
Styloid Jugular Nutcracker: The Possible Role of the Styloid Process Spatial Orientation—A Preliminary Morphometric Computed Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
- -
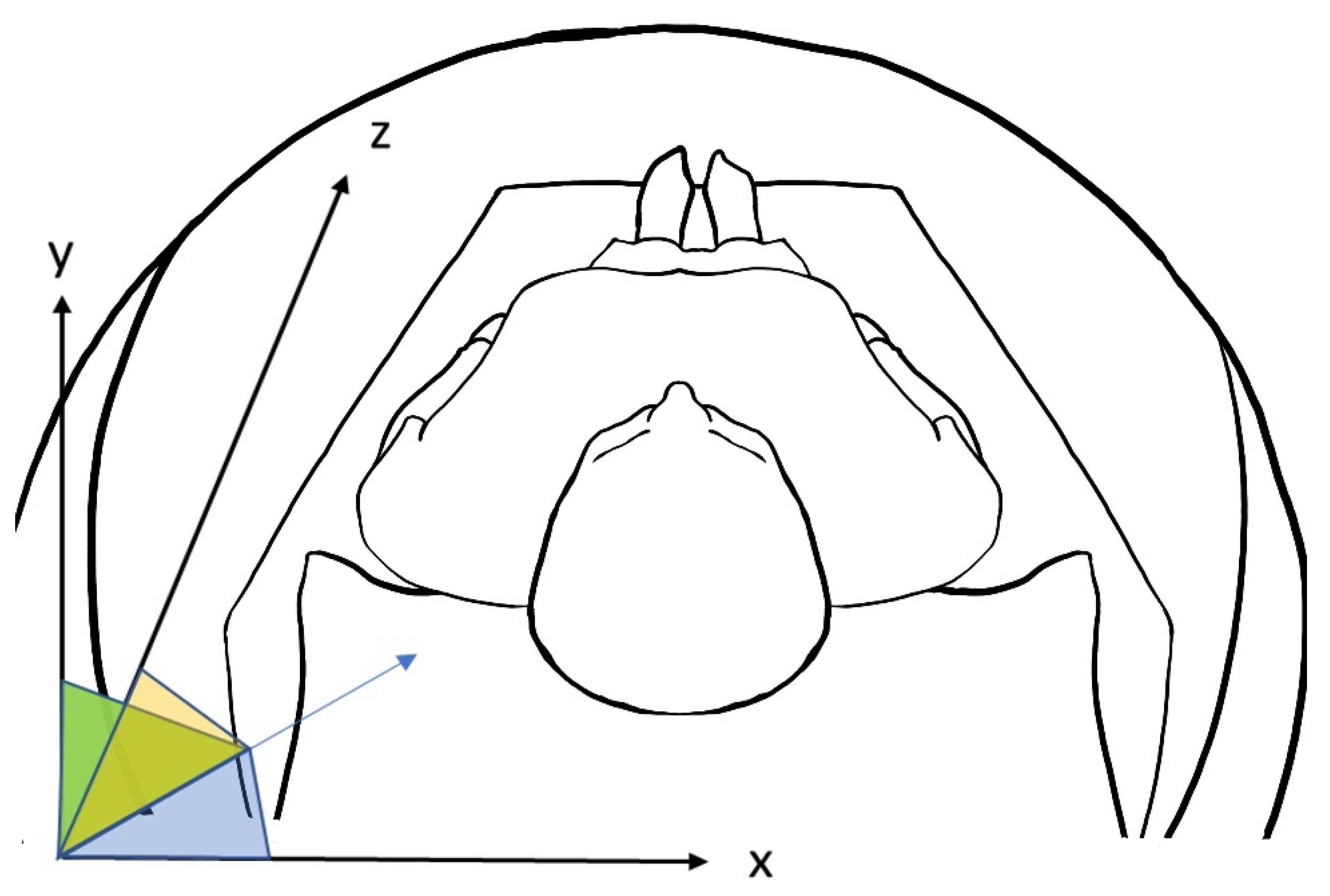
- Angle on x-axis: the angle between the styloid major axis and the x-axis. Visually, it is the direction from lateral to medial. The bigger this angle, the lesser the medial direction of the styloid bone.
