
Pylephlebitis: A Systematic Review on Etiology, Diagnosis, and Treatment of Infective Portal Vein Thrombosis

 , and
, and
Abstract
:1. Introduction
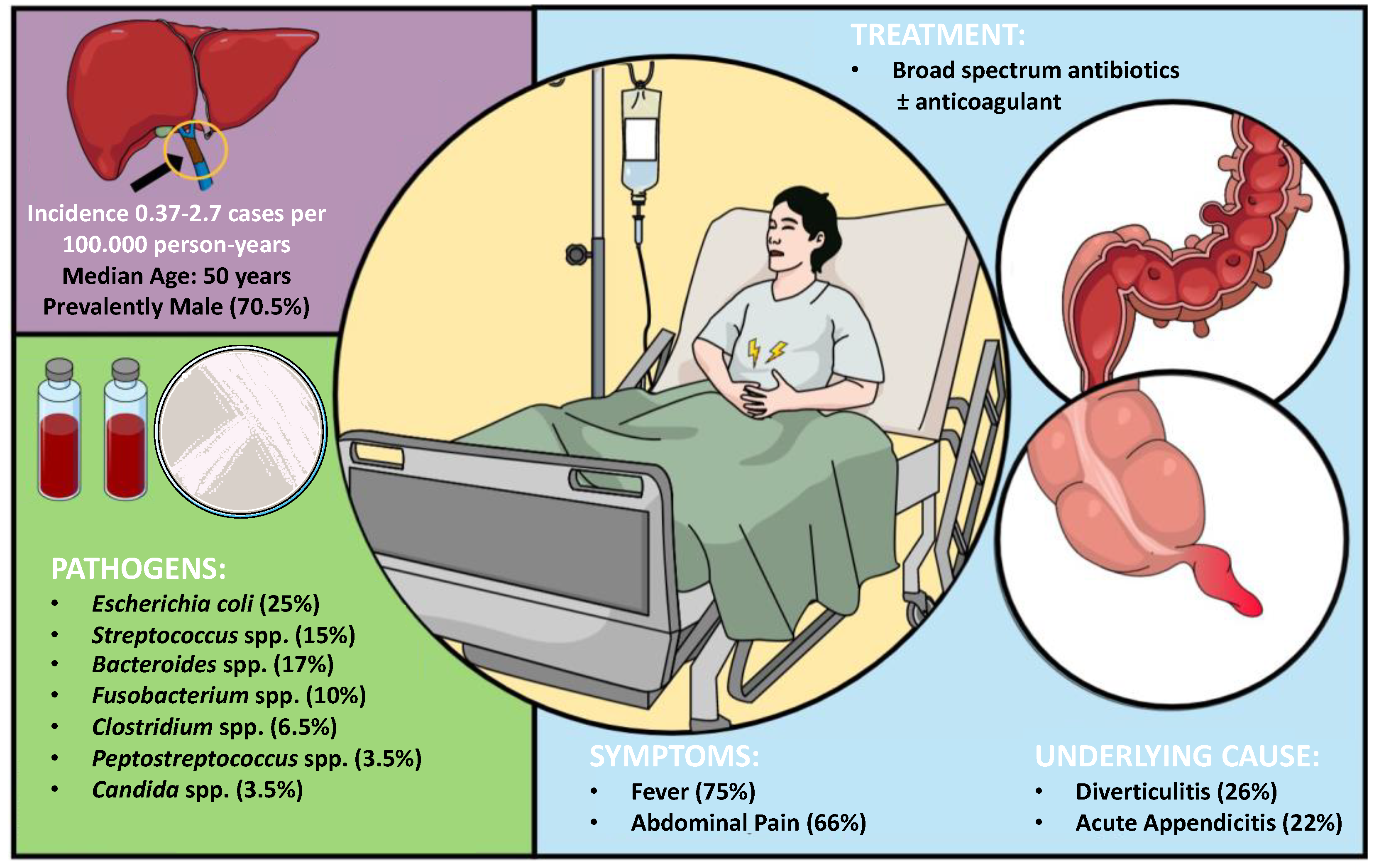
2. Epidemiology and Etiology
Microbiology
3. Clinical Manifestation
Laboratory Findings
4. Diagnosis
4.1. Pathogen Identification
4.2. Imaging Studies
5. Treatment
6. Complications and Mortality
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Osler, W. Case of Obliteration of the Portal Vein (Pylephlebitis Adhesiva). J. Anat. Physiol. 1882, 16, 208. [Google Scholar] [PubMed]
- Saxena, R.; Adolph, M.; Ziegler, J.R.; Murphy, W.; Rutecki, G.W. Pylephlebitis: A case report and review of outcome in the antibiotic era. Am. J. Gastroenterol. 1996, 91, 1251–1253. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Takahashi, H.; Sakata, I.; Adachi, Y. Treatment of portal vein septic thrombosis by infusion of antibiotics and an antifungal agent into portal vein and superior mesenteric artery: A case report. Hepatogastroenterology 2003, 50, 1133–1135. [Google Scholar]
- Mannaerts, L.; Bleeker-Rovers, C.P.; Koopman, M.; Punt, C.J.A.; Van Herpen, C.M.L. Pylephlebitis after a duodenal ulcer in a patient with metastasised colon carcinoma treated with chemotherapy and bevacizumab: A case report. Neth. J. Med. 2009, 67, 69–71. [Google Scholar] [PubMed]
- Chau, T.N.; Loke, T.K.L.; Leung, V.K.S.; Law, S.T.; Lai, M.H.Y.; Ho, Y.W. Hepatic portal venous gas complicating septic thrombophlebitis of the superior mesenteric vein. Hong Kong Med. J. 2007, 13, 69–72. [Google Scholar] [PubMed]
- van de Wauwer, C.; Irvin, T.T. Pylephlebitis due to perforated diverticulitis. Acta Chir. Belg. 2005, 105, 229–230. [Google Scholar] [CrossRef]
- Aggarwal, S.; Mathur, N.B.; Garg, A. Portal vein thrombosis complicating neonatal hepatic abscess. Indian Pediatr. 2003, 40, 997–1001. [Google Scholar]
- Pitcher, R.; McKenzie, C. Simultaneous ultrasound identification of acute appendicitis, septic thrombophlebitis of the portal vein and pyogenic liver abscess. South Afr. Med. J. 2003, 93, 426–428. [Google Scholar]
- Stitzenberg, K.B.; Piehl, M.D.; Monahan, P.E.; Phillips, J.D. Interval laparoscopic appendectomy for appendicitis complicated by pylephlebitis. J. Soc. Laparosc. Robot. Surg. 2006, 10, 108–113. [Google Scholar]
- de Jong, I.M.; Muller, M.C.A.; Peterson, G.M.; Polle, S.W. An uncommon cause of portal vein thrombosis. Neth. J. Med. 2013, 71, 431. [Google Scholar] [PubMed]
- Mailleux, P.; Maldague, P.; Coulier, B. Pylephlebitis complicating peridiverticulitis without hepatic abscess: Early detection with contrast-enhanced ct of the abdomen. J. Belg. Soc. Radiol. 2012, 95, 13–14. [Google Scholar] [CrossRef]
- Tulsidas, H.; Ong, Y.Y.; Chan, K.C. Aeromonas hydrophila bacteraemia and portal pyaemia. Singapore Med. J. 2008, 49, 346–348. [Google Scholar] [PubMed]
- Güz, G.; Yegyn, Z.A.; Dogan, I.; Kizel, K.; Bali, M.; Sindel, Ş. Portal vein thrombosis and liver abscess due to Lactococcus lactis. Turkis J. Gastroenterol. 2006, 17, 144–147. [Google Scholar]
- Ferkolj, I.; Vrh-Jermancic, J.; Štabuc, B. Fatal hemorrhage due to thrombosis and rupture of the portal vein and hepatic artery. Wien. Klin. Wochenschr. 2009, 121, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Muguruma, T.; Idoguchi, K.; Matsuoka, T. Percutaneous drainage for suppurative pylethrombophlebitis developing in a patient with chronic pancreatitis. J. Gastroenterol. 2007, 42, 589–592. [Google Scholar] [CrossRef]
- Ibiş, M.; Odemiş, B.; Başar, O.; Cakal, B.; Beyazt, F.; Köklü, S. Postpartum severe portal vein thrombosis and pyogenic liver abscess. J. Clin. Gastroenterol. 2005, 39, 646. [Google Scholar] [CrossRef]
- von Bertele, M.J. Late presentation of portal vein thrombosis as a complication of appendicitis. J. R. Army Med. Corps 1993, 139, 135–136. [Google Scholar] [CrossRef]
- Knockaert, D.; Robaeys, G.; Cox, E.; Marchal, G. Suppurative pylethrombosis: A changing clinical picture. Gastroenterology 1989, 97, 1028–1030. [Google Scholar] [CrossRef]
- Castillo, M.; Murphy, B. Septic portal vein thrombophlebitis: Computed tomography appearance. Case report. Comput. Radiol. 1986, 10, 289–292. [Google Scholar] [CrossRef]
- Walsh, M.; Moriarity, J.; Peterson, J.; Friend, G.; Chodock, R.; Rogan, M. Portal Venous Thrombosis in a Backpacker. Phys. Sportsmed 1996, 24, 75–81. [Google Scholar] [CrossRef]
- Díaz-Cuervo, F.; Posada-Calderon, L.; Ramirez-Rodríguez, N.; Perdomo, C.F.; Duran-Rehbein, G.A. Pylephlebitis with splenic abscess following transrectal prostate biopsy: Rare complications of intra-abdominal infection. J. Surg. Case Rep. 2017, 2017, rjw075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jadrijević, S.; Sef, D.; Kocman, B.; Mrzljak, A.; Matasic, H.; Škegro, D. Right hepatectomy due to portal vein thrombosis in vasculobiliary injury following laparoscopic cholecystectomy: A case report. J. Med. Case Rep. 2014, 8, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pohl, J.F.; Murarka, P.; Farrell, M.K.; Bezerra, J. Insights. Pylephlebitis. J. Pediatr. 1999, 135, 529. [Google Scholar] [CrossRef] [PubMed]
- Slovis, T.L.; Haller, J.O.; Cohen, H.; Berdon, W.E.; Watts, F.B. Complicated appendiceal inflammatory disease in children: Pylephlebitis and liver abscess. Radiology 1989, 171, 823–825. [Google Scholar] [CrossRef] [PubMed]
- Knobel, B.; Sommer, I.; Menashes, Z. A rare presentation of systemic salmonellosis. Infection 1985, 13, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Doklestić, K.; Dobrić, M.; Mijović, K.; Mišković, B.; Maričić, B.; Vasin, D. Case report of falciform ligament abscess-The importance of early diagnosis. Radiol. Case Rep. 2022, 17, 4608–4612. [Google Scholar] [CrossRef] [PubMed]
- Nasir, S.A.; Chambers, E.; Wojkiewicz, S. Pylephlebitis With Splenic and Mesenteric Vein Thrombosis in a Patient With Diverticulitis. Cureus 2022, 14, e28524. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, M.; Petrola, C.; Lopez, P.; Vilallonga, R.; de Gordejuela, A.G.R.; Armengol, M. A case of pylephlebitis complicating an acute appendicitis: Uncommon cholangitis-like situation. Int. J. Surg. Case Rep. 2022, 99, 107657. [Google Scholar] [CrossRef]
- Mohammadian, M.; Rath, P.; Dikhtyar, A.; Jesani, S.; Alyacoub, R. Portal Vein Thrombosis Associated With Fusobacterium nucleatum Bacteremia: A Rare Abdominal Variant of Lemierre’s Syndrome. Cureus 2022, 14, e27918. [Google Scholar] [CrossRef]
