
The Role of mpMRI in the Assessment of Prostate Cancer Recurrence Using the PI-RR System: Diagnostic Accuracy and Interobserver Agreement in Readers with Different Expertise
 , , and
on behalf of the Uro-Oncology Disease Management Team (DMT) of the IRCCS Ospedale Policlinico San Martino Genoa, Italy
, , and
on behalf of the Uro-Oncology Disease Management Team (DMT) of the IRCCS Ospedale Policlinico San Martino Genoa, Italy
Abstract
:1. Introduction
2. Materials and Methods
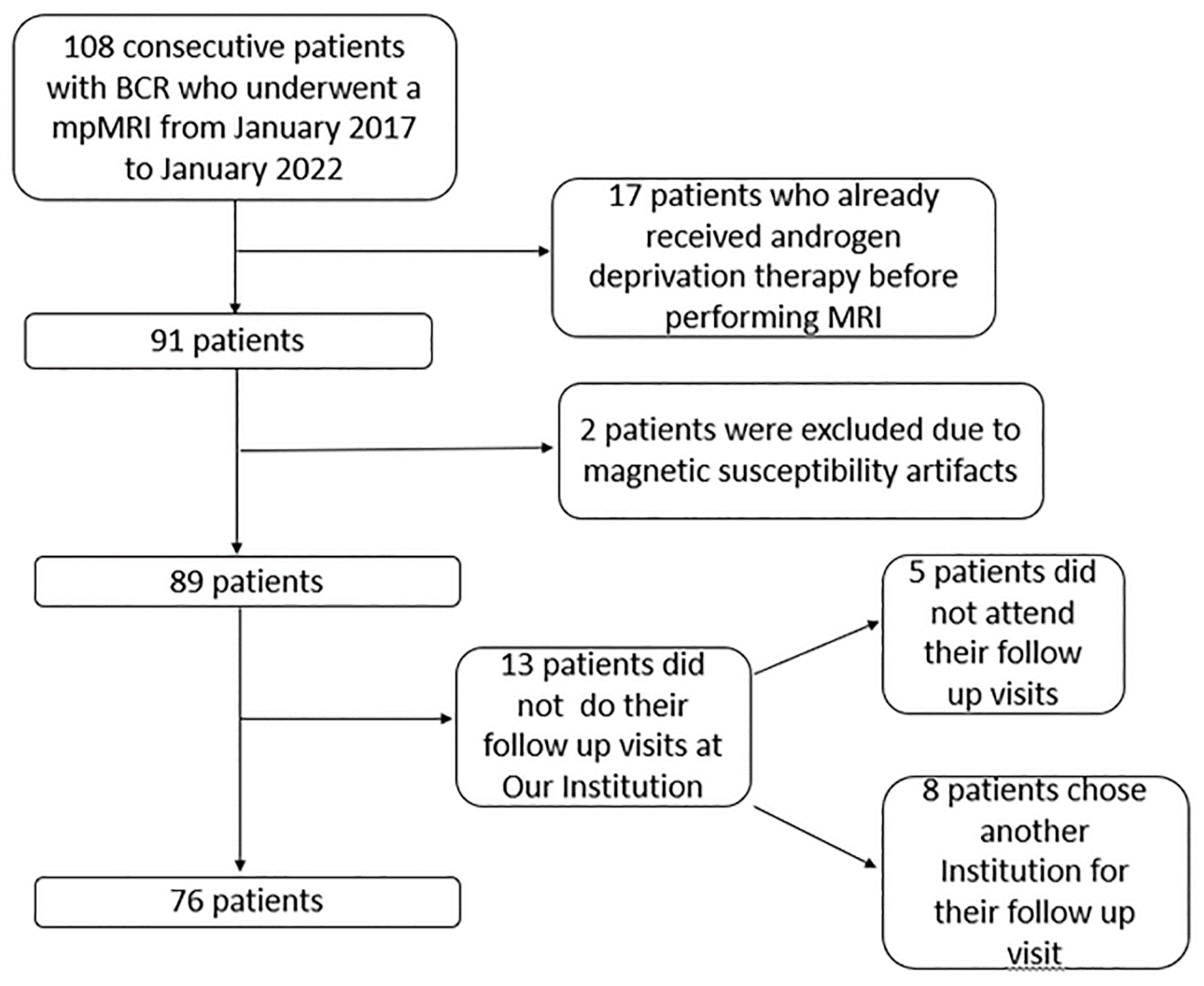
2.1. Patient Sample and Study Design
2.2. Exclusion Criteria
2.3. MRI Acquisition
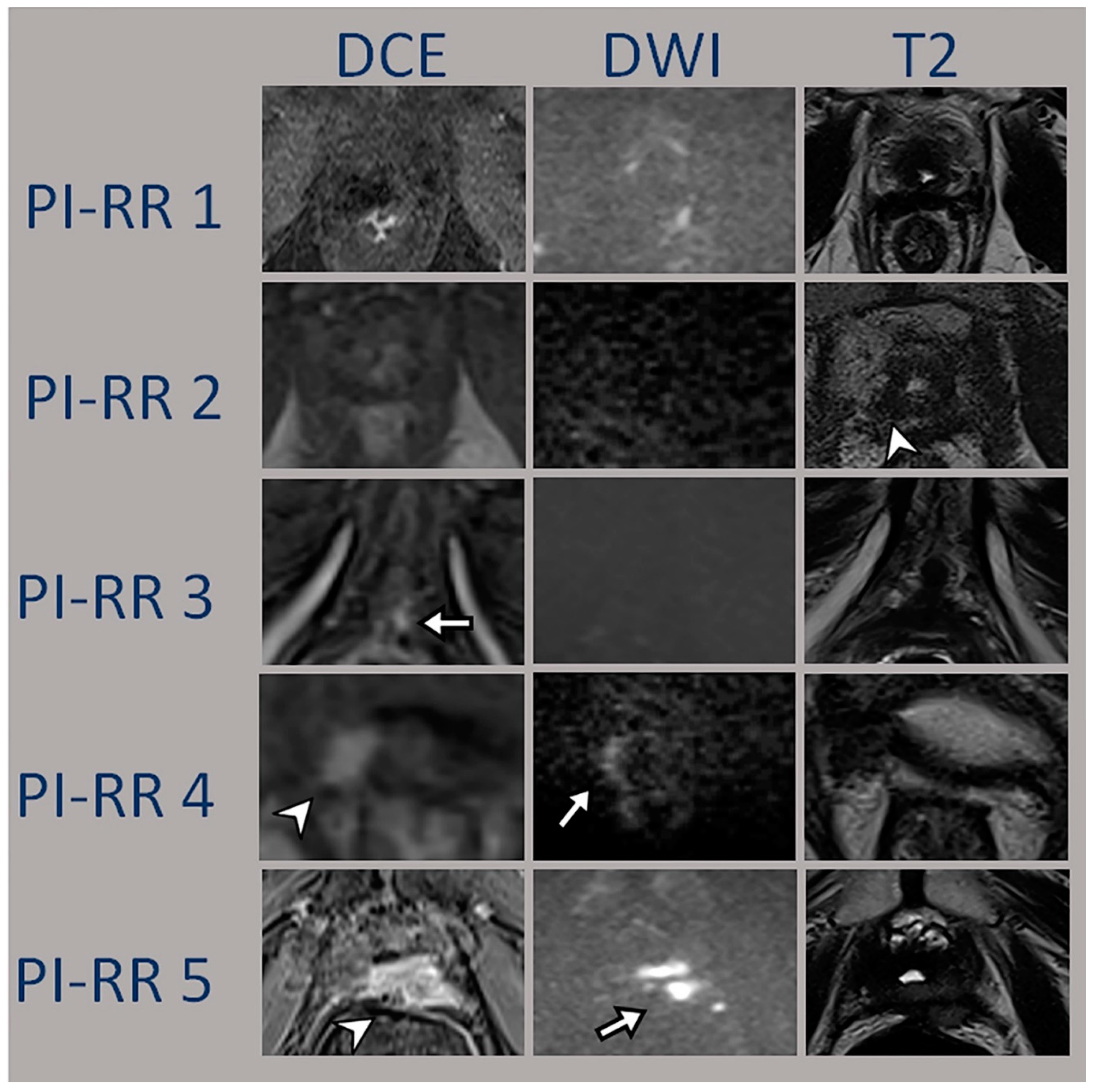
2.4. MRI Analysis
2.5. Reference Standard Definition
2.6. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. MRI Detection Performance
3.3. Correlation Analysis between Local Recurrence and Risk Factors
4. Discussion
4.1. Accuracy
4.2. Agreement
4.3. PET/CT
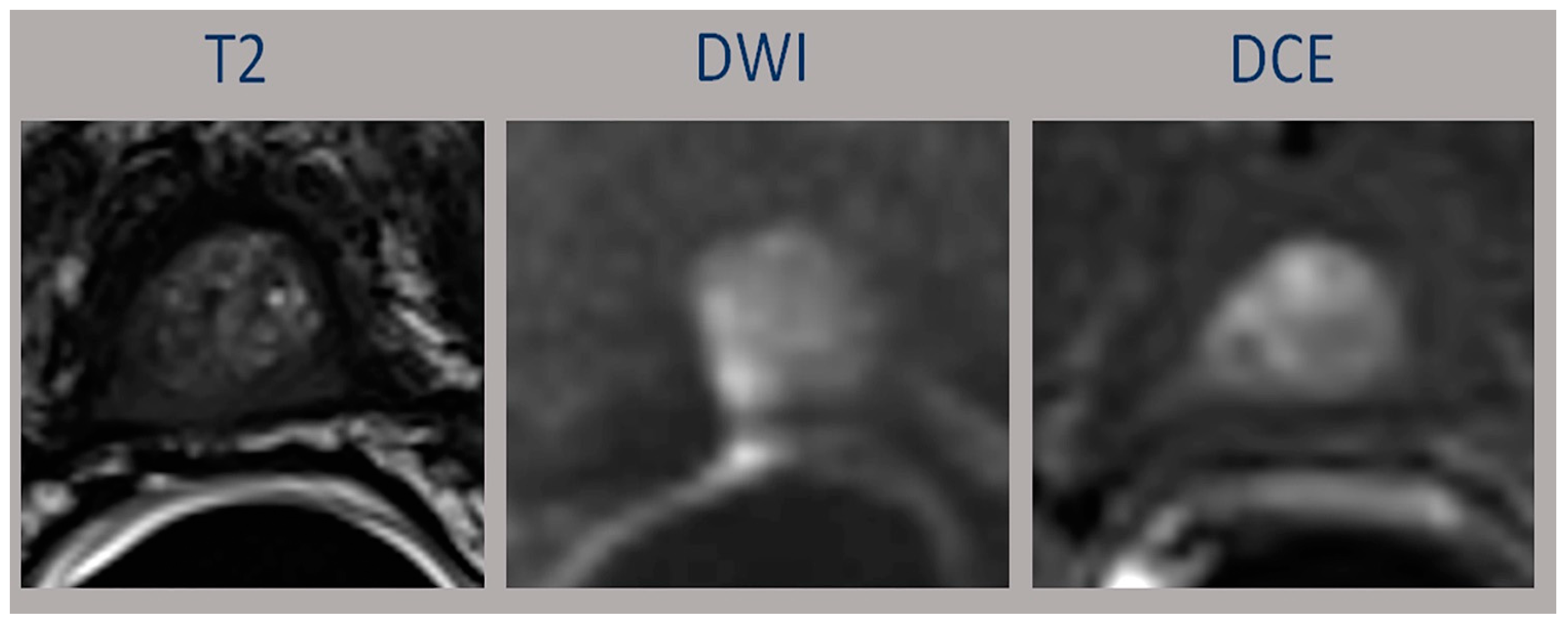
4.4. Pitfalls
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADC | Apparent diffusion coefficient |
| AUC | Area under the curve |
| BCR | biochemical recurrence |
| CI | Confidence Interval |
| DCE | Dynamic contrast-enhanced |
| DWI | Diffusion-weighted imaging |
| ESUR | European Society of Urogenital Radiology |
| FOV | field-of-view |
| IQR | Interquartile range |
| IQR | Interquartile range |
| ISUP | International Society of Urological Pathology |
| LQ | Lower Quartile |
| MRI | Magnetic Resonance Imaging |
| Mp-MRI | Multiparametric Magnetic Resonance Imaging |
| OR | Odds ratio |
| PCa | Prostate cancer |
| PET/CT | Positron Emission Tomography/Computed Tomography |
| PI-RADS | Prostate Imaging Reporting and Data System |
| PSA | Prostate-specific antigen |
| PSMA | Prostate Specific Membrane Antigen |
| RP | Radical prostatectomy |
| RT | Radiotherapy |
