
Role of Inferior Vena Cava (IVC) Recanalization in Patients with Back Pain, Secondary to IVC Obstruction in Budd–Chiari Syndrome
 , ,
, ,
Abstract
:1. Introduction
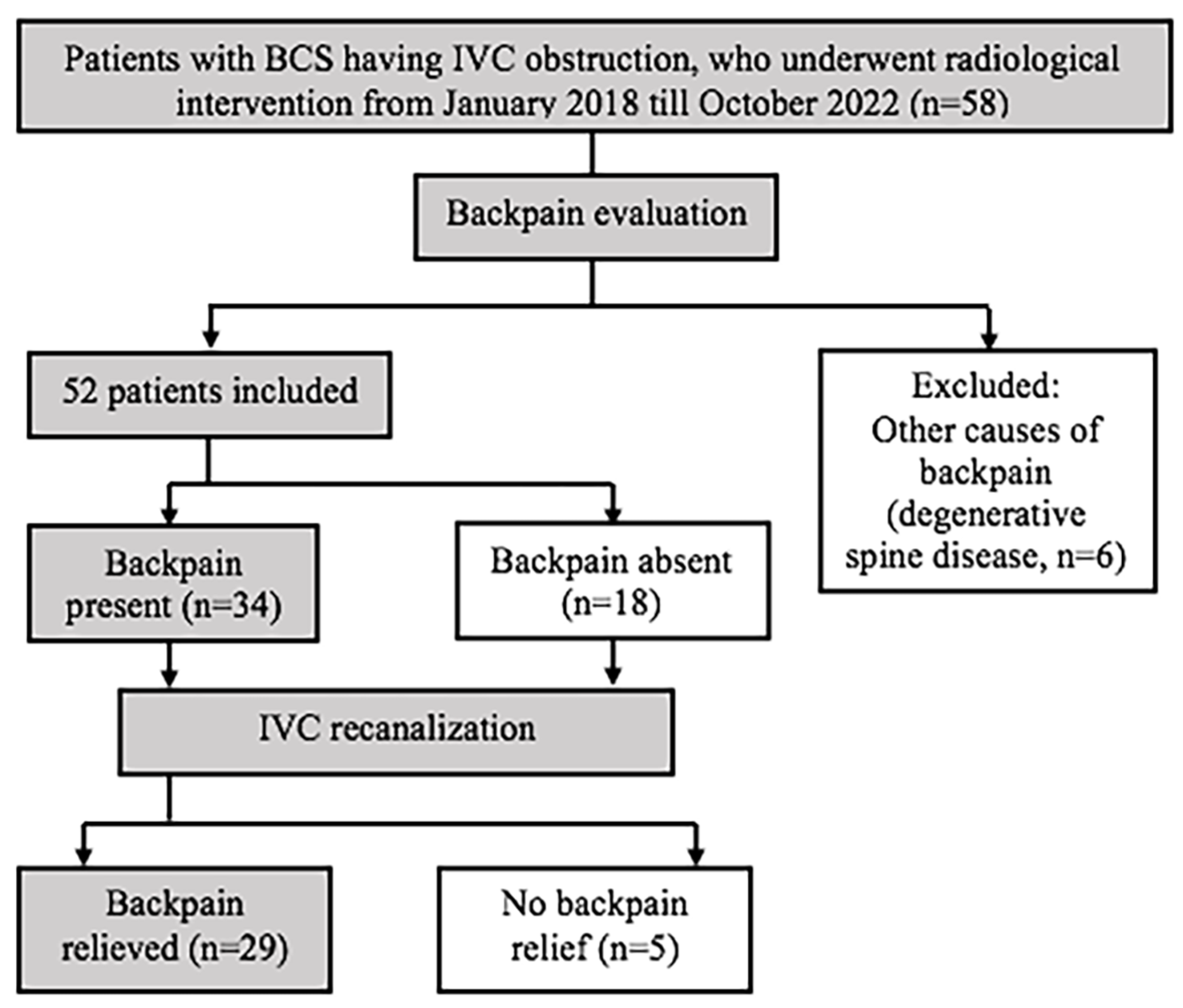
2. Methodology
2.1. Inclusion Criteria
2.2. Exclusion Criteria
Patients Lost to Follow Up
2.3. Statistical Analysis
3. Results
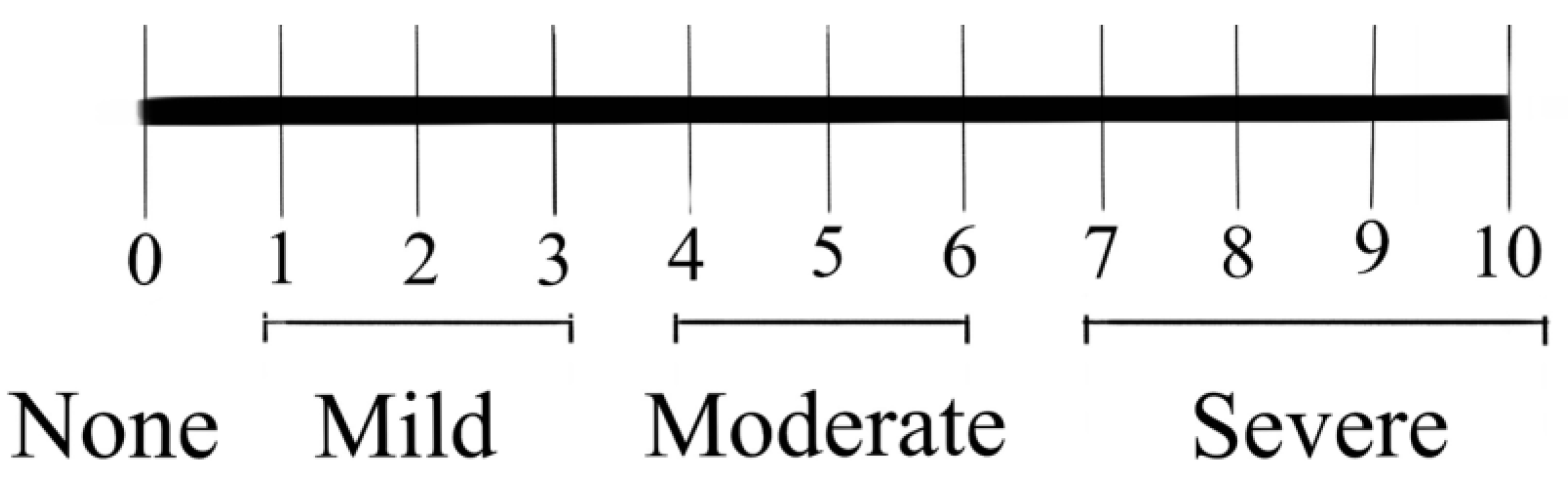
Evaluation of Back Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grus, T.; Lambert, L.; Grusová, G.; Banerjee, R.; Burgetová, A. Budd-Chiari Syndrome. Prague Med. Rep. 2017, 118, 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukund, A.; Gamanagatti, S. Imaging and Interventions in Budd-Chiari Syndrome. World J. Radiol. 2011, 3, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Song, W.J.; Kang, K.C. Myelopathy-mimicking symptoms of epidural venous engorgement and syringomyelia due to inferior vena cava stenosis at the thoracolumbar junction in a patient with Budd-Chiari syndrome. J. Neurosurg. Spine 2015, 23, 467–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukund, A.; Sarin, S.K. Budd–Chiari syndrome: A focussed and collaborative approach. Hepatol. Int. 2018, 12, 483–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukund, A.; Mittal, K.; Mondal, A.; Sarin, S.K. Anatomic Recanalization of Hepatic Vein and Inferior Vena Cava versus Direct Intrahepatic Portosystemic Shunt Creation in Budd-Chiari Syndrome: Overall Outcome and Midterm Transplant-Free Survival. J. Vasc. Interv. Radiol. 2018, 29, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Paksoy, Y.; Gormus, N. Epidural Venous Plexus Enlargements Presenting with Radiculopathy and Back Pain in Patients with Inferior Vena Cava Obstruction or Occlusion. Spine 2004, 29, 2419–2424. [Google Scholar] [CrossRef] [PubMed]
- Dudeck, O.; Zeile, M.; Poellinger, A.; Kluhs, L.; Ludwig, W.D.; Hamm, B. Epidural Venous Enlargements Presenting with Intractable Lower Back Pain and Sciatica in a Patient with Absence of the Infrarenal Inferior Vena Cava and Bilateral Deep Venous Thrombosis. Spine 2007, 32, E688–E691. [Google Scholar] [CrossRef] [PubMed]
- Mohit, A.A.; Fisher, D.J.; Matthews, D.C.; Hoffer, E.; Avellino, A.M. Inferior vena cava thrombosis causing acute cauda equina syndrome: Case report. J. Neurosurg. Pediatr. 2006, 104, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, G.; Çil, B.; Akbay, A.; Türk, C.Ç.; Palaoğlu, S. Intractable Radicular and Low Back Pain Secondary Inferior Vena Cava Stenosis Associated with Budd-Chiari Syndrome: Endovascular Treatment with Cava Stenting: Case Report and Review of the Literature. Spine 2006, 31, E383–E386. [Google Scholar] [CrossRef] [PubMed]
