
Deep-Learning-Based Segmentation of the Shoulder from MRI with Inference Accuracy Prediction
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
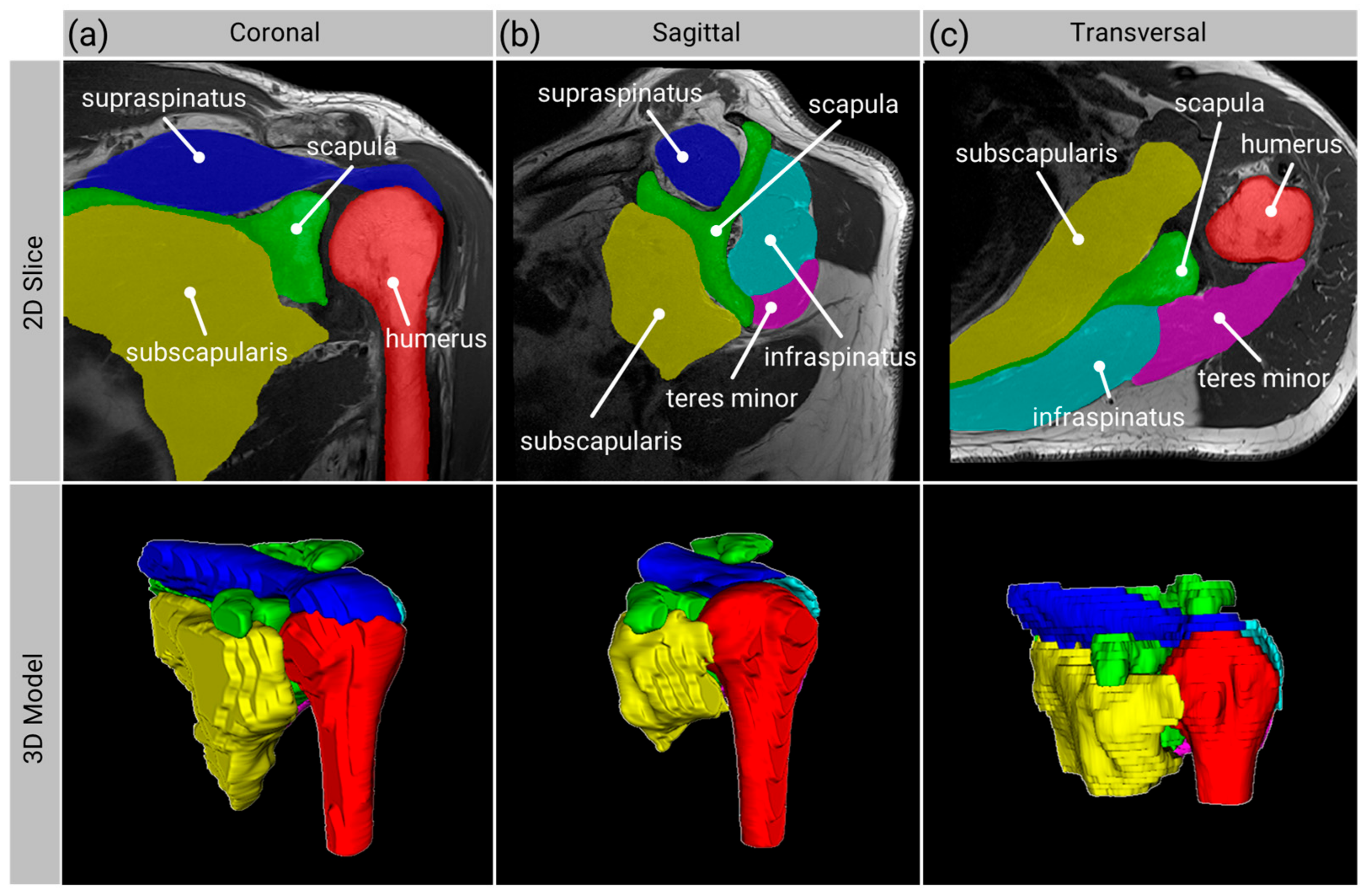
2.1. Anatomy Segmentation
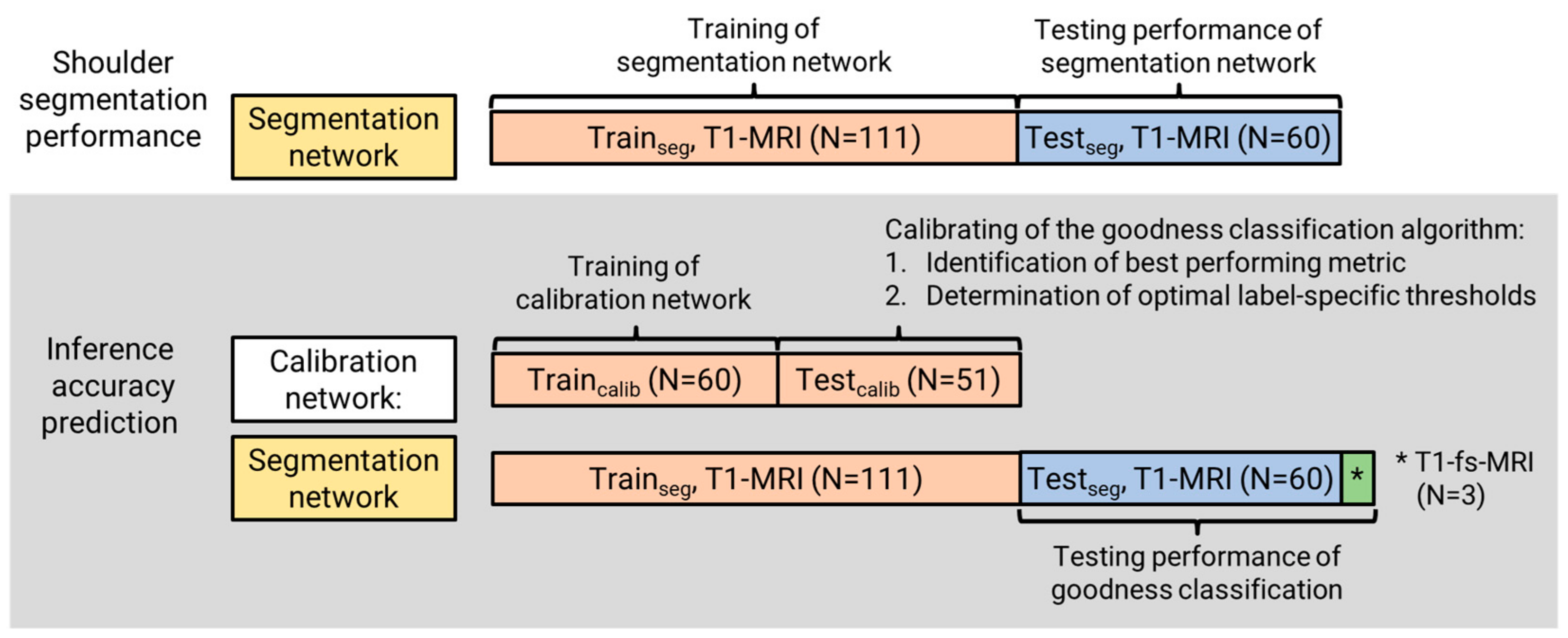
2.1.1. Data
2.1.2. Segmentation Network Training
2.1.3. Segmentation Network Verification
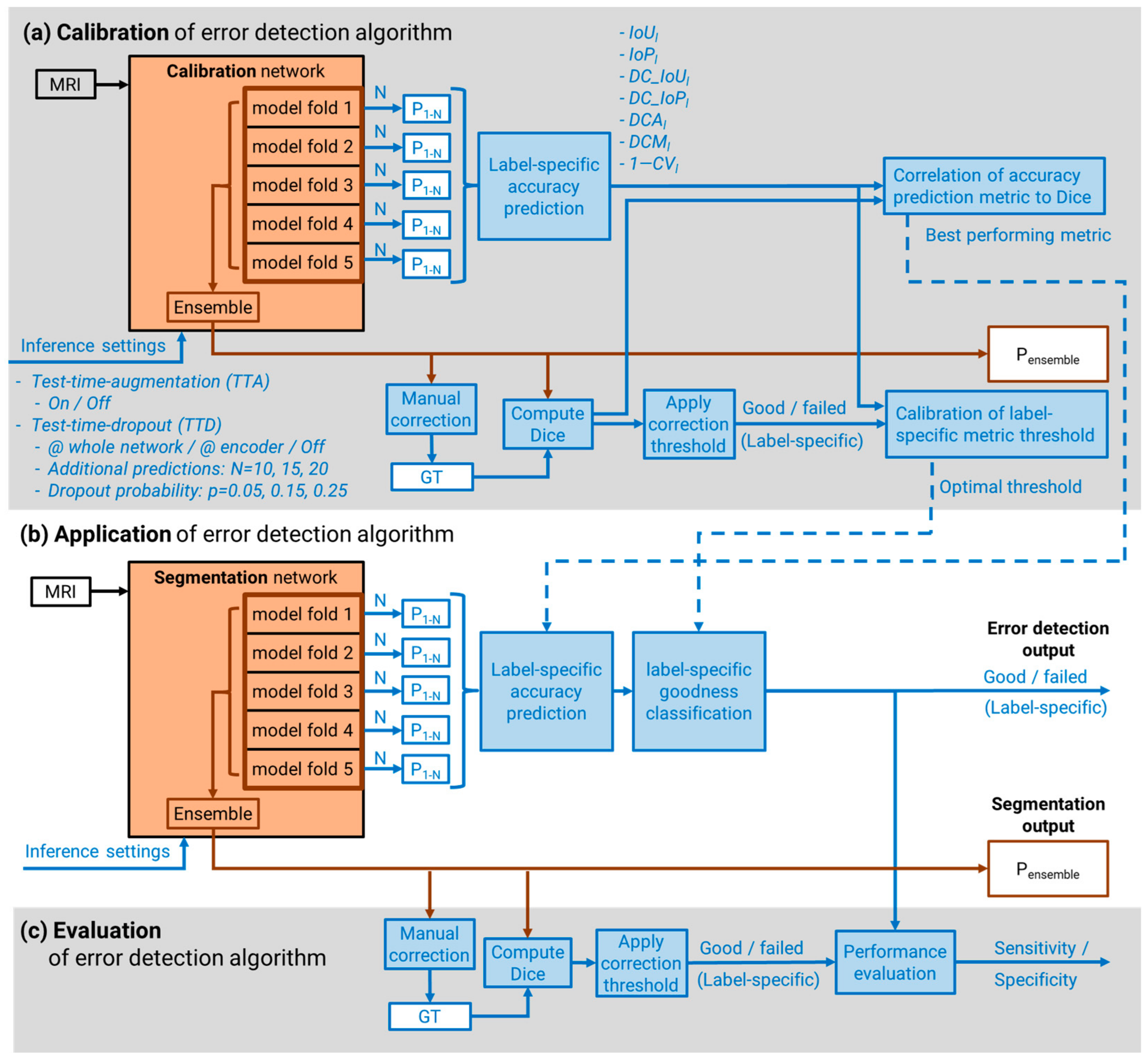
2.2. Inference Accuracy Prediction
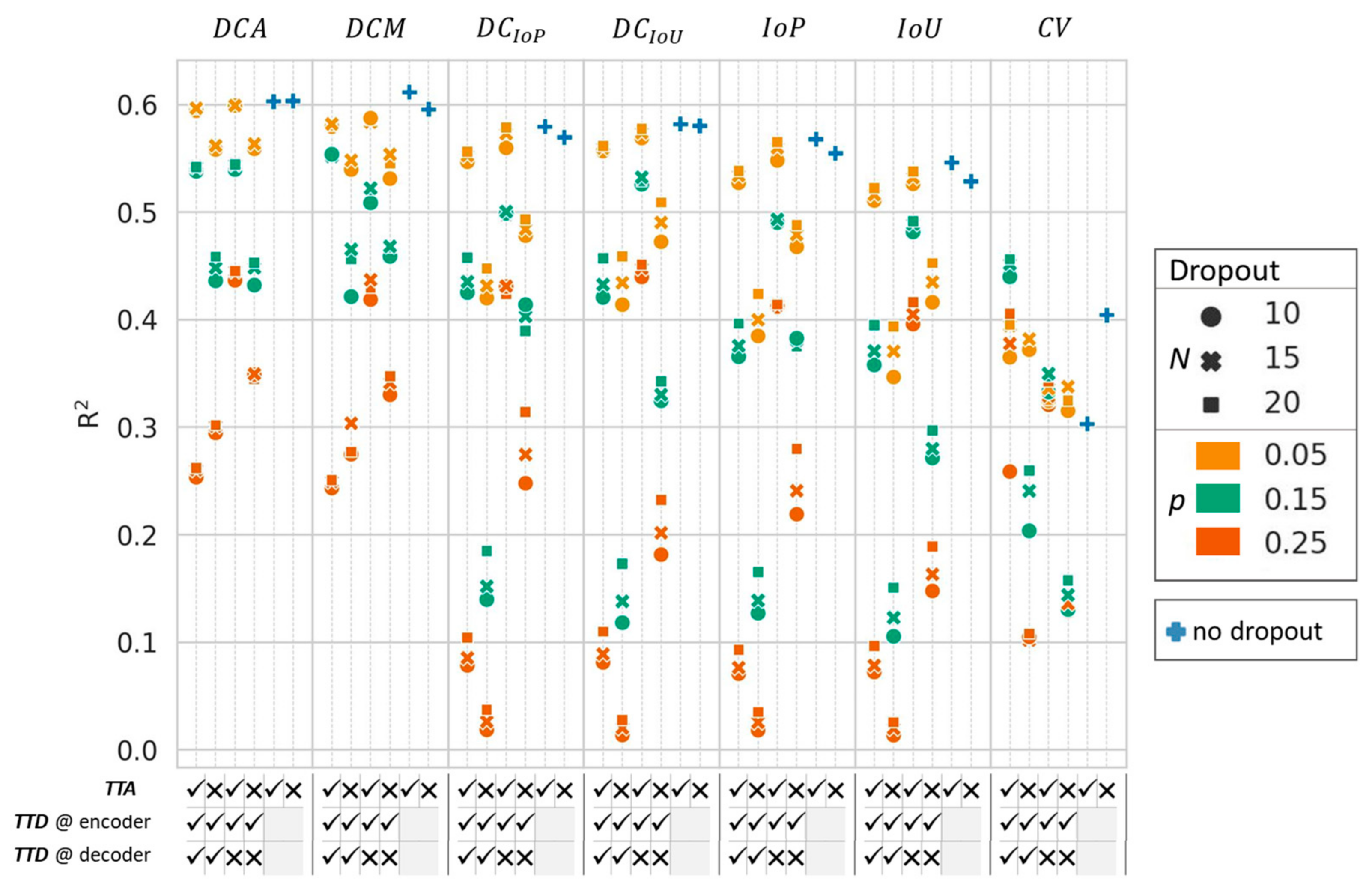
2.2.1. Auxiliary Predictions for Uncertainty Calculation
2.2.2. Accuracy Prediction Metrics
2.2.3. Inference Accuracy Prediction Performance
2.2.4. Segmentation Goodness Classification
2.2.5. Performance Testing of Goodness Classification
3. Results
3.1. Anatomy Segmentation
3.2. Inference Accuracy Prediction
3.3. Performance Testing of Goodness Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Minagawa, H.; Yamamoto, N.; Abe, H.; Fukuda, M.; Seki, N.; Kikuchi, K.; Kijima, H.; Itoi, E. Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. J. Orthop. 