- Ali, J.S.; Kinden, R.H.; Emsley, J.G. A Case of Septic Portal Vein Thrombosis in a 71-Year-Old Female. Cureus 2022, 14, e27256. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, R.; Motohashi, I.; Suyama, Y. Pylephlebitis due to Listeria monocytogenes. BMJ Case Rep. 2022, 15, e250014. [Google Scholar] [CrossRef]
- Yoshikawa, S.; Ueda, T.; Fujiwara, T. Use of intravascular hypo- and hyper-attenuation on non-contrast-enhanced computed tomography in diagnosing acute septic thrombophlebitis. J. Radiol. Case Rep. 2022, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Trad, G.; Sheikhan, N.; Nguyen, A.; Valenta, J.; Iraninezhad, H. Portal Vein Thrombosis and Pyogenic Liver Abscess With Concomitant Bacteroides Bacteremia in a Patient With COVID-19 Infection: A Case Report and Brief Review. J. Investig. Med. High Impact Case Rep. 2022, 10. [Google Scholar] [CrossRef]
- Mehta, S.J.; Malhotra, S.; Panwar, A.; Sibal, A. Complicated Pylephlebitis Secondary to Perforated Appendicitis in an Adolescent. J. Indian Assoc. Pediatr. Surg. 2022, 27, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Adidam, S.; Leys, L.; Mahgoub, S. An Interesting Case of Klebsiella Pneumoniae Pylephlebitis. Cureus 2022, 14, e21297. [Google Scholar] [CrossRef] [PubMed]
- Talwar, D.; Acharya, S.; Shukla, S.; Kumar, S.; Annadatha, A. Pylephlebitis With Hepatic Abscess Complicating a Case of Acute Pancreatitis in a Young Male: Startling Complication of Intra-Abdominal Sepsis. Cureus 2022, 14, e21288. [Google Scholar] [CrossRef]
- Abbas, M.; Constantin, M.I.; Narendra, A. Pylephlebitis Caused by Fusobacterium nucleatum in a Septuagenarian Healthy Caucasian Male: Atypical Presentation of Lemierre’s Syndrome. Case Rep. Infect. Dis. 2022, 2022, 5160408. [Google Scholar] [CrossRef]
- Balthazar, E.J.; Gollapudi, P. Septic thrombophlebitis of the mesenteric and portal veins: CT imaging. J. Comput. Assist. Tomogr. 2000, 24, 755–760. [Google Scholar] [CrossRef]
- Gasparri, M.G.; Pipinos, I.I.; Bleza, D.A.; Shepard, A.D. Pylephlebitis secondary to intestinal ischemia. J. Am. Coll. Surg. 2000, 190, 265. [Google Scholar] [CrossRef]
- Sakamoto, H.; Suga, M.; Ozeki, I.; Kobayashi, T.; Sugaya, T.; Sasaki, Y.; Azuma, N.; Itoh, F.; Sakamoto, S.-I.; Yachi, A.; et al. Subcapsular hematoma of the liver and pylethrombosis in the setting of cholestatic liver injury. J. Gastroenterol. 1996, 31, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Bleeker-Rovers, C.P.; Jager, G.; Tack, C.J.; Van Der Meer, J.W.M.; Oyen, W.J.G. F-18-fluorodeoxyglucose positron emission tomography leading to a diagnosis of septic thrombophlebitis of the portal vein: Description of a case history and review of the literature. J. Intern. Med. 2004, 255, 419–423. [Google Scholar] [CrossRef]
- Arakura, N.; Ozaki, Y.; Yamazaki, S.; Ueda, K.; Maruyama, M.; Chou, Y.; Kodama, R.; Takayama, M.; Hamano, H.; Tanaka, E.; et al. Abscess of the round ligament of the liver associated with acute obstructive cholangitis and septic thrombosis. Intern. Med. 2009, 48, 1885–1888. [Google Scholar] [CrossRef] [Green Version]
- Dean, J.W.; Trerotola, S.O.; Harris, V.J.; Snidow, J.J.; Hawes, D. Percutaneous management of suppurative pylephlebitis. J. Vasc. Interv. Radiol. 1995, 6, 585–588. [Google Scholar] [CrossRef] [PubMed]
- Maeshima, K.; Ishii, K.; Inoue, M.; Himeno, K.; Seike, M. Behçet’s disease complicated by multiple aseptic abscesses of the liver and spleen. World J. Gastroenterol. 2013, 19, 3165–3168. [Google Scholar] [CrossRef] [PubMed]
- Huurman, V.A.; Visser, L.G.; Steens, S.C.; Terpstra, O.T.; Schaapherder, A.F. Persistent portal venous gas. J. Gastrointest. Surg. 2006, 10, 783–785. [Google Scholar] [CrossRef]
- Drabick, J.J.; Landry, C.F.J. Suppurative pylephlebitis. South Med. J. 1991, 84, 1396–1398. [Google Scholar] [CrossRef]
- Plemmons, R.M.; Dooley, D.P.; Longfield, R.N. Septic thrombophlebitis of the portal vein (pylephlebitis): Diagnosis and management in the modern era. Clin. Infect. Dis. 1995, 21, 1114–1120. [Google Scholar] [CrossRef]
- Soo, R.; Gosbell, I.; Gallo, J.; Pokorny, C.S. Septic portal vein thrombosis due to Fusobacterium necrophorum. Aust. N. Z. J. Med. 1999, 29, 569–570. [Google Scholar] [CrossRef]
- Tsao, Y.-T.; Lin, S.-H.; Cheng, C.-J.; Chang, F.-Y. Pylephlebitis associated with acute infected choledocholithiasis. Am. J. Med. Sci. 2006, 332, 85–87. [Google Scholar] [CrossRef]
- Palacios, E.J.; White, H.J.; Read, R.C. Suppurative pylephlebitis with multiple liver abscesses secondary to incarcerated incisional abdominal hernia. Report of one case. Review of literature. J. Ark. Med. Soc. 1971, 68, 73–74. [Google Scholar]
- Gold, R.P.; Seaman, W.B. Splenic flexure carcinoma as a source of hepatic portal venous gas. Radiology 1977, 122, 329–330. [Google Scholar] [CrossRef]
- Peters, T.G.; Locke, J.R.; Weight, G.R. Suppurative pylephlebitis caused by toothpick perforation. South Med. J. 1988, 81, 414–415. [Google Scholar] [CrossRef]
- Kasper, D.L.; Sahani, D.; Misdraji, J. Case records of the Massachusetts General Hospital. Case 25-2005. A 40-year-old man with prolonged fever and weight loss. N. Engl. J. Med. 2005, 353, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Sanchez, N.; Sánchez-Gómez, H.; Rojas, E.; Uribe, M. Pylephlebitis of portal venous system associated with urinary infection. Dig. Dis. Sci. 2003, 48, 834–836. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Sedlack, R.E.; Brandhagen, D.J.; Nyberg, S.L. Late presentation of pylephlebitis after orthotopic liver transplantation. Liver Transplant. 2003, 9, 776–777. [Google Scholar] [CrossRef]
- Tandon, R.; Davidoff, A.; Worthington, M.G.; Ross, J.J. Pylephlebitis after CT-guided percutaneous liver biopsy. AJR Am. J. Roentgenol. 2005, 184, S70–S72. [Google Scholar] [CrossRef] [PubMed]
- Wireko, M.; Berry, P.A.; Brennan, J.; Aga, R. Unrecognized pylephlebitis causing life-threatening septic shock: A case report. World J. Gastroenterol. 2005, 11, 614–615. [Google Scholar] [CrossRef] [PubMed]
- De Roover, A.; Detry, O.; Coimbra, C.; Hamoir, E.; Honoré, P.; Meurisse, M. Pylephlebitis of the portal vein complicating intragastric migration of an adjustable gastric band. Obes. Surg. 2006, 16, 369–371. [Google Scholar] [CrossRef]
- Wakisaka, M.; Mori, H.; Kiyosue, H.; Kamegawa, T.; Uragami, S. Septic thrombosis of the portal vein due to peripancreatic ligamental abscess. Eur. Radiol. 1999, 9, 90–92. [Google Scholar] [CrossRef]
