

Development and External Validation of a Radiomics Model Derived from Preoperative Gadoxetic Acid-Enhanced MRI for Predicting Histopathologic Grade of Hepatocellular Carcinoma
 ,
,
Abstract
:1. Introduction
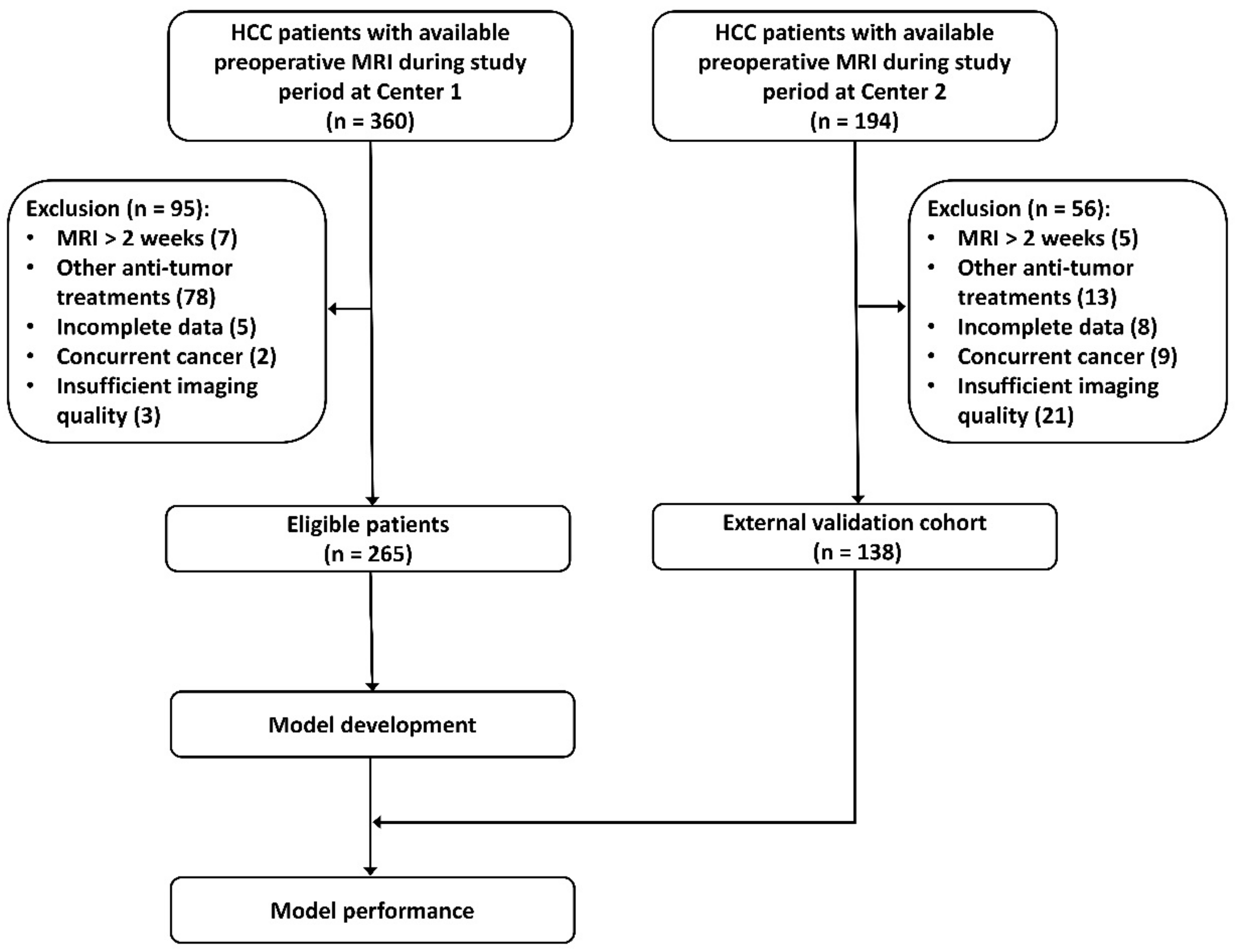
2. Patients and Methods
2.1. Clinicopathological Variables
2.2. Gadoxetic Acid-Enhanced MRI Exam
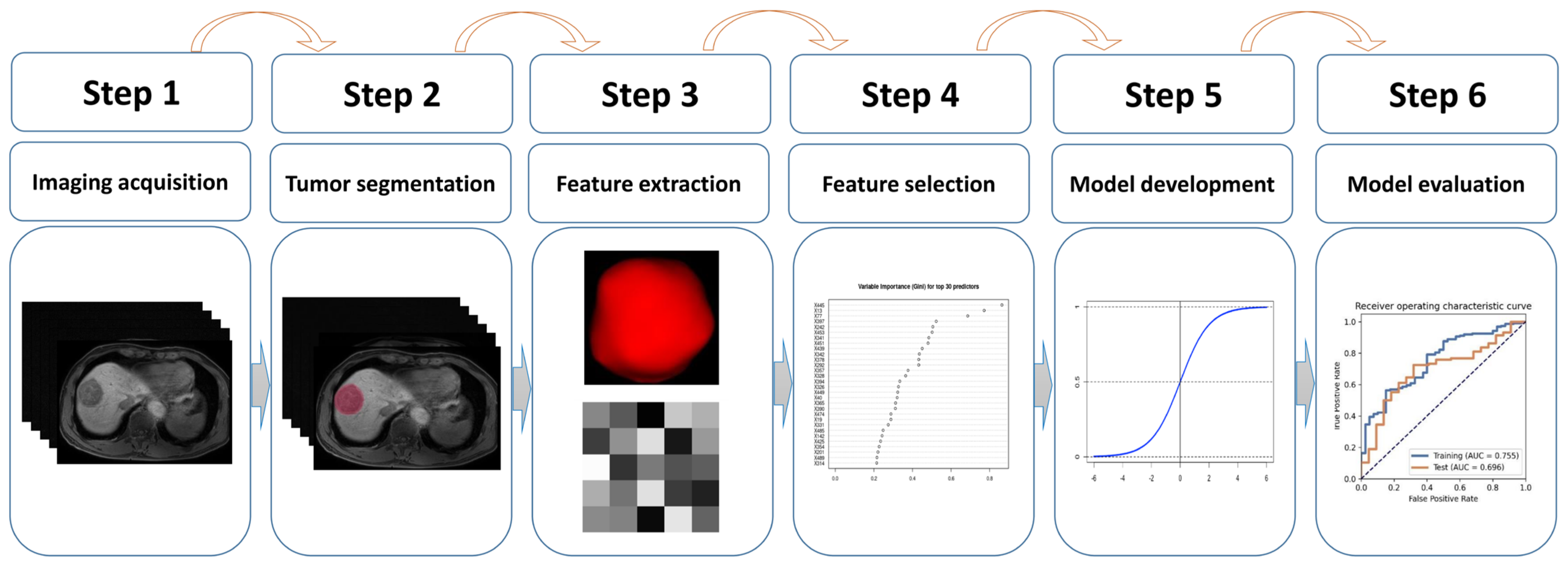
2.3. Tumor Segmentation and Inter-Observer Agreement Assessment
2.4. Feature Extraction
2.5. Feature Selection, Model Development, and External Validation
2.6. Statistical Analysis
3. Results
3.1. Basic Characteristics of Patient in the Two Cohorts
3.2. Independent Clinical Predictor for Histopathological Grading
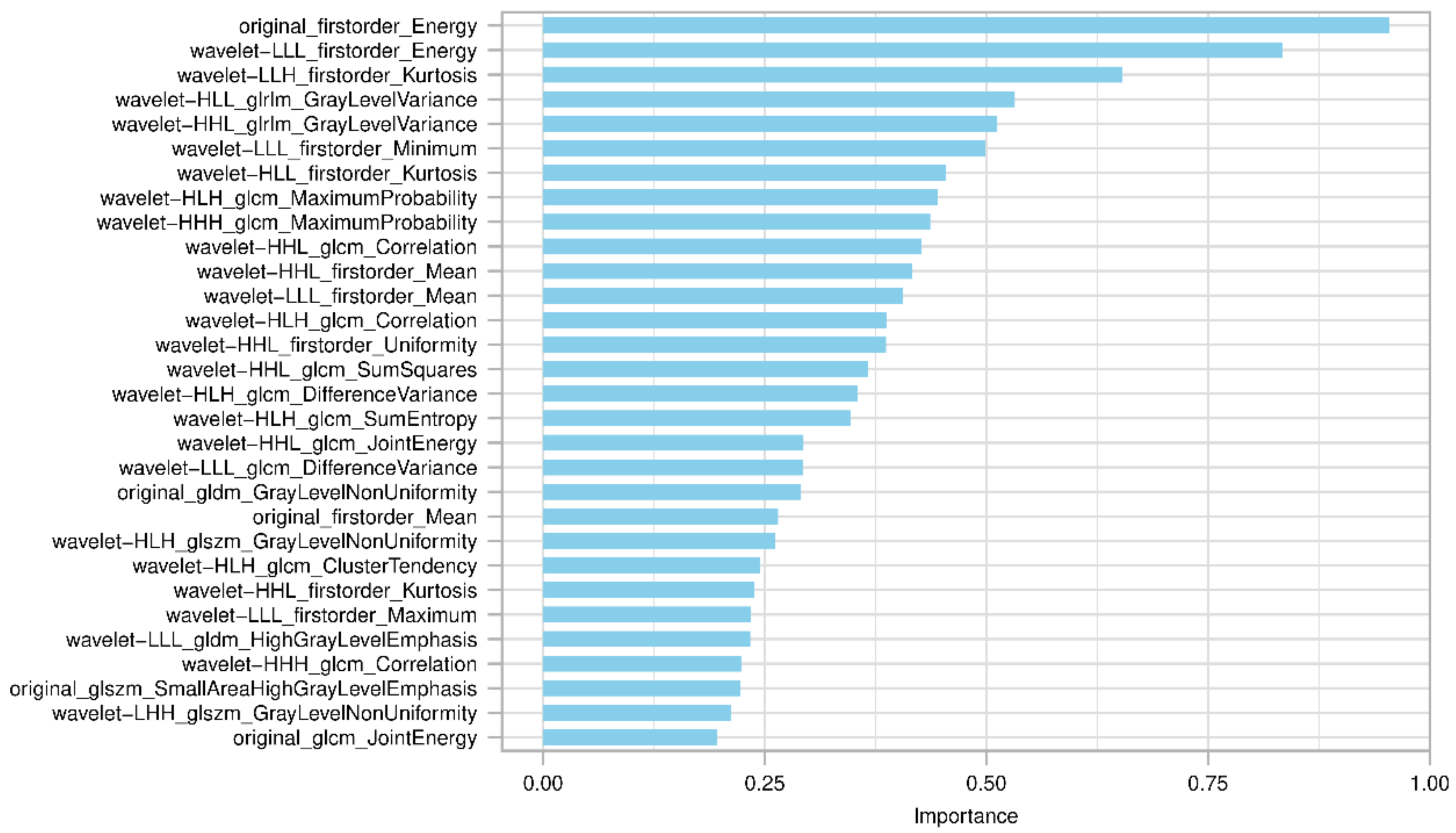
3.3. Feature Selection and Model Development
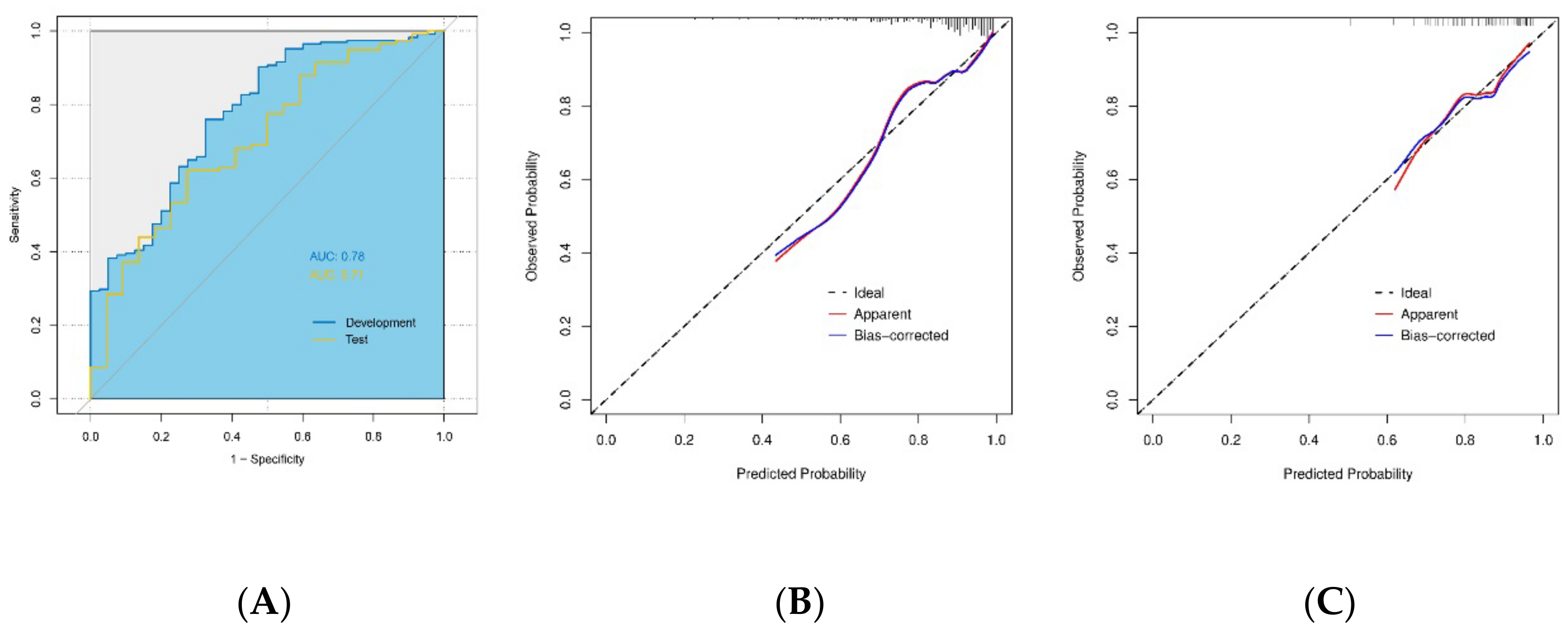
3.4. Prediction Performance of the Radiomics Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins-Filho, S.N.; Paiva, C.; Azevedo, R.S.; Alves, V.A.F. Histological Grading of Hepatocellular Carcinoma—A Systematic Review of Literature. Front. Med. 2017, 4, 