
Predicting Extrathyroidal Extension in Papillary Thyroid Carcinoma Using a Clinical-Radiomics Nomogram Based on B-Mode and Contrast-Enhanced Ultrasound

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
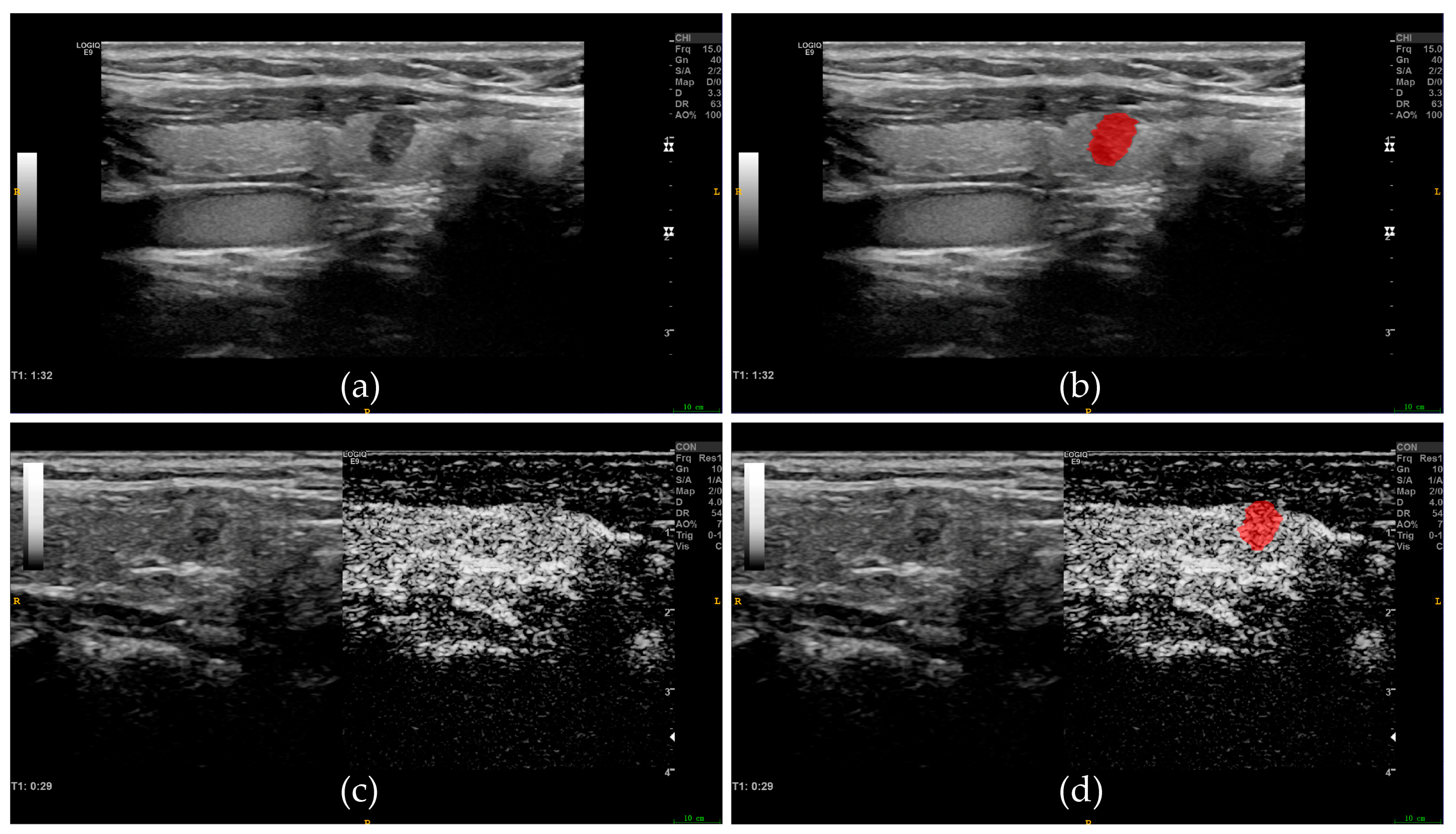
2.2. BMUS and CEUS Examination
2.3. Clinicoradiological Data Acquisition
2.4. Image Segmentation and Feature Extraction
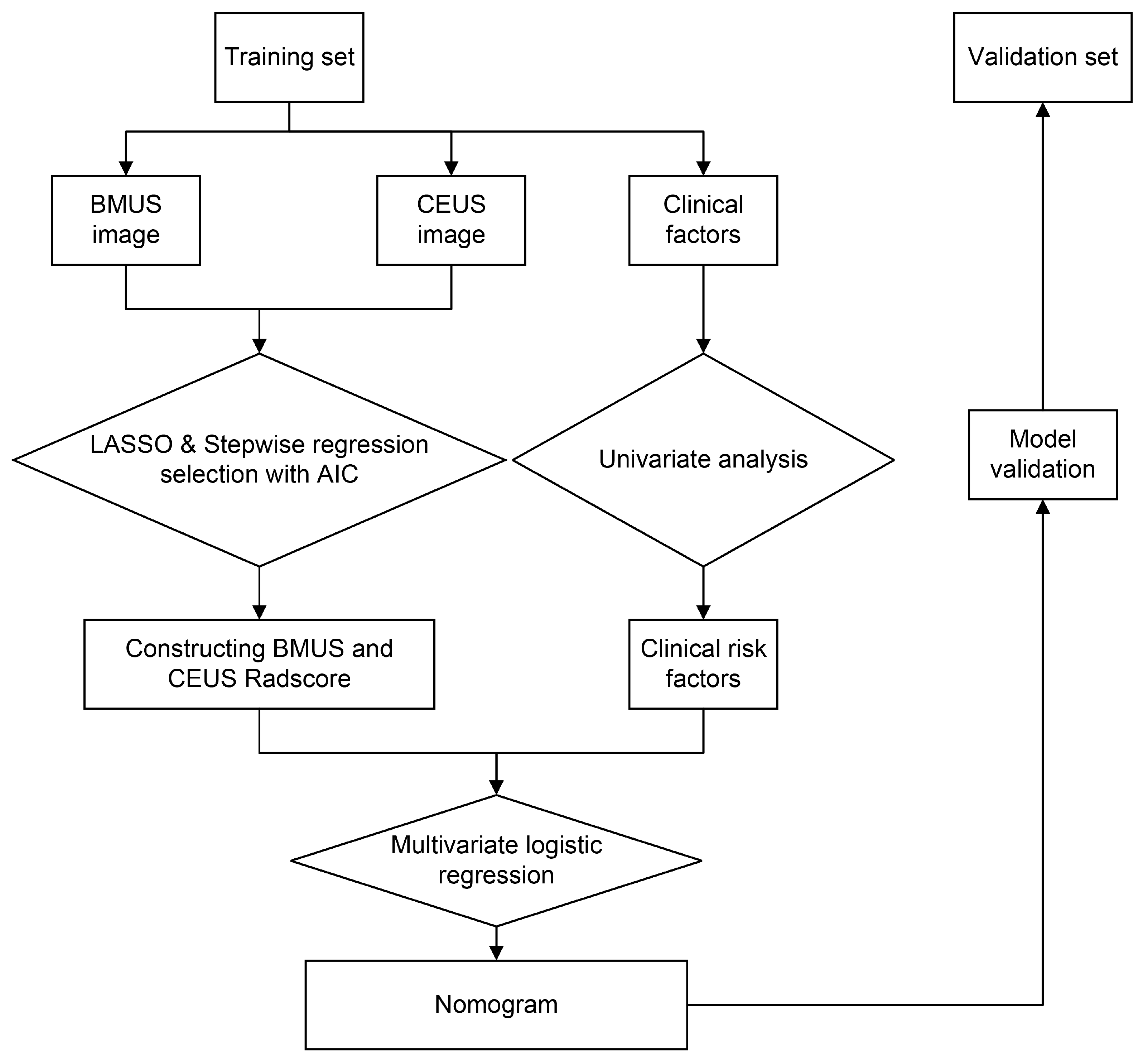
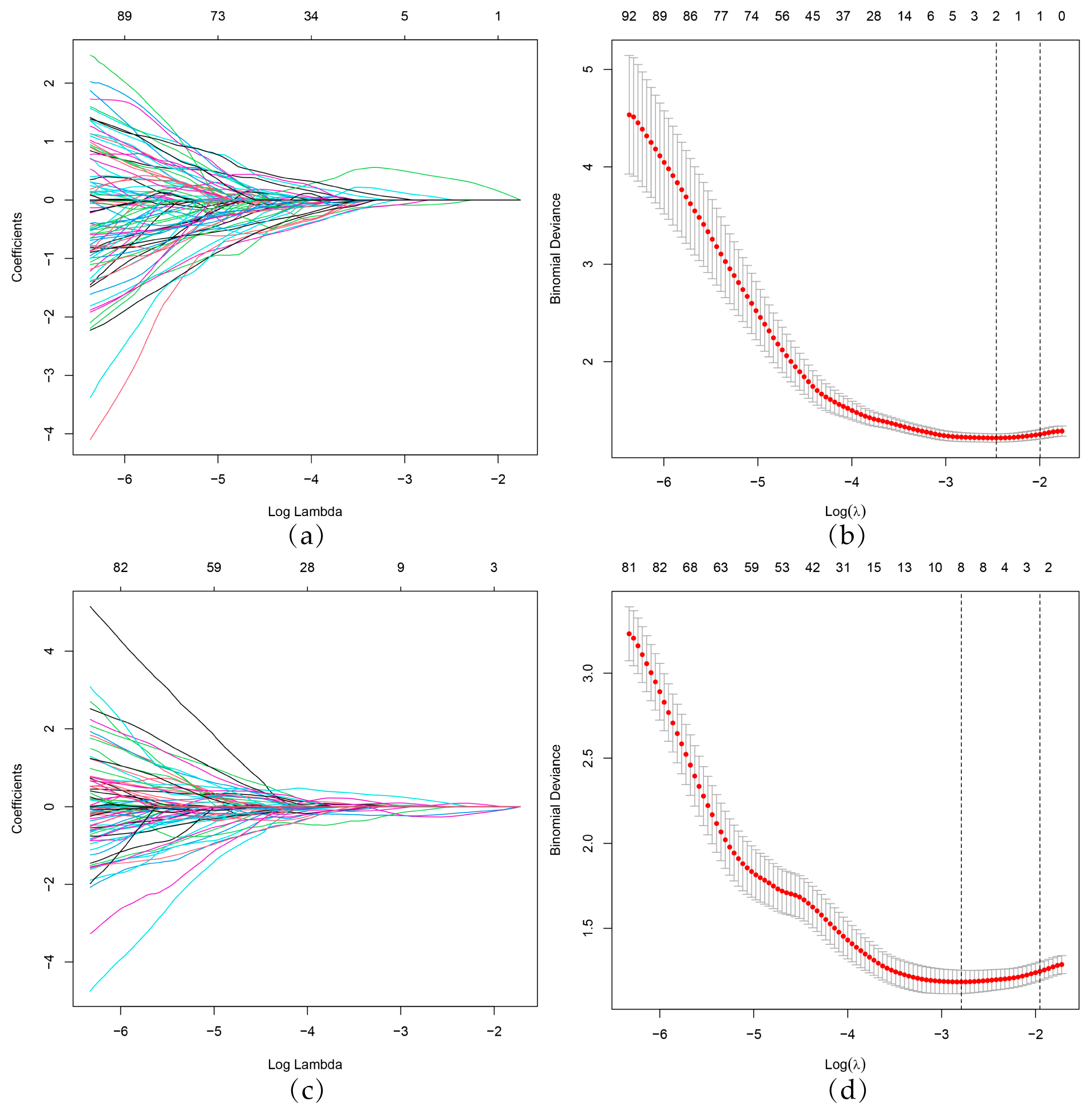
2.5. Feature Selection and Model Construction
2.6. Model Comparison and Nomogram Development
2.7. Statistical Analysis
3. Results
3.1. Clinico-Pathological Information
3.2. Radiomics Scores
wavelet.HLL_gldm_DependenceVariance + 0.5294 × wavelet.HLL_ngtdm_Complexity
3.3. Clinical Model
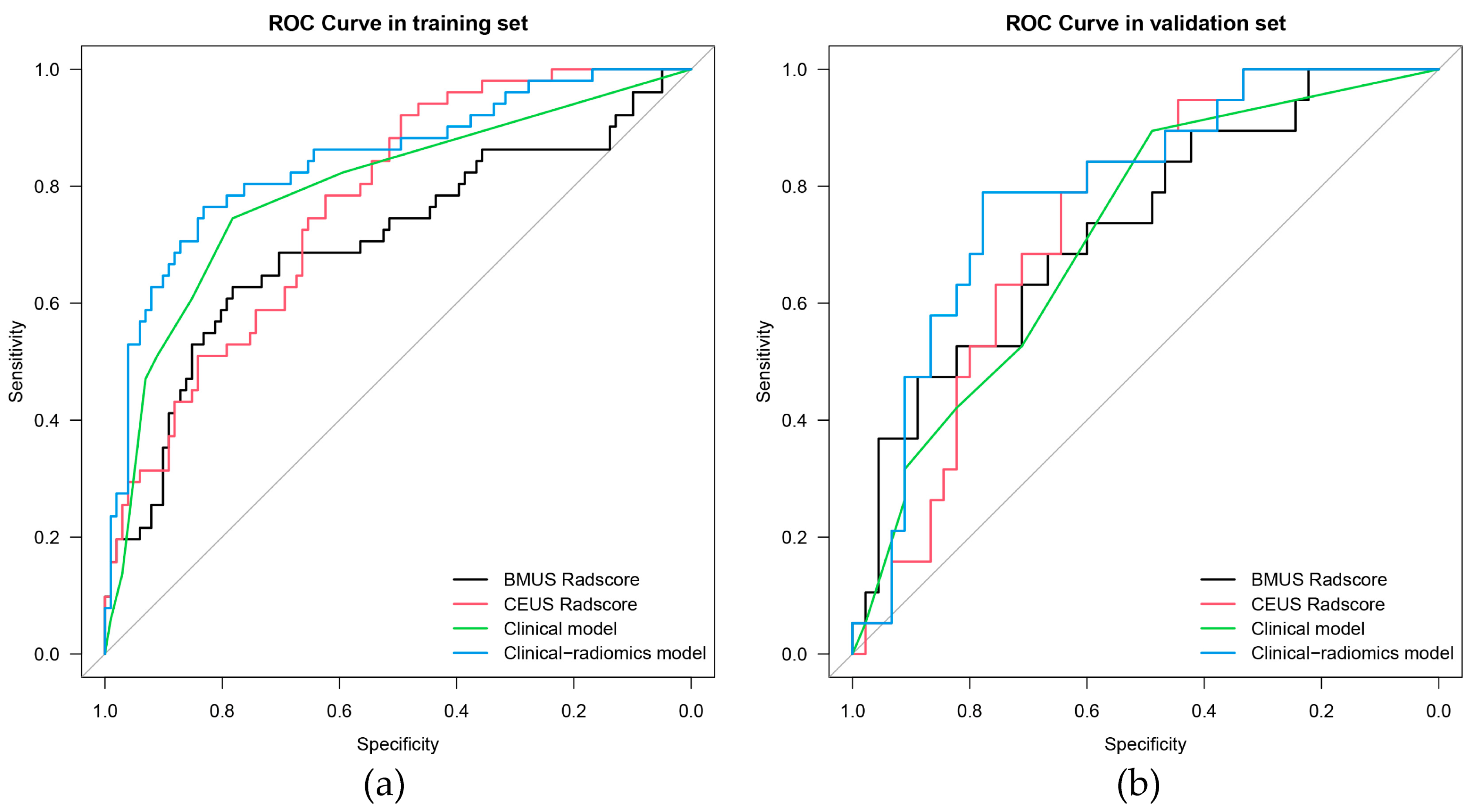
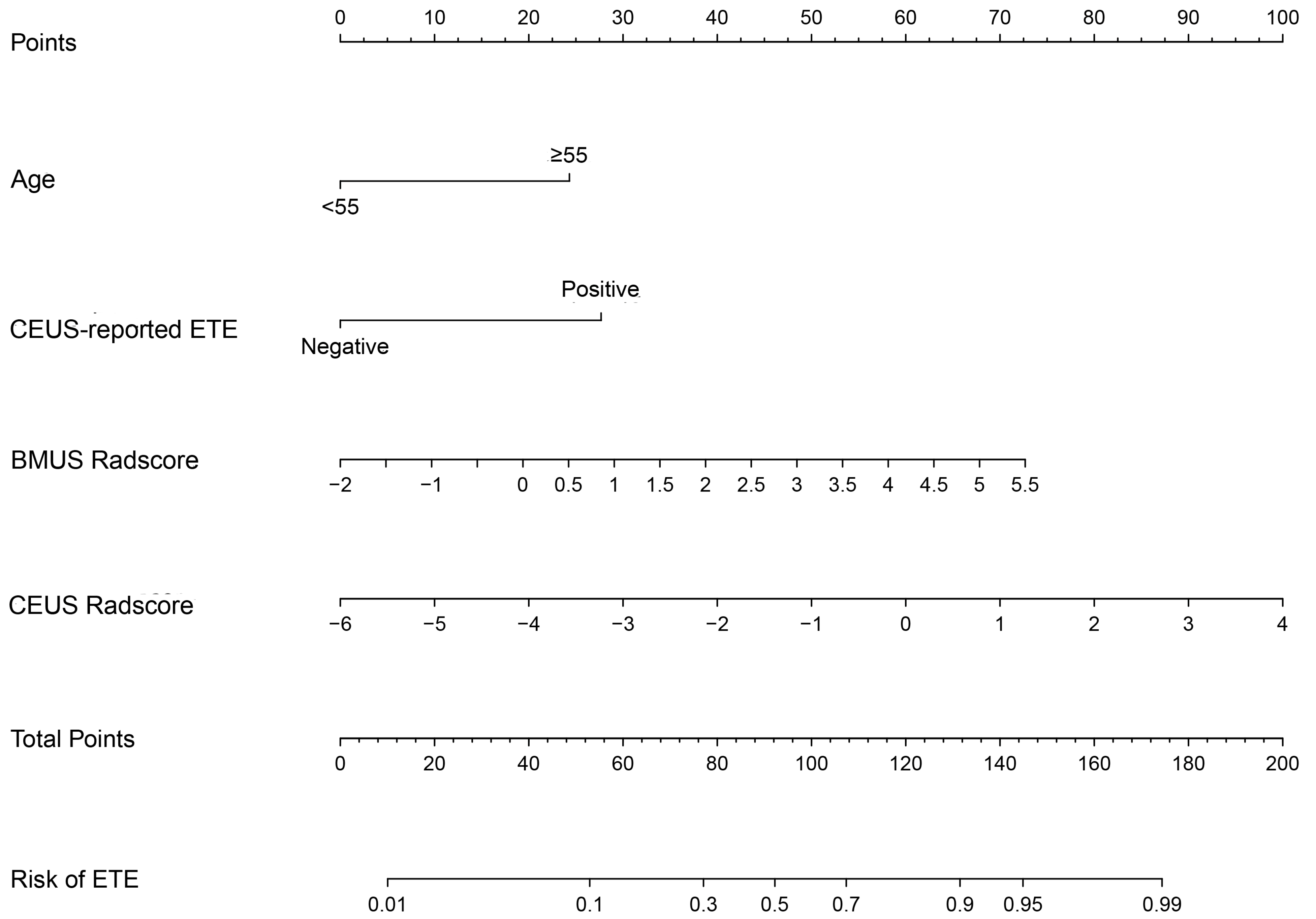
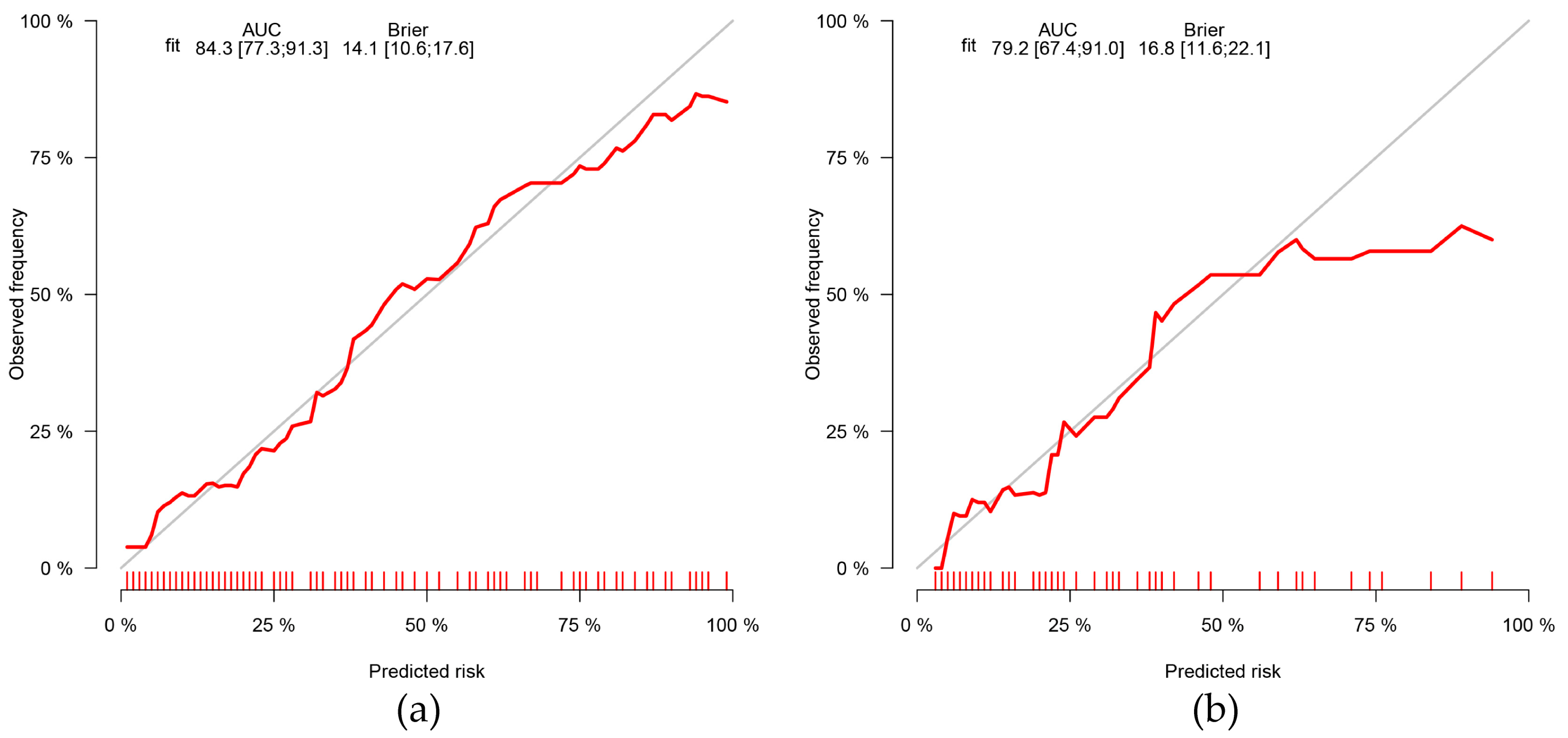
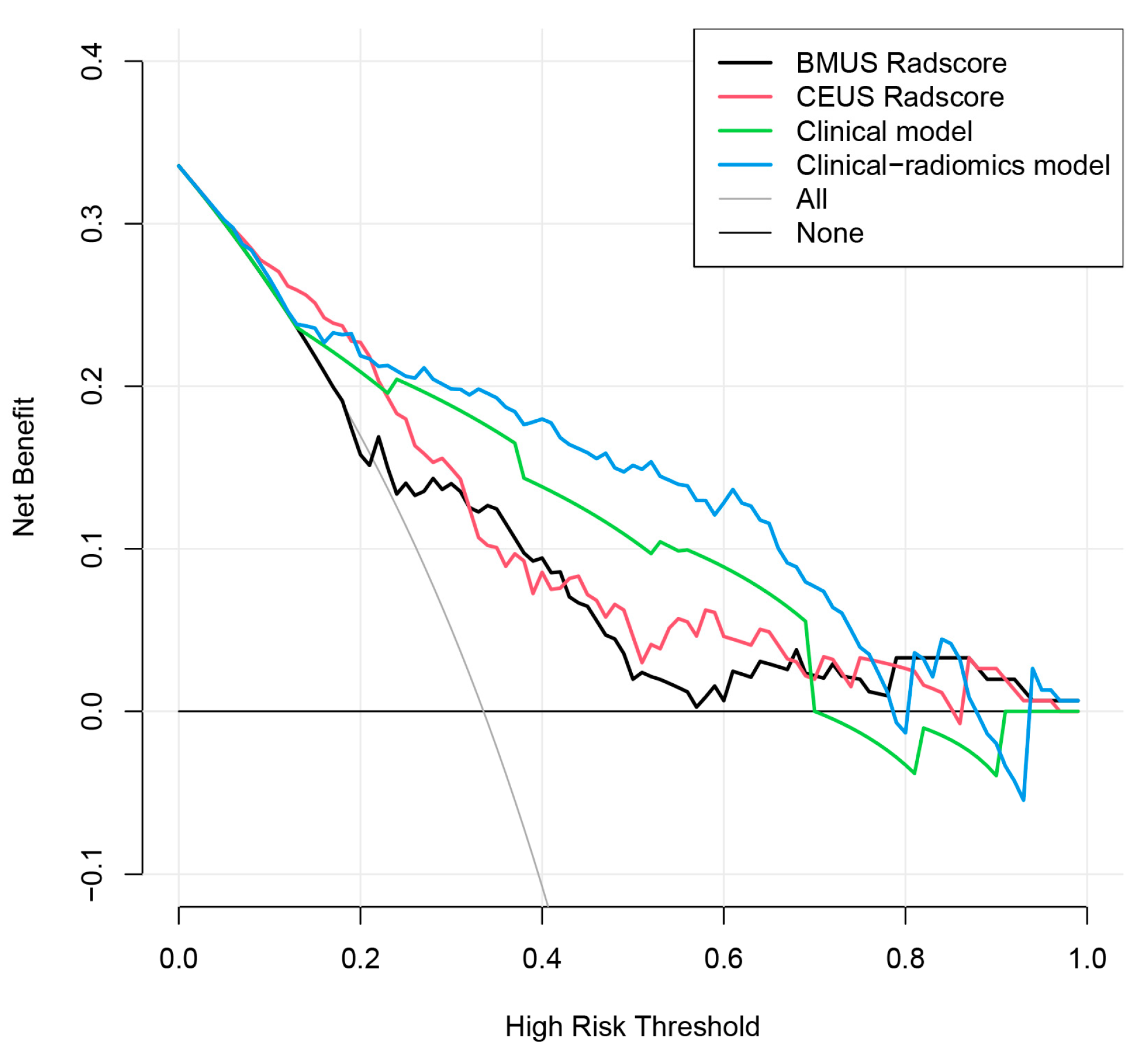
3.4. Clinical-Radiomics Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, H.; Kwon, H.; Moon, B.I. Predictors of Recurrence in Patients with Papillary Thyroid Carcinoma: Does Male Sex Matter? Cancers 2022, 14, 1896. [Google Scholar] [CrossRef] [PubMed]
- Bulfamante, A.M.; Lori, E.; Bellini, M.I.; Bolis, E.; Lozza, P.; Castellani, L.; Saibene, A.M.; Pipolo, C.; Fuccillo, E.; Rosso, C.; et al. Advanced Differentiated Thyroid Cancer: A Complex Condition Needing a Tailored Approach. Front. Oncol. 2022, 12, 954759. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Sun, W.; Wang, Z.; Dong, W.; He, L.; Zhang, T.; Lv, C.; Zhang, H. RBM47/SNHG5/FOXO3 axis activates autophagy and inhibits cell proliferation in papillary thyroid carcinoma. Cell Death Dis. 2022, 13, 270. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.W.; Pan, H.; Wang, L.; Ye, J.; Jiang, Y.; Qu, Z. Determine the Optimal Extent of Thyroidectomy and Lymphadenectomy for Patients With Papillary Thyroid Microcarcinoma. Front. Endocrinol. 2019, 10, 363. [Google Scholar] [CrossRef]
- Ortiz, S.; Rodriguez, J.M.; Soria, T.; Perez-Flores, D.; Pinero, A.; Moreno, J.; Parrilla, P. Extrathyroid spread in papillary carcinoma of the thyroid: Clinicopathological and prognostic study. Otolaryngol. Head Neck Surg. 2001, 124, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Chen, J.; Zou, J.; Zhu, W.; Zang, Y.; Li, H. Circular RNA coiled-coil domain containing 66 regulates malignant development of papillary thyroid carcinoma by upregulating La ribonucleoprotein 1 via the sponge effect on miR-129-5p. Bioengineered 2022, 13, 7181–7196. [Google Scholar] [CrossRef]
- Shaha, A.R.; Shah, J.P.; Loree, T.R. Risk group stratification and prognostic factors in papillary carcinoma of thyroid. Ann. Surg. Oncol. 1996, 3, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Hay, I.D.; Bergstralh, E.J.; Goellner, J.R.; Ebersold, J.R.; Grant, C.S. Predicting outcome in papillary thyroid carcinoma: Development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 1993, 114, 1050–1057, discussion 1057–1058. [Google Scholar]