- Hallan, D.R.; McNutt, S.; Reiter, G.T.; Thamburaj, K.; Specht, C.S.; Knaub, M. Dilated Epidural Venous Plexus Causing Radiculopathy: A Report of 2 Cases and Review of the Literature. World Neurosurg. 2020, 144, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Tabatabai, M.A.W.; Butros, V.M.; Mahdi, S.A.; Ahmad, M.J. Severe low back pain as the initial symptom of venous thrombosis of the inferior vena cava. Case Rep. 2014, 2014, bcr2014205259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, D.Z.; Hughes, J.D.; Liebo, G.B.; Bendel, E.C.; Bjarnason, H.; Klaas, J.P. Venous Congestive Myelopathy due to Chronic Inferior Vena Cava Thrombosis Treated with Endovascular Stenting: Case Report and Review of the Literature. J. Vasc. Interv. Neurol. 2015, 8, 49–53. [Google Scholar] [PubMed]
- Kamerath, J.; Morgan, W.E. Absent inferior vena cava resulting in exercise-induced epidural venous plexus congestion and lower extremity numbness: A case report and review of the literature. Spine 2010, 35, E921–E924. [Google Scholar] [CrossRef] [PubMed]
- Donmez, F.Y. Epidural Venous Plexus Engorgement: What Lies Beneath? Case Rep. Radiol. 2015, 2015, 965106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, K.; Reddy, V.; Hogg, J.P. Neuroanatomy, Spinal Cord Veins. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK542182/ (accessed on 22 February 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of patients (n) | 58 | |||
| Age [range, mean (SD)] | 11 years to 75 years, 36.9 years (13.3 years) | |||
| Sex | Male—38 Female—20 | |||
| Cause of IVC obstruction | Acute thrombosis—3 Chronic stenosis / obstruction—25 Membranous obstruction—21 Caudate lobe hypertrophy—7 Stent related—2 | |||
| Level of IVC obstruction | Suprahepatic—40 Intrahepatic—8 Multisegmental—10 | |||
| Length of IVC obstruction [mean (SD)] | 22.3 mm (27 mm) | |||
| Degree of luminal narrowing | Complete obstruction—39 Partial obstruction—19 | |||
| IVC recanalization | Angioplasty alone—47 Angioplasty with stenting—11 | |||
| Laboratory parameters [mean (SD)] | Pre-procedure | 1 month post-procedure | p-value | |