- Pelsang, R.E.; Johlin, F.; Dhadha, R.; Bogdanowicz, M.; Schweiger, G.D. Management of suppurative pylephlebitis by percutaneous drainage: Placing a drainage catheter into the portal vein. Am. J. Gastroenterol. 2001, 96, 3192–3194. [Google Scholar] [CrossRef]
- Nouira, K.; Bedioui, H.; Azaiez, O.; Belhiba, H.; Ben Messaoud, M.; Ksantini, R.; Jouini, M.; Menif, E. Percutaneous drainage of suppurative pylephlebitis complicating acute pancreatitis. Cardiovasc. Interv. Radiol. 2007, 30, 1242–1244. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, S.A.; Gibney, R.G.; Cooperberg, P.L.; Scudamore, C.H.; Miller, R.R. Enterovenous fistula: Unusual complication of Crohn disease. Radiology 1988, 166, 745–746. [Google Scholar] [CrossRef]
- Aguas, M.; Bastida, G.; Nos, P.; Beltrán, B.; Grueso, J.L.; Grueso, J. Septic thrombophlebitis of the superior mesenteric vein and multiple liver abscesses in a patient with Crohn’s disease at onset. BMC Gastroenterol. 2007, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farin, P.; Paajanen, H.; Miettinen, P. Intraoperative US diagnosis of pylephlebitis (portal vein thrombosis) as a complication of appendicitis: A case report. Abdom. Imaging 1997, 22, 401–403. [Google Scholar] [CrossRef]
- Chang, Y.S.; Min, S.Y.; Joo, S.H.; Lee, S.-H. Septic thrombophlebitis of the porto-mesenteric veins as a complication of acute appendicitis. World J. Gastroenterol. 2008, 14, 4580–4582. [Google Scholar] [CrossRef]
- Cambria, R.P.; Margolies, M.N. Hepatic portal venous gas in diverticulitis: Survival in a steroid-treated patient. Arch. Surg. 1982, 117, 834–835. [Google Scholar] [CrossRef]
- Rodning, C.B.; Williams, L. Suppurative pylephlebitis due to pseudodiverticulosis coli. South Med. J. 1984, 77, 1164–1167. [Google Scholar] [CrossRef] [PubMed]
- Witte, C.L.; Brewer, M.L.; Witte, M.H.; Pond, G.B. Protean manifestations of pylethrombosis. A review of thirty-four patients. Ann. Surg. 1985, 202, 191–202. [Google Scholar] [CrossRef]
- Gage, T.P.; Eagan, J.; Gagnier, M. Diverticulitis complicated by candidal pylephlebitis. South Med. J. 1985, 78, 1265–1266. [Google Scholar] [CrossRef]
- Topiel, M.S.; Simon, G.L. Peptococcaceae bacteremia. Diagn. Microbiol. Infect. Dis. 1986, 4, 109–117. [Google Scholar] [CrossRef]
- Draghetti, M.J.; Salvo, A.F. Gas in the mesenteric veins as a nonfatal complication of diverticulitis: Report of a case. Dis. Colon. Rectum. 1999, 42, 1497–1498. [Google Scholar] [CrossRef] [PubMed]
- Liappis, A.P.; Roberts, A.D.; Simon, G.L.; Schwartz, A.M. Thrombosis and infection: A case of transient anti-cardiolipin antibody associated with pylephlebitis. Am. J. Med. Sci. 2003, 325, 365–368. [Google Scholar] [CrossRef] [PubMed]
- El Braks, R.; Harnois, F.; Boutros, N.; Fallik, D.; Roudie, J.; Smadja, C.; De Laveaucoupet, J.; Chaput, J.-C.; Naveau, S.; Mathurin, P. Mesenteric adenitis and portal vein thrombosis due to Fusobacterium nucleatum. Eur. J. Gastroenterol. Hepatol. 2004, 16, 1063–1066. [Google Scholar] [CrossRef]
- Dourakis, S.P.; Tsochatzis, E.; Alexopoulou, A.; Archimandritis, A.J. Pylephlebitis complicating silent diverticulitis. Lancet 2006, 368, 422. [Google Scholar] [CrossRef]
- Sellner, F.; Sobhian, B.; Baur, M.; Sellner, S.; Horvath, B.; Mostegel, M.; Karner, J.; Stättner, S. Intermittent hepatic portal vein gas complicating diverticulitis--a case report and literature review. Int. J. Color. Dis. 2007, 22, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.H.; Khot, U.P.; Thomas, D. Portal venous gas--case report and review of the literature. Anaesthesia 2007, 62, 400–404. [Google Scholar] [CrossRef]
- Jaber, M.R.; Holland, C. Septic pylephlebitis mimicking biliary obstruction. Am. J. Gastroenterol. 2008, 103, 807–808. [Google Scholar] [CrossRef]
- Perez-Cruet, M.J.; Grable, E.; Drapkin, M.S.; Jablons, D.M.; Cano, G. Pylephlebitis associated with diverticulitis. South Med. J. 1993, 86, 578–580. [Google Scholar] [CrossRef]
- Cheong, H.J.; Woo, H.J.; Kim, W.J.; Kim, M.J.; Lee, C.H.; Park, S.C.; Lim, H.E. Pylephlebitis associated with appendicitis. Korean J. Intern. Med. 1999, 14, 73–76. [Google Scholar] [CrossRef]
- Wildi, S.M.; Wallace, M.B.; Hunter, B.; Noone, T.C.; Hoffman, B.J. EUS diagnosis of an unusual case of pylephlebitis mimicking metastatic pancreatic cancer. Dig. Dis. Sci. 2005, 50, 2255–2258. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.S.-M.; Yiu, R.Y.-C.; Lee, J.F.-Y.; Li, J.C.-M.; Leung, K.-L. Portal venous gas and thrombosis in a Chinese patient with fulminant Crohn’s colitis: A case report with literature review. World J. Gastroenterol. 2006, 12, 5582–5586. [Google Scholar] [CrossRef]
- Nobili, C.; Uggeri, F.; Romano, F.; Degrate, L.; Caprotti, R.; Perego, P.; Franciosi, C. Pylephlebitis and mesenteric thrombophlebitis in sigmoid diverticulitis: Medical approach, delayed surgery. Dig. Liver Dis. 2007, 39, 1088–1090. [Google Scholar] [CrossRef] [PubMed]
- Waxman, B.P.; Cavanagh, L.L.; Nayman, J. Suppurative pyephlebitis and multiple hepatic abscesses with silent colonic diverticulitis. Med. J. Aust. 1979, 2, 376–378. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.I.; Venables, C.W.; Lendrum, R. ERCP diagnosis of multiple hepatic abscesses due to portal pylephlebitis. Br. J. Surg. 1985, 72, 439. [Google Scholar] [CrossRef] [PubMed]
- Joly, V.; Belmatoug, N.; Sibert, A.; Carbon, C.; Yeni, P. Septic thrombophlebitis of the portal vein. Clin. Infect. Dis. 1996, 23, 417–418. [Google Scholar] [CrossRef]
- Baddley, J.W.; Singh, D.; Correa, P.; Persich, N.J. Crohn’s disease presenting as septic thrombophlebitis of the portal vein (pylephlebitis): Case report and review of the literature. Am. J. Gastroenterol. 1999, 94, 847–849. [Google Scholar] [CrossRef]
- Loi, T.-H.; See, J.-Y.; Diddapur, R.K.; Issac, J.R. Emphysematous gastritis: A case report and a review of literature. Ann. Acad. Med. Singap. 2007, 36, 72–73. [Google Scholar] [CrossRef]
- Juler, G.L.; Dietrick, W.R.; Eisenman, J.I. Intramesenteric perforation of sigmoid diverticulitis with nonfatal venous intravasation. Am. J. Surg. 1976, 132, 653–656. [Google Scholar] [CrossRef]