- Su, H.K.; Wenig, B.M.; Haser, G.C.; Rowe, M.E.; Asa, S.L.; Baloch, Z.; Du, E.; Faquin, W.C.; Fellegara, G.; Giordano, T.; et al. Inter-Observer Variation in the Pathologic Identification of Minimal Extrathyroidal Extension in Papillary Thyroid Carcinoma. Thyroid 2016, 26, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef]
- Parvathareddy, S.K.; Siraj, A.K.; Annaiyappanaidu, P.; Siraj, N.; Haqawi, W.; Al-Sobhi, S.S.; Al-Dayel, F.; Al-Kuraya, K.S. Tumor size is an independent negative prognostic factor for event free survival in children with differentiated thyroid cancer. Front. Endocrinol. 2022, 13, 979054. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Niu, G.; Li, X.; Ma, F.; Ma, Y.; Hu, S. Lobectomy may be more appropriate for patients with early-stage medullary thyroid cancer older than 60 years old. Front. Endocrinol. 2022, 13, 1015319. [Google Scholar] [CrossRef]
- Huang, H.; Liu, J.; Wang, X.; Liu, S. Outcomes of nonsuspicious contralateral nodules with active surveillance after lobectomy in patients with papillary thyroid carcinoma. Front. Endocrinol. 2022, 13, 941080. [Google Scholar] [CrossRef]
- Haddad, R.I.; Bischoff, L.; Ball, D.; Bernet, V.; Blomain, E.; Busaidy, N.L.; Campbell, M.; Dickson, P.; Duh, Q.Y.; Ehya, H.; et al. Thyroid Carcinoma, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Nat. Compr. Cancer Netw. 2022, 20, 925–951. [Google Scholar] [CrossRef]
- Xu, S.; Ni, X.; Zhou, W.; Zhan, W.; Zhang, H. Development and validation of a novel diagnostic tool for predicting the malignancy probability of thyroid nodules: A retrospective study based on clinical, B-mode, color doppler and elastographic ultrasonographic characteristics. Front. Endocrinol. 2022, 13, 966572. [Google Scholar] [CrossRef]
- Verde, F.; Ponsiglione, A. Role of perfusion features in contrast-enhanced ultrasound differential diagnosis of hepatocellular adenoma and carcinoma: Far beyond the gray-scale ultrasound. J. Clin. Ultrasound 2022, 50, 222–223. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Xi, X.; Gao, Q.; Tang, J.; Yang, X.; Zhu, S.; Zhao, R.; Lai, X.; Zhang, X.; Zhang, B.; et al. Blood-Rich Enhancement in Ultrasonography Predicts Worse Prognosis in Patients With Papillary Thyroid Cancer. Front. Oncol. 2020, 10, 546378. [Google Scholar] [CrossRef]
- Hu, S.; Zhang, H.; Sun, Z.; Ge, Y.; Li, J.; Yu, C.; Deng, Z.; Dou, W.; Wang, X. Preoperative assessment of extrathyroidal extension of papillary thyroid carcinomas by ultrasound and magnetic resonance imaging: A comparative study. La Radiol. Med. 2020, 125, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Bidault, S.; Hadoux, J.; Guerlain, J.; Girard, E.; Breuskin, I.; Attard, M.; Suciu, V.; Baudin, E.; Al Ghuzlan, A.; et al. Can preoperative ultrasound predict extrathyroidal extension of differentiated thyroid cancer? Eur. J. Endocrinol. 2021, 185, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Chen, L.; Liang, Z.; Shao, Y.; Sun, X.; Liu, J. Value of Contrast-Enhanced Ultrasound in the Preoperative Evaluation of Papillary Thyroid Carcinoma Invasiveness. Front. Oncol. 2021, 11, 795302. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, X.; Li, J.; Cai, Q.; Qiao, Z.; Luo, Y.K. Contrast-enhanced ultrasound: A valuable modality for extracapsular extension assessment in papillary thyroid cancer. Eur. Radiol. 2021, 31, 4568–4575. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.W.; Ye, J.; Hong, L.Z.; Hu, J.; Wang, F.; Liu, S.Y.; Jiang, Y.; Qu, Z. Nomograms for the prediction of lateral lymph node metastasis in papillary thyroid carcinoma: Stratification by size. Front. Oncol. 2022, 12, 944414. [Google Scholar] [CrossRef] [PubMed]