193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oishi, K.; Itamoto, T.; Amano, H.; Fukuda, S.; Ohdan, H.; Tashiro, H.; Shimamoto, F.; Asahara, T. Clinicopathologic features of poorly differentiated hepatocellular carcinoma. J. Surg. Oncol. 2007, 95, 311–316. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Practice Guidelines Committee; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatol. Baltim. Md. 2005, 42, 1208–1236. [Google Scholar] [CrossRef]
- Okusaka, T.; Okada, S.; Ueno, H.; Ikeda, M.; Shimada, K.; Yamamoto, J.; Kosuge, T.; Yamasaki, S.; Fukushima, N.; Sakamoto, M. Satellite lesions in patients with small hepatocellular carcinoma with reference to clinicopathologic features. Cancer 2002, 95, 1931–1937. [Google Scholar] [CrossRef]
- Thampanitchawong, P.; Piratvisuth, T. Liver biopsy: Complications and risk factors. World J. Gastroenterol. 1999, 5, 301–304. [Google Scholar] [CrossRef]
- Mani, H.; Kleiner, D.E. Liver biopsy findings in chronic hepatitis B. Hepatology 2009, 49, S61–S71. [Google Scholar] [CrossRef]
- Joo, I.; Lee, J.M. Recent Advances in the Imaging Diagnosis of Hepatocellular Carcinoma: Value of Gadoxetic Acid-Enhanced MRI. Liver Cancer 2015, 5, 67–87. [Google Scholar] [CrossRef]
