective Observational | 20 | NA | NA | NA |
| Trelles et al. [16] | 2013 | Am J Neuroradiol | Retrospective of prospective data | 2008–2010 | Retrospective Observational | 51 | 71.3 ± 0.9 | 38 | 13 |
| Gupta et al. [8] | 2015 | Cerebrovasc Dis | Retrospective of prospective data | 2009–2014 | Retrospective Observational | 43 | 74.5 ± 9.8 | 28 | 15 |
| Eisenmenger et al. [17] | 2016 | Am J Neuroradiol | Retrospective of prospective data | 2009–2016 | Retrospective Observational | 96 | 65.7 ± 13.4 | 75 | 21 |
| Author | Number of Patients | Number of Plaques | Symptomatic | Asymptomatic | Stroke | TIA | Stenosis Severity (NASCET) Number of Plaques (Mild/Moderate/Severe) |
|---|---|---|---|---|---|---|---|
| U-Kind-Im et al. [9] | 167 | 319 | 153 | 14 | NA | NA | 193/60/66 |
| Anzidei et al. [15] | 20 | 40 | 20 | 0 | NA | NA | 7/6/17 |
| Trelles et al. [16] | 51 | 100 | NA | NA | NA | NA | NA |
| Gupta et al. [8] | 43 | 48 | 34 | 9 | 30 | 4 | 0/23/25 |
| Eisenmenger et al. [17] | 96 | 188 | 96 | 0 | NA | NA | 128/30/30 |
| Author | Imaging (Control) | Imaging (Comparator) | Time Interval between Modalities (Days) | Researcher | MRA Power (Tesla) | CTA Slice (Number) | MRA Contrast—Type (Yes/No) | CTA Contrast—Type (Yes/No) |
|---|---|---|---|---|---|---|---|---|
| U-Kind-Im et al. [9] | MRA | CTA | 21 | 1 neuroradiologist for MRA, 2 for CTA | 1.5 | 4 or 64 | No | Yes (Iohexol or Iodixalon) |
| Anzidei et al. [15] | DSA | MRA, CTA | 6 ± 2 | 2 observers, 1 vascular radiologist | 1.5 | 64 | Yes (Gadofosveset Trisodium) | Yes (Iomeprol or Iomeron) |
| Trelles et al. [16] | MRA | CTA | 7.8 | 2 radiologists | 3 | 64 | Yes (Gadobutrol) | Yes (Iopromide) |
| Gupta et al. [8] | CTA | MR | 2 | 2 neuroradiologists | 1.5/3 | NA | No | Yes (Iohexol) |
| Eisenmenger et al. [17] | MRA | CTA | IPH(+): 6.9 ± 9.3, IPH(−): 5.6 ± 8.2 | 3 neuroradiologist (resident, fellow, attending) | 1.5/3 | 64 | Yes (NA) | Yes (Iopamidol) |
| Author | Number of Patients | Number of Plaques | Vulnerable Plaque Characteristic (MRA) | Vulnerable Plaque Characteristic (CTA) |
|---|---|---|---|---|
| U-Kind-Im et al. [9] | 167 | 319 | IPH (n = 56) | Mean plaque density: IPH(+): 47HU, SD: 15—IPH(−): 43HU, SD: 14 (p = 0.001) Mean NASCET percentage stenosis: IPH(+): 58%, SD: 26)—IPH(−): 20, SD: 26 (p = 0.02) Plaque ulceration: IPH(+): n = 45, n = 51 (2 readers) |
| Anzidei et al. [15] | 20 | 40 | Plaque ulceration (SS) (n = 9) | Plaque Ulceration (n = 8) |
| Trelles et al. [16] | 51 | 100 | Type VI plaque (AHA classification) (n = 23) | Maximum wall thickness: Type VI(+): 5.3 ± 0.4 mm—Type VI(−): 3.9 ± 0.3 mm (p < 0.001) Maximum soft plaque thickness: Type VI(+): 4.7 ± 0.5 mm—Type VI(−): 2.2 ± 0.3 mm (p < 0.001) Mean NASCET percentage stenosis: Type VI(+): 46.3% ± 10.6%—Type VI(−): 20.5% ± 6.0% (p < 0.001) |
| Gupta et al. [8] | 43 | 48 | IHIS (n = 27) | Mean soft-plaque thickness: IHIS(+): 4.47 ± 1.41 mm—IHIS(−): 2.32.3 ± 1.58 (p < 0.0001) |
| Eisenmenger et al. [17] | 96 | 188 | IPH (n = 44) | Mean NASCET percentage stenosis: IPH(+): 53.9%—IPH(−): 24.9% (p < 0.001) Mean maximum-plaque thickness: IPH(+): 5.93 mm—IPH(−): 3.42 mm (p < 0.001) Mean soft-plaque thickness: IPH(+): 5.26 mm—IPH(−): 2.99 mm (p < 0.001) Mean hard-plaque thickness: IPH(+): 2.97—IPH(−): 1.91 mm (p = 0.002) Rim-sign (Prevalence ratio = 11.9; 95% CI: 4.4–32, p < 0.001) |
| Study | Risk of Bias (QUADAS-2) | Applicability Concerns (QUADAS-2) | Risk of Bias (QUADAS-C) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P | I | R | FT | P | I | R | P | I | R | FT | |||
| CTA | MRA | CTA | MRA | ||||||||||
| U-Kind-Im et al. [9] | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ? | ✗ | ✓ | ✓ | ✓ |
| Anzidei et al. [15] | ✗ | ? | ✗ | ✓ | ✓ | ✓ | ✗ | ? | ✓ | ✗ | ✗ | ? | ✓ |
| Trelles et al. [16] | ✗ | ? | ✗ | ✓ | ✓ | ✓ | ✗ | ? | ✓ | ✗ | ? | ✗ | ✓ |
| Gupta et al. [8] | ✗ | ? | ✗ | ✓ | ✓ | ✓ | ? | ✗ | ✓ | ✗ | ? | ✗ | ✓ |
| Eisenmenger et al. [17] | ✗ | ✗ | ? | ✓ | ✓ | ✓ | ✗ | ? | ✓ | ✗ | ✗ | ? | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dakis, K.; Nana, P.; Athanasios, C.; Spanos, K.; Konstantinos, B.; Giannoukas, A.; Kouvelos, G. Carotid Plaque Vulnerability Diagnosis by CTA versus MRA: A Systematic Review. Diagnostics 2023, 13, 646. https://doi.org/10.3390/diagnostics13040646
Dakis K, Nana P, Athanasios C, Spanos K, Konstantinos B, Giannoukas A, Kouvelos G. Carotid Plaque Vulnerability Diagnosis by CTA versus MRA: A Systematic Review. Diagnostics. 2023; 13(4):646. https://doi.org/10.3390/diagnostics13040646
Chicago/Turabian StyleDakis, Konstantinos, Petroula Nana, Chaidoulis Athanasios, Konstantinos Spanos, Batzalexis Konstantinos, Athanasios Giannoukas, and George Kouvelos. 2023. "Carotid Plaque Vulnerability Diagnosis by CTA versus MRA: A Systematic Review" Diagnostics 13, no. 4: 646. https://doi.org/10.3390/diagnostics13040646