
Finger-Floor Distance Is Not a Valid Parameter for the Assessment of Lumbar Mobility
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
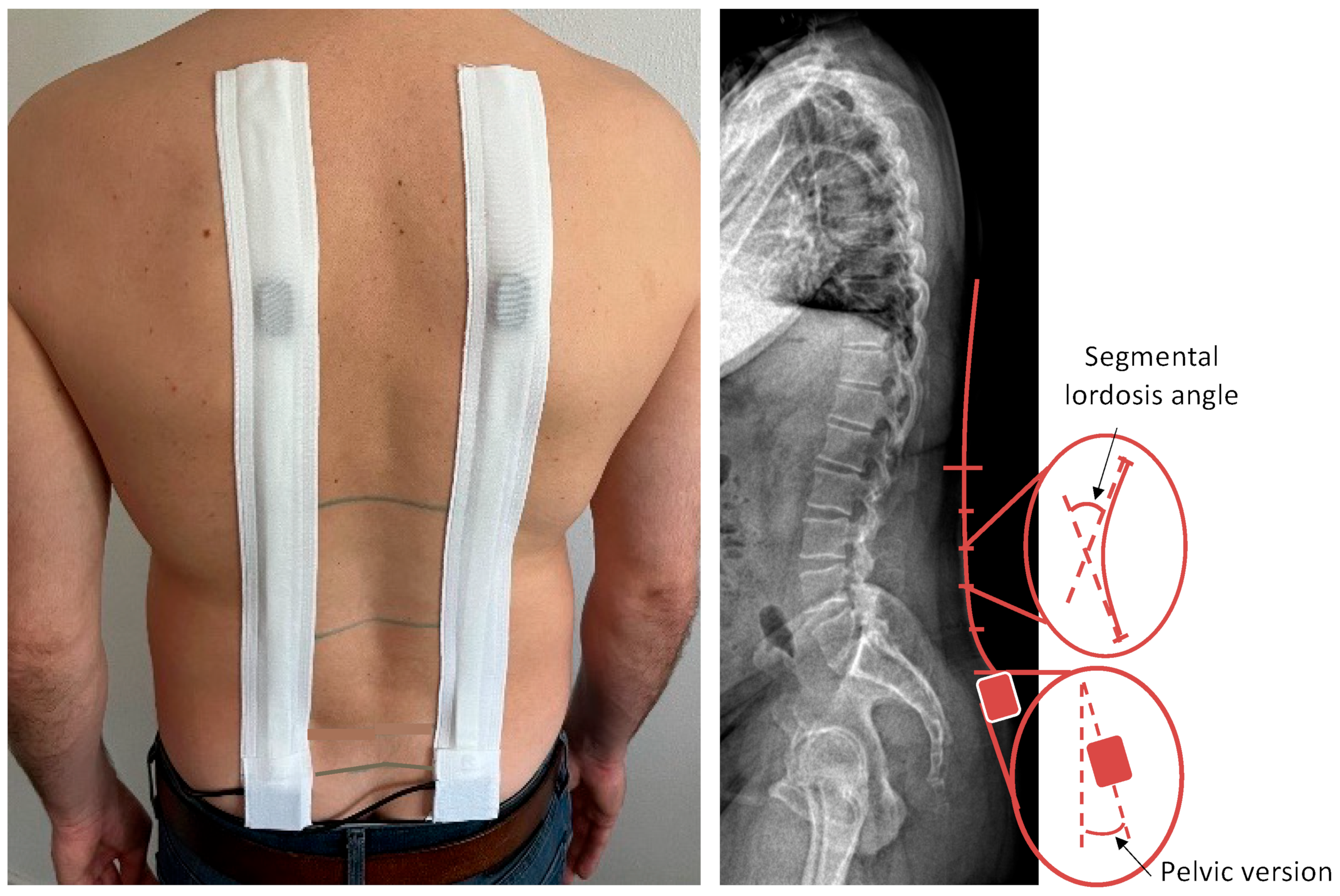
2.3. Epionics SPINE Measurement Device
2.4. Measurement Protocol
2.5. Measurement Protocol “Gradual Trunk Flexion”
2.6. Data Analysis
3. Results
3.1. Demographics
3.2. Sex Differences in Pelvic Version, Lumbar Lordosis, Pelvic- and Lumbar-RoF
3.3. Influence of LBP
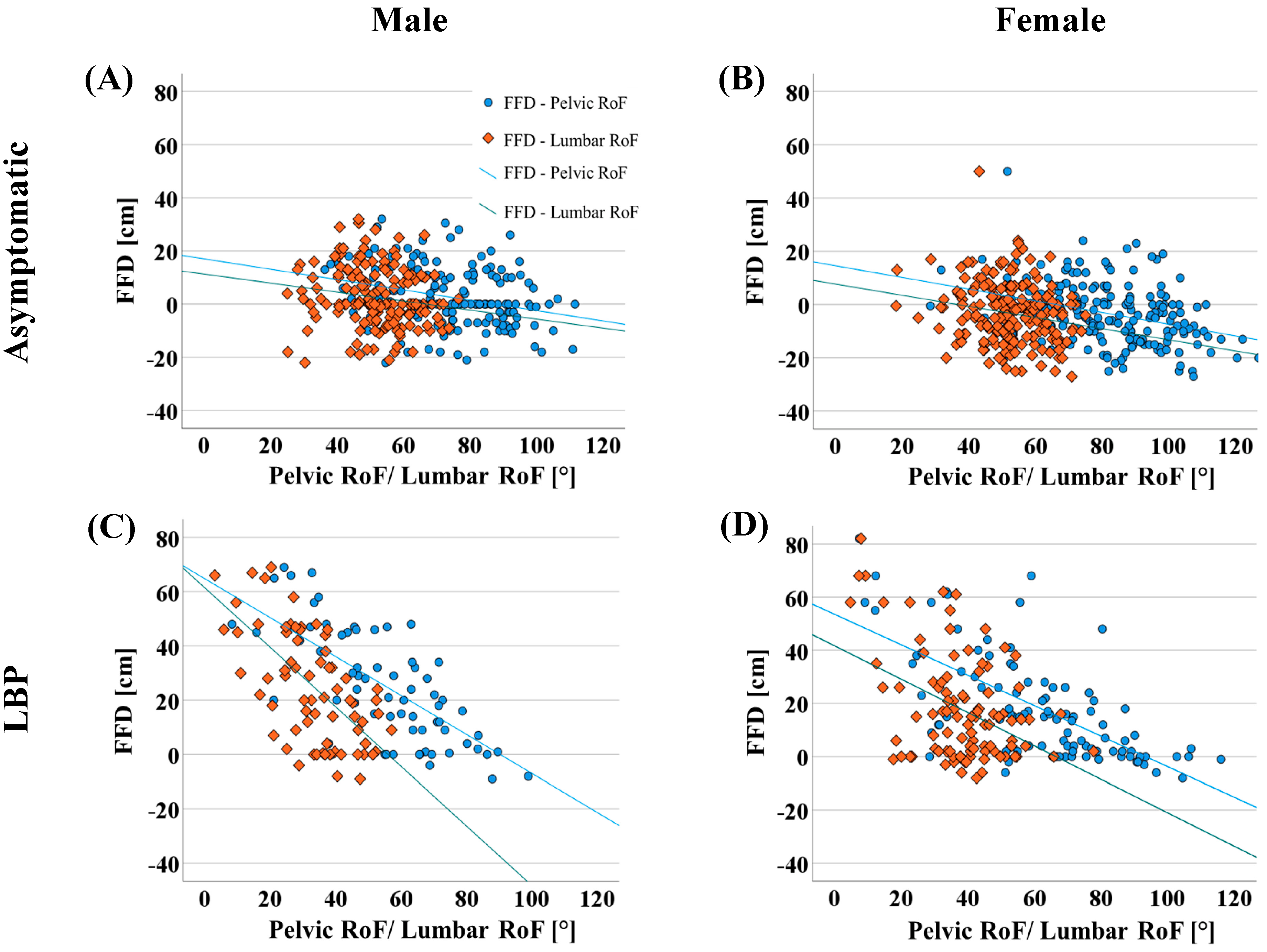
3.4. Correlation between Lumbar and Pelvic-RoF and FFD
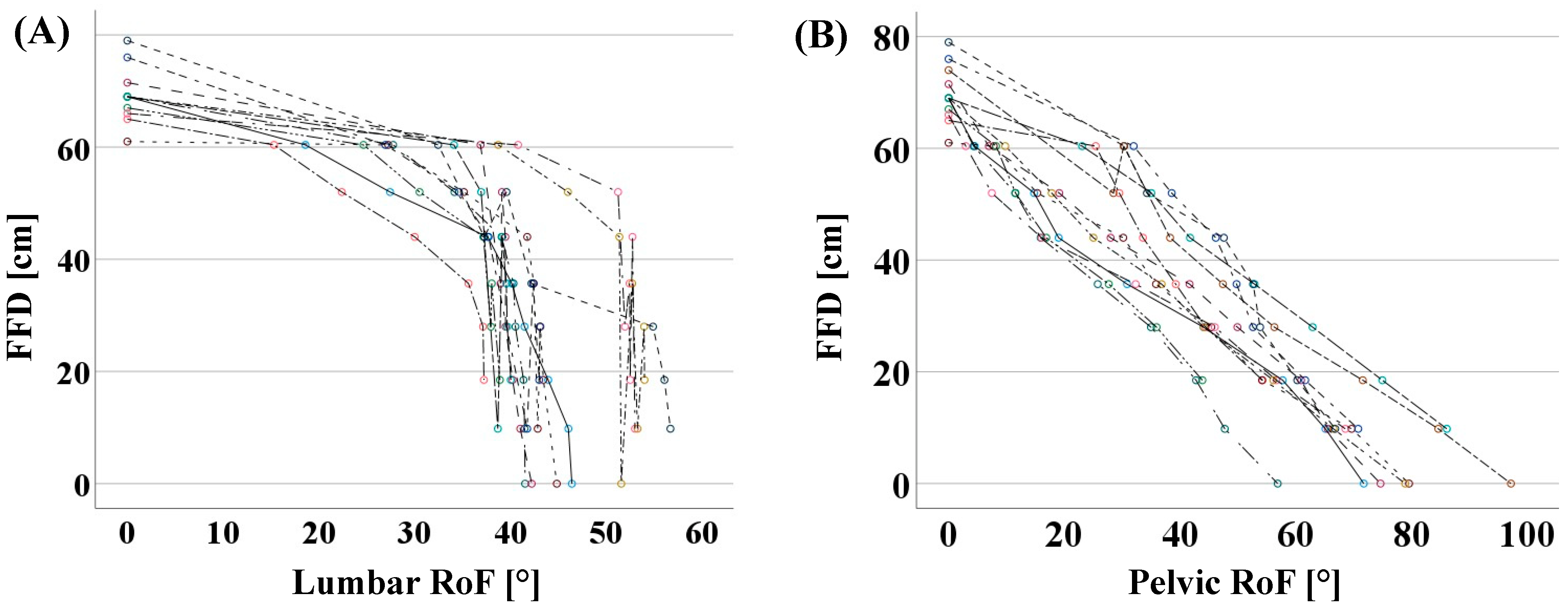
3.5. Relationship between Pelvic-RoF, Lumbar-RoF, and Gradual FFD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, A.; March, L.; Zheng, X.; Huang, J.; Wang, X.; Zhao, J.; Blyth, F.M.; Smith, E.; Buchbinder, R.; Hoy, D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020, 8, 299. [Google Scholar] [CrossRef] [PubMed]
- Laird, R.A.; Gilbert, J.; Kent, P.; Keating, J.L. Comparing lumbo-pelvic kinematics in people with and without back pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2014, 15, 229. [Google Scholar] [CrossRef] [PubMed]
- Wernli, K.; Tan, J.S.; O’Sullivan, P.; Smith, A.; Campbell, A.; Kent, P. Does Movement Change When Low Back Pain Changes? A Systematic Review. J. Orthop. Sport. Phys. Ther. 2020, 50, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Agnus Tom, A.; Rajkumar, E.; John, R.; Joshua George, A. Determinants of quality of life in individuals with chronic low back pain: A systematic review. Health Psychol. Behav. Med. 2022, 10, 124–144. [Google Scholar] [CrossRef]
- de Luca, K.; Anderson, D.; Dutt, A.; Magennis, L.; Parrello, T.; Ferreira, M.L.; Chiarotto, A. Outcome Domain and Measurement Instrument Reporting in Randomized Controlled Trials of Interventions for Lumbar Spinal Stenosis: A Systematic Review. J. Orthop. Sport. Phys. Ther. 2022, 52, 446-A2. [Google Scholar] [CrossRef]