- Van Beers, B.E.; Pastor, C.M.; Hussain, H.K. Primovist, Eovist: What to expect? J. Hepatol. 2012, 57, 421–429. [Google Scholar] [CrossRef]
- Brismar, T.B.; Dahlström, N.; Edsborg, N.; Persson, A.; Smedby, Ö.; Albiin, N. Liver vessel enhancement by gd-bopta and gd-eob-dtpa: A comparison in healthy volunteers. Acta Radiol. 2009, 50, 709–715. [Google Scholar] [CrossRef]
- Zhang, K.; Li, W.-C.; Xie, S.-S.; Lin, L.-Y.; Shen, Z.-W.; Ye, Z.-X.; Shen, W. Preoperative determination of pathological grades of primary single HCC: Development and validation of a scoring model. Abdom. Imaging 2022, 47, 3468–3477. [Google Scholar] [CrossRef]
- An, C.; Park, M.-S.; Jeon, H.-M.; Kim, Y.-E.; Chung, W.-S.; Chung, Y.E.; Kim, M.-J.; Kim, K.W. Prediction of the histopathological grade of hepatocellular carcinoma using qualitative diffusion-weighted, dynamic, and hepatobiliary phase MRI. Eur. Radiol. 2012, 22, 1701–1708. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [Green Version]
