
Retinal Blood Vessel Analysis Using Optical Coherence Tomography (OCT) in Multiple Sclerosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
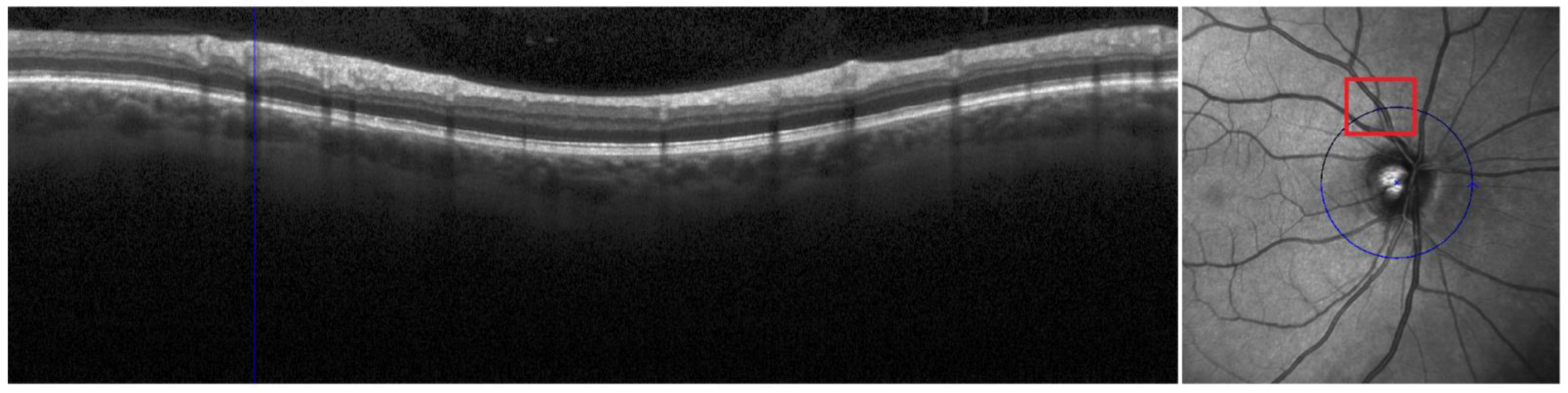
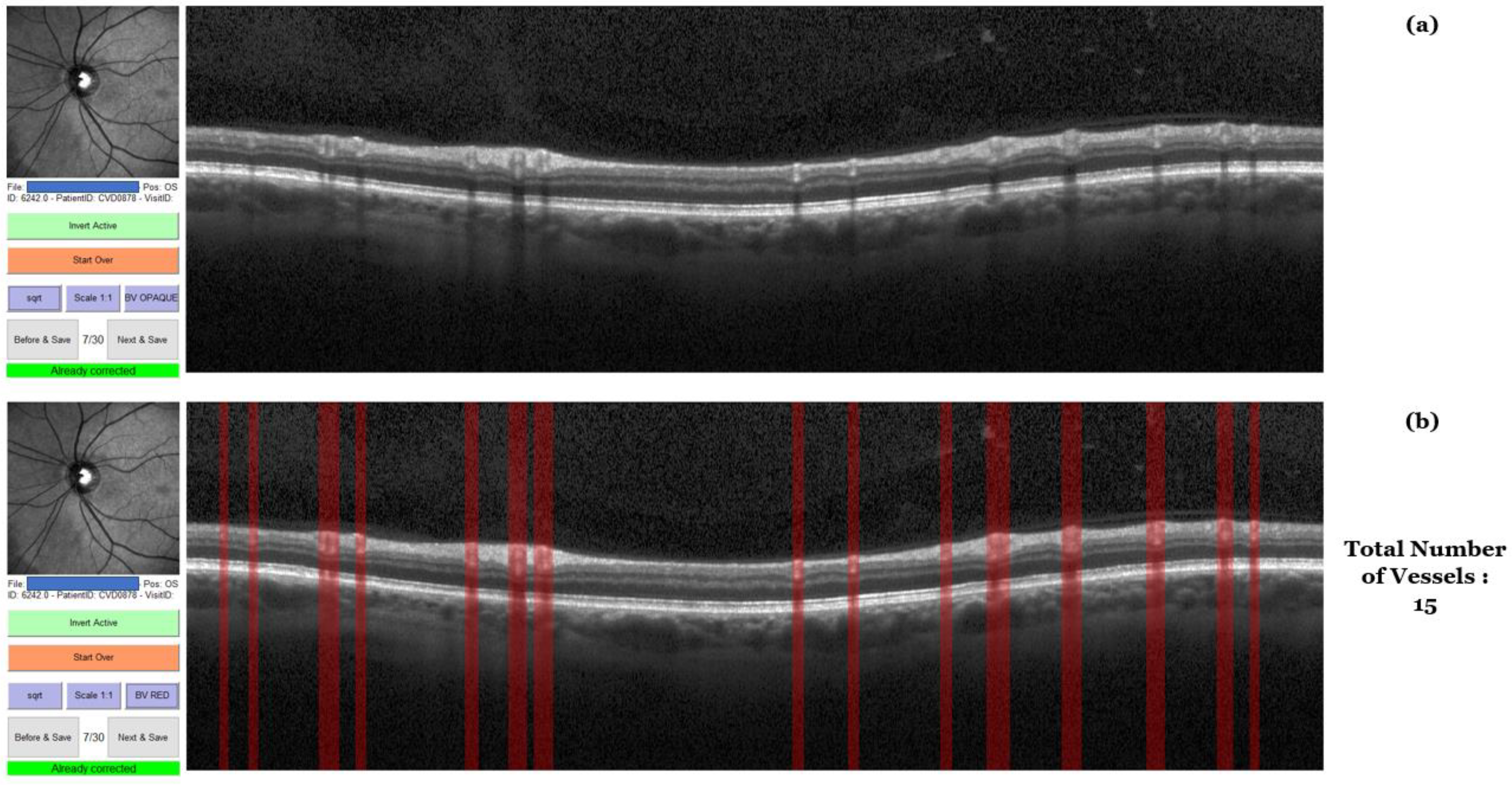
2.2. OCT Acquisition and Analyses
2.3. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of the Study Population
3.2. OCT-Based Measures at Baseline and Follow-Up
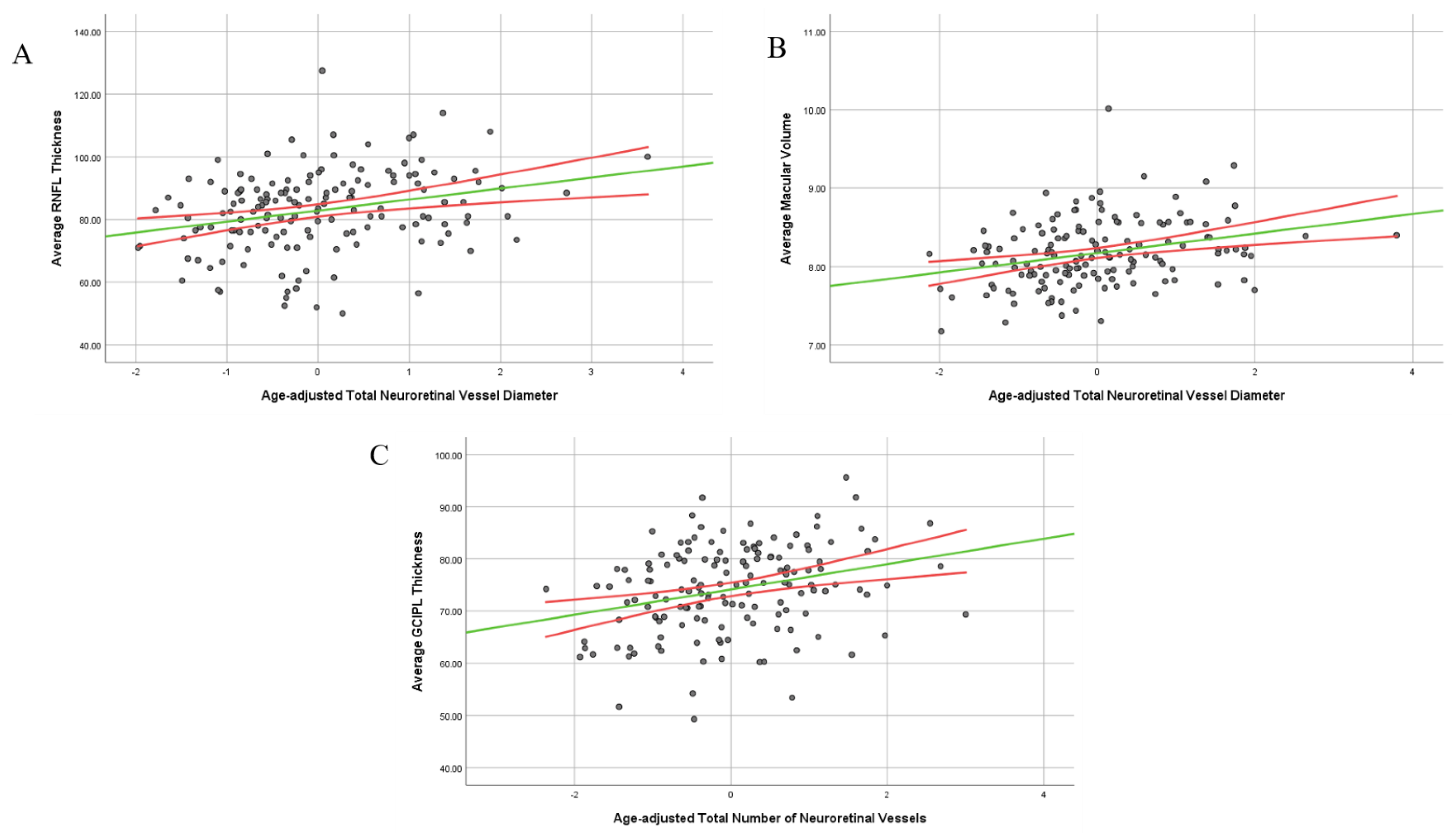
3.3. Relationship between Retinal Vasculature and Retinal Layer Thickness in the Study Population
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple Sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef] [PubMed]
- D’Haeseleer, M.; Cambron, M.; Vanopdenbosch, L.; De Keyser, J. Vascular aspects of multiple sclerosis. Lancet Neurol. 2011, 10, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Jakimovski, D.; Topolski, M.; Genovese, A.V.; Weinstock-Guttman, B.; Zivadinov, R. Vascular aspects of multiple sclerosis: Emphasis on perfusion and cardiovascular comorbidities. Expert Rev. Neurother. 2019, 19, 445–458. [Google Scholar] [CrossRef]
- Jakimovski, D.; Gandhi, S.; Paunkoski, I.; Bergsland, N.; Hagemeier, J.; Ramasamy, D.P.; Hojnacki, D.; Kolb, C.; Benedict, R.H.B.; Weinstock-Guttman, B.; et al. Hypertension and heart disease are associated with development of brain atrophy in multiple sclerosis: A 5-year longitudinal study. Eur. J. Neurol. 2019, 26, 87–88. [Google Scholar] [CrossRef]
- Thormann, A.; Magyari, M.; Koch-Henriksen, N.; Laursen, B.; Sorensen, P.S. Vascular comorbidities in multiple sclerosis: A nationwide study from Denmark. J. Neurol. 2016, 263, 2484–2493. [Google Scholar] [CrossRef]
- Geraldes, R.; Esiri, M.M.; Perera, R.; Yee, S.A.; Jenkins, D.; Palace, J.; DeLuca, G.C. Vascular disease and multiple sclerosis: A post-mortem study exploring their relationships. Brain 2020, 143, 2998–3012. [Google Scholar] [CrossRef]