- Saltzman, D.A.; Smithline, N.; Davis, J.R. Fulminant hepatic failure secondary to amebic abscesses. Am. J. Dig. Dis. 1978, 23, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Navarro, C.; Clain, D.J.; Kondlapoodi, P. Perforated diverticulum of the terminal ileum. A previously unreported cause of suppurative pylephlebitis and multiple hepatic abscesses. Dig. Dis. Sci. 1984, 29, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Sillero, J.M.; Calvet, X.; Musulen, E.; Diaz-Ruiz, M.J.; Tolosa, C.; Pardo, A.; Corcuera, A.; Malet, A.; Font, J. Idiopathic pylephlebitis and idiopathic sclerosing peritonitis in a man with protein S deficiency. J. Clin. Gastroenterol. 2001, 32, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Etienne, M.; Gueit, I.; Abboud, P.; Pons, J.-L.; Jacquot, S.; Caron, F. Fusobacterium nucleatum hepatic abscess with pylephlebitis associated with idiopathic CD4(+) T lymphocytopenia. Clin. Infect. Dis. 2001, 32, 326–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherigar, R.; Amir, K.A.; Bobba, R.K.; Arsura, E.L.; Srinivas, N. Abdominal pain secondary to pylephlebitis: An uncommon disease of the portal venous system, treated with local thrombolytic therapy. Dig. Dis. Sci. 2005, 50, 983–987. [Google Scholar] [CrossRef]
- Shah, I.; Bhatnagar, S. Liver abscess in a newborn leading to portal vein thrombosis. Indian J. Pediatr. 2009, 76, 1268–1269. [Google Scholar] [CrossRef] [PubMed]
- Shaw, P.J.; Saunders, A.J.; Drake, D.P. Case report: Ultrasonographic demonstration of portal vein thrombosis in the acute abdomen. Clin. Radiol. 1986, 37, 101–102. [Google Scholar] [CrossRef] [PubMed]
- Casals, S.; Enriquez, G.; Gomez, J.M.; Cabot, A. Sonographic diagnosis of pylephlebitis in children. Pediatr. Radiol. 1993, 23, 567–568. [Google Scholar] [CrossRef]
- Tung, J.Y.; Johnson, J.L.; Liacouras, C.A. Portal-mesenteric pylephlebitis with hepatic abscesses in a patient with Crohn’s disease treated successfully with anticoagulation and antibiotics. J. Pediatr. Gastroenterol. Nutr. 1996, 23, 474–478. [Google Scholar] [CrossRef]
- Ohtake, H.; Urayama, H.; Nozaki, Z.; Harada, T.; Kawasuji, M.; Wantanabe, Y. Surgical drainage for idiopathic suppurative pylephlebitis. Ann. Vasc. Surg. 1998, 12, 83–85. [Google Scholar] [CrossRef]
- Kader, H.; Baldassano, R.N.; Harty, M.P.; Nicotra, J.J.; Von Allmen, D.; Finn, L.; Markowitz, J.; Carrier, M.; Piccoli, D.A. Ruptured retrocecal appendicitis in an adolescent presenting as portal-mesenteric thrombosis and pylephlebitis. J. Pediatr. Gastroenterol. Nutr. 1998, 27, 584–588. [Google Scholar] [CrossRef]
- Vanamo, K.; Kiekara, O. Pylephlebitis after appendicitis in a child. J. Pediatr. Surg. 2001, 36, 1574–1576. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.N.; Tang, L.; Keller, K.; Harrison, M.R.; Farmer, D.L.; Albanese, C.T. Pylephlebitis, portal-mesenteric thrombosis, and multiple liver abscesses owing to perforated appendicitis. J. Pediatr. Surg. 2001, 36, 19. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, L.; Panero, A.; Colarizi, P.; Matrunola, M.; Simonetti, A.F.; Chiesa, C. Neonatal Candida albicans septic thrombosis of the portal vein followed by cavernous transformation of the vessel. J. Clin. Microbiol. 2004, 42, 4379–4382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimori, H.; Ezoe, E.; Ura, H.; Imaizumi, H.; Meguro, M.; Furuhata, T.; Katsuramaki, T.; Hata, F.; Yasoshima, T.; Hirata, K.; et al. Septic thrombophlebitis of the portal and superior mesenteric veins as a complication of appendicitis: Report of a case. Surg. Today 2004, 34, 173–176. [Google Scholar] [CrossRef]
- Muorah, M.; Hinds, R.; Verma, A.; Yu, D.; Samyn, M.; Mieli-Vergani, G.; Hadžić, N. Liver abscesses in children: A single center experience in the developed world. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 201–206. [Google Scholar] [CrossRef]
- Bogue, C.O.; Leahy, T.R.; Rea, D.J.; Bitnun, A.; Brandão, L.R.; Kahr, W.H.A.; Jacobson, S.; Amaral, J.; Connolly, B.L. Idiopathic suppurative pylephlebitis: Interventional radiological diagnosis and management. Cardiovasc. Interv. Radiol. 2009, 32, 1304–1307. [Google Scholar] [CrossRef]
- Patel, A.J.; Ong, P.V.; Higgins, J.P.; Kerner, J.A. Liver abscesses, pylephlebitis, and appendicitis in an adolescent male. Dig. Dis. Sci. 2009, 54, 2546–2548. [Google Scholar] [CrossRef]
- Levin, C.; Koren, A.; Miron, D.; Lumelsky, D.; Nussinson, E.; Siplovich, L.; Horovitz, Y. Pylephlebitis due to perforated appendicitis in a teenager. Eur. J. Pediatr. 2009, 168, 633–635. [Google Scholar] [CrossRef]
- Shyam, V.; Rana, S.; Kumar, B.V.; Choudhury, A.; Mukund, A. Suppurative Pylephlebitis With Portal Vein Abscess Mimicking Portal Vein Thrombosis: A Report of Two Cases. J. Clin. Exp. Hepatol. 2022, 12, 208–211. [Google Scholar] [CrossRef]
- Serracant-Barrera, A.; Llaquet-Bayo, H.; Sánchez-Delgado, J.; Romaguera-Monzonis, A.; Dalmau-Obrador, B.; Bejarano-González, N.; Navas-Pérez, A.M.; Llopart-Valdor, E.; García-Borobia, F.J.; Navarro-Soto, S. Pylephlebitis and liver abscesses secondary to acute advanced appendicitis. Rev. Esp. Enferm. Dig. 2015, 107, 397–398. [Google Scholar]
- Menclová, K.; Parobková, H.; Murinova, I.; Pudil, J.; Langer, D.; Ryska, M. Pylephlebitis in patient with covered perforated rectosigmoid cancer. Rozhl. Chir. 2014, 93, 507–511. [Google Scholar]
- Al Hajjar, N.; Crişan, D.; Grigorescu, M.; Boruah, P. Acute diverticulitis--an unusual cause of liver abcesses in a young man: A case report. Chirurgia 2012, 107, 267–272. [Google Scholar] [PubMed]
- Furuncuoğlu, Y.; Oven, B.B.; Mert, B.; Yılmaz, E.; Demir, M.K. Abdominal Variant of Lemierre’s Syndrome in a Patient with Pancreatic Adenocarcinoma. Medeni. Med. J. 2021, 6, 58–62. [Google Scholar] [CrossRef]
- Nigussie, B.; Woredekal, D.; Abaleka, F.I.; Gizaw, M.; Tharu, B. A Sporadic Case of Disseminated Fusobacterium Causing Pylephlebitis and Intracranial and Hepatic Abscesses in a Healthy Young Patient. Cureus 2020, 12, e9229. [Google Scholar] [CrossRef]
- Lawler, C.; King, B.; Milliron, M.L. Portomesenteric Venous Thrombosis in an Emergency Department Patient After Laparoscopic Sleeve Gastrectomy. Cureus 2021, 13, e19872. [Google Scholar] [CrossRef] [PubMed]
- Zardi, E.M.; Giorgi, C.; Zardi, D.M. Pylephlebitis as a Complication of Cholangitis and Sepsis in an HIV-Positive Patient. Dig. Dis. Sci. 2019, 64, 1719–1721. [Google Scholar] [CrossRef]
- Al Akhrass, F.; Abdallah, L.; Berger, S.; Sartawi, R. Gastrointestinal variant of Lemierre’s syndrome complicating ruptured appendicitis. Idcases 2015, 2, 72–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yazgan, C.; Akkas, M.; Ozmen, M.M. Inferior mesenteric vein pylephlebitis due to sigmoid diverticulitis. BMJ Case Rep. 2015, 2015, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adnan, M.M.; Gavin, M.; Eberhardt, S.C.; McCarthy, D.M. Pylephlebitis: Through These Portals Pass Bad Bugs. Dig. Dis. Sci. 2016, 61, 2807–2811. [Google Scholar] [CrossRef]