- Miranda Magalhaes Santos, J.M.; Clemente Oliveira, B.; Araujo-Filho JD, A.B.; Assuncao, A.N., Jr.; de MMachado, F.A.; Carlos Tavares Rocha, C. State-of-the-art in radiomics of hepatocellular carcinoma: A review of basic principles, applications, and limitations. Abdom. Radiol. 2020, 45, 342–353. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Wang, J.; Zhu, Y.; Chen, J.; Mao, L.; Kong, W.; Qiu, Y.; Wu, X.; Guan, Y.; He, J. Gd-EOB-DTPA-enhanced MRI radiomic features for predicting histological grade of hepatocellular carcinoma. Hepatobiliary Surg. Nutr. 2022, 11, 13–24. [Google Scholar] [CrossRef]
- Choi, J.M.; Yu, J.-S.; Cho, E.-S.M.; Kim, J.H.M.; Chung, J.-J.M. Texture Analysis of Hepatocellular Carcinoma on Magnetic Resonance Imaging: Assessment for Performance in Predicting Histopathologic Grade. J. Comput. Assist. Tomogr. 2020, 44, 901–910. [Google Scholar] [CrossRef]
- Han, Y.E.; Cho, Y.; Kim, M.J.; Park, B.J.; Sung, D.J.; Han, N.Y.; Sim, K.C.; Park, Y.S.; Na Park, B. Hepatocellular Carcinoma Pathologic Grade Prediction Using Radiomics and Machine Learning Models of Gadoxetic Acid-Enhanced MRI: A Two-Center Study. Abdom Radiol. 21 September 2022. Available online: https://link.springer.com/10.1007/s00261-022-03679-y (accessed on 17 December 2022).