| TE | Time of echo |
| TR | Time of repetition |
| UP | Upper Quartile |
References
- Suardi, N.; Porter, C.R.; Reuther, A.M.; Walz, J.; Kodama, K.; Gibbons, R.P.; Correa, R.; Montorsi, F.; Graefen, M.; Huland, H.; et al. A nomogram predicting long-term biochemical recurrence after radical prostatectomy. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2008, 112, 1254–1263. [Google Scholar] [CrossRef]
- Bianchi, L.; Schiavina, R.; Borghesi, M.; Casablanca, C.; Chessa, F.; Bianchi, F.M.; Pultrone, C.; Vagnoni, V.; Ercolino, A.; Dababneh, H.; et al. Patterns of positive surgical margins after open radical prostatectomy and their association with clinical recurrence. Minerva Urol. Nephrol. 2020, 72, 464–473. [Google Scholar] [CrossRef]
- Froemming, A.T.; Verma, S.; Eberhardt, S.C.; Oto, A.; Alexander, L.F.; Allen, B.C.; Coakley, F.V.; Davis, B.J.; Fulgham, P.F.; Hosseinzadeh, K.; et al. ACR Appropriateness Criteria ® Post-treatment Follow-up Prostate Cancer. J. Am. Coll. Radiol. 2018, 15, S132–S149. [Google Scholar] [CrossRef] [Green Version]
- Ljungberg, B.; Albiges, L.; Bensalah, K.; Bex, A.; Giles, R.H.; Hora, M. EAU Guidelines; Edn. Presented at the EAU Annual Congress, Amsterdam, The Netherlands, 1–4 July 2022; EAU Guidelines Office: Arnhem, The Netherlands, 2022; ISBN 978-94-92671-16-5. [Google Scholar]
- Panebianco, V.; Villeirs, G.; Weinreb, J.C.; Turkbey, B.I.; Margolis, D.J.; Richenberg, J.; Schoots, I.G.; Moore, C.M.; Futterer, J.; Macura, K.J.; et al. Prostate Magnetic Resonance Imaging for Local Recurrence Reporting (PI-RR): International Consensus -based Guidelines on Multiparametric Magnetic Resonance Imaging for Prostate Cancer Recur-rence after Radiation Therapy and Radical Prostatectomy. Eur Urol Oncol. 2021, 4, 868–876. [Google Scholar] [CrossRef]