- Falkowski, A.L.; Cathomas, G.; Zerz, A.; Rasch, H.; Tarr, P.E. Pylephlebitis of a variant mesenteric vein complicating sigmoid diverticulitis. J. Radiol. Case Rep. 2014, 8, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.; Lerner, T.; Lingamaneni, G.; Richards, K. Superior mesenteric vein thrombosis as a complication of cecal diverticulitis: A case report. Int. J. Surg. Case Rep. 2016, 25, 71–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ufuk, F.; Herek, D.; Karabulut, N. Pylephlebitis Complicating Acute Appendicitis: Prompt Diagnosis with Contrast-Enhanced Computed Tomography. J. Emerg. Med. 2016, 50, e147–e149. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, M.; Gohar, A.; Gowda, S.N.; Abdullah, H.M.; Al-Hajjaj, A. Pylephlebitis Associated with Inferior Mesenteric Vein Thrombosis Treated Successfully with Anticoagulation and Antibiotics in a 37-Year-Old Male. Case Rep. Gastrointest. Med. 2020, 2020, 3918080. [Google Scholar] [CrossRef]
- Altamirano, J.; Zapata, L.; Poblano, M.; Rodriguez, A.; Camargo, L.; Martinez, B.; Bataller, R. Acute pylephlebitis following gastrointestinal infection: An unrecognized cause of septic shock. South Med. J. 2010, 103, 956–959. [Google Scholar] [CrossRef]
- Lee, B.K.; Ryu, H.H. A case of pylephlebitis secondary to cecal diverticulitis. J. Emerg. Med. 2012, 42, e81–e85. [Google Scholar] [CrossRef]
- Kashiura, M.; Sugiyama, K.; Akashi, A.; Hamabe, Y. Diverticulitis-induced pylephlebitis possibly misdiagnosed as biliary duct obstruction. Acute Med. Surg. 2016, 3, 404–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, B.; Jones, D.; Sarrazin, J.; Coburn, N.G. Porta hepatis abscess and portal vein thrombosis following ingestion of a fishbone. BMJ Case Rep. 2019, 12, e227271. [Google Scholar] [CrossRef]
- Kaenkumchorn, T.; Kesavan, A. A Rare Complication of Campylobacter Sepsis in an Infant. Clin. Pediatr. 2018, 57, 484–487. [Google Scholar] [CrossRef]
- Anand, S.; Umeh, C.A.; Giberson, C.; Wassel, E.; Nguyen, A.; Porter, H.; Choday, P.; Kaur, H.; Kundu, A.; Penaherrera, J. Septic Portal Vein Thrombosis, Clinical Presentation, and Management. Cureus 2021, 13, e19840. [Google Scholar] [CrossRef]
- Kalbitz, S.; Ermisch, J.; Schmidt, J.M.; Wallstabe, I.; Lübbert, C. Unhappy Triad: Infection with Leptospira spp. Escherichia coli and Bacteroides uniformis Associated with an Unusual Manifestation of Portal Vein Thrombosis. Case Rep. Gastroenterol. 2021, 15, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Wakui, N.; Takayama, R.; Matsukiyo, Y.; Shinohara, M.; Kobayashi, S.; Kanekawa, T.; Nakano, S.; Nagai, H.; Kudo, T.; Maruyama, K.; et al. Visualization of segmental arterialization with arrival time parametric imaging using Sonazoid-enhanced ultrasonography in portal vein thrombosis: A case report. Exp. Ther. Med. 2013, 5, 673–677. [Google Scholar] [CrossRef]
- Radovanovic, N.; Dumic, I.; Veselinovic, M.; Burger, S.; Milovanovic, T.; Nordstrom, C.W.; Niendorf, E.; Ramanan, P. Fusobacterium necrophorum subsp. necrophorum Liver Abscess with Pylephlebitis: An Abdominal Variant of Lemierre’s Syndrome. Case Rep. Infect. Dis. 2020, 2020, 9237267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadano, Y.; Iwata, H. Septic thrombophlebitis of the superior mesenteric vein with bacteraemia caused by Bacteroides fragilis and Streptococcus intermedius as a complication of diverculitis. BMJ Case Rep. 2013, 2013, bcr2013008661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meersseman, W. Candida tropicalis pylephlebitis with persistent fungaemia in a 72-year-old lady with severe pancreatitis. Mycoses 2011, 54, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Coyne, C.J.; Jain, A. Pylephlebitis in a previously healthy emergency department patient with appendicitis. West. J. Emerg. Med. 2013, 14, 428–430. [Google Scholar] [CrossRef] [Green Version]
- Warren, L.R.; Chandrasegaram, M.D.; Madigan, D.J.; Dolan, P.M.; Neo, E.L.; Worthley, C.S. Falciform ligament abscess from left sided portal pyaemia following malignant obstructive cholangitis. World J. Surg. Oncol. 2012, 10, 278. [Google Scholar] [CrossRef] [Green Version]
- Queiroz, R.M.; Sampaio, F.D.C.; Marques, P.E.; Ferez, M.A.; Febronio, E.M. Pylephlebitis and septic thrombosis of the inferior mesenteric vein secondary to diverticulitis. Radiol. Bras. 2018, 51, 336–337. [Google Scholar] [CrossRef] [Green Version]
- De Zylva, J.; Padley, J.; Badbess, R.; Dedigama, M. Multiorgan failure following gastroenteritis: A case report. J. Med. Case Rep. 2020, 14, 74. [Google Scholar] [CrossRef]
- Zia, A.; Sohal, S.; Costas, C. Pylephlebitis: A Case of Inferior Mesenteric Vein Thrombophlebitis in a Patient with Acute Sigmoid Diverticulitis—A Case Report and Clinical Management Review. Case Rep. Infect. Dis. 2019, 2019, 5341281. [Google Scholar] [CrossRef]
- Wong, C.S.; Cho, G.; Godfrey, E.M.; Harper, S. Portal pyaemia secondary to colonic perforation. BMJ Case Rep. 2019, 12, e228400. [Google Scholar] [CrossRef]
- Granero-Castro, P.; Raposo-Rodríguez, L.; Moreno-Gijón, M.; Prieto-Fernández, A.; Granero-Trancón, J.; González-González, J.J.; Barneo-Serra, L. Pylephlebitis as a complication of acute appendicitis. Rev. Esp. Enferm. Dig. 2010, 102, 217–218. [Google Scholar] [CrossRef] [Green Version]
- Rahmati, E.; She, R.C.; Kazmierski, B.; Geiseler, P.J.; Wong, D. A case of liver abscess and fusobacterium septicemia. IDCases 2017, 9, 98–100. [Google Scholar] [CrossRef]
- Zamora, J.A.G.; Alvarez, M.R.; Henry, Z.; Baracco, G.J.; Dickinson, G.; Lichtenberger, P. Liver abscess caused by Lawsonella clevelandensis in a patient with rheumatoid arthritis: A case report and literature review. IDCases 2020, 20, e00734. [Google Scholar] [CrossRef]
- Cho, E.; Jun, C.H.; Yoon, J.H.; Wi, J.W.; Shin, S.S.; Cho, S.B.; Park, C.H.; Kim, H.S.; Choi, S.K.; Rew, J.S. A rare case of portal biliopathy and pylephlebitis following the injection of cyanoacrylate into the duodenal varix. J. Clin. Gastroenterol. 2016, 50, 897. [Google Scholar] [CrossRef]
- Chaudhary, H.; Jindal, P.; Pandiarajan, V.; Kumar, J.; Sudhakar, M.; Ezhumalai, G.; Nada, R.; Gupta, K. Portal vein thrombosis, livedo reticularis, polymicrobial sepsis and high antiphospholipid antibody titers in a newborn: A clinicopathological conference of antiphospholipid-associated neonatal syndrome. Lupus 2021, 30, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Krzak, A.M.; Townson, A.; Malam, Y.; Mathews, J. Diverticulitis complicated by colovenous fistula formation and pylephlebitis. J. Surg. Case Rep. 2022, 2022, rjab591. [Google Scholar] [CrossRef]