- Chapman, J.R.; Norvell, D.C.; Hermsmeyer, J.T.; Bransford, R.J.; DeVine, J.; McGirt, M.J.; Lee, M.J. Evaluating common outcomes for measuring treatment success for chronic low back pain. Spine 2011, 36, S54–S68. [Google Scholar] [CrossRef]
- Garg, A.; Pathak, H.; Churyukanov, M.V.; Uppin, R.B.; Slobodin, T.M. Low back pain: Critical assessment of various scales. Eur. Spine J. 2020, 29, 503–518. [Google Scholar] [CrossRef]
- Poitras, S.; Loisel, P.; Prince, F.; Lemaire, J. Disability measurement in persons with back pain: A validity study of spinal range of motion and velocity. Arch. Phys. Med. Rehabil. 2000, 81, 1394–1400. [Google Scholar] [CrossRef]
- Shahvarpour, A.; Henry, S.M.; Preuss, R.; Mecheri, H.; Lariviere, C. The effect of an 8-week stabilization exercise program on the lumbopelvic rhythm and flexion-relaxation phenomenon. Clin. Biomech. 2017, 48, 1–8. [Google Scholar] [CrossRef]
- Ge, L.; Pereira, M.J.; Yap, C.W.; Heng, B.H. Chronic low back pain and its impact on physical function, mental health, and health-related quality of life: A cross-sectional study in Singapore. Sci. Rep. 2022, 12, 20040. [Google Scholar] [CrossRef]
- Abd Rahman, N.A.; Li, S.; Schmid, S.; Shaharudin, S. Biomechanical factors associated with non-specific low back pain in adults: A systematic review. Phys. Ther. Sport 2023, 59, 60–72. [Google Scholar] [CrossRef]
- Fritz, J.M.; Cleland, J.A.; Childs, J.D. Subgrouping patients with low back pain: Evolution of a classification approach to physical therapy. J. Orthop. Sport. Phys. Ther. 2007, 37, 290–302. [Google Scholar] [CrossRef]
- Enix, D.; Cho, C.; Sembrano, J.; Easa, J.; Annaswamy, T.; Meagher, R.; Cassidy, R.; O’Toole, J.; Matz, P.; Asgari, M.; et al. Evidence-Based Clinical Guidelines for Multidisciplinary Spine Care: Diagnosis & Treatment of Low Back Pain. N. Am. Spine Soc. 2020, 1–217. [Google Scholar]