- Grani, G.; Cera, G.; Conzo, G.; Del Gatto, V.; di Gioia, C.R.T.; Maranghi, M.; Lucia, P.; Cantisani, V.; Metere, A.; Melcarne, R.; et al. Preoperative Ultrasonography in the Evaluation of Suspected Familial Non-Medullary Thyroid Cancer: Are We Able to Predict Multifocality and Extrathyroidal Extension? J. Clin. Med. 2021, 10, 5277. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef]
- Caruso, D.; Polici, M.; Zerunian, M.; Pucciarelli, F.; Guido, G.; Polidori, T.; Landolfi, F.; Nicolai, M.; Lucertini, E.; Tarallo, M.; et al. Radiomics in Oncology, Part 1: Technical Principles and Gastrointestinal Application in CT and MRI. Cancers 2021, 13, 2522. [Google Scholar] [CrossRef]
- Li, G.; Li, L.; Li, Y.; Qian, Z.; Wu, F.; He, Y.; Jiang, H.; Li, R.; Wang, D.; Zhai, Y.; et al. An MRI radiomics approach to predict survival and tumour-infiltrating macrophages in gliomas. Brain J. Neurol. 2022, 145, 1151–1161. [Google Scholar] [CrossRef]
- Primakov, S.P.; Ibrahim, A.; van Timmeren, J.E.; Wu, G.; Keek, S.A.; Beuque, M.; Granzier, R.W.Y.; Lavrova, E.; Scrivener, M.; Sanduleanu, S.; et al. Automated detection and segmentation of non-small cell lung cancer computed tomography images. Nat. Commun. 2022, 13, 3423. [Google Scholar] [CrossRef]
- Guo, S.Y.; Zhou, P.; Zhang, Y.; Jiang, L.Q.; Zhao, Y.F. Exploring the Value of Radiomics Features Based on B-Mode and Contrast-Enhanced Ultrasound in Discriminating the Nature of Thyroid Nodules. Front. Oncol. 2021, 11, 738909. [Google Scholar] [CrossRef]
- Lu, W.; Zhang, D.; Zhang, Y.; Qian, X.; Qian, C.; Wei, Y.; Xia, Z.; Ding, W.; Ni, X. Ultrasound Radiomics Nomogram to Diagnose Sub-Centimeter Thyroid Nodules Based on ACR TI-RADS. Cancers 2022, 14, 4826. [Google Scholar] [CrossRef]
- Park, V.Y.; Lee, E.; Lee, H.S.; Kim, H.J.; Yoon, J.; Son, J.; Song, K.; Moon, H.J.; Yoon, J.H.; Kim, G.R.; et al. Combining radiomics with ultrasound-based risk stratification systems for thyroid nodules: An approach for improving performance. Eur. Radiol. 2021, 31, 2405–2413. [Google Scholar] [CrossRef]
- Agyekum, E.A.; Ren, Y.Z.; Wang, X.; Cranston, S.S.; Wang, Y.G.; Wang, J.; Akortia, D.; Xu, F.J.; Gomashie, L.; Zhang, Q.; et al. Evaluation of Cervical Lymph Node Metastasis in Papillary Thyroid Carcinoma Using Clinical-Ultrasound Radiomic Machine Learning-Based Model. Cancers 2022, 14, 5266. [Google Scholar] [CrossRef]
- Yu, J.; Deng, Y.; Liu, T.; Zhou, J.; Jia, X.; Xiao, T.; Zhou, S.; Li, J.; Guo, Y.; Wang, Y.; et al. Lymph node metastasis prediction of papillary thyroid carcinoma based on transfer learning radiomics. Nat. Commun. 2020, 11, 4807. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Yu, B.; Li, Y.; Zhang, Y.; Jin, J.; Ai, Y.; Jin, X.; Yang, Y. Models of ultrasonic radiomics and clinical characters for lymph node metastasis assessment in thyroid cancer: A retrospective study. PeerJ 2023, 11, e14546. [Google Scholar] [CrossRef] [PubMed]