- Pecoraro, M.; Turkbey, B.; Purysko, A.S.; Girometti, R.; Giannarini, G.; Villeirs, G.; Roberto, M.; Catalano, C.; Padhani, A.R.; Barentsz, J.O.; et al. Diagnostic Accuracy and Observer Agreement of the MRI Prostate Imaging for Recurrence Reporting Assessment Score. Radiology 2022, 304, 342–350. [Google Scholar] [CrossRef]
- Ciccarese, F.; Corcioni, B.; Bianchi, L.; De Cinque, A.; Paccapelo, A.; Galletta, G.L.; Schiavina, R.; Brunocilla, E.; Golfieri, R.; Gaudiano, C. Clinical Application of the New Prostate Imaging for Recurrence Reporting (PI-RR) Score Proposed to Evaluate the Local Recurrence of Prostate Cancer after Radical Prostatectomy. Cancers 2022, 14, 4725. [Google Scholar] [CrossRef]
- Paller, C.J.; Antonarakis, E.S. Management of biochemically recurrent prostate cancer after local therapy: Evolving standards of care and new directions. Clin. Adv. Hematol. Oncol. HO 2013, 11, 14–23. [Google Scholar]
- Roach, M.; Hanks, G.; Thames, H.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. 2006, 65, 965–974. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System version 2.1: 2019 update of Prostate Imaging Reporting and Data System version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- De Visschere, P.J.; Standaert, C.; Fütterer, J.J.; Villeirs, G.M.; Panebianco, V.; Walz, J.; Maurer, T.; Hadaschik, B.A.; Lecouvet, F.E.; Giannarini, G. A systematic review on the role of imaging in early recurrent prostate cancer. Eur. Urol. Oncol. 2019, 2, 47–76. [Google Scholar] [CrossRef]
- Liauw, S.L.; Pitroda, S.P.; Eggener, S.E.; Stadler, W.M.; Pelizzari, C.A.; Vannier, M.W.; Oto, A. Evaluation of the Prostate Bed for Local Recurrence After Radical Prostatectomy Using Endorectal Magnetic Resonance Imaging. Int. J. Radiat. Oncol. Biol Phys. 2013, 85, 378–384. [Google Scholar] [CrossRef]