- Perret, C.; Poiraudeau, S.; Fermanian, J.; Colau, M.M.; Benhamou, M.A.; Revel, M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch. Phys. Med. Rehabil. 2001, 82, 1566–1570. [Google Scholar] [CrossRef]
- Ekedahl, H.; Jonsson, B.; Frobell, R.B. Fingertip-to-floor test and straight leg raising test: Validity, responsiveness, and predictive value in patients with acute/subacute low back pain. Arch. Phys. Med. Rehabil. 2012, 93, 2210–2215. [Google Scholar] [CrossRef]
- Wong, T.K.; Lee, R.Y. Effects of low back pain on the relationship between the movements of the lumbar spine and hip. Hum. Mov. Sci. 2004, 23, 21–34. [Google Scholar] [CrossRef]
- Schmidt, H.; Bashkuev, M.; Weerts, J.; Altenscheidt, J.; Maier, C.; Reitmaier, S. What does the shape of our back tell us? Correlation between sacrum orientation and lumbar lordosis. Spine J. 2018, 18, 655–662. [Google Scholar] [CrossRef]
- Pries, E.; Dreischarf, M.; Bashkuev, M.; Putzier, M.; Schmidt, H. The effects of age and gender on the lumbopelvic rhythm in the sagittal plane in 309 subjects. J. Biomech. 2015, 48, 3080–3087. [Google Scholar] [CrossRef]
- Mayer, T.G.; Tencer, A.F.; Kristoferson, S.; Mooney, V. Use of noninvasive techniques for quantification of spinal range-of-motion in normal subjects and chronic low-back dysfunction patients. Spine 1984, 9, 588–595. [Google Scholar] [CrossRef]
- Esola, M.A.; McClure, P.W.; Fitzgerald, G.K.; Siegler, S. Analysis of lumbar spine and hip motion during forward bending in subjects with and without a history of low back pain. Spine 1996, 21, 71–78. [Google Scholar] [CrossRef]
- Porter, J.L.; Wilkinson, A. Lumbar-hip flexion motion. A comparative study between asymptomatic and chronic low back pain in 18- to 36-year-old men. Spine 1997, 22, 1508–1513, discussion 1513–1504. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Yi, C.H.; Kwon, O.Y.; Cho, S.H.; Cynn, H.S.; Kim, Y.H.; Hwang, S.H.; Choi, B.R.; Hong, J.A.; Jung, D.H. Comparison of lumbopelvic rhythm and flexion-relaxation response between 2 different low back pain subtypes. Spine 2013, 38, 1260–1267. [Google Scholar] [CrossRef] [PubMed]