- James, T.W.; Sheikh, S.Z.; McGowan, C.E. Perigastric abscess as a delayed adverse event in endoscopic sleeve gastroplasty. Gastrointest. Endosc. 2019, 89, 890–891. [Google Scholar] [CrossRef]
- Lee, H.; Sung, K.; Cho, J. Retroperitoneal abscess with pylephlebitis caused by lumbar acupuncture: A case report. BMC Surg. 2019, 19, 145. [Google Scholar] [CrossRef] [PubMed]
- Lazar, N.; Sardarli, K.; Imam, Z.; Khasawneh, M.; Hader, I. A Rare Twist of the Forgotten Disease: A Case of Fusobacterium necrophorum Sepsis with Portomesenteric Thrombosis and a Review of the Literature. Case Rep. Gastrointest. Med. 2021, 2021, 6699867. [Google Scholar] [CrossRef]
- Hamera, L.; Abraham, S.; Jordan, J. Pylephlebitis as a Rare Complication of Ulcerative Colitis: A Case Report. Cureus 2019, 11, e4792. [Google Scholar] [CrossRef] [PubMed]
- al Bshabshe, A.; Joseph, M.R.; Battayah, E.S.; Hamid, M.E. Fungal peritonitis caused by Pichia kudriavzevii following sleeve gastrectomy. Ann. Saudi Med. 2019, 39, 205–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashiura, M.; Tanabe, T.; Akashi, A.; Hamabe, Y. Pylephlebitis: A severe complication of intra-abdominal infection. Intern. Med. 2014, 53, 2829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, K.; Weisman, D.S.; Patrice, K.-A. Pylephlebitis: A rare complication of an intra-abdominal infection. J. Community Hosp. Intern. Med. Perspect. 2013, 3, 20732. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Tian, X.; Xie, X.; Yang, Y. Intestinal Infarction Caused by Thrombophlebitis of the Portomesenteric Veins as a Complication of Acute Gangrenous Appendicitis after Appendectomy. Medicine 2015, 94, e1033. [Google Scholar] [CrossRef]
- Stone, N.R.H.; Barrett, J.; Hickish, T.; Dasgupta, D.; Newsholme, W.; Biswas, J.; Martin, T. Case report: Bacteroides-associated pylephlebitis in a patient with strongyloidiasis. Am. J. Trop. Med. Hyg. 2015, 92, 340–341. [Google Scholar] [CrossRef] [Green Version]
- Abughanimeh, O.; Tahboub, M.; Zafar, Y.; Abu Ghanimeh, M. Pylephlebitis Caused by Actinomyces Bacteremia. Cureus 2018, 10, e2887. [Google Scholar] [CrossRef] [Green Version]
- Shahani, L.; Khardori, N. Fusobacterium necrophorum—Beyond Lemierres syndrome. BMJ Case Rep. 2011, 2011, bcr0720114527. [Google Scholar] [CrossRef] [Green Version]
- Fukahori, M.; Shirayama, S.; Kawasaki, A.; Takasugi, T.; Sano, H.; Iwasaki, H. A case of silent perforated diverticulitis in the ascending colon combined with pylephlebitis resulting in complete occlusion of the portal trunk. Clin. J. Gastroenterol. 2015, 8, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Hale, G.R.; Sakkal, L.A.; Galanis, T. Pylephlebitis treated with apixaban. Hosp. Pr. 2019, 47, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Gallinger, Z.R.; May, G.; Kortan, P.; Bayoumi, A.M. Pylephlebitis After Colonic Polypectomy Causing Fever and Abdominal Pain. ACG Case Rep. J. 2015, 2, 142–145. [Google Scholar] [CrossRef]
- Mellor, T.E.; Mitchell, N.; Logan, J. Lemierre’s syndrome variant of the gut. BMJ Case Rep. 2017, 2017, bcr221567. [Google Scholar] [CrossRef]
- Milner, D.A.; Chatterjee, A. A case of portal vein thrombosis caused by ingestion of a foreign body. Gastrointest. Endosc. 2011, 74, 1168–1170. [Google Scholar] [CrossRef] [PubMed]
- Ram, P.; Lapumnuaypol, K.; Punjabi, C. Diverticular Pylephlebitis and Polymicrobial Septicemia. Case Rep. Infect. Dis. 2017, 2017, 6819474. [Google Scholar] [CrossRef] [PubMed]
- Řezáč, T.; Zbořil, P.; Vomáčková, K.; Špička, P. A biliary tract obstruction complicated by acute appendicitis and portal vein thrombosis-a case report and review of literature. Int. J. Surg. Case Rep. 2021, 84, 106140. [Google Scholar] [CrossRef] [PubMed]
- Garrett, A.; Carnish, E.; Das, N.; Slome, M.; Measley, R. Once universally fatal: Pylephlebitis. Am. J. Med. 2014, 127, 595–597. [Google Scholar] [CrossRef]
- Prabhu, R.; Natarajan, A.; Krishna, S.; Thangavelu, S. Portal pyaemia secondary to open haemorrhoidectomy: Need for prophylactic broad spectrum antibiotics. BMJ Case Rep. 2013, 2013, bcr2013200222. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Chen, S.; Li, W.; Qu, J. An unusual increase of D-dimer level-pylephlebitis caused by acute appendicitis: A case report. Ann. Palliat. Med. 2021, 10, 4917–4921. [Google Scholar] [CrossRef] [PubMed]
- Rustagi, T.; Uy, E.M.; Rai, M. Pyogenic liver abscesses secondary to pylephlebitis complicating acute on chronic pancreatitis. J. Dig. Dis. 2012, 13, 439–443. [Google Scholar] [CrossRef]
- Kim, J.H.; Kwon, H.Y.; Durey, A. Thrombophlebitis of superior mesenteric vein with bacteremia of Gemella sanguinis and Streptococcus gordonii. J. Microbiol. Immunol. Infect. 2019, 52, 672–673. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, S.; França, N.J.; Mineiro, F.; Capela, G.; Duarte, C.; Mendes, A.R. Pylephlebitis—A rare complication of a fish bone migration mimicking metastatic pancreatic cancer: A case report. World J. Clin. Cases 2021, 9, 6768–6774. [Google Scholar] [CrossRef]
- Wali, L.; Shah, A.; Sleiman, S.; Hogsand, T.; Humphries, S. Acute pylephlebitis secondary to perforated sigmoid diverticulitis: A case report. Radiol. Case Rep. 2021, 16, 1504–1507. [Google Scholar] [CrossRef]
- Gajendran, M.; Muniraj, T.; Yassin, M. Diverticulitis complicated by pylephlebitis: A case report. J. Med. Case Rep. 2011, 5, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rea, J.D.; Jundt, J.P.; Jamison, R.L. Pylephlebitis: Keep it in your differential diagnosis. Am. J. Surg. 2010, 200, e69–e71. [Google Scholar] [CrossRef]
- Khandwala, K.; Ahmed, A.; Abid, S. Migration of Fish Bone Into the Portal Vein Resulting in Pylephlebitis and Pyogenic Liver Abscesses. Am. J. Gastroenterol. 2019, 114, 1414. [Google Scholar] [CrossRef]
- Bakti, N.; Hussain, A.; El-Hasani, S. A rare complication of acute appendicitis: Superior mesenteric vein thrombosis. Int. J. Surg. Case Rep. 2011, 2, 250–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- L’Ollivier, C.; Eldin, C.; Lambourg, E.; Brouqui, P.; Lagier, J.C. Case report: First Molecular Diagnosis of Liver Abscesses Due to Fasciola hepatica Acute Infection Imported from Vietnam. Am. J. Trop. Med. Hyg. 2020, 102, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Kenny, C.; Sohan, O.; Murray, L.; Fox, T.P. Branch portal vein pyaemia secondary to amoebic liver abscess. BMJ Case Rep. 2015, 2015, bcr2014209098. [Google Scholar] [CrossRef] [Green Version]