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients With Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; the WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Xu, R.; Mei, H.; Zhang, L.; Yu, Q.; Liu, R.; Fan, B. Application of Enhanced T1WI of MRI Radiomics in Glioma Grading. Int. J. Clin. Pract. 2022, 2022, 3252574. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, H.; Duan, S.; Hao, D.; Liu, J. Radiomics and Machine Learning With Multiparametric Preoperative MRI May Accurately Predict the Histopathological Grades of Soft Tissue Sarcomas. J. Magn. Reson. Imaging 2019, 51, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Woźnicki, P.; Westhoff, N.; Huber, T.; Riffel, P.; Froelich, M.F.; Gresser, E.; Von Hardenberg, J.; Mühlberg, A.; Michel, M.S.; Schoenberg, S.O.; et al. Multiparametric MRI for Prostate Cancer Characterization: Combined Use of Radiomics Model with PI-RADS and Clinical Parameters. Cancers 2020, 12, 1767. [Google Scholar] [CrossRef]
- Peng, Z.; Jiang, M.; Cai, H.; Chan, T.; Dong, Z.; Luo, Y.; Li, Z.-P.; Feng, S.-T. Gd-EOB-DTPA-enhanced magnetic resonance imaging combined with T1 mapping predicts the degree of differentiation in hepatocellular carcinoma. BMC Cancer 2016, 16, 625. [Google Scholar] [CrossRef] [Green Version]
- Haimerl, M.; Utpatel, K.; Götz, A.; Zeman, F.; Fellner, C.; Nickel, D.; Luerken, L.; Brennfleck, F.; Stroszczynski, C.; Scheiter, A.; et al. Quantification of contrast agent uptake in the hepatobiliary phase helps to differentiate hepatocellular carcinoma grade. Sci. Rep. 2021, 11, 22991. [Google Scholar] [CrossRef]
- Zhou, J.; Lu, J.; Gao, C.; Zeng, J.; Zhou, C.; Lai, X.; Cai, W.; Xu, M. Predicting the response to neoadjuvant chemotherapy for breast cancer: Wavelet transforming radiomics in MRI. BMC Cancer 2020, 20, 100. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.X.; Feng, W.; Wei, J.C.; Zeng, T.S.; Li, Z.D.; Zhang, L.J.; Lin, P.; Luo, R.Z.; He, J.H.; Fu, J.H. Support vector machine-based nomogram predicts postoperative distant metastasis for patients with oesophageal squamous cell carcinoma. Br. J. Cancer 2013, 109, 1109–1116. [Google Scholar] [CrossRef] [Green Version]
- Angelis, I.; Exarchos, T. Hepatocellular Carcinoma Detection Using Machine Learning Techniques. In GeNeDis 2020; Vlamos, P., Ed.; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 21–29, (Advances in Experimental Medicine and Biology). [Google Scholar]
- Wang, Q.; Li, C.; Zhang, J.; Hu, X.; Fan, Y.; Ma, K.; Sparrelid, E.; Brismar, T.B. Radiomics Models for Predicting Microvascular Invasion in Hepatocellular Carcinoma: A Systematic Review and Radiomics Quality Score Assessment. Cancers 2021, 13, 5864. [Google Scholar] [CrossRef]
- Christodoulou, E.; Ma, J.; Collins, G.S.; Steyerberg, E.W.; Verbakel, J.Y.; Van Calster, B. A systematic review shows no performance benefit of machine learning over logistic regression for clinical prediction models. J. Clin. Epidemiol. 2019, 110, 12–22. [Google Scholar] [CrossRef]