2013, 10, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.L.; Harryman, D.T.; Antoniou, J.; Campbell, B.; Sidles, J.A.; Matsen, F.A. A prospective, multipractice study of shoulder function and health status in patients with documented rotator cuff tears. J. Shoulder Elb. Surg. 2000, 9, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Zumstein, M.A.; Jost, B.; Hempel, J.; Hodler, J.; Gerber, C. The Clinical and Structural Long-Term Results of Open Repair of Massive Tears of the Rotator Cuff. J. Bone Jt. Surg. Am. Vol. 2008, 90, 2423–2431. [Google Scholar] [CrossRef] [PubMed]
- Lädermann, A.; Collin, P.; Athwal, G.S.; Scheibel, M.; Zumstein, M.A.; Nourissat, G. Current concepts in the primary management of irreparable posterosuperior rotator cuff tears without arthritis. EFORT Open Rev. 2018, 3, 200–209. [Google Scholar] [CrossRef]
- Longo, U.G.; Carnevale, A.; Piergentili, I.; Berton, A.; Candela, V.; Schena, E.; Denaro, V. Retear rates after rotator cuff surgery: A systematic review and meta-analysis. BMC Musculoskelet Disord 2021, 22, 749. [Google Scholar] [CrossRef]
- Goutallier, D.; Postel, J.M.; Bernageau, J.; Lavau, L.; Voisin, M.C. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Li, H.; Chen, Y.; Chen, J.; Hua, Y.; Chen, S. Large Critical Shoulder Angle Has Higher Risk of Tendon Retear After Arthroscopic Rotator Cuff Repair. Am. J. Sports Med. 2018, 46, 1892–1900. [Google Scholar] [CrossRef]