- -
- Angle on y-axis: the angle between the styloid major axis and the y-axis. Visually, it is the direction from back to nose. The bigger this angle, the lesser the anterior direction of the styloid bone.
- -
- Angle on z-axis: the angle between the styloid major axis and the z-axis. Visually, it is the direction from head to feet. The bigger this angle, lesser the inferior direction of the styloid bone.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zamboni, P.; Scerrati, A.; Menegatti, E.; Galeotti, R.; Lapparelli, M.; Traina, L.; Tessari, M.; Ciorba, A.; De Bonis, P.; Pelucchi, S. The eagle jugular syndrome. BMC Neurol. 2019, 19, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusco, D.J.; Asteraki, S.; Spetzler, R.F. Eagle’s syndrome: Embryology, anatomy, and clinical management. Acta Neurochir. 2012, 154, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Piagkou, M.; Anagnostopoulou, S.; Kouladouros, K.; Piagkos, G. Eagle’s syndrome: A review of the literature. Clin. Anat. N. Y. 2009, 22, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Sisman, Y.; Gokce, C.; Sipahioglu, M. Bilateral Elongated Styloid Process in an End-stage Renal Disease Patient with Peritoneal Dialysis: Is there Any Role for Ectopic Calcification? Eur. J. Dent. 2009, 3, 155–157. [Google Scholar] [CrossRef] [Green Version]
- Lengele, B.; Dhem, A. Microradiographic and histological study of the styloid process of the temporal bone. Acta Anat. 1989, 135, 193–199. [Google Scholar] [CrossRef]
- Guo, B.; Jaovisidha, S.; Sartoris, D.J.; Ryu, K.N.; Berthiaume, M.J.; Clopton, P.; Brossman, J.; Resnick, D. Correlation between ossification of the stylohyoid ligament and osteophytes of the cervical spine. J. Rheumatol. 1997, 24, 1575–1581. [Google Scholar]
- Ferrario, V.F.; Sigurta, D.; Daddona, A.; Dalloca, L.; Miani, A.; Tafuro, F.; Sforza, C. Calcification of the stylohyoid ligament: Incidence and morphoquantitative evaluations. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 524–529. [Google Scholar] [CrossRef]
- Saccomanno, S.; Quinzi, V.; D’Andrea, N.; Albani, A.; Paskay, L.C.; Marzo, G. Traumatic Events and Eagle Syndrome: Is There Any Correlation? A Systematic Review. Healthcare 2021, 9, 825. [Google Scholar] [CrossRef]
- Petrović, B.; Radak, Đ.; Kostić, V.; Čovičković-Šternić, N. Styloid syndrome: A review of literature. Srp. Arh. Celok. Lek. 2008, 136, 667–674. [Google Scholar] [CrossRef]
- Balbuena, L.; Hayes, D.; Ramirez, S.G.; Johnson, R. Eagle’s syndrome (elongated styloid process). South Med. J. 1997, 90, 331–334. [Google Scholar] [CrossRef]
- de Souza Carvalho, A.C.G.; Filho, O.M.; Garcia, I.R.; de Holanda, M.E.; de Menezes, J.M.S. Intraoral approach for surgical treatment of Eagle syndrome. Br. J. Oral Maxillofac. Surg. 2009, 47, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, A.H.; Berke, G.S.; Chhetri, D.K. Heterogeneity in the clinical presentation of Eagle’s syndrome. Otolaryngol.–Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg. 2006, 134, 389–393. [Google Scholar] [CrossRef]
- Ramadan, S.M. Stylocarotid syndrome causing middle cerebral artery infarction. J. R. Coll. Physicians Edinb. 2021, 51, 380–381. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Celada, W.R.; Jin, D.; Neves, G.; Windisch, T. Bilateral carotid dissection due to Eagle syndrome in a young female. eNeurologicalSci 2021, 24, 100353. [Google Scholar] [CrossRef] [PubMed]
- Baldino, G.; Di Girolamo, C.; De Blasis, G.; Gori, A. Eagle Syndrome and Internal Carotid Artery Dissection: Description of Five Cases Treated in Two Italian Institutions and Review of the Literature. Ann. Vasc. Surg. 2020, 67, 565.e17–565.e24. [Google Scholar] [CrossRef]