- Petzold, A.; de Boer, J.F.; Schippling, S.; Vermersch, P.; Kardon, R.; Green, A.; Calabresi, P.A.; Polman, C. Optical coherence tomography in multiple sclerosis: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Jakimovski, D.; Zivadinov, R.; Vaughn, C.B.; Ozel, O.; Weinstock-Guttman, B. Clinical effects associated with five-year retinal nerve fiber layer thinning in multiple sclerosis. J. Neurol. Sci. 2021, 427, 117552. [Google Scholar] [CrossRef]
- Jakimovski, D.; Ramasamy, D.P.; Zivadinov, R. Magnetic Resonance Imaging and Analysis in Multiple Sclerosis. In Clinical Neuroimmunology: Multiple Sclerosis and Related Disorders; Rizvi, S.A., Cahill, J.F., Coyle, P.K., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 109–136. [Google Scholar]
- Kanda, T.; Fukusato, T.; Matsuda, M.; Toyoda, K.; Oba, H.; Kotoku, J.i.; Haruyama, T.; Kitajima, K.; Furui, S. Gadolinium-based Contrast Agent Accumulates in the Brain Even in Subjects without Severe Renal Dysfunction: Evaluation of Autopsy Brain Specimens with Inductively Coupled Plasma Mass Spectroscopy. Radiology 2015, 276, 228–232. [Google Scholar] [CrossRef]
- Hood, D.C.; Fortune, B.; Arthur, S.N.; Xing, D.; Salant, J.A.; Ritch, R.; Liebmann, J.M. Blood vessel contributions to retinal nerve fiber layer thickness profiles measured with optical coherence tomography. J. Glaucoma 2008, 17, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Tavazzi, E.; Jakimovski, D.; Kuhle, J.; Hagemeier, J.; Ozel, O.; Ramanathan, M.; Barro, C.; Bergsland, N.; Tomic, D.; Kropshofer, H.; et al. Serum neurofilament light chain and optical coherence tomography measures in MS: A longitudinal study. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sørensen, P.S.; Thompson, A.J.; Wolinsky, J.S.; Balcer, L.J.; Banwell, B.; Barkhof, F.; et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Bhaduri, B.; Nolan, R.M.; Shelton, R.L.; Pilutti, L.A.; Motl, R.W.; Moss, H.E.; Pula, J.H.; Boppart, S.A. Detection of retinal blood vessel changes in multiple sclerosis with optical coherence tomography. Biomed. Opt. Express 2016, 7, 2321–2330. [Google Scholar] [CrossRef] [PubMed]