- Zhang, J.; Chen, G.; Zhang, P.; Zhang, J.; Li, X.; Gan, D.; Cao, X.; Han, M.; Du, H.; Ye, Y. The threshold of alpha-fetoprotein (AFP) for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0228857. [Google Scholar] [CrossRef]
- Shen, J.; Liu, J.; Li, C.; Wen, T.; Yan, L.; Yang, J. The Impact of Tumor Differentiation on the Prognosis of HBV-Associated Solitary Hepatocellular Carcinoma Following Hepatectomy: A Propensity Score Matching Analysis. Dig. Dis. Sci. 2018, 63, 1962–1969. [Google Scholar] [CrossRef]
- Wu, M.; Tan, H.; Gao, F.; Hai, J.; Ning, P.; Chen, J.; Zhu, S.; Wang, M.; Dou, S.; Shi, D. Predicting the grade of hepatocellular carcinoma based on non-contrast-enhanced MRI radiomics signature. Eur. Radiol. 2018, 29, 2802–2811. [Google Scholar] [CrossRef]
- Schraiber, L.S.; de Mattos, A.A.; Zanotelli, M.L.; Cantisani, G.P.C.; Brandão, A.B.M.; Marroni, C.A.; Kiss, G.; Ernani, L.; Marcon, P.S. Alpha-fetoprotein Level Predicts Recurrence After Transplantation in Hepatocellular Carcinoma. Medicine 2016, 95, e2478. [Google Scholar] [CrossRef]
- Rungsakulkij, N.; Suragul, W.; Mingphruedhi, S.; Tangtawee, P.; Muangkaew, P.; Aeesoa, S. Prognostic role of alpha-fetoprotein response after hepatocellular carcinoma resection. World J. Clin. Cases 2018, 6, 110–120. [Google Scholar] [CrossRef]
- Bai, D.-S.; Zhang, C.; Chen, P.; Jin, S.-J.; Jiang, G.-Q. The prognostic correlation of AFP level at diagnosis with pathological grade, progression, and survival of patients with hepatocellular carcinoma. Sci. Rep. 2017, 7, 12870. [Google Scholar] [CrossRef] [Green Version]
- Muscari, F.; Maulat, C. Preoperative alpha-fetoprotein (AFP) in hepatocellular carcinoma (HCC): Is this 50-year biomarker still up-to-date? Transl. Gastroenterol. Hepatol. 2020, 5, 46. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Pencina, M.J.; Lingsma, H.F.; Kattan, M.W.; Vickers, A.J.; Van Calster, B. Assessing the incremental value of diagnostic and prognostic markers: A review and illustration. Eur. J. Clin. Investig. 2012, 42, 216–228. [Google Scholar] [CrossRef] [Green Version]
- Bodalal, Z.; Trebeschi, S.; Nguyen-Kim, T.D.L.; Schats, W.; Beets-Tan, R. Radiogenomics: Bridging imaging and genomics. Abdom. Imaging 2019, 44, 1960–1984. [Google Scholar] [CrossRef] [Green Version]
- Saini, A.; Breen, I.; Pershad, Y.; Naidu, S.; Knuttinen, M.G.; Alzubaidi, S.; Sheth, R.; Albadawi, H.; Kuo, M.; Oklu, R. Radiogenomics and Radiomics in Liver Cancers. Diagnostics 2018, 9, 4. [Google Scholar] [CrossRef]