- Farhat, H.I.; Elhammady, M.S.; Ziayee, H.; Aziz-Sultan, M.A.; Heros, R.C. Eagle syndrome as a cause of transient ischemic attacks. J. Neurosurg. 2009, 110, 90–93. [Google Scholar] [CrossRef]
- Gervickas, A.; Kubilius, R.; Sabalys, G. Clinic, Diagnostics and Treatment Pecularities of Eagle’s syndrome. Stomatol. Balt. Dent. Maxillofac. J. 2004, 6, 11–13. [Google Scholar]
- HWoo, G.; Ryu, J.; Kim, E.J.; Lee, K.M. Styloidogenic jugular venous compression syndrome as a source of cerebral venous sinus thrombosis. Quant. Imaging Med. Surg. 2022, 12, 4316–4319. [Google Scholar] [CrossRef]
- Scerrati, A.; Norri, N.; Mongardi, L.; Dones, F.; Ricciardi, L.; Trevisi, G.; Menegatti, E.; Zamboni, P.; Cavallo, M.A.; De Bonis, P. Styloidogenic-cervical spondylotic internal jugular venous compression, a vascular disease related to several clinical neurological manifestations: Diagnosis and treatment—A comprehensive literature review. Ann. Transl. Med. 2021, 9, 718. [Google Scholar] [CrossRef]
- Zamboni, P.; Galeotti, R. The chronic cerebrospinal venous insufficiency syndrome. Phlebology 2010, 25, 269–279. [Google Scholar] [CrossRef]
- Gadda, G.; Taibi, A.; Sisini, F.; Gambaccini, M.; Zamboni, P.; Ursino, M. A new hemodynamic model for the study of cerebral venous outflow. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H217–H231. [Google Scholar] [CrossRef] [PubMed]
- Scerrati, A.; De Bonis, P.; Zamboni, P.; Dones, F.; Fontanella, M.; Cenzato, M.; Visani, J.; Bianchi, F.; Zanin, L.; Cavallo, M.A.; et al. A New Insight in Nonaneurysmal Subarachnoid Hemorrhage: The Potential Role of the Internal Jugular Veins. J. Neurol. Surg. Part Cent. Eur. Neurosurg. 2021, 83, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, G.; Della Pepa, G.M.; Scerrati, A.; Maira, G.; Rollo, M.; Albanese, A.; Marchese, E. Anatomical variants of the basal vein of Rosenthal: Prevalence in idiopathic subarachnoid hemorrhage. Acta Neurochir. 2014, 156, 45–51. [Google Scholar] [CrossRef]
- Yamakawa, H.; Ohe, N.; Yano, H.; Yoshimura, S.; Iwama, T. Venous drainage patterns in perimesencephalic nonaneurysmal subarachnoid hemorrhage. Clin. Neurol. Neurosurg. 2008, 110, 587–591. [Google Scholar] [CrossRef]
- Ho, S.; Luginbuhl, A.; Finden, S.; Curry, J.M.; Cognetti, D.M. Styloid/C1 transverse process juxtaposition as a cause of Eagle’s syndrome. Head Neck 2015, 37, E153–E156. [Google Scholar] [CrossRef] [PubMed]
- Monsour, P.A.; Young, W.G. Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg. Oral Med. Oral Pathol. 1986, 61, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Balcioglu, H.A.; Kilic, C.; Akyol, M.; Ozan, H.; Kokten, G. Length of the styloid process and anatomical implications for Eagle’s syndrome. Folia Morphol. 2009, 68, 265–270. [Google Scholar]
- Rechtweg, J.S.; Wax, M.K. Eagle’s syndrome: A review. Am. J. Otolaryngol. 1998, 19, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Werne, S. Studies in spontaneous atlas dislocation. Acta Orthop. Scand. Suppl. 1957, 23, 1–150. [Google Scholar] [CrossRef]
- Steel, H. Anatomical and mechanical considerations of the atlantoaxial articulations. J. Bone Jt. Surg. Am. 1968, 50, 1481–1482. [Google Scholar]
- Jayaraman, V.M.; Boxerman, J.L.; Davis, L.M.; Haas, R.A.; Rogg, J.M. Incidence of extrinsic compression of the internal jugular vein in unselected patients undergoing CT angiography. AJNR Am. J. Neuroradiol. 2012, 33, 1247–1250. [Google Scholar] [CrossRef] [Green Version]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Anaconda Software Distribution. Disponibile su. 2020. Available online: https://docs.anaconda.com/ (accessed on 1 September 2020).
- Buch, K.; Groller, R.; Nadgir, R.N.; Fujita, A.; Qureshi, M.M.; Sakai, O. Variability in the Cross-Sectional Area and Narrowing of the Internal Jugular Vein in Patients Without Multiple Sclerosis. AJR Am. J. Roentgenol. 2016, 206, 1082–1086. [Google Scholar] [CrossRef] [PubMed]
- Fritch, C.; Voronovich, Z.; Carlson, A.P. C1 Transverse Process Resection for Management of Jugular Stenosis. Oper. Neurosurg. Hagerstown Md 2020, 19, E209–E213. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.N.; Garnett, M.R.; Pickard, J.D.; Axon, P.R. An Evaluation of Styloidectomy as an Adjunct or Alternative to Jugular Stenting in Idiopathic Intracranial Hypertension and Disturbances of Cranial Venous Outflow. J. Neurol. Surg. Part B Skull Base 2017, 78, 158–163. [Google Scholar] [CrossRef] [Green Version]
- Nogueira-Reis, F.; de Oliveira Reis, L.; Fontenele, R.C.; Freitas, D.Q.; Tabchoury, C.P.M. Prevalence and features of elongated styloid process on imaging studies: A systematic review and meta-analysis. Clin. Oral Investig. 2022, 26, 1199–1215. [Google Scholar] [CrossRef] [PubMed]
- De Bonis, P.; Menegatti, E.; Cavallo, M.A.; Sisini, F.; Trapella, G.; Scerrati, A.; Zamboni, P. JEDI (jugular entrapment, dilated ventricles, intracranial hypertension) syndrome: A new clinical entity? A case report. Acta Neurochir. 2019, 161, 1367–1370. [Google Scholar] [CrossRef]
- Zhao, X.; Cavallo, C.; Hlubek, R.J.; A Mooney, M.; Belykh, E.; Gandhi, S.; Moreira, L.B.; Lei, T.; Albuquerque, F.C.; Preul, M.C.; et al. Styloidogenic Jugular Venous Compression Syndrome: Clinical Features and Case Series. Oper. Neurosurg. Hagerstown Md 2019, 17, 554–561. [Google Scholar] [CrossRef]
- Mejia-Vergara, A.J.; Sultan, W.; Kostas, A.; Mulholland, C.B.; Sadun, A. Styloidogenic Jugular Venous Compression Syndrome with Papilloedema: Case Report and Review of the Literature. Neuro-Ophthalmol. 2021, 46, 54–58. [Google Scholar] [CrossRef]
- Dashti, S.R.; Nakaji, P.; Hu, Y.C.; Frei, D.F.; Abla, A.A.; Yao, T.; Fiorella, D.; Ogungbo, B. Styloidogenic jugular venous compression syndrome: Diagnosis and treatment: Case report. Neurosurgery 2012, 70, E795–E799. [Google Scholar] [CrossRef] [Green Version]
- Sultan, S.; Acharya, Y.; Soliman, O.; Hynes, N. Stylohyoid Eagle syndrome and EXTracranial INternal Carotid arTery pseudoaneurysms (EXTINCT) with internal jugular vein nutcracker syndrome: A challenging clinical scenario. BMJ Case Rep. 2022, 15, e249558. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, P.; Galeotti, R.; Menegatti, E.; Malagoni, A.M.; Gianesini, S.; Bartolomei, I.; Mascoli, F.; Salvi, F. A prospective open-label study of endovascular treatment of chronic cerebrospinal venous insufficiency. J. Vasc. Surg. 2009, 50, 1348–1358.e1-e3. [Google Scholar] [CrossRef] [PubMed]
- Lehrman, J.N.; Narayanan, M.; Cavallo, C.; Newcomb, A.G.; Zhao, X.; Kelly, B.P.; Crawford, N.R.; Nakaji, P. Evaluation of abnormal styloid anatomy as a cause of internal jugular vein compression using a 3D-printed model: A laboratory investigation. J. Clin. Neurosci. 2020, 72, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Rashid, A.; Iqrar, S.A.; Rashid, A.; Simka, M. Results of Numerical Modeling of Blood Flow in the Internal Jugular Vein Exhibiting Different Types of Strictures. Diagnostics 2022, 12, 2862. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex (M/F) | Mean Age (M/F, years) | |
|---|---|---|
| Case (n = 8) | 4/4 | 73/61.5 |
| Control (n = 8) | 4/4 | 73/61.5 |
| Variables | Overall Sample | Eagle Syndrome | No Eagle Syndrome | p-Value * |
|---|---|---|---|---|
| (n=32) | (n=15) | (n=12) | ||
| Styloid-C1 process (mm): | ||||
| Minimum distance, mean (SD) | 7.72 (3.47) | 8.03 (3.59) | 7.44 (3.44) | 0.7 |
| Maximum distance, mean (SD) | 84.7 (14.4) | 87.9 (7.97) | 81.7 (18.1) | 0.5 |
| Average distance, mean (SD) | 45.2 (2.76) | 45.3 (2.52) | 45.2 (3.03) | 0.9 |
| Styloid-angle (degrees): | ||||
| x-axis, mean (SD) | 90.7 (15.7) | 90.6 (16.4) | 90.7 (15.5) | 0.9 |
| y-axis, mean (SD) | 74.2 (16.9) | 83.3 (19.5) | 66.1 (8.40) | 0.005 |
| z-axis, mean (SD) | 26.9 (8.60) | 24.9 (7.44) | 28.7 (9.37) | 0.2 |
| Right-left styloid processes (mm): | (n=16) | (n=7) | (n=9) | |
| Minimum distance, mean (SD) | 63.2 (12.4) | 66.5(5.32) | 60.7 (15.9) | 0.8 |
| Maximum distance, mean (SD) | 89.7 (6.86) | 91.7 (8.51) | 88.2 (5.27) | 0.6 |
| Average distance, mean (SD) | 77.7 (3.84) | 78.5 (3.23) | 77.1 (4.33) | 0.6 |
| * Kruskal-Wallis test; SD: standard deviation. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, G.; Zangrossi, P.; Flacco, M.E.; Di Domenico, G.; Nastro Siniscalchi, E.; De Ponte, F.S.; Maugeri, R.; De Bonis, P.; Cavallo, M.A.; Zamboni, P.; et al. Styloid Jugular Nutcracker: The Possible Role of the Styloid Process Spatial Orientation—A Preliminary Morphometric Computed Study. Diagnostics 2023, 13, 298. https://doi.org/10.3390/diagnostics13020298
Mantovani G, Zangrossi P, Flacco ME, Di Domenico G, Nastro Siniscalchi E, De Ponte FS, Maugeri R, De Bonis P, Cavallo MA, Zamboni P, et al. Styloid Jugular Nutcracker: The Possible Role of the Styloid Process Spatial Orientation—A Preliminary Morphometric Computed Study. Diagnostics. 2023; 13(2):298. https://doi.org/10.3390/diagnostics13020298
Chicago/Turabian StyleMantovani, Giorgio, Pietro Zangrossi, Maria Elena Flacco, Giovanni Di Domenico, Enrico Nastro Siniscalchi, Francesco Saverio De Ponte, Rosario Maugeri, Pasquale De Bonis, Michele Alessandro Cavallo, Paolo Zamboni, and et al. 2023. "Styloid Jugular Nutcracker: The Possible Role of the Styloid Process Spatial Orientation—A Preliminary Morphometric Computed Study" Diagnostics 13, no. 2: 298. https://doi.org/10.3390/diagnostics13020298