| Serum bilirubin | 1.9 (1.5) mg/dL | 1.2 (0.4) mg/dL | <0.001 | |
| AST | 156.8 (860.4) U/L | 44.9 (101.1) U/L | 0.327 | |
| ALT | 55.5 (196.7) U/L | 35.9 (60.4) U/L | 0.470 | |
| Characteristics | Back Pain | No Back Pain | |
|---|---|---|---|
| Age | Mean (SD)—34.3 (10.6) | Mean (SD)—34.1 (12.4) | p = 0.928 |
| Sex | M—20 F—14 | M—14 F—4 | p = 0.227 |
| Type of IVC obstruction | Acute—2 Chronic—32 | Acute—1 Chronic—17 | p = 1.000 |
| Length of IVC obstruction (mean (SD)) | Mean (SD)—21 mm (25 mm) | Mean (SD)—23.8 mm (28.5 mm) | p = 0.714 |
| Degree of luminal narrowing | Complete—26 Partial—8 | Complete—8 Partial—10 | p = 0.021 |
| EVEs | Present—30 Absent—4 | Present—8 Absent—10 | p = 0.002 |
| IVC recanalization | Angioplasty alone—25 Angioplasty + stenting—9 | Angioplasty alone—17 Angioplasty + stenting—1 |
| Characteristics | Pain Relief Present | No Pain Relief | |
|---|---|---|---|
| Age | Mean (SD)—35.2 (11) | Mean (SD)—29.6 (6.9) | p = 0.286 |
| Sex | M—18 F—11 | M—2 F—3 | p = 0.627 |
| Type of IVC obstruction | Acute—2 Chronic—27 | Acute—0 Chronic—5 | p = 1.000 |
| Length of IVC obstruction (mean (SD)) | Mean (SD)—21.8 mm (26.2 mm) | Mean (SD)—16.1 mm (18.1 mm) | p = 0.641 |
| Degree of luminal narrowing | Complete—23 Partial—6 | Complete—3 Partial—2 | p = 0.570 |
| EVEs | Present—28 Absent—1 | Present—2 Absent—3 | p < 0.001 |
| IVC recanalization | Angioplasty alone—21 Angioplasty + stenting—8 | Angioplasty alone—4 Angioplasty + stenting—1 |
| Year | Authors | Type of the Study | Location of IVC Obstruction | Cause | Presenting Features | Intervention | Results |
|---|---|---|---|---|---|---|---|
| 2004 | Paksoy and Gormus [6] | Retrospective review of 13 patients | Infrarenal IVC | IVC thrombosis in 10 patients IVC compression by gravid uterus in 2 patients IVC invasion by abdominal malignancy in 1 patient | Intractable low back and radicular pain | Venous thrombectomy in 2 patients with acute IVC thrombosis Anticoagulation in 8 patients with IVC thrombosis Timely delivery in 2 pregnant patients Untreated in patient with inoperable abdominal malignancy | Symptoms resolved in 12 treated patients |
| 2006 | Bozkurt et al. [9] | Case report | Hepatic IVC | Budd–Chiari syndrome—caudate lobe hypertrophy | Intractable low back and radicular pain | IVC stent | Symptoms resolved |