- Wen, Q.; Wang, Z.; Traverso, A.; Liu, Y.; Xu, R.; Feng, Y.; Qian, L. A radiomics nomogram for the ultrasound-based evaluation of central cervical lymph node metastasis in papillary thyroid carcinoma. Front. Endocrinol. 2022, 13, 1064434. [Google Scholar] [CrossRef]
- Li, J.; Xia, F.; Wang, X.; Jin, Y.; Yan, J.; Wei, X.; Zhao, Q. Multiclassifier Radiomics Analysis of Ultrasound for Prediction of Extrathyroidal Extension in Papillary Thyroid Carcinoma in Children. Int. J. Med. Sci. 2023, 20, 278–286. [Google Scholar] [CrossRef]
- Wang, X.; Agyekum, E.A.; Ren, Y.; Zhang, J.; Zhang, Q.; Sun, H.; Zhang, G.; Xu, F.; Bo, X.; Lv, W.; et al. A Radiomic Nomogram for the Ultrasound-Based Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma. Front. Oncol. 2021, 11, 625646. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.L.; Guan, Q.; Wen, D.; Ma, B.; Xu, W.B.; Hu, J.Q.; Wei, W.J.; Li, D.S.; Wang, Y.; Xiang, J.; et al. PRDM16 Inhibits Cell Proliferation and Migration via Epithelial-to-Mesenchymal Transition by Directly Targeting Pyruvate Carboxylase in Papillary Thyroid Cancer. Front. Cell Dev. Biol. 2021, 9, 723777. [Google Scholar] [CrossRef]
- Caruso, D.; Polici, M.; Zerunian, M.; Del Gaudio, A.; Parri, E.; Giallorenzi, M.A.; De Santis, D.; Tarantino, G.; Tarallo, M.; Dentice di Accadia, F.M.; et al. Radiomic Cancer Hallmarks to Identify High-Risk Patients in Non-Metastatic Colon Cancer. Cancers 2022, 14, 3438. [Google Scholar] [CrossRef]
- Caruso, D.; Polici, M.; Rinzivillo, M.; Zerunian, M.; Nacci, I.; Marasco, M.; Magi, L.; Tarallo, M.; Gargiulo, S.; Iannicelli, E.; et al. CT-based radiomics for prediction of therapeutic response to Everolimus in metastatic neuroendocrine tumors. La Radiol. Med. 2022, 127, 691–701. [Google Scholar] [CrossRef]
- Stanzione, A.; Cuocolo, R.; Ugga, L.; Verde, F.; Romeo, V.; Brunetti, A.; Maurea, S. Oncologic Imaging and Radiomics: A Walkthrough Review of Methodological Challenges. Cancers 2022, 14, 4871. [Google Scholar] [CrossRef]
- Petrillo, A.; Fusco, R.; Di Bernardo, E.; Petrosino, T.; Barretta, M.L.; Porto, A.; Granata, V.; Di Bonito, M.; Fanizzi, A.; Massafra, R.; et al. Prediction of Breast Cancer Histological Outcome by Radiomics and Artificial Intelligence Analysis in Contrast-Enhanced Mammography. Cancers 2022, 14, 2132. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Shi, D.; Guo, Q.; Zhang, H.; Wang, S.; Ren, K. Radiomics Based on Digital Mammography Helps to Identify Mammographic Masses Suspicious for Cancer. Front. Oncol. 2022, 12, 843436. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Zhu, J.; Qiu, Q.; Wang, Y.; Bai, T.; Yin, Y. Prediction of Immunohistochemistry of Suspected Thyroid Nodules by Use of Machine Learning-Based Radiomics. Am. J. Roentgenol. 2019, 213, 1348–1357. [Google Scholar] [CrossRef] [PubMed]