- Ding, Y.; Ruan, S.; Wang, Y.; Shao, J.; Sun, R.; Tian, W.; Xiang, N.; Ge, W.; Zhang, X.; Su, K.; et al. Novel deep learning radiomics model for preoperative evaluation of hepatocellular carcinoma differentiation based on computed tomography data. Clin. Transl. Med. 2021, 11, e570. Available online: https://onlinelibrary.wiley.com/doi/10.1002/ctm2.570 (accessed on 17 December 2022). [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Center 1 | Center 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Overall (n = 265) | Poorly Differentiated HCC (n = 40) | Non-Poorly Differentiated HCC (n = 225) | p Value | Overall (n = 138) | Poorly Differentiated HCC (n = 22) | Non-Poorly Differentiated HCC (n = 116) | p Value | |
| Gender: | 0.343 | 1.000 | ||||||
| Female | 37 (14.0%) | 8 (20.0%) | 29 (12.9%) | 17 (12.3%) | 2 (9.09%) | 15 (12.9%) | ||
| Male | 228 (86.0%) | 32 (80.0%) | 196 (87.1%) | 121 (87.7%) | 20 (90.9%) | 101 (87.1%) | ||
| Age (years): | 0.334 | 0.617 | ||||||
| ≤55 | 186 (70.2%) | 25 (62.5%) | 161 (71.6%) | 78 (56.5%) | 14 (63.6%) | 64 (55.2%) | ||
| >55 | 79 (29.8%) | 15 (37.5%) | 64 (28.4%) | 60 (43.5%) | 8 (36.4%) | 52 (44.8%) | ||
| Etiology: | 0.64 | 1.000 | ||||||
| HBV | 203 (76.6%) | 29 (72.5%) | 174 (77.3%) | 112 (81.2%) | 18 (81.8%) | 94 (81.0%) | ||
| Non HBV | 62 (23.4%) | 11 (27.5%) | 51 (22.7%) | 26 (18.8%) | 4 (18.2%) | 22 (19.0%) | ||
| Cirrhosis: | 1.000 | 0.725 | ||||||
| Cirrhosis | 142 (53.6%) | 21 (52.5%) | 121 (53.8%) | 58 (42.0%) | 8 (36.4%) | 50 (43.1%) | ||
| Non cirrhosis | 123 (46.4%) | 19 (47.5%) | 104 (46.2%) | 80 (58.0%) | 14 (63.6%) | 66 (56.9%) | ||
| ALT (IU/L): | 0.663 | 0.678 | ||||||
| ≤42 | 154 (58.1%) | 25 (62.5%) | 129 (57.3%) | 105 (76.1%) | 18 (81.8%) | 87 (75.0%) | ||
| >42 | 111 (41.9%) | 15 (37.5%) | 96 (42.7%) | 33 (23.9%) | 4 (18.2%) | 29 (25.0%) | ||
| AST (IU/L): | 0.836 | 0.441 | ||||||
| ≤42 | 153 (57.7%) | 22 (55.0%) | 131 (58.2%) | 106 (76.8%) | 15 (68.2%) | 91 (78.4%) | ||
| >42 | 112 (42.3%) | 18 (45.0%) | 94 (41.8%) | 32 (23.2%) | 7 (31.8%) | 25 (21.6%) | ||
| Platelet (×109/L): | 0.153 | 1.000 | ||||||
| ≤125 | 89 (33.6%) | 9 (22.5%) | 80 (35.6%) | 29 (21.0%) | 4 (18.2%) | 25 (21.6%) | ||
| >125 | 176 (66.4%) | 31 (77.5%) | 145 (64.4%) | 109 (79.0%) | 18 (81.8%) | 91 (78.4%) | ||
| ALBI grade: | 0.213 | 0.738 | ||||||
| Grade 1 | 120 (45.3%) | 14 (35.0%) | 106 (47.1%) | 49 (35.5%) | 9 (40.9%) | 40 (34.5%) | ||
| Grade 2 | 145 (54.7%) | 26 (65.0%) | 119 (52.9%) | 89 (64.5%) | 13 (59.1%) | 76 (65.5%) | ||
| MELD score: | 0.629 | 0.589 | ||||||
| ≤9 | 256 (96.6%) | 38 (95.0%) | 218 (96.9%) | 132 (95.7%) | 22 (100%) | 110 (94.8%) | ||
| >9 | 9 (3.40%) | 2 (5.00%) | 7 (3.11%) | 6 (4.35%) | 0 (0.00%) | 6 (5.17%) | ||
| Tumor size (cm): | 0.446 | 0.596 | ||||||
| ≤5 | 124 (46.8%) | 16 (40.0%) | 108 (48.0%) | 73 (52.9%) | 10 (45.5%) | 63 (54.3%) | ||
| >5 | 141 (53.2%) | 24 (60.0%) | 117 (52.0%) | 65 (47.1%) | 12 (54.5%) | 53 (45.7%) | ||
| AFP (ng/mL): | 0.006 * | 0.204 | ||||||
| <400 | 155 (58.5%) | 15 (37.5%) | 140 (62.2%) | 100 (72.5%) | 13 (59.1%) | 87 (75.0%) | ||