- Moor, B.K.; Bouaicha, S.; Rothenfluh, D.A.; Sukthankar, A.; Gerber, C. Is there an association between the individual anatomy of the scapula and the development of rotator cuff tears or osteoarthritis of the glenohumeral joint? Bone Jt. J. 2013, 95-B, 935–941. [Google Scholar] [CrossRef]
- Nyffeler, R.W.; Werner, C.M.L.; Sukthankar, A.; Schmid, M.R.; Gerber, C. Association of a Large Lateral Extension of the Acromion with Rotator Cuff Tears. J. Bone Jt. Surg. 2006, 88, 800–805. [Google Scholar]
- Fuchs, B.; Weishaupt, D.; Zanetti, M.; Hodler, J.; Gerber, C. Fatty degeneration of the muscles of the rotator cuff: Assessment by computed tomography versus magnetic resonance imaging. J. Shoulder Elb. Surg. 1999, 8, 599–605. [Google Scholar] [CrossRef]
- Suter, T.; Gerber Popp, A.; Zhang, Y.; Zhang, C.; Tashjian, R.Z.; Henninger, H.B. The influence of radiographic viewing perspective and demographics on the critical shoulder angle. J. Shoulder Elb. Surg. 2015, 24, e149–e158. [Google Scholar] [CrossRef]