- Sandgren, K.; Westerlinck, P.; Jonsson, J.H.; Blomqvist, L.; Karlsson, C.T.; Nyholm, T.; Dirix, P. Imaging for the Detection of Locoregional Recurrences in Biochemical Progression After Radical Prostatectomy—A Systematic Review. Eur. Urol. Focus 2019, 5, 550–560. [Google Scholar] [CrossRef]
- Rouvière, O.; Valette, O.; Grivolat, S.; Colin-Pangaud, C.; Bouvier, R.; Chapelon, J.Y.; Gelet, A.; Lyonnet, D. Recurrent prostate cancer after external beam radiotherapy: Value of con-trast-enhanced dynamic MRI in localizing intraprostatic tumor—correlation with biopsy findings. Urology 2004, 63, 922–927. [Google Scholar] [CrossRef]
- Tsechelidis, I.; Vrachimis, A. PSMA PET in Imaging Prostate Cancer. Front. Oncol. 2022, 12. [Google Scholar] [CrossRef]
- Radzina, M.; Tirane, M.; Roznere, L.; Zemniece, L.; Dronka, L.; Kalnina, M.; Mamis, E.; Biederer, J.; Lietuvietis, V.; Freimanis, A.; et al. Accuracy of 68Ga-PSMA-11 PET/CT and multiparametric MRI for the detection of local tumor and lymph node metastases in early biochemical recurrence of prostate cancer. Am. J. Nucl. Med. Mol. Imaging 2020, 10, 106–118. [Google Scholar]
- Mottaghy, F.M.; Heinzel, A.; Verburg, F.A. Molecular imaging using PSMA PET/CT versus multiparametric MRI for initial staging of prostate cancer: Comparing apples with oranges? Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1397–1399. [Google Scholar] [CrossRef]
- Lindenberg, L.; Mena, E.; Turkbey, B.; Shih, J.H.; Reese, S.E.; Harmon, S.A.; Lim, I.; Lin, F.; Ton, A.; McKinney, Y.L.; et al. Evaluating biochemically recurrent prostate cancer: Histologic validation of 18 F-DCFPyL PET/CT with comparison to multiparametric MRI. Radiology 2020, 296, 564–572. [Google Scholar] [CrossRef]
- Panebianco, V.; Turkbey, B. Magnetic resonance imaging for prostate cancer recurrence: It’s time for precision diagnostic with Prostate Imaging for Recurrence Reporting (PI-RR) score. Eur. Radiol. 2022, 33, 1–4. [Google Scholar] [CrossRef]