- Tafazzol, A.; Arjmand, N.; Shirazi-Adl, A.; Parnianpour, M. Lumbopelvic rhythm during forward and backward sagittal trunk rotations: Combined in vivo measurement with inertial tracking device and biomechanical modeling. Clin. Biomech. 2014, 29, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Arshad, R.; Pan, F.; Reitmaier, S.; Schmidt, H. Effect of age and sex on lumbar lordosis and the range of motion. A systematic review and meta-analysis. J. Biomech. 2019, 82, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.D.; Shultz, S.J. Sex differences in clinical measures of lower extremity alignment. J. Orthop. Sport. Phys. Ther. 2007, 37, 389–398. [Google Scholar] [CrossRef]
- Medina McKeon, J.M.; Hertel, J. Sex differences and representative values for 6 lower extremity alignment measures. J. Athl. Train. 2009, 44, 249–255. [Google Scholar] [CrossRef]
- Merrill, R.K.; Kim, J.S.; Leven, D.M.; Kim, J.H.; Meaike, J.J.; Bronheim, R.S.; Suchman, K.I.; Nowacki, D.; Gidumal, S.S.; Cho, S.K. Differences in Fundamental Sagittal Pelvic Parameters Based on Age, Sex, and Race. Clin. Spine Surg. 2018, 31, E109–E114. [Google Scholar] [CrossRef]
- Czuppon, S.; Prather, H.; Hunt, D.M.; Steger-May, K.; Bloom, N.J.; Clohisy, J.C.; Larsen, R.; Harris-Hayes, M. Gender-Dependent Differences in Hip Range of Motion and Impingement Testing in Asymptomatic College Freshman Athletes. PM R 2017, 9, 660–667. [Google Scholar] [CrossRef]
- Chun, S.W.; Lim, C.Y.; Kim, K.; Hwang, J.; Chung, S.G. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine J. 2017, 17, 1180–1191. [Google Scholar] [CrossRef]
- Laird, R.A.; Kent, P.; Keating, J.L. How consistent are lordosis, range of movement and lumbo-pelvic rhythm in people with and without back pain? BMC Musculoskelet. Disord. 2016, 17, 403. [Google Scholar] [CrossRef]