- Henninger, H.B.; Suter, T.; Chalmers, P.N. Editorial Commentary: Is Your Critical Shoulder Angle Accurate? Only If You Can Verify That You Have the Correct Images. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 447–449. [Google Scholar] [CrossRef]
- Suter, T.; Henninger, H.B.; Zhang, Y.; Wylie, J.D.; Tashjian, R.Z. Comparison of measurements of the glenopolar angle in 3D CT reconstructions of the scapula and 2D plain radiographic views. Bone Jt. J. 2016, 98-B, 1510–1516. [Google Scholar] [CrossRef]
- Mah, D.; Chamoli, U.; Smith, G.C.S. Usefulness of computed tomography based three-dimensional reconstructions to assess the critical shoulder angle. World J. Orthop. 2021, 12, 301–309. [Google Scholar] [CrossRef]
- Anwander, H.; Fuhrer, F.; Diserens, G.; Moor, B.K.; Boesch, C.; Vermathen, P.; Valenzuela, W.; Zumstein, M.A. Muscle fat content in the intact infraspinatus muscle correlates with age and BMI, but not critical shoulder angle. Eur. J. Trauma Emerg. Surg. 2021, 47, 607–616. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. 2015. Available online: https://arxiv.org/pdf/1505.04597 (accessed on 1 May 2023).
- Medina, G.; Buckless, C.G.; Thomasson, E.; Oh, L.S.; Torriani, M. Deep learning method for segmentation of rotator cuff muscles on MR images. Skelet. Radiol. 2021, 50, 683–692. [Google Scholar] [CrossRef]