- Rouvière, O.; Vitry, T.; Lyonnet, D. Imaging of prostate cancer local recurrences: Why and how? Eur. Radiol. 2010, 20, 1254–1266. [Google Scholar] [CrossRef]
- Sella, T.; Schwartz, L.H.; Swindle, P.W.; Onyebuchi, C.N.; Scardino, P.T.; Scher, H.I.; Hricak, H. Suspected local recurrence after radical prostatectomy: Endorectal coil MR imaging. Radiology 2004, 231, 379–385. [Google Scholar] [CrossRef]
- Potretzke, T.A.; Froemming, A.T.; Gupta, R.T. Post-treatment prostate MRI. Abdom. Imaging 2019, 45, 2184–2197. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Takahashi, N.; Karnes, R.J. Prostatic Remnant After Prostatectomy: MR Findings and Prevalence in Clinical Practice. Am. J. Roentgenol. 2020, 214, W37–W43. [Google Scholar] [CrossRef] [PubMed]
- Olivier, P.; Giraudet, A.-L.; Skanjeti, A.; Merlin, C.; Weinmann, P.; Rudolph, I.; Hoepping, A.; Gauthé, M. Phase III study of18F-PSMA-1007 versus18F-fluorocholine PET/CT for localization of prostate cancer biochemical recurrence: A prospective, randomized, cross-over, multicenter study. J. Nucl. Med. 2022, 64, 264743. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Reader 1 | Reader 2 | Reader 3 | |
|---|---|---|---|
| Sens | 68.4 (51.3–82.5) | 71.1 (54.1–84.6) | 71.1 (54.1–84.6) |
| Spec | 81.6 (65.7–92.3) | 89.5 (75.2–97.1) | 86.8 (71.9–95.6) |
| AUC | 0.75 (0.65–0.85) | 0.80 (0.71–0.89) | 0.79 (0.70–0.88) |
| PPV | 78.8 (61.1–91) | 87.1 (70.2–96.4) | 84.4 (67.2–94.7) |
| NPV | 72.1 (56.3–84.7) | 75.6 (60.5–87.1) | 75 (59.7–86.8) |
| Univariable OR (95% CI); p-Value | Multivariable ^ OR (95% CI); p-Value | |
|---|---|---|
| Age (1-year) | 1.10 (1.01–1.19); p = 0.026 | |
| Gleason (1-point) | 0.67 (0.39–1.14); p = 0.14 | |
| Stage of disease | ||