- Szanto, P.; Vasile, T.; Ciobanu, L.; Munteanu, D.; Badea, R. Ingested foreign body causing pylephlebitis identified by trans-abdominal ultrasound. Balk. Med. J. 2016, 33, 587–588. [Google Scholar] [CrossRef]
- Chao, G.F.; Hirji, S.; Shikora, S.A. Extensive thrombus and brain microabscesses after sleeve gastrectomy. J. Radiol. Case Rep. 2018, 12, 10–17. [Google Scholar] [CrossRef]
- Tamaki, I.; Kami, K.; Yamamoto, E.; Morimoto, T. Catheter-directed thrombolysis through the operatively recanalized umbilical vein for acute extensive portal vein thrombosis: Report of a case. Clin. J. Gastroenterol. 2014, 7, 376–380. [Google Scholar] [CrossRef]
- Nazir, S.; Jehangir, A.; Siddiqui, A.; Tachamo, N.; Lohani, S.; York, E. A rare case of pylephlebitis after colonic polypectomy. J. Community Hosp. Intern. Med. Perspect. 2017, 7, 40–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, E.Y.T.; Taneja, R. Thrombophlebitis of abdominal veins as an unusual cause for acute abdomen: Avoiding the diagnostic pitfalls. Emerg. Radiol. 2021, 28, 187–192. [Google Scholar] [CrossRef]
- Mouat, S.; Bishop, J.; Glamuzina, E.; Chin, S.; Best, E.J.; Evans, H.M. Fatal hyperammonemia associated with disseminated Serratia marcescens infection in a pediatric liver transplant recipient. Pediatr. Transplant. 2018, 22, e13180. [Google Scholar] [CrossRef] [PubMed]
- Ogah, K.; Sethi, K.; Karthik, V. Clostridium clostridioforme liver abscess complicated by portal vein thrombosis in childhood. J. Med. Microbiol. 2012, 61, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Davarpanah, A.H.; Eberhardt, L.W. Case 282: Fishbone pylephlebitis. Radiology 2020, 297, 239–243. [Google Scholar] [CrossRef]
- Castro, R.; Fernandes, T.; Oliveira, M.I.; Castro, M. Acute Appendicitis Complicated by Pylephlebitis: A Case Report. Case Rep. Radiol. 2013, 2013, 627521. [Google Scholar] [CrossRef] [Green Version]
- Ozawa, K.; Shikino, K. Pylephlebitis due to acute cholecystitis and cholangitis. BMJ Case Rep. 2021, 14, e244912. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, T.; D’Souza, D.; Varma, P.; Burnes, J.; Croagh, D. A minimally invasive solution for a complication of minimally invasive treatment. ANZ J. Surg. 2018, 88, 1079–1081. [Google Scholar] [CrossRef]
- Bockmeyer, J.; Taha-Mehlitz, S.; Heeren, N.; Ristic, S.; Metzger, J.; Gass, J.-M. Jejunal Diverticulosis Probably Leading to Pylephlebitis of the Superior Mesenteric Vein. Case Rep. Surg. 2020, 2020, 2343218. [Google Scholar] [CrossRef] [PubMed]
- Zimhony, O.; Katz, M. A patient with fever and jaundice. QJM 2012, 105, 381–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, A.R.; Lee, C.K.; Kim, H.J.; Shim, J.-J.; Jang, J.Y.; Dong, S.H.; Kim, B.H.; Chang, Y.W. Septic pylephlebitis as a rare complication of Crohn’s disease. Korean J. Gastroenterol. 2013, 61, 219–224. [Google Scholar] [CrossRef] [Green Version]
- El Mouhadi, S.; Ait-Oufella, H.; Maury, E.; Menu, Y.; Arrivé, L. Ileal diverticulitis complicated by portal-mesenteric pylephlebitis and pulmonary septic foci. Diagn. Interv. Imaging 2012, 93, 57–59. [Google Scholar] [CrossRef] [Green Version]
- Hakeem, A.R.; Nasim, N.; Raza, S.S.; Ahmad, N. Portal pyaemia following renal transplantation. BMJ Case Rep. 2014, 2014, bcr2014204026. [Google Scholar] [CrossRef] [Green Version]
- Sapmaz, F.; Kalkan, I.H.; Guliter, S.; Bilgili, Y.K. Acute cholecystitis complicated by pylephlebitis. Turk. J. Gastroenterol. 2014, 25, 266–267. [Google Scholar] [CrossRef]
- Pradka, S.P.; Trankiem, C.T.; Ricotta, J.J. Pylephlebitis and acute mesenteric ischemia in a young man with inherited thrombophilia and suspected foodborne illness. J. Vasc. Surg. 2012, 55, 1769–1772. [Google Scholar] [CrossRef] [Green Version]
- Karam, M.M.; Abdalla, M.F.; Bedair, S. Isolated superior mesenteric venous thrombophlebitis with acute appendicitis. Int. J. Surg. Case Rep. 2013, 4, 432–434. [Google Scholar] [CrossRef] [Green Version]
- Figueiras, R.G.; Paz, M.L.; González, S.B.; Martín, C.V. Case 158: Pylephlebitis. Radiology 2010, 255, 1003–1007. [Google Scholar] [CrossRef]
- Santosh, D.; Low, G. Pylephlebitis with Liver Abscess Secondary to Chronic Appendicitis: A Radiological Conundrum. J. Clin. Imaging Sci. 2016, 6, 37. [Google Scholar] [CrossRef] [Green Version]
- Kubo, H.; Asai, G.; Haraguchi, K.; Shibahara, Y.; Kihara, T.; Yamakawa, G.; Kira, F.; Higashi, H.; Morishita, S.; Fujie, H.; et al. Liver abscess and portal vein thrombosis due to ileal diverticulitis mediated by barium fluoroscopy. Intern. Med. 2017, 56, 3255–3259. [Google Scholar] [CrossRef] [Green Version]
- Imaoka, K.; Fukuda, S.; Tazawa, H.; Fukuhara, S.; Hirata, Y.; Fujisaki, S.; Takahashi, M.; Sakimoto, H. A Rare Case of Pylephlebitis as a Complication of Cholecystocolonic Fistula. Case Rep. Surg. 2018, 2018, 3931674. [Google Scholar] [CrossRef]
- Giuffrè, M.; Verso, C.L.; Serra, G.; Moceri, G.; Cimador, M.; Corsello, G. Portal Vein Thrombosis in a Preterm Newborn with Mutation of the MTHFR and PAI-1 Genes and Sepsis by Candida parapsilosis. Am. J. Perinatol. 2016, 33, 1099–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, J.A.; Rambally, S. Fusobacterium nucleatum Bacteremia Presenting with Portal Vein Thrombosis: An Abdominal Lemierre Syndrome? Am. J. Med. 2017, 130, e255–e256. [Google Scholar] [CrossRef] [Green Version]
- Lauretta, A.; Almoudaris, A.M.; Jiao, L.R. Septic thrombophlebitis of portal vein: Unusual presentation of appendicitis. Am. Surg. 2011, 77, 206–207. [Google Scholar] [CrossRef]
- Phoompoung, P.; Chayakulkeeree, M.; Ngamskulrungroj, P.; Pongpaibul, A. Asymptomatic Histoplasma Pylephlebitis in an Orthotopic Liver Transplant Recipient: A Case Report and Literature Review. Mycopathologia 2019, 184, 177–180. [Google Scholar] [CrossRef]
- Choudhry, A.J.; Baghdadi, Y.M.K.; Amr, M.A.; Alzghari, M.J.; Jenkins, D.; Zielinski, M.D. Pylephlebitis: A Review of 95 Cases. J. Gastrointest. Surg. 2016, 20, 656–661. [Google Scholar] [CrossRef] [Green Version]
- Belhassen-García, M.; Gomez-Munuera, M.; Pardo-Lledias, J.; Velasco-Tirado, V.; Perez-Persona, E.; Galindo-Perez, I.; Alvela-Suárez, L.; Romero-Alegría, Á.; Muñoz-Bellvis, L.; Cordero-Sánchez, M. Pylephlebitis: Incidence and prognosis in a tertiary hospital. Enferm. Infecc Microbiol. Clin. 2014, 32, 350–354. [Google Scholar] [CrossRef]
- Kanellopoulou, T.; Alexopoulou, A.; Theodossiades, G.; Koskinas, J.; Archimandritis, A.J. Pylephlebitis: An overview of non-cirrhotic cases and factors related to outcome. Scand. J. Infect. Dis. 2010, 42, 804–811. [Google Scholar] [CrossRef]