- Morrison, G.; Buckley, J.; Ostrow, D.; Varghese, B.; Cen, S.Y.; Werbin, J.; Ericson, N.; Cunha, A.; Lu, Y.T.; George, T.; et al. Non-Invasive Profiling of Advanced Prostate Cancer via Multi-Parametric Liquid Biopsy and Radiomic Analysis. Int. J. Mol. Sci. 2022, 23, 2571. [Google Scholar] [CrossRef]
- Eertink, J.J.; van de Brug, T.; Wiegers, S.E.; Zwezerijnen, G.J.C.; Pfaehler, E.A.G.; Lugtenburg, P.J.; van der Holt, B.; de Vet, H.C.W.; Hoekstra, O.S.; Boellaard, R.; et al. (18)F-FDG PET baseline radiomics features improve the prediction of treatment outcome in diffuse large B-cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Sorrenti, S.; Dolcetti, V.; Radzina, M.; Bellini, M.I.; Frezza, F.; Munir, K.; Grani, G.; Durante, C.; D’Andrea, V.; David, E.; et al. Artificial Intelligence for Thyroid Nodule Characterization: Where Are We Standing? Cancers 2022, 14, 3357. [Google Scholar] [CrossRef]
- Yang, C.; Jiang, Z.; Cheng, T.; Zhou, R.; Wang, G.; Jing, D.; Bo, L.; Huang, P.; Wang, J.; Zhang, D.; et al. Radiomics for Predicting Response of Neoadjuvant Chemotherapy in Nasopharyngeal Carcinoma: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 893103. [Google Scholar] [CrossRef]
- Polici, M.; Laghi, A.; Caruso, D. Editorial for Special Issue on Imaging Biomarker in Oncology. Cancers 2023, 15, 1071. [Google Scholar] [CrossRef]
- Chen, B.; Zhong, L.; Dong, D.; Zheng, J.; Fang, M.; Yu, C.; Dai, Q.; Zhang, L.; Tian, J.; Lu, W.; et al. Computed Tomography Radiomic Nomogram for Preoperative Prediction of Extrathyroidal Extension in Papillary Thyroid Carcinoma. Front. Oncol. 2019, 9, 829. [Google Scholar] [CrossRef]
- Yu, P.; Wu, X.; Li, J.; Mao, N.; Zhang, H.; Zheng, G.; Han, X.; Dong, L.; Che, K.; Wang, Q.; et al. Extrathyroidal Extension Prediction of Papillary Thyroid Cancer With Computed Tomography Based Radiomics Nomogram: A Multicenter Study. Front. Endocrinol. 2022, 13, 874396. [Google Scholar] [CrossRef]
- Xu, X.Q.; Zhou, Y.; Su, G.Y.; Tao, X.W.; Ge, Y.Q.; Si, Y.; Shen, M.P.; Wu, F.Y. Iodine Maps from Dual-Energy CT to Predict Extrathyroidal Extension and Recurrence in Papillary Thyroid Cancer Based on a Radiomics Approach. Am. J. Neuroradiol. 2022, 43, 748–755. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhang, H.; Wang, X.; Sun, Z.; Ge, Y.; Wang, K.; Yu, C.; Deng, Z.; Feng, J.; Xu, X.; et al. A pilot study of radiomics signature based on biparametric MRI for preoperative prediction of extrathyroidal extension in papillary thyroid carcinoma. J. X-ray Sci. Technol. 2021, 29, 171–183. [Google Scholar] [CrossRef]
- Wei, R.; Wang, H.; Wang, L.; Hu, W.; Sun, X.; Dai, Z.; Zhu, J.; Li, H.; Ge, Y.; Song, B. Radiomics based on multiparametric MRI for extrathyroidal extension feature prediction in papillary thyroid cancer. BMC Med. Imaging 2021, 21, 20. [Google Scholar] [CrossRef] [PubMed]