- Cennamo, G.; Carotenuto, A.; Montorio, D.; Petracca, M.; Moccia, M.; Melenzane, A.; Tranfa, F.; Lamberti, A.; Spiezia, A.L.; Servillo, G.; et al. Peripapillary Vessel Density as Early Biomarker in Multiple Sclerosis. Front. Neurol. 2020, 11, 542. [Google Scholar] [CrossRef] [PubMed]
- Montorio, D.; Lanzillo, R.; Carotenuto, A.; Petracca, M.; Moccia, M.; Criscuolo, C.; Spiezia, A.L.; Lamberti, A.; Perrotta, F.; Pontillo, G.; et al. Retinal and Choriocapillary Vascular Changes in Early Stages of Multiple Sclerosis: A Prospective Study. J. Clin. Med. 2021, 10, 5756. [Google Scholar] [CrossRef] [PubMed]
- Drobnjak Nes, D.; Berg-Hansen, P.; de Rodez Benavent, S.A.; Høgestøl, E.A.; Beyer, M.K.; Rinker, D.A.; Veiby, N.; Karabeg, M.; Petrovski, B.É.; Celius, E.G.; et al. Exploring Retinal Blood Vessel Diameters as Biomarkers in Multiple Sclerosis. J. Clin. Med. 2022, 11, 3109. [Google Scholar] [CrossRef]
- Murphy, O.C.; Kwakyi, O.; Iftikhar, M.; Zafar, S.; Lambe, J.; Pellegrini, N.; Sotirchos, E.S.; Gonzalez-Caldito, N.; Ogbuokiri, E.; Filippatou, A.; et al. Alterations in the retinal vasculature occur in multiple sclerosis and exhibit novel correlations with disability and visual function measures. Mult. Scler. 2020, 26, 815–828. [Google Scholar] [CrossRef]
- Qureshi, S.S.; Beh, S.C.; Frohman, T.C.; Frohman, E.M. An update on neuro-ophthalmology of multiple sclerosis: The visual system as a model to study multiple sclerosis. Curr. Opin. Neurol. 2014, 27, 300–308. [Google Scholar] [CrossRef]
- Van Gelder, R.N.; Sen, H.N.; Tufail, A.; Lee, A.Y. Here Comes the SUN (Part 2): Standardization of Uveitis Nomenclature for Disease Classification Criteria. Am. J. Ophthalmol. 2021, 228, A2–A6. [Google Scholar] [CrossRef] [PubMed]
- Shugaiv, E.; Tüzün, E.; Kürtüncü, M.; Kıyat-Atamer, A.; Çoban, A.; Akman-Demir, G.; Tugal-Tutkun, I.; Eraksoy, M. Uveitis as a prognostic factor in multiple sclerosis. Mult. Scler. 2015, 21, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.M.; Pulido, J.S.; Eckels, D.D.; Han, D.P.; Mieler, W.F.; Pierce, K. The association of HLA-DR15 and intermediate uveitis. Am. J. Ophthalmol. 1997, 123, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Pérez, S.; Martínez-Lapiscina, E.H.; Gabilondo, I.; Fraga-Pumar, E.; Martínez-Heras, E.; Saiz, A.; Sanchez-Dalmau, B.; Villoslada, P. Retinal periphlebitis is associated with multiple sclerosis severity. Neurology 2013, 81, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Khushzad, F.; Yarp, J.; Hargrave, A.; Sredar, N.; Mahesh, V.; Tomczak, A.; Kipp, L.; Han, M.; Dubra, A.; Moss, H. Characterization of Retinal vascular changes in Multiple Sclerosis using Adaptive Optics and OCTA. Investig. Ophthalmol. Vis. Sci. 2020, 61, 5104. [Google Scholar]
- Belov, P.; Jakimovski, D.; Krawiecki, J.; Magnano, C.; Hagemeier, J.; Pelizzari, L.; Weinstock-Guttman, B.; Zivadinov, R. Lower Arterial Cross-Sectional Area of Carotid and Vertebral Arteries and Higher Frequency of Secondary Neck Vessels Are Associated with Multiple Sclerosis. Am. J. Neuroradiol. 2018, 39, 123–130. [Google Scholar] [CrossRef]
- Pelizzari, L.; Jakimovski, D.; Laganà, M.M.; Bergsland, N.; Hagemeier, J.; Baselli, G.; Weinstock-Guttman, B.; Zivadinov, R. Five-Year Longitudinal Study of Neck Vessel Cross-Sectional Area in Multiple Sclerosis. Am. J. Neuroradiol. 2018, 39, 1703–1709. [Google Scholar] [CrossRef]
- Jakimovski, D.; Topolski, M.; Kimura, K.; Pandya, V.; Weinstock-Guttman, B.; Zivadinov, R. Decrease in Secondary Neck Vessels in Multiple Sclerosis: A 5-year Longitudinal Magnetic Resonance Angiography Study. Curr. Neurovasc. Res. 2019, 16, 215–223. [Google Scholar] [CrossRef]
- Weel, V.v.; Toes, R.E.M.; Seghers, L.; Deckers, M.M.L.; Vries, M.R.d.; Eilers, P.H.; Sipkens, J.; Schepers, A.; Eefting, D.; Hinsbergh, V.W.M.v.; et al. Natural Killer Cells and CD4+ T-Cells Modulate Collateral Artery Development. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2310–2318. [Google Scholar] [CrossRef] [PubMed]
- la Sala, A.; Pontecorvo, L.; Agresta, A.; Rosano, G.; Stabile, E. Regulation of collateral blood vessel development by the innate and adaptive immune system. Trends Mol. Med. 2012, 18, 494–501. [Google Scholar] [CrossRef]
- Absinta, M.; Nair, G.; Monaco, M.C.G.; Maric, D.; Lee, N.J.; Ha, S.K.; Luciano, N.J.; Sati, P.; Jacobson, S.; Reich, D.S. The “central vein sign” in inflammatory demyelination: The role of fibrillar collagen type I. Ann. Neurol. 2019, 85, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, B.; Koc, P.; Ozaydin Goksu, E.; Karacay, E.; Kurtulus, F.; Cekin, Y.; Bicer Gomceli, Y. Is multiple sclerosis a risk factor for atherosclerosis? J. Neuroradiol. 2021, 48, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.M.; Westergaard, T.; Frisch, M.; Rostgaard, K.; Wohlfahrt, J.; Koch-Henriksen, N.; Melbye, M.; Hjalgrim, H. Type 1 Diabetes and Multiple Sclerosis: A Danish Population-Based Cohort Study. Arch. Neurol. 2006, 63, 1001–1004. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Rusinek, H.; Chen, J.; Bokacheva, L.; Vedvyas, A.; Masurkar, A.V.; Haacke, E.M.; Wisniewski, T.; Ge, Y. Reduced white matter venous density on MRI is associated with neurodegeneration and cognitive impairment in the elderly. Front. Aging Neurosci. 2022, 14, 972282. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics Characteristics | pwMS (n = 167) | pwRRMS (n = 122) | pwPMS (n = 45) | HCs (n = 48) | pwMS vs. HCs p-Value | pwRRMS vs. pwPMS p-Value |
|---|---|---|---|---|---|---|
| Female, n (%) | 122 (73.1) | 86 (70.5) | 36 (80.0) | 33 (68.8) | 0.558 | 0.402 |
| Age in years, mean (SD) | 47.4 (11.5) | 44.4 (11.2) | 55.5 (7.9) | 43.75 (14.8) | 0.125 | <0.001 |
| Time of follow-up, mean (SD) | 5.5 (0.6) | 5.5 (0.6) | 5.4 (0.6) | 5.6 (0.5) | 0.293 | 0.76 |
| Disease duration, mean years (SD) | 13.8 (9.9) | 11.08 (8.4) | 21.00 (10.2) | - | - | <0.001 |
| Age of symptom onset, mean (SD) | 33.45 (10.1) | 33.08 (9.7) | 34.44 (11.3) | - | - | 0.442 |
| RRMS/PMS, n (RRMS %) | 122/45 (73.1) | - | - | - | - | - |
| EDSS at baseline, median (IQR) | 2.5 (1.5–4.5) | 1.5 (1.5–2.5) | 5.7 (4.0–6.5) | - | - | <0.001 |
| EDSS at follow-up, median (IQR) | 3.0 (1.5–6.0) | 2.0 (1.5–3.4) | 6.5 (4.5–6.5) | - | - | <0.001 |
| EDSS change, mean (SD) | 0.46 (0.9) | 0.44 (1.0) | 0.49 (0.8) | - | - | 0.814 |
| ARR, mean (SD) | 0.18 (0.43) | 0.20 (0.41) | 0.09 (0.3) | - | - | 0.115 |
| History of ON, n (%) | 84 (50.3) | 62 (50.8) | 22 (48.8) | - | - | 0.688 |
| LCLA 100%, mean (SD) | 52.6 (7.9) | 53.9 (7.8) | 49.3 (7.6) | 55.9 (4.5) | 0.001 | 0.002 |
| LCLA 2.5%, mean (SD) | 36.9 (12.9) | 38.9 (11.7) | 31.9 (14.3) | 43.2 (8.6) | <0.001 | 0.004 |
| LCLA 1.25, mean (SD) | 29.8 (18.1) | 31.1 (17.9) | 26.5 (18.2) | 36.0 (13.9) | 0.018 | 0.193 |
| DMT at baseline, n (%) | - | |||||
| IFN-β | 66 (39.4) | 47 (38.5) | 19 (42.2) | - | - | 0.038 |
| GA | 33 (19.8) | 22 (18.0) | 11 (24.4) | |||
| Natalizumab | 23 (13.8) | 18 (14.8) | 5 (11.1) | |||
| Oral DMT | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Off-label DMT | 4 (2.4) | 2 (1.7) | 2 (4.4) | |||
| Not on any DMT | 41 (24.6) | 33 (27.0) | 8 (17.8) | |||
| OCT-Based Measure | Rater 1—Trial 1 | Rater 1—Trial 2 | Rater 2 | Intra-Rater Reproducibility | Inter-Rater Reproducibility | ||
|---|---|---|---|---|---|---|---|
| ICC | p-Value | ICC | p-Value | ||||
| Total vessel diameter | 1.19 (0.2) | 1.09 (0.2) | 0.92 (0.2) | 0.906 (0.8–0.956) | <0.001 | 0.774 (0.519–0.894) | <0.001 |
| Number of vessels | 15.1 (2.5) | 16.4 (3.3) | 15.1 (2.9) | 0.762 (0.493–0.888) | <0.001 | 0.876 (0.736–0.942) | <0.001 |
| Retinal Layer Thickness and Retinal Vasculature Measures | pwMS | pwRRMS | pwPMS | HCs | pwMS vs. HCs Age Adjusted p-Value | pwRRMS vs. pwPMS Age-Adjusted p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 101 | n = 167 | n = 73 | n = 113 | n = 28 | n = 54 | n = 35 | n = 48 | |||
| Baseline peripapillary RNFLT (µm) | 86.3 (12.9) | 88.6 (12.1) | 79.4 (13.2) | 99.9 (9.5) | 0.004 | 0.015 | ||||
| Follow-up peripapillary RNFLT (µm) | 82.8 (12.9) | 86.1 (11.6) | 74.1 (12.3) | 95.9 (11.4) | <0.001 | <0.001 | ||||
| Baseline macular volume (mm3) | 7.9 (0.9) | 7.9 (0.9) | 7.6 (0.8) | 8.8 (0.6) | 0.004 | 0.317 | ||||
| Follow-up macular volume (mm3) | 8.2 (0.4) | 8.3 (0.4) | 7.9 (0.4) | 8.5 (0.5) | 0.001 | 0.003 | ||||
| Baseline macular GCIPLT (µm) | 75.3 (12.2) | 78.2 (9.9) | 65.4 (13.7) | 86.8 (7.2) | 0.016 | 0.095 | ||||
| Follow-up macular GCIPLT (µm) | 74.1 (8.3) | 75.5 (8.2) | 70.4 (7.6) | 79.9 (9.3) | <0.001 | 0.176 | ||||
| Baseline total vessel diameter (cm) | 2.6 (0.3) | 2.60 (0.31) | 2.50 (0.4) | 2.5 (0.4) | 0.082 | 0.794 | ||||
| Follow-up total vessel diameter (cm) | 2.5 (0.4) | 2.56 (0.42) | 2.43 (0.3) | 2.7 (0.3) | 0.182 | 0.899 | ||||
| Baseline number of vessels (n) | 36.7 (7.4) | 37.14 (7.3) | 35.18 (7.6) | 34.8 (7.2) | 0.987 | 0.691 | ||||
| Follow-up number of vessels (n) | 35.1 (5.9) | 35.7 (5.9) | 33.6 (5.6) | 36.8 (5.3) | 0.017 | 0.973 | ||||
| Baseline average vessel diameter (cm) | 0.07 (0.01) | 0.07 (0.01) | 0.07 (0.01) | 0.07 (0.01) | 0.167 | 0.975 | ||||
| Follow-up average vessel diameter (cm) | 0.074 (0.01) | 0.07 (0.1) | 0.08 (0.1) | 0.075 (0.01) | 0.457 | 0.527 | ||||
| pwMS (n = 167) | HCs (n = 48) | pwRRMS (n = 122) | pwPMS (n = 45) | pwMS vs. HCs p-Value | pwRRMS vs. pwPMS p-Value | |
|---|---|---|---|---|---|---|
| Change in total vessel diameter (cm), mean (SD) | 0.06 (0.5) | 0.3 (0.5) | 0.08 (0.5) | 0.005 (0.6) | 0.017 | 0.504 |
| Change in number of vessels (n), mean (SD) | −3.7 (8.4) | 0.7 (7.6) | −3.5 (8.9) | −4.4 (7.2) | 0.007 | 0.617 |
| Change in average per-vessel diameter (cm), mean (SD) | 0.008 (0.02) | 0.007 (0.02) | 0.007 (0.02) | 0.01 (0.02) | 0.661 | 0.482 |
| RNFL Associations | pwMS (n = 167) | pwRRMS (n = 113) | pwPMS (n = 54) | HCs (n = 48) | ||||
|---|---|---|---|---|---|---|---|---|
| r-Value | p-Value | r-Value | p-Value | r-Value | p-Value | r-Value | p-Value | |
| Total vessel diameter | 0.216 | 0.007 | 0.187 | 0.058 | 0.238 | 0.096 | 0.249 | 0.099 |
| Number of vessels | 0.191 | 0.018 | 0.221 | 0.025 | 0.091 | 0.53 | 0.289 | 0.054 |
| Average vessel diameter | −0.002 | 0.983 | −0.017 | 0.862 | 0.095 | 0.513 | −0.218 | 0.151 |
| MV Associations | pwMS (n = 167) | pwRRMS (n = 113) | pwPMS (n = 54) | HCs (n = 48) | ||||
| Total vessel diameter | 0.259 | 0.001 | 0.238 | 0.017 | 0.335 | 0.017 | −0.027 | 0.864 |
| Number of vessels | 0.174 | 0.033 | 0.136 | 0.177 | 0.22 | 0.124 | 0.068 | 0.668 |
| Average vessel diameter | 0.05 | 0.543 | 0.066 | 0.514 | 0.109 | 0.45 | −0.256 | 0.102 |
| GCIPLT Associations | pwMS (n = 167) | pwRRMS (n = 113) | pwPMS (n = 54) | HCs (n = 48) | ||||
| Total vessel diameter | 0.112 | 0.172 | −0.013 | 0.893 | 0.387 | 0.007 | 0.111 | 0.462 |
| Number of vessels | 0.252 | 0.002 | 0.165 | 0.096 | 0.355 | 0.013 | 0.025 | 0.867 |
| Average vessel diameter | −0.152 | 0.063 | −0.155 | 0.119 | −0.07 | 0.636 | −0.071 | 0.641 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Young, N.; Zivadinov, R.; Dwyer, M.G.; Bergsland, N.; Weinstock-Guttman, B.; Jakimovski, D. Retinal Blood Vessel Analysis Using Optical Coherence Tomography (OCT) in Multiple Sclerosis. Diagnostics 2023, 13, 596. https://doi.org/10.3390/diagnostics13040596
Young N, Zivadinov R, Dwyer MG, Bergsland N, Weinstock-Guttman B, Jakimovski D. Retinal Blood Vessel Analysis Using Optical Coherence Tomography (OCT) in Multiple Sclerosis. Diagnostics. 2023; 13(4):596. https://doi.org/10.3390/diagnostics13040596
Chicago/Turabian StyleYoung, Nicholas, Robert Zivadinov, Michael G. Dwyer, Niels Bergsland, Bianca Weinstock-Guttman, and Dejan Jakimovski. 2023. "Retinal Blood Vessel Analysis Using Optical Coherence Tomography (OCT) in Multiple Sclerosis" Diagnostics 13, no. 4: 596. https://doi.org/10.3390/diagnostics13040596