- Jevtic, D.; Gavrancic, T.; Pantic, I.; Nordin, T.; Nordstrom, C.W.; Antic, M.; Pantic, N.; Kaljevic, M.; Joksimovic, B.; Jovanovic, M.; et al. Suppurative Thrombosis of the Portal Vein (Pylephlebits): A Systematic Review of Literature. J. Clin. Med. 2022, 11, 4992. [Google Scholar] [CrossRef]
- Baril, N.; Wren, S.; Radin, R.; Ralls, P.; Stain, S. The role of anticoagulation in pylephlebitis. Am. J. Surg. 1996, 172, 449–453. [Google Scholar] [CrossRef]
- Naymagon, L.; Tremblay, D.; Schiano, T.; Mascarenhas, J. The role of anticoagulation in pylephlebitis: A retrospective examination of characteristics and outcomes. J. Thromb. Thrombolysis 2020, 49, 325–331. [Google Scholar] [CrossRef]
- Murray, J.L.; Connell, J.L.; Stacy, A.; Turner, K.H.; Whiteley, M. Mechanisms of synergy in polymicrobial infections. J. Microbiol. 2014, 52, 188. [Google Scholar] [CrossRef]
- Shah, P.M.; Edwards, B.L.; Dietch, Z.C.; Guidry, C.A.; Davies, S.W.; Hennessy, S.A.; Duane, T.M.; O’Neill, P.J.; Coimbra, R.; Cook, C.H.; et al. Do Polymicrobial Intra-Abdominal Infections Have Worse Outcomes than Monomicrobial Intra-Abdominal Infections? Surg. Infect. 2016, 17, 27. [Google Scholar] [CrossRef] [Green Version]
- Duffy, F.J.; Millan, M.T.; Schoetz, D.J.; Larsen, C.R. Suppurative pylephlebitis and pylethrombosis: The role of anticoagulation. Am. Surg. 1995, 61, 1041–1044. [Google Scholar]
- Decuypere, S.; Meehan, C.J.; Van Puyvelde, S.; De Block, T.; Maltha, J.; Palpouguini, L.; Tahita, M.; Tinto, H.; Jacobs, J.; Deborggraeve, S. Diagnosis of Bacterial Bloodstream Infections: A 16S Metagenomics Approach. PLoS Negl. Trop. Dis. 2016, 10, e0004470. [Google Scholar] [CrossRef]
- Gyarmati, P.; Kjellander, C.; Aust, C.; Kalin, M.; Öhrmalm, L.; Giske, C.G. Bacterial Landscape of Bloodstream Infections in Neutropenic Patients via High Throughput Sequencing. PLoS ONE 2015, 10, e0135756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faria, M.M.P.; Conly, J.M.; Surette, M.M.G. The development and application of a molecular community profiling strategy to identify polymicrobial bacterial DNA in the whole blood of septic patients. BMC Microbiol. 2015, 15, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, W.; Honickman, S.; Ohki, S.; Buckman, R.; Warner, E. Percutaneous diagnosis and drainage of pylephlebitis: A case report. Surgery 1987, 101, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Pylephlebitis—UpToDate. Available online: https://www.uptodate.com/contents/pylephlebitis (accessed on 7 November 2022).
- Case 25-2005: A 40-Year-Old Man with Prolonged Fever and Weight Loss. N. Engl. J. Med. 2005, 353, 2827. [CrossRef]
- Riccabona, M.; Kuttnig-Haim, M.; Dacar, D.; Urlesberger, B.; Reiterer, F.; Maurer, U.; Zobel, G. Venous thrombosis in and after extracorporeal membrane oxygenation: Detection and follow-up by color Doppler sonography. Eur. Radiol. 1997, 7, 1383–1386. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Yamanaka, K.; Izumi, A.; Matsui, J.; Kurimoto, M.; Aoki, H.; Tamura, J. Endovascular repair using a covered stent for a ruptured infected aneurysm of the superior mesenteric artery after pancreaticoduodenectomy: A case report. Surg. Case Rep. 2020, 6, 270. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Characteristics | |
|---|---|
| Median Age, years 50 (29;63) | Gender, n (%) Male, 155 (70.5%) Female, 65 (29.5%) |
| Symptoms on hospital admission, n (%) | |
| Fever, 166 (75.5%) Abdominal Pain, 146 (66.4%) Nausea/Vomiting, 56 (25.5%) Diarrhea, 38 (17.3%) | Jaundice, 28 (12.7%) None, 10 (4.5%) Weight Loss, 3 (1.4%) |
| Mortality, n (%) Death, 28 (14%) | |
| Data Regarding Infection Source and Pathogens | |
| Possible Source of Infection, n (%) | |
| Diverticulitis, 53 (26.5%) Acute appendicitis, 44 (22%) None/not reported, 23 (11.5%) Liver abscess, 17 (8.5%) Gastroenteritis, 13 (6.5%) Surgery, 12 (6%) Pancreatitis, 11 (5.5%) Inflammatory bowel diseases, 8 (4%) Foreign body, 7 (3.5%) Cholangitis/cholecystitis, 7 (3.5%) Malignancy, 3 (1.5%) Gastric ulcer 3 (1.5%) Ischemia, 2 (1%) | Umbilical catheter, 2 (1%) Polypectomy, 2 (1%) Invasive liver procedures, 2 (1%) Retroperitoneal abscess, 2 (1%) Renal abscess, 1 (0.5%) Endometriosis, 1 (0.5%) Splenic abscess, 1 (0.5%) Endoscopic variceal ligation, 1 (0.5%) Cholecystocolonic fistula, 1 (0.5%) Dental abscess, 1 (0.5%) Urinary tract infections, 1 (0.5%) Burns, 1 (0.5%) Prostate biopsy, 1 (0.5%) |
| Detected Microorganisms, n (%) | |
| Not detected/Reported, 66(30%) Aerobes Gram-positive Streptococcus spp., 30 (15%) Staphylococcus spp., 8 (4%) Enterococcus spp., 3 (1.5%) Gram-negative Escherichia coli, 50 (25%) Klebsiella spp., 9 (4.5%) Pseudomonas aeruginosa, 2 (1%) Eikenella corrodens, 2 (1%) Acinetobacter spp., 2 (1%) Campylobacter jejuni, 2 (1%) Aeromonas hydrophila, 2 (1%) Morganella morganii, 2 (1%) Leptospira spp., 1 (0.5%) Proteus spp., 1 (0.5%) | Anaerobes Bacteroides spp., 34 (17%) Clostridium spp., 13 (6.5%) Fusobacterium spp., 20 (10%) Peptostreptococcus spp., 7 (3.5%) Lactobacillus spp., 1 (0.5%) Propionibacterium acnes, 1 (0.5%) Granulicatella adiacens, 1 (0.5%) Parvimonas micra, 1 (0.5%) Fungi Candida spp., 7 (3.5%) Helminths Fasciola hepatica, 1 (0.5%) Strongyloides stercoralis, 1 (0.5%) Amoebas Amoeba spp., 1 (0.5%) Entoamoeba hystolytica, 1 (0.5%) |
| Number of different bacteria detected, n (%) Not detected/reported, 66 (30%) One, 94 (42.8%) Two, 32 (14.5%) More than two, 28 (12.7%) | |
| Combination Therapy |
|---|
Metronidazole (500 mg every 6–8 h), PLUS ONE of the following:
|
| Monotherapy |
Based on carbapenem, with ONE of the following:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusaro, L.; Di Bella, S.; Martingano, P.; Crocè, L.S.; Giuffrè, M. Pylephlebitis: A Systematic Review on Etiology, Diagnosis, and Treatment of Infective Portal Vein Thrombosis. Diagnostics 2023, 13, 429. https://doi.org/10.3390/diagnostics13030429
Fusaro L, Di Bella S, Martingano P, Crocè LS, Giuffrè M. Pylephlebitis: A Systematic Review on Etiology, Diagnosis, and Treatment of Infective Portal Vein Thrombosis. Diagnostics. 2023; 13(3):429. https://doi.org/10.3390/diagnostics13030429
Chicago/Turabian StyleFusaro, Lisa, Stefano Di Bella, Paola Martingano, Lory Saveria Crocè, and Mauro Giuffrè. 2023. "Pylephlebitis: A Systematic Review on Etiology, Diagnosis, and Treatment of Infective Portal Vein Thrombosis" Diagnostics 13, no. 3: 429. https://doi.org/10.3390/diagnostics13030429