- Parks, K.A.; Crichton, K.S.; Goldford, R.J.; McGill, S.M. A comparison of lumbar range of motion and functional ability scores in patients with low back pain: Assessment for range of motion validity. Spine 2003, 28, 380–384. [Google Scholar] [CrossRef]
- Matheve, T.; De Baets, L.; Bogaerts, K.; Timmermans, A. Lumbar range of motion in chronic low back pain is predicted by task-specific, but not by general measures of pain-related fear. Eur. J. Pain 2019, 23, 1171–1184. [Google Scholar] [CrossRef]
- Shum, G.L.; Crosbie, J.; Lee, R.Y. Effect of low back pain on the kinematics and joint coordination of the lumbar spine and hip during sit-to-stand and stand-to-sit. Spine 2005, 30, 1998–2004. [Google Scholar] [CrossRef]
- Reeves, S.L.; Varakamin, C.; Henry, C.J. The relationship between arm-span measurement and height with special reference to gender and ethnicity. Eur. J. Clin. Nutr. 1996, 50, 398–400. [Google Scholar]
- Haffer, H.; Adl Amini, D.; Perka, C.; Pumberger, M. The Impact of Spinopelvic Mobility on Arthroplasty: Implications for Hip and Spine Surgeons. J. Clin. Med. 2020, 9, 2569. [Google Scholar] [CrossRef]
- Consmuller, T.; Rohlmann, A.; Weinland, D.; Druschel, C.; Duda, G.N.; Taylor, W.R. Comparative evaluation of a novel measurement tool to assess lumbar spine posture and range of motion. Eur. Spine J. 2012, 21, 2170–2180. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Overall | |||||
|---|---|---|---|---|---|
| LBP (n = 167) | Asymptomatic Control (n = 356) | ||||
| Male Median (IQR) | Female Median (IQR) | Male Median (IQR) | Female Median (IQR) | ||
| n | 70 | 97 | 159 | 197 | |
| Age [years] | 49 (22) | 51 (20) | 36 (21) | 37 (22) | |
| Height [cm] | 178 (11) | 167 (8) | 179 (11) | 168 (9) | |
| BMI [kg/m2] | 26.3 (6.0) | 25.8 (6.1) | 24.0 (2.0) | 22.0 (3.0) | |
| Matched Groups | |||||
| LBP (n = 120) | Asymptomatic Control (n = 120) | p-value | |||