| ≥400 | 110 (41.5%) | 25 (62.5%) | 85 (37.8%) | 38 (27.5%) | 9 (40.9%) | 29 (25.0%) | ||
| Clinicopathological Variable | OR | 95%CI | p Value |
|---|---|---|---|
| Gender (Female vs. male) | 0.59 | 0.25–1.41 | 0.24 |
| Age (≤55 vs. >55 years) | 1.51 | 0.75–3.05 | 0.25 |
| Etiology (Non HBV vs. HBV) | 0.77 | 0.36–1.65 | 0.51 |
| Cirrhosis (Non cirrhosis vs. cirrhosis) | 0.95 | 0.48–1.86 | 0.88 |
| ALT (≤42 vs. >42 IU/L) | 0.81 | 0.40–1.61 | 0.54 |
| AST (≤42 vs. >42 IU/L) | 1.14 | 0.58–2.24 | 0.70 |
| Platelet (≤125 vs. >125 × 109/L) | 1.90 | 0.86–4.19 | 0.11 |
| ALBI grade (Grade 1 vs. 2) | 1.65 | 0.82–3.33 | 0.16 |
| MELD score (≤9 vs. >9) | 1.64 | 0.33–8.19 | 0.55 |
| Tumor size (≤5 vs. >5 cm) | 1.38 | 0.70–2.75 | 0.35 |
| AFP (<400 vs. ≥400 ng/mL) | 2.75 | 1.37–5.50 | <0.001 * |
| Model | AUC (95%CI) | Cut-Off Value | Accuracy | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|---|---|
| Development cohort | LR | 0.75 (0.68–0.83) | 0.56 | 0.61 | 0.56 | 0.85 | 0.95 | 0.26 |
| SVM | 0.75 (0.68–0.83) | 0.41 | 0.81 | 0.85 | 0.58 | 0.92 | 0.40 | |
| Adaboost | 0.93 (0.89–0.97) | 0.50 | 0.85 | 0.85 | 0.88 | 0.97 | 0.51 | |
| LR+AFP | 0.78 (0.70–0.86) | 0.83 | 0.75 | 0.76 | 0.68 | 0.93 | 0.33 | |
| SVM+AFP | 0.78 (0.70–0.85) | 0.84 | 0.73 | 0.73 | 0.73 | 0.94 | 0.33 | |
| Adaboost+AFP | 0.94 (0.90–0.98) | 0.73 | 0.91 | 0.92 | 0.85 | 0.97 | 0.67 | |
| Test cohort | LR | 0.70 (0.58–0.81) | - | 0.72 | 0.72 | 0.68 | 0.92 | 0.32 |
| SVM | 0.67 (0.56–0.79) | - | 0.68 | 0.68 | 0.68 | 0.92 | 0.29 | |
| Adaboost | 0.61 (0.47–0.74) | - | 0.75 | 0.80 | 0.45 | 0.89 | 0.30 | |
| LR+AFP | 0.71 (0.59–0.82) | - | 0.64 | 0.62 | 0.72 | 0.92 | 0.27 | |
| SVM+AFP | 0.69 (0.57–0.81) | - | 0.80 | 0.86 | 0.45 | 0.89 | 0.38 | |
| Adaboost+AFP | 0.58 (0.45–0.72) | - | 0.77 | 0.83 | 0.45 | 0.89 | 0.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, X.; Li, C.; Wang, Q.; Wu, X.; Chen, Z.; Xia, F.; Cai, P.; Zhang, L.; Fan, Y.; Ma, K. Development and External Validation of a Radiomics Model Derived from Preoperative Gadoxetic Acid-Enhanced MRI for Predicting Histopathologic Grade of Hepatocellular Carcinoma. Diagnostics 2023, 13, 413. https://doi.org/10.3390/diagnostics13030413
Hu X, Li C, Wang Q, Wu X, Chen Z, Xia F, Cai P, Zhang L, Fan Y, Ma K. Development and External Validation of a Radiomics Model Derived from Preoperative Gadoxetic Acid-Enhanced MRI for Predicting Histopathologic Grade of Hepatocellular Carcinoma. Diagnostics. 2023; 13(3):413. https://doi.org/10.3390/diagnostics13030413
Chicago/Turabian StyleHu, Xiaojun, Changfeng Li, Qiang Wang, Xueyun Wu, Zhiyu Chen, Feng Xia, Ping Cai, Leida Zhang, Yingfang Fan, and Kuansheng Ma. 2023. "Development and External Validation of a Radiomics Model Derived from Preoperative Gadoxetic Acid-Enhanced MRI for Predicting Histopathologic Grade of Hepatocellular Carcinoma" Diagnostics 13, no. 3: 413. https://doi.org/10.3390/diagnostics13030413