- Ro, K.; Kim, J.Y.; Park, H.; Cho, B.H.; Kim, I.Y.; Shim, S.B.; Choi, I.Y.; Yoo, J.C. Deep-learning framework and computer assisted fatty infiltration analysis for the supraspinatus muscle in MRI. Sci. Rep. 2021, 11, 15065. [Google Scholar] [CrossRef]
- Godoy, I.R.B.; Silva, R.P.; Rodrigues, T.C.; Skaf, A.Y.; Pochini, A.D.C.; Yamada, A.F. Automatic MRI segmentation of pectoralis major muscle using deep learning. Sci. Rep. 2022, 12, 5300. [Google Scholar] [CrossRef]
- Riem, L.; Feng, X.; Cousins, M.; DuCharme, O.; Leitch, E.B.; Werner, B.C.; Sheean, A.J.; Hart, J.; Antosh, I.J.; Blemker, S.S. A Deep Learning Algorithm for Automatic 3D Segmentation of Rotator Cuff Muscle and Fat from Clinical MRI Scans. Radiol. Artif. Intell. 2023, 5, e220132. [Google Scholar] [CrossRef]
- de Jesus, J.O.; Parker, L.; Frangos, A.J.; Nazarian, L.N. Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: A meta-analysis. Am. J. Roentgenol. 2009, 192, 1701–1707. [Google Scholar] [CrossRef]
- Roy, A.G.; Conjeti, S.; Navab, N.; Wachinger, C. Bayesian QuickNAT: Model uncertainty in deep whole-brain segmentation for structