
Diagnostic Ability of Endoscopic Ultrasound-Guided Tissue Acquisition Using 19-Gauge Fine-Needle Biopsy Needle for Abdominal Lesions

 , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Patients and Data Collection
2.3. EUS-TA Procedure
2.4. Histological Evaluation
2.5. Study Definitions
2.6. Statistical Analysis
3. Results
3.1. Patient Background Characteristics
3.2. Procedure Outcomes
3.3. Final Diagnosis
3.4. Clinical Outcomes
3.5. Adverse Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levine, I.; Trindade, A.J. Endoscopic ultrasound fine needle aspiration vs fine needle biopsy for pancreatic masses, subepithelial lesions, and lymph nodes. World J. Gastroenterol. 2021, 27, 4194–4207. [Google Scholar] [CrossRef] [PubMed]
- de Moura, D.T.H.; McCarty, T.R.; Jirapinyo, P.; Ribeiro, I.B.; Hathorn, K.E.; Madruga-Neto, A.C.; Lee, L.S.; Thompson, C.C. Evaluation of endoscopic ultrasound fine-needle aspiration versus fine-needle biopsy and impact of rapid on-site evaluation for pancreatic masses. Endosc. Int. Open 2020, 8, E738–E747. [Google Scholar] [CrossRef] [PubMed]
- Fujita, A.; Ryozawa, S.; Tanisaka, Y.; Ogawa, T.; Suzuki, M.; Katsuda, H.; Tashima, T.; Araki, R.; Mizuide, M. Evaluation of endoscopic ultrasound-guided fine-needle biopsy for preoperative pancreatic solid lesions. Scand. J. Gastroenterol. 2021, 56, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Kawashima, H.; Ohno, E.; Tanaka, H.; Sakai, D.; Iida, T.; Nishio, R.; Yamamura, T.; Furukawa, K.; Nakamura, M.; et al. Clinical impact of EUS-guided fine needle biopsy using a novel franseen needle for histological assessment of pancreatic diseases. Can. J. Gastroenterol. Hepatol. 2019, 2019, 8581743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naveed, M.; Siddiqui, A.A.; Kowalski, T.E.; Loren, D.E.; Khalid, A.; Soomro, A.; Mazhar, S.M.; Yoo, J.; Hasan, R.; Yalamanchili, S.; et al. A Multicenter comparative trial of a novel EUS-guided core biopsy needle (SharkCore™) with the 22-gauge needle in patients with solid pancreatic mass lesions. Endosc. Ultrasound. 2018, 7, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Irie, H.; Takagi, T.; Suzuki, R.; Konno, N.; Asama, H.; Sato, Y.; Nakamura, J.; Takasumi, M.; Hashimoto, M.; et al. Efficacy of EUS-guided FNB using a Franseen needle for tissue acquisition and microsatellite instability evaluation in unresectable pancreatic lesions. BMC Cancer 2020, 20, 1094. [Google Scholar] [CrossRef] [PubMed]
- Asokkumar, R.; Yung Ka, C.; Loh, T.; Kah Ling, L.; Gek San, T.; Ying, H.; Tan, D.; Khor, C.; Lim, T.; Soetikno, R. Comparison of tissue and molecular yield between fine-needle biopsy (FNB) and fine-needle aspiration (FNA): A randomized study. Endosc. Int. Open 2019, 7, E955–E963. [Google Scholar] [CrossRef]
- Cheng, B.; Zhang, Y.; Chen, Q.; Sun, B.; Deng, Z.; Shan, H.; Dou, L.; Wang, J.; Li, Y.; Yang, X.; et al. Analysis of fine-needle biopsy vs fine-needle aspiration in diagnosis of pancreatic and abdominal masses: A prospective, multicenter, randomized controlled trial. Clin. Gastroenterol. Hepatol. 2018, 16, 1314–1321. [Google Scholar] [CrossRef]
- Kandel, P.; Nassar, A.; Gomez, V.; Raimondo, M.; Woodward, T.A.; Crook, J.E.; Fares, N.S.; Wallace, M.B. Comparison of endoscopic ultrasound-guided fine-needle biopsy versus fine-needle aspiration for genomic profiling and DNA yield in pancreatic cancer: A randomized crossover trial. Endoscopy 2021, 53, 376–382. [Google Scholar] [CrossRef]
- Matsuno, J.; Ogura, T.; Kurisu, Y.; Miyano, A.; Imanishi, M.; Onda, S.; Okuda, A.; Nishioka, N.; Higuchi, K. Prospective comparison study of franseen needle and standard needle use for pancreatic lesions under EUS guidance. Endosc. Ultrasound 2019, 8, 412–417. [Google Scholar] [CrossRef]
- Li, D.F.; Wang, J.Y.; Yang, M.F.; Xiong, F.; Zhang, D.G.; Xu, Z.L.; Luo, M.H.; Jing, Z.D.; Wang, K.X.; Wang, L.S.; et al. Factors associated with diagnostic accuracy, technical success and adverse events of endoscopic ultrasound-guided fine-needle biopsy: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 1264–1276. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, J.; Kocjan, G.; Sgouros, S.N.; Deheragoda, M.; Pereira, S.P. Endoscopic ultrasound-guided tissue sampling by combined fine needle aspiration and trucut needle biopsy: A prospective study. Cytopathology 2006, 17, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Itoi, T.; Itokawa, F.; Sofuni, A.; Nakamura, K.; Tsuchida, A.; Yamao, K.; Kawai, T.; Moriyasu, F. Puncture of solid pancreatic tumors guided by endoscopic ultrasonography: A pilot study series comparing Trucut and 19-gauge and 22-gauge aspiration needles. Endoscopy 2005, 37, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Ginès, A.; Wiersema, M.J.; Clain, J.E.; Pochron, N.L.; Rajan, E.; Levy, M.J. Prospective study of a trucut needle for performing EUS-guided biopsy with EUS-guided FNA rescue. Gastrointest. Endosc. 2005, 62, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Hebert-Magee, S.; Trevino, J.; Ramesh, J.; Varadarajulu, S. Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions. Gastrointest. Endosc. 2012, 76, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Vanbiervliet, G.; Napoléon, B.; Saint Paul, M.C.; Sakarovitch, C.; Wangermez, M.; Bichard, P.; Subtil, C.; Koch, S.; Grandval, P.; Gincul, R.; et al. Core needle versus standard needle for endoscopic ultrasound-guided biopsy of solid pancreatic masses: A randomized crossover study. Endoscopy 2014, 46, 1063–1070. [Google Scholar] [CrossRef]
- Lee, Y.N.; Moon, J.H.; Kim, H.K.; Choi, H.J.; Choi, M.H.; Kim, D.C.; Lee, T.H.; Cha, S.W.; Cho, Y.D.; Park, S.H. Core biopsy needle versus standard aspiration needle for endoscopic ultrasound-guided sampling of solid pancreatic masses: A randomized parallel-group study. Endoscopy 2014, 46, 1056–1062. [Google Scholar] [CrossRef]
- Aadam, A.A.; Wani, S.; Amick, A.; Shah, J.N.; Bhat, Y.M.; Hamerski, C.M.; Klapman, J.B.; Muthusamy, V.R.; Watson, R.R.; Rademaker, A.W.; et al. A randomized controlled cross-over trial and cost analysis comparing endoscopic ultrasound fine needle aspiration and fine needle biopsy. Endosc. Int. Open 2016, 4, E497–E505. [Google Scholar] [CrossRef] [Green Version]
- Imaoka, H.; Sasaki, M.; Hashimoto, Y.; Watanabe, K.; Ikeda, M. New Era of endoscopic ultrasound-guided tissue acquisition: Next-generation sequencing by endoscopic ultrasound-guided sampling for pancreatic cancer. J. Clin. Med. 2019, 8, 1173. [Google Scholar] [CrossRef] [Green Version]
- van Riet, P.A.; Larghi, A.; Attili, F.; Rindi, G.; Nguyen, N.Q.; Ruszkiewicz, A.; Kitano, M.; Chikugo, T.; Aslanian, H.; Farrell, J.; et al. A multicenter randomized trial comparing a 25-gauge EUS fine-needle aspiration device with a 20-gauge EUS fine-needle biopsy device. Gastrointest. Endosc. 2019, 89, 329–339. [Google Scholar] [CrossRef]
- Ashat, M.; Klair, J.S.; Rooney, S.L.; Vishal, S.J.; Jensen, C.; Sahar, N.; Murali, A.R.; El-Abiad, R.; Gerke, H. Randomized controlled trial comparing the Franseen needle with the Fork-tip needle for EUS-guided fine-needle biopsy. Gastrointest. Endosc. 2021, 93, 140–150.e2. [Google Scholar] [CrossRef] [PubMed]
- Mohan, B.P.; Shakhatreh, M.; Garg, R.; Asokkumar, R.; Jayaraj, M.; Ponnada, S.; Navaneethan, U.; Adler, D.G. Comparison of Franseen and fork-tip needles for EUS-guided fine-needle biopsy of solid mass lesions: A systematic review and meta-analysis. Endosc. Ultrasound. 2019, 8, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Miyoshi, J.; Toki, M.; Kambayashi, K.; Kitada, S.; Nosaka, T.; Goto, T.; Ota, H.; Ochiai, K.; Gondo, K.; et al. Effectiveness of introducing a 20-gauge core biopsy needle with a core trap in EUS-FNA/B for diagnosing pancreatic cancer. BMC Gastroenterol. 2021, 21, 8. [Google Scholar] [CrossRef]
- Karsenti, D.; Tharsis, G.; Zeitoun, J.D.; Denis, P.; Perrot, B.; Coelho, J.; Bellaiche, G.; Charbit, L.; Hakoune, J.J.; Doumet, S.; et al. Comparison of 20-gauge Procore® and 22-gauge Acquire® needles for EUS-FNB of solid pancreatic masses: An observational study. Scand. J. Gastroenterol. 2019, 54, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yasuda, I.; Hanaoka, T.; Hayashi, Y.; Motoo, I.; Kajiura, S.; Ando, T.; Fujinami, H.; Tajiri, K.; Imura, J.; et al. Comparison of histological sample volumes among various endoscopic ultrasound-guided biopsy needles. J. Clin. Med. 2021, 10, 3560. [Google Scholar] [CrossRef]
- Iwashita, T.; Nakai, Y.; Mukai, T.; Togawa, O.; Matsubara, S.; Hatano, Y.; Hara, A.; Tanaka, M.; Shibahara, J.; Fukayama, M.; et al. A 19-gauge histology needle versus a 19-gauge standard needle in endoscopic ultrasound-guided fine-needle aspiration for solid lesions: A multicenter randomized comparison study (GREATER study). Dig. Dis. Sci. 2018, 63, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Ching-Companioni, R.A.; Diehl, D.L.; Johal, A.S.; Confer, B.D.; Khara, H.S. 19 G aspiration needle versus 19 G core biopsy needle for endoscopic ultrasound-guided liver biopsy: A prospective randomized trial. Endoscopy 2019, 51, 1059–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeWitt, J.; Cho, C.M.; Lin, J.; Al-Haddad, M.; Canto, M.I.; Salamone, A.; Hruban, R.H.; Messallam, A.A.; Khashab, M.A. Comparison of EUS-guided tissue acquisition using two different 19-gauge core biopsy needles: A multicenter, prospective, randomized, and blinded study. Endosc. Int. Open 2015, 3, E471–E478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.K.; Lee, J.H.; Noh, D.H.; Park, J.K.; Lee, K.T.; Lee, J.K.; Lee, K.H.; Jang, K.T.; Cho, J. Factors of endoscopic ultrasound-guided tissue acquisition for successful next-generation sequencing in pancreatic ductal adenocarcinoma. Gut Liver. 2020, 14, 387–394. [Google Scholar] [CrossRef] [Green Version]
- Larson, B.K.; Tuli, R.; Jamil, L.H.; Lo, S.K.; Deng, N.; Hendifar, A.E. Utility of endoscopic ultrasound-guided biopsy for next-generation sequencing of pancreatic exocrine malignancies. Pancreas 2018, 47, 990–995. [Google Scholar] [CrossRef]
- Ikeda, G.; Hijioka, S.; Nagashio, Y.; Maruki, Y.; Ohba, A.; Hisada, Y.; Yoshinari, M.; Harai, S.; Kitamura, H.; Koga, T.; et al. Fine-needle biopsy with 19G needle is effective in combination with endoscopic ultrasound-guided tissue acquisition for genomic profiling of unresectable pancreatic cancer. Dig. Endosc. 2022, 35, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Attili, F.; Fabbri, C.; Yasuda, I.; Fuccio, L.; Palazzo, L.; Tarantino, I.; Dewitt, J.; Frazzoni, L.; Rimbaş, M.; Larghi, A. Low diagnostic yield of transduodenal endoscopic ultrasound-guided fine needle biopsy using the 19-gauge Flex needle: A large multicenter prospective study. Endosc. Ultrasound 2017, 6, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Laquière, A.; Lefort, C.; Maire, F.; Aubert, A.; Gincul, R.; Prat, F.; Grandval, P.; Croizet, O.; Boulant, J.; Vanbiervliet, G.; et al. 19 G nitinol needle versus 22 G needle for transduodenal endoscopic ultrasound-guided sampling of pancreatic solid masses: A randomized study. Endoscopy 2019, 51, 436–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawa, S.; Kamisawa, T.; Notohara, K.; Fujinaga, Y.; Inoue, D.; Koyama, T.; Okazaki, K. Japanese clinical diagnostic criteria for autoimmune pancreatitis, 2018: Revision of Japanese clinical diagnostic criteria for autoimmune pancreatitis, 2011. Pancreas 2020, 49, e13–e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcek, A.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef]
- Song, T.J.; Kim, J.H.; Lee, S.S.; Eum, J.B.; Moon, S.H.; Park, D.Y.; Seo, D.W.; Lee, S.K.; Jang, S.J.; Yun, S.C.; et al. The prospective randomized, controlled trial of endoscopic ultrasound-guided fine-needle aspiration using 22G and 19G aspiration needles for solid pancreatic or peripancreatic masses. Am. J. Gastroenterol. 2010, 105, 1739–1745. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Garcia, J.; Poley, J.W.; Larghi, A.; Giovannini, M.; Petrone, M.C.; Abdulkader, I.; Monges, G.; Costamagna, G.; Arcidiacono, P.; Biermann, K.; et al. Feasibility and yield of a new EUS histology needle: Results from a multicenter, pooled, cohort study. Gastrointest. Endosc. 2011, 73, 1189–1196. [Google Scholar] [CrossRef]
- Iwashita, T.; Yasuda, I.; Mukai, T.; Doi, S.; Nakashima, M.; Uemura, S.; Mabuchi, M.; Shimizu, M.; Hatano, Y.; Hara, A.; et al. Macroscopic on-site quality evaluation of biopsy specimens to improve the diagnostic accuracy during EUS-guided FNA using a 19-gauge needle for solid lesions: A single-center prospective pilot study (MOSE study). Gastrointest. Endosc. 2015, 81, 177–185. [Google Scholar] [CrossRef]
- Hann, A.; Epp, S.; Veits, L.; Rosien, U.; Siegel, J.; Möschler, O.; Bohle, W.; Meining, A. Multicenter, randomized comparison of the diagnostic accuracy of 19-gauge stainless steel and nitinol-based needles for endoscopic ultrasound-guided fine-needle biopsy of solid pancreatic masses. United Eur. Gastroenterol. J. 2020, 8, 314–320. [Google Scholar] [CrossRef] [Green Version]
- de Nucci, G.; Petrone, M.C.; Imperatore, N.; Forti, E.; Grassia, R.; Giovanelli, S.; Ottaviani, L.; Mirante, V.; Sabatino, G.; Fabbri, C.; et al. Feasibility and accuracy of transduodenal endoscopic ultrasound-guided fine-needle aspiration of solid lesions using a 19-gauge flexible needle: A multicenter study. Clin. Endosc. 2021, 54, 229–235. [Google Scholar] [CrossRef]
- Hisada, Y.; Hijioka, S.; Ikeda, G.; Maehara, K.; Hashimoto, T.; Kitamura, H.; Harai, S.; Yoshinari, M.; Kawasaki, Y.; Murashima, Y.; et al. Proportion of unresectable pancreatic cancer specimens obtained by endoscopic ultrasound-guided tissue acquisition meeting the OncoGuide™ NCC Oncopanel System analysis suitability criteria: A single-arm, phase II clinical trial. J. Gastroenterol. 2022, 57, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Kanno, A.; Yasuda, I.; Irisawa, A.; Hara, K.; Ashida, R.; Iwashita, T.; Takenaka, M.; Katanuma, A.; Takikawa, T.; Kubota, K.; et al. Adverse events of endoscopic ultrasound-guided fine-needle aspiration for histologic diagnosis in Japanese tertiary centers: Multicenter retrospective study. Dig. Endosc. 2021, 33, 1146–1157. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | N = 147 Cases (160 Lesions) | |
|---|---|---|
| Median age, year (range) | 70 | (15–92) |
| Sex, male (%) | 81/147 | (55.1%) |
| Objects (%) | N = 160 lesions | |
| Pancreas | 122/160 | (76.3%) |
| Liver | 18/160 | (11.3%) |
| Lymph node | 17/160 | (10.6%) |
| Others | 3/160 | (1.9%) |
| Median diameter of the object, mm (range) | 30 | (7.4–100) |
| The lesion of the pancreas (%) | N = 122 lesions | |
| Head | 41/122 | (33.6%) |
| Body or tail | 81/122 | (66.4%) |
| Preprocedural diagnosis (%) | N = 160 lesions | |
| Malignancy | 143/160 | (89.4%) |
| Benign | 3/160 | (1.9%) |
| Indeterminate | 14/160 | (8.8%) |
| Procedure Details | 160 Lesions | |
|---|---|---|
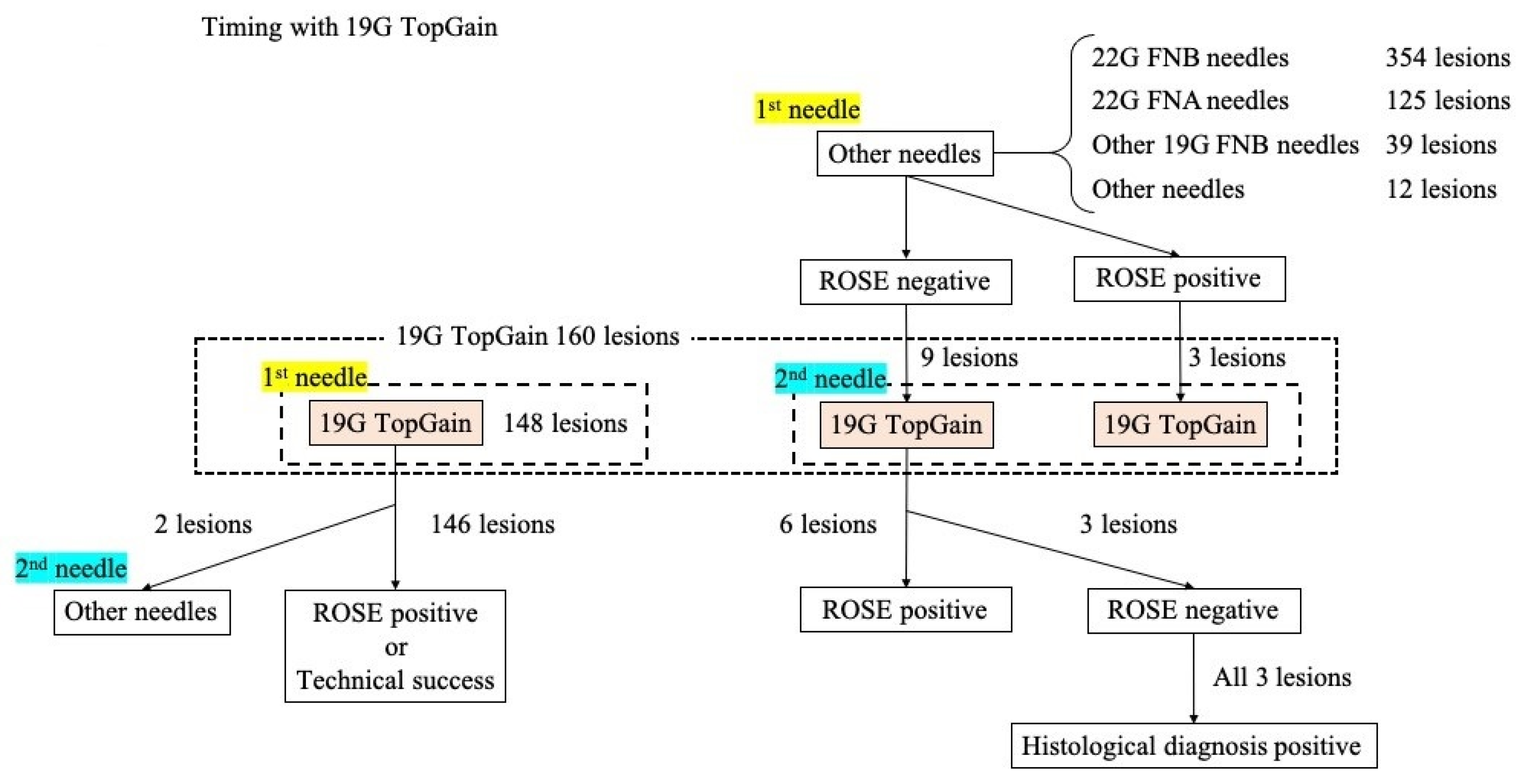
| 19G TopGain as the first needle (%) | 148 | (92.5%) |
| 19G TopGain as the second needle (%) | 12 | (7.5%) |
| First needle: 22G SharkCore (%) | 11/12 | (91.7%) |
| First needle: 22G TopGain (%) | 1/12 | (8.3%) |
| Puncture site (%) | ||
| Stomach | 118 | (73.8%) |
| Duodenum | 38 | (23.8%) |
| Stomach and duodenum | 3 | (1.9%) |
| Jejunum | 1 | (0.6%) |
| Median number of punctures per lesion (range) | 3 | (0–6) |
| Suction, slow pull (%) | 160 | (100%) |
| Rapid on-site evaluation (%) | 160 | (100%) |
| Clinical and Histological Diagnosis | 160 Lesions | |
|---|---|---|
| Malignant lesion (%) | 150 | (93.8%) |
| Benign lesion (%) | 7 | (4.4%) |
| Indeterminate lesion (%) | 3 | (1.9%) |
| Target organ (%) | ||
| Pancreas | 122/160 | (76.3%) |
| Adenocarcinoma | 96 | (78.7%) |
| Adenosquamous carcinoma | 6 | (4.9%) |
| Neuroendocrine tumor | 6 | (4.9%) |
| Neuroendocrine carcinoma | 4 | (3.3%) |
| Intraductal papillary mucinous carcinoma | 1 | (0.8%) |
| Acinar cell carcinoma | 1 | (0.8%) |
| Malignant lymphoma | 1 | (0.8%) |
| Autoimmune pancreatitis | 4 | (3.3%) |
| Normal pancreatic tissue | 1 | (0.8%) |
| Indeterminate lesion | 2 | (1.6%) |
| Liver | 18/160 | (11.3%) |
| Pancreatic ductal adenocarcinoma | 6 | (33.3%) |
| Cholangiocellular carcinoma | 5 | (27.8%) |
| Pancreatic adenosquamous carcinoma | 2 | (11.1%) |
| Mixed neuroendocrine non-neuroendocrine neoplasm of the pancreas | 2 | (11.1%) |
| Carcinoma of the bile duct | 1 | (5.6%) |
| Neuroendocrine tumor of the pancreas | 1 | (5.6%) |
| Indeterminate lesion | 1 | (5.6%) |
| Lymph node | 17/160 | (10.6%) |
| Malignant lymphoma | 4 | (23.5%) |
| Cholangiocellular carcinoma | 3 | (17.6%) |
| Pancreatic ductal adenocarcinoma | 3 | (17.6%) |
| Neuroendocrine carcinoma of the pancreas | 2 | (11.8%) |
| Carcinoma of the bile duct | 1 | (5.9%) |
| Neuroendocrine tumor of the pancreas | 1 | (5.9%) |
| Mixed neuroendocrine non-neuroendocrine neoplasm of the pancreas | 1 | (5.9%) |
| Carcinoma of the gallbladder | 1 | (5.9%) |
| Small cell lung carcinoma | 1 | (5.9%) |
| Abdominal mass | 2/160 | (1.3%) |
| Pancreatic adenosquamous carcinoma | 1 | (50%) |
| Desmoid fibrosis | 1 | (50%) |
| Submucosal tumor | 1/160 | (0.6%) |
| Brunner’s glands | 1 | (100%) |
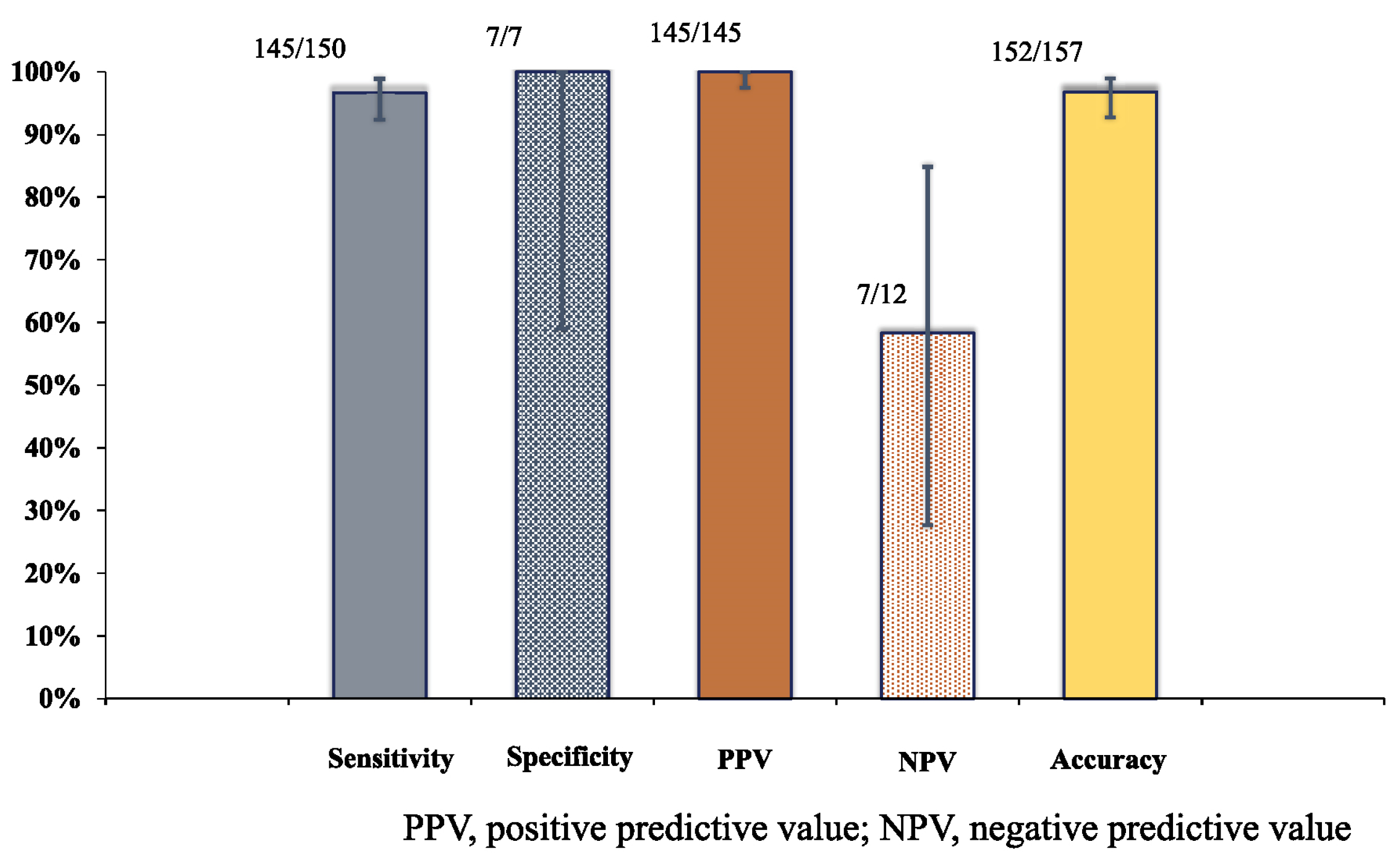
| Final Diagnosis | Total | |||
|---|---|---|---|---|
| Malignancy | Benign | |||
| EUS-FNA outcome | Malignancy | 145 | 0 | 145 |
| Benign | 5 | 7 | 12 | |
| Total | 150 | 7 | 157 | |
| Clinical Outcomes | N = 147 Cases (160 Lesions) | |
|---|---|---|
| Technical success (%) | 159/160 | (99.4%) |
| Technical success with only TopGain19G(%) | 146/148 | (98.6%) |
| Adverse events during the procedure (%) | 0/146 | (0%) |
| Early adverse events (%) | 6/146 | (4.1%) |
| Bleeding | 2/6 | (33.3%) |
| Infection | 2/6 | (33.3%) |
| Pancreatitis | 1/6 | (16.7%) |
| Aspiration pneumonia | 1/6 | (16.7%) |
| Late adverse events (%) | 0/146 | (0%) |
| Success of CGP analysis | 24/24 | (100%) |
| Case | Object | Diameter (mm) | Preprocedural Diagnosis | Puncture Site | Puncture by the First Needle | Rescue Puncture by TopGain19G | Final Diagnosis | |||
|---|---|---|---|---|---|---|---|---|---|---|
| The Type of the First Needle | The Number of Punctures | ROSE (Papanicolaou Classification) | The Number of Punctures | ROSE (Papanicolaou Classification) | ||||||
| 1 | Panc head | 24.7 | PDAC | duodenum | FNB 22G | 3 | 1 | 2 | 5 | PDAC |
| 2 | Panc body~tail | 7.4 | NET | stomach | FNB 22G | 3 | 1 | 1 | 3 | NET |
| 3 | Panc body~tail | 24.6 | PDAC | stomach | FNB 22G | 4 | 1 | 1 | 1 | PDAC |
| 4 | Panc body~tail | 8.9 | NET | stomach | FNB 22G | 3 | inadequate | 3 | 3 | NET |
| 5 | Panc body~tail | 17.6 | NET | stomach | FNB 22G | 2 | inadequate | 1 | 3 | No tumor seen |
| 6 | Panc body~tail | 13.5 | PDAC | stomach | FNB 22G | 4 | 3 | 1 | 3 | PDAC |
| 7 | Panc body~tail | 8.1 | NET | stomach | FNB 22G | 4 | 1 | 1 | 1 | Benign |
| 8 | Abdominal mass | 24.4 | Not diagnosed | duodenum | FNB 22G | 3 | 2 | 2 | 2 (stromal cell) | Desmoid fibrosis |
| 9 | Panc head | 20 | PDAC | stomach | FNB 22G | 5 | 1 | 2 | 5 | PDAC |
| Literatures | Design | Cases | Type of Needle | Material Used in the Needle | Diagnostic Accuracy | Technical Success | Adverse Events |
|---|---|---|---|---|---|---|---|
| [36] | Prospective randomized | 60 | FNA/19G (ECHO19, COOK) | stainless | 86.7% | 91.7% | 0% |
| 57 | FNA/22G (ECHO22, COOK) | 78.9% | 100% | 4.6% | |||
| [37] | Prospective, single-arm | 114 | FNB/19G (Procore, COOK) | stainless | 92.9% | 98.2% | 0% |
| [28] | Prospective randomized | 44 | FNB/19G (Procore, COOK) | stainless | 88% | 94% | 13% |
| 41 | FNB/19G (Quick-Core, COOK) | stainless | 62% | 86% | 16% | ||
| [38] | Prospective, single-arm | 111 | FNA/19G (Echotip, COOK) | stainless | 95.5% | 99.1% | 0% |
| [32] | Prospective, single-arm | 246 | FNA/19G (Expect19 Flex, Boston) | Nitinol | 73.6% | 92.7% | 2.4% |
| [26] | Prospective randomized | 55 | FNB/19G (Procore, COOK) | stainless | 90% | 98.2% | 3.6% |
| 55 | FNA/19G (Echotip, COOK) | stainless | 79.1% | 97.3% | |||
| [39] | Prospective randomized, crossover | 46 | FNA/19G (EZ shot3 plus, Olympus) | nitinol | 68% | 100% | 4.3% |
| FNA/19G (EZ shot2, Olympus) | stainless | 66% | 93.4% | ||||
| [33] | Prospective randomized | 59 | FNA/19G (Expect19 Flex, Boston) | nitinol | 69.5% | 86.4% | 15% |
| 63 | FNA/22G (various) | various | 87.3% | 100% | 8% | ||
| [40] | Retrospective, single-arm | 88 | FNA/19G (Expect slimline flex Boston) | Nitinol | 92.9% | 100% | 0% |
| 113 | FNA/19G (Expect, Boston) | Cobalt chromium | 94.4% | ||||
| Present study | Retrospective, single-arm | 160 | FNB/19G (TopGain, Medico’s HIRATA) | stainless | 96.8% | 99.4% | 4.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeshita, K.; Hijioka, S.; Nagashio, Y.; Maruki, Y.; Kawasaki, Y.; Maehara, K.; Murashima, Y.; Okada, M.; Ikeda, G.; Yamada, N.; et al. Diagnostic Ability of Endoscopic Ultrasound-Guided Tissue Acquisition Using 19-Gauge Fine-Needle Biopsy Needle for Abdominal Lesions. Diagnostics 2023, 13, 450. https://doi.org/10.3390/diagnostics13030450
Takeshita K, Hijioka S, Nagashio Y, Maruki Y, Kawasaki Y, Maehara K, Murashima Y, Okada M, Ikeda G, Yamada N, et al. Diagnostic Ability of Endoscopic Ultrasound-Guided Tissue Acquisition Using 19-Gauge Fine-Needle Biopsy Needle for Abdominal Lesions. Diagnostics. 2023; 13(3):450. https://doi.org/10.3390/diagnostics13030450
Chicago/Turabian StyleTakeshita, Kotaro, Susumu Hijioka, Yoshikuni Nagashio, Yuta Maruki, Yuki Kawasaki, Kosuke Maehara, Yumi Murashima, Mao Okada, Go Ikeda, Natsumi Yamada, and et al. 2023. "Diagnostic Ability of Endoscopic Ultrasound-Guided Tissue Acquisition Using 19-Gauge Fine-Needle Biopsy Needle for Abdominal Lesions" Diagnostics 13, no. 3: 450. https://doi.org/10.3390/diagnostics13030450