- Romeo, V.; Cuocolo, R.; Apolito, R.; Stanzione, A.; Ventimiglia, A.; Vitale, A.; Verde, F.; Accurso, A.; Amitrano, M.; Insabato, L.; et al. Clinical value of radiomics and machine learning in breast ultrasound: A multicenter study for differential diagnosis of benign and malignant lesions. Eur. Radiol. 2021, 31, 9511–9519. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Gan, F.; Gan, M.; Deng, H.; Chen, X.; Yuan, X.; Huang, D.; Liu, S.; Qin, B.; Wei, Y.; et al. Predicting the Risk of Diabetic Foot Ulcers From Diabetics With Dysmetabolism: A Retrospective Clinical Trial. Front. Endocrinol. 2022, 13, 929864. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yu, X.; Li, W.; Li, Y.; Yang, J.; Hu, Z.; Wang, Y.; Chen, P.; Li, W.; Chen, Y. Development and validation of a nomogram for predicting late-onset sepsis in preterm infants on the basis of thyroid function and other risk factors: Mixed retrospective and prospective cohort study. J. Adv. Res. 2020, 24, 43–51. [Google Scholar] [CrossRef]
- Han, M.; Sun, Y.; Zhao, W.; Xiang, G.; Wang, X.; Jiang, Z.; Xue, Z.; Zhou, W. Comprehensive characterization of TNFSF14/LIGHT with implications in prognosis and immunotherapy of human gliomas. Front. Immunol. 2022, 13, 1025286. [Google Scholar] [CrossRef]
- Scarpi, E.; Nanni, O.; Maltoni, M. Development and Validation of the PaP Score Nomogram for Terminally Ill Cancer Patients. Cancers 2022, 14, 2510. [Google Scholar] [CrossRef]
- Li, Q.; Jiang, T.; Zhang, C.; Zhang, Y.; Huang, Z.; Zhou, H.; Huang, P. A nomogram based on clinical information, conventional ultrasound and radiomics improves prediction of malignant parotid gland lesions. Cancer Lett. 2022, 527, 107–114. [Google Scholar] [CrossRef]
- Zhang, S.; Duan, C.; Zhou, X.; Liu, F.; Wang, X.; Shao, Q.; Gao, Y.; Duan, F.; Zhao, R.; Wang, G. Radiomics nomogram for prediction of microvascular invasion in hepatocellular carcinoma based on MR imaging with Gd-EOB-DTPA. Front. Oncol. 2022, 12, 1034519. [Google Scholar] [CrossRef]
- Li, Y.; Wang, B.; Wen, L.; Li, H.; He, F.; Wu, J.; Gao, S.; Hou, D. Machine learning and radiomics for the prediction of multidrug resistance in cavitary pulmonary tuberculosis: A multicentre study. Eur. Radiol. 2023, 33, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Li, L.; Liu, S.; Chen, Y.; Liu, C.; Han, Y.; Wang, F.; Zhan, P.; Zhao, H.; Li, J.; et al. Enhanced CT-based radiomics predicts pathological complete response after neoadjuvant chemotherapy for advanced adenocarcinoma of the esophagogastric junction: A two-center study. Insights Into Imaging 2022, 13, 134. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, H.; Qian, C.L.; Lin, M.S.; Li, F.H. Utility of quantitative contrast-enhanced ultrasound for the prediction of extracapsular extension in papillary thyroid carcinoma. Sci. Rep. 2017, 7, 1472. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Training Set (n = 152) | Validation Set (n = 64) | p-Value |
|---|---|---|---|
| Extrathyroidal extension | 0.579 | ||
| Negative | 101 (66.4) | 45 (70.3) | |
| Positive | 51 (33.6) | 19 (29.7) | |
| Age | 0.622 | ||
| <55 years | 124 (81.6) | 54 (84.4) | |
| ≥55 years | 28 (18.4) | 10 (15.6) | |
| Gender | 0.919 | ||
| Female | 113 (74.3) | 48 (75.0) | |
| Male | 39 (25.7) | 16 (25.0) | |
| Primary site | 0.537 | ||
| Left lobe | 66 (43.4) | 31 (48.4) | |
| Right lobe | 76 (50.0) | 31 (48.4) | |
| Isthmus | 10 (6.6) | 2 (3.1) | |
| Tumor size | 0.266 | ||
| ≤10 mm | 100 (65.8) | 37 (57.8) | |
| >10 mm | 52 (34.2) | 27 (42.2) | |
| Echogenicity | 0.120 | ||
| Iso/hyperechoic | 6 (3.9) | 5 (7.8) | |
| Hypoechoic | 53 (34.9) | 29 (45.3) | |
| Marked hypoechoic | 93 (61.2) | 30 (46.9) | |
| Aspect ratio > 1 | 0.381 | ||
| Absent | 95 (62.5) | 44 (68.8) | |
| Present | 57 (37.5) | 20 (31.2) | |
| Margin | 0.133 | ||
| Smooth | 6 (3.9) | 7 (10.9) | |
| Ill-defined | 20 (13.2) | 9 (14.1) | |
| Irregular | 126 (82.9) | 48 (75.0) | |
| Microcalcification | 0.222 | ||
| Absent | 43 (28.3) | 13 (20.3) | |
| Present | 109 (71.7) | 51 (79.7) | |
| Enhancement degree | 0.974 | ||
| Hyper-enhancement | 7 (4.6) | 3 (4.7) | |
| Iso-enhancement | 33 (21.7) | 13 (20.3) | |
| Hypo-enhancement | 112 (73.7) | 48 (75) | |
| BMUS-reported ETE | 0.886 | ||
| Negative | 80 (52.6) | 33 (51.6) | |
| Positive | 72 (47.4) | 31 (48.4) | |
| CEUS-reported ETE | 0.523 | ||
| Negative | 110 (72.4) | 49 (76.6) | |
| Positive | 42 (27.6) | 15 (23.4) | |
| BMUS Radscore, | 0.438 | ||
| Median (interquartile range) | −1.01 (−1.29, −0.48) | −0.90 (−1.30, −0.35) | |
| CEUS Radscore, | 0.317 | ||
| Median (interquartile range) | −0.84 (−1.68, −0.11) | −0.64 (−1.29, −0.03) |
| Characteristics | Training Set | Validation Set | ||||
|---|---|---|---|---|---|---|
| ETE− | ETE+ | p-Value | ETE− | ETE+ | p-Value | |
| Age | 0.003 | 0.466 | ||||
| <55 years | 89 (88.1) | 35 (68.6) | 39 (86.7) | 15 (78.9) | ||
| ≥55 years | 12 (11.9) | 16 (31.4) | 6 (13.3) | 4 (21.1) | ||
| Gender | 0.252 | 0.530 | ||||
| Female | 78 (77.2) | 35 (68.6) | 35 (77.8) | 13 (68.4) | ||
| Male | 23 (22.8) | 16 (31.4) | 10 (22.2) | 6 (31.6) | ||
| Primary site | 0.338 | 1.000 | ||||
| Left lobe | 42 (41.6) | 24 (47.1) | 22 (48.9) | 9 (47.4) | ||
| Right lobe | 54 (53.5) | 22 (43.1) | 21 (46.7) | 10 (52.6) | ||
| Isthmus | 5 (5.0) | 5 (9.8) | 2 (4.4) | 0 (0.0) | ||
| Tumor size | 0.002 | 0.006 | ||||
| >10 mm | 75 (74.3) | 25 (49) | 31 (68.9) | 6 (31.6) | ||
| ≤10 mm | 26 (25.7) | 26 (51) | 14 (31.1) | 13 (68.4) | ||
| Echogenicity | 0.527 | 0.271 | ||||
| Iso/hyperechoic | 5 (5.0) | 1 (2.0) | 3 (6.7) | 2 (10.5) | ||
| Hypoechoic | 37 (36.6) | 16 (31.4) | 18 (40) | 11 (57.9) | ||
| Marked hypoechoic | 59 (58.4) | 34 (66.7) | 24 (53.3) | 6 (31.6) | ||
| Aspect ratio > 1 | 0.690 | 0.531 | ||||
| Absent | 62 (61.4) | 33 (64.7) | 32 (71.1) | 12 (63.2) | ||
| Present | 39 (38.6) | 18 (35.3) | 13 (28.9) | 7 (36.8) | ||
| Margin | 0.467 | 0.108 | ||||
| Smooth | 4 (4.0) | 2 (3.9) | 3 (6.7) | 4 (21.1) | ||
| Ill-defined | 11 (10.9) | 9 (17.6) | 5 (11.1) | 4 (21.1) | ||
| Irregular | 86 (85.1) | 40 (78.4) | 37 (82.2) | 11 (57.9) | ||
| Microcalcification | 0.355 | 0.739 | ||||
| Absent | 31 (30.7) | 12 (23.5) | 10 (22.2) | 3 (15.8) | ||
| Present | 70 (69.3) | 39 (76.5) | 35 (77.8) | 16 (84.2) | ||
| Enhancement degree | 0.230 | 0.298 | ||||
| Hyper-enhancement | 5 (5.0) | 2 (3.9) | 2 (4.4) | 1 (5.3) | ||
| Iso-enhancement | 26 (25.7) | 7 (13.7) | 7 (15.6) | 6 (31.6) | ||
| Hypo-enhancement | 70 (69.3) | 42 (82.4) | 36 (80) | 12 (63.2) | ||
| BMUS-reported ETE | 0.019 | 0.038 | ||||
| Negative | 60 (59.4) | 20 (39.2) | 27 (60.0) | 6 (31.6) | ||
| Positive | 41 (40.6) | 31 (60.8) | 18 (40.0) | 13 (68.4) | ||
| CEUS-reported ETE | <0.001 | 0.117 | ||||
| Negative | 88 (87.1) | 22 (43.1) | 37 (82.2) | 12 (63.2) | ||
| Positive | 13 (12.9) | 29 (56.9) | 8 (17.8) | 7 (36.8) | ||
| BMUS Radscore | <0.001 | 0.004 | ||||
| Median (interquartile range) | −1.11 (−1.31, −0.85) | −0.56 (−1.13, 0.05) | −0.97 (−1.31, −0.61) | −0.36 (−0.93, 0.45) | ||
| CEUS Radscore | <0.001 | 0.003 | ||||
| Median (interquartile range) | −1.28 (−2.00, −0.48) | −0.23 (−0.83, 0.52) | −0.97 (−1.79, −0.28) | −0.09 (−0.60, 0.21) | ||
| Characteristics | Odds Ratio (95%CI) | p-Value |
|---|---|---|
| BMUS radiomics model | ||
| original_ngtdm_Busyness | 2.58 (1.60, 4.15) | <0.001 |
| CEUS radiomics model | ||
| wavelet.LHL_glszm_SmallAreaEmphasis | 1.87 (1.14, 3.08) | 0.013 |
| wavelet.HLL_gldm_DependenceVariance | 0.50 (0.31, 0.79) | 0.003 |
| wavelet.HLL_ngtdm_Complexity | 1.70 (1.11, 2.61) | 0.015 |
| Clinical model | ||
| Age (≥55 years vs. <55 years) | 4.00 (1.52, 10.50) | 0.005 |
| Tumor size (>10 mm vs. ≤10 mm) | 2.08 (0.90, 4.81) | 0.087 |
| CEUS-reported ETE (positive vs. negative) | 7.42 (3.14, 17.56) | <0.001 |
| Clinical-radiomics model | ||
| Age (≥55 years vs. <55 years) | 3.89 (1.45, 10.49) | 0.007 |
| CEUS-reported ETE (positive vs. negative) | 4.70 (1.84, 11.99) | 0.001 |
| BMUS Radscore | 1.72 (0.98, 3.01) | 0.058 |
| CEUS Radscore | 1.75 (1.09, 2.80) | 0.020 |
| Group | Model | AUC (95% CI) | p Value (vs. Combined Model) | Sensitivity | Specificity | Cutoff Value |
|---|---|---|---|---|---|---|
| Training set | BMUS radiomics | 0.704 (0.610–0.799) | <0.001 | 0.627 | 0.782 | 0.305 |
| CEUS radiomics | 0.768 (0.694–0.843) | 0.009 | 0.922 | 0.495 | 0.213 | |
| Clinical | 0.793 (0.715–0.871) | 0.004 | 0.745 | 0.782 | 0.307 | |
| Clinical-radiomics | 0.843 (0.773–0.913) | - | 0.765 | 0.832 | 0.356 | |
| Validation set | BMUS radiomics | 0.731 (0.595–0.867) | 0.343 | 0.632 | 0.689 | 0.305 |
| CEUS radiomics | 0.739 (0.617–0.861) | 0.419 | 0.947 | 0.333 | 0.213 | |
| Clinical | 0.718 (0.588–0.847) | 0.044 | 0.526 | 0.711 | 0.307 | |
| Clinical-radiomics | 0.792 (0.674–0.910) | - | 0.789 | 0.778 | 0.356 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, L.; Guo, S.; Zhao, Y.; Cheng, Z.; Zhong, X.; Zhou, P. Predicting Extrathyroidal Extension in Papillary Thyroid Carcinoma Using a Clinical-Radiomics Nomogram Based on B-Mode and Contrast-Enhanced Ultrasound. Diagnostics 2023, 13, 1734. https://doi.org/10.3390/diagnostics13101734
Jiang L, Guo S, Zhao Y, Cheng Z, Zhong X, Zhou P. Predicting Extrathyroidal Extension in Papillary Thyroid Carcinoma Using a Clinical-Radiomics Nomogram Based on B-Mode and Contrast-Enhanced Ultrasound. Diagnostics. 2023; 13(10):1734. https://doi.org/10.3390/diagnostics13101734
Chicago/Turabian StyleJiang, Liqing, Shiyan Guo, Yongfeng Zhao, Zhe Cheng, Xinyu Zhong, and Ping Zhou. 2023. "Predicting Extrathyroidal Extension in Papillary Thyroid Carcinoma Using a Clinical-Radiomics Nomogram Based on B-Mode and Contrast-Enhanced Ultrasound" Diagnostics 13, no. 10: 1734. https://doi.org/10.3390/diagnostics13101734