| <T3 | 1.00 (ref) | |
| ≥T3 | 0.59 (0.24–1.46); p = 0.25 | |
| Therapy | ||
| PR | 1.00 (ref) | |
| RT | 8.35 (0.97–71.65); p = 0.053 | |
| R | ||
| 0 | 1.00 (ref) | |
| 1 | 1.23 (0.32–4.72); p = 0.76 | |
| PSA | 2.69 (1.05–6.92); p = 0.040 | 2.22 (0.88–5.53); p = 0.088 |
| PSA in RP § | 2.25 (0.88–5.72); p = 0.089 | |
| Score | ||
| <3 | 1.00 (ref) | 1.00 (ref) |
| ≥3 (Reader 1) | 9.59 (3.30–27.92); p < 0.001 | |
| ≥3 (Reader 2) | 20.86 (5.97–72.89); p < 0.001 | |
| ≥3 (Reader 3) | 16.20 (5.01–52.36); p < 0.001 | 7.72 (2.17–27.44); p = 0.002 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bergaglio, C.; Giasotto, V.; Marcenaro, M.; Barra, S.; Turazzi, M.; Bauckneht, M.; Casaleggio, A.; Sciabà, F.; Terrone, C.; Mantica, G.; et al. The Role of mpMRI in the Assessment of Prostate Cancer Recurrence Using the PI-RR System: Diagnostic Accuracy and Interobserver Agreement in Readers with Different Expertise. Diagnostics 2023, 13, 387. https://doi.org/10.3390/diagnostics13030387
Bergaglio C, Giasotto V, Marcenaro M, Barra S, Turazzi M, Bauckneht M, Casaleggio A, Sciabà F, Terrone C, Mantica G, et al. The Role of mpMRI in the Assessment of Prostate Cancer Recurrence Using the PI-RR System: Diagnostic Accuracy and Interobserver Agreement in Readers with Different Expertise. Diagnostics. 2023; 13(3):387. https://doi.org/10.3390/diagnostics13030387
Chicago/Turabian StyleBergaglio, Chiara, Veronica Giasotto, Michela Marcenaro, Salvina Barra, Marianna Turazzi, Matteo Bauckneht, Alessandro Casaleggio, Francesca Sciabà, Carlo Terrone, Guglielmo Mantica, and et al. 2023. "The Role of mpMRI in the Assessment of Prostate Cancer Recurrence Using the PI-RR System: Diagnostic Accuracy and Interobserver Agreement in Readers with Different Expertise" Diagnostics 13, no. 3: 387. https://doi.org/10.3390/diagnostics13030387