| 2006 | Mohit et al. [8] | Case report | Renal and Infrarenal IVC | IVC thrombosis | Intractable low back pain Lower extremity numbness and weakness | Mechanical thrombectomy and IVC balloon angioplasty Anticoagulation | Symptoms resolved |
| 2007 | Dudeck et al. [7] | Case report | Infrarenal IVC | Agenesis of infraranal IVC DVT of right common iliac vein | Intractable low back and radicular pain | Anticoagulation | Symptoms resolved |
| 2010 | Kamerath and Morgan [13] | Case report | Infrarenal IVC | Agenesis of infraranal IVC | Low back and radicular pain Exercise induced numbness in lower extremity Urinary and fecal incontinence | None | Not reported |
| 2014 | Tabatabai et al. [11] | Case report | Infrarenal IVC | IVC thrombosis | Intractable low back and radicular pain Lower limb and testicular swelling | Anticoagulation | Significant improvement of symptoms |
| 2015 | Lee et al. [3] | Case report | Hepatic IVC | Budd–Chiari syndrome—Chronic obstruction | Intractable low back and radicular pain Lower extremity weakness and voiding difficulty | IVC stent | Symptoms resolved |
| 2015 | Carvalho et al. [12] | Case report | Hepatic IVC | Chronic IVC obstruction | Low back pain Bilateral lower extremity weakness Urinary retention | IVC stent | Symptoms resolved |
| 2015 | Donmez [14] | Case report | Entire IVC | Thin IVC with absence of left common iliac vein | Intractable back pain | Prophylactic antithrombotic | Not reported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubihal, V.; Mukund, A.; Pandey, Y.; Vashistha, C.; Maiwall, R.; Patidar, Y.; Yadav, A.Y.; Koul, R.L.; Sarin, S.K. Role of Inferior Vena Cava (IVC) Recanalization in Patients with Back Pain, Secondary to IVC Obstruction in Budd–Chiari Syndrome. Diagnostics 2023, 13, 438. https://doi.org/10.3390/diagnostics13030438
Kubihal V, Mukund A, Pandey Y, Vashistha C, Maiwall R, Patidar Y, Yadav AY, Koul RL, Sarin SK. Role of Inferior Vena Cava (IVC) Recanalization in Patients with Back Pain, Secondary to IVC Obstruction in Budd–Chiari Syndrome. Diagnostics. 2023; 13(3):438. https://doi.org/10.3390/diagnostics13030438
Chicago/Turabian StyleKubihal, Vijay, Amar Mukund, Yasha Pandey, Chitranshu Vashistha, Rakhi Maiwall, Yashwant Patidar, Anil Yogendra Yadav, Roshan Lal Koul, and Shiv Kumar Sarin. 2023. "Role of Inferior Vena Cava (IVC) Recanalization in Patients with Back Pain, Secondary to IVC Obstruction in Budd–Chiari Syndrome" Diagnostics 13, no. 3: 438. https://doi.org/10.3390/diagnostics13030438