| Male Median (IQR) | Female Median (IQR) | Male Median (IQR) | Female Median (IQR) | ||
| n | 49 | 71 | 49 | 71 | 1.000 |
| Age [years] | 49 (23) | 50 (22) | 48 (18) | 49 (22) | 0.804 |
| Height [cm] | 178 (12) | 168 (9) | 178 (14) | 168 (7) | 0.802 |
| BMI [kg/m2] | 24.9 (3.8) | 24.1 (5.1) | 25.0 (2.0) | 24.0 (4.0) | 0.380 |
| All Median (IQR) (n = 523) | Male Median (IQR) (n = 229) | Female Median (IQR) (n = 294) | p-Value | |
|---|---|---|---|---|
| Pelvic version [°] | 17.9 (11.7) | 16.0 (11.8) | 19.0 (10.9) | <0.001 |
| Lumbar lordosis [°] | 30.8 (14.4) | 28.3 (16.0) | 32.1 (13.4) | <0.001 |
| Pelvic-RoF [°] | 72.9 (30.1) | 69.5 (28.4) | 76.2 (27.7) | <0.001 |
| Lumbar-RoF [°] | 48.5 (17.8) | 48.0 (19.4) | 49.5 (16.6) | 0.277 |
| FFD [cm] | 1.0 (20.0) | 5.0 (19.5) | 0.0 (20) | <0.001 |
| LBP Median (IQR) (n = 120) | Control Median (IQR) (n = 120) | p-Value | |
|---|---|---|---|
| Pelvic version [°] | 13.5 (11.0) | 17.7 (11.9) | <0.001 |
| Lumbar lordosis [°] | 23.7 (11.9) | 30.5 (16.2) | <0.001 |
| Pelvic-RoF [°] | 61.2 (29.4) | 74.2 (26.3) | <0.001 |
| Lumbar-RoF [°] | 37.7 (15.8) | 50.7 (14.6) | <0.001 |
| FFD [cm] | 16.5 (33.3) | 0.0 (15.0) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker, L.; Schömig, F.; Cordes, L.M.-S.; Duda, G.N.; Pumberger, M.; Schmidt, H. Finger-Floor Distance Is Not a Valid Parameter for the Assessment of Lumbar Mobility. Diagnostics 2023, 13, 638. https://doi.org/10.3390/diagnostics13040638
Becker L, Schömig F, Cordes LM-S, Duda GN, Pumberger M, Schmidt H. Finger-Floor Distance Is Not a Valid Parameter for the Assessment of Lumbar Mobility. Diagnostics. 2023; 13(4):638. https://doi.org/10.3390/diagnostics13040638
Chicago/Turabian StyleBecker, Luis, Friederike Schömig, Lea Marie-Sophie Cordes, Georg N. Duda, Matthias Pumberger, and Hendrik Schmidt. 2023. "Finger-Floor Distance Is Not a Valid Parameter for the Assessment of Lumbar Mobility" Diagnostics 13, no. 4: 638. https://doi.org/10.3390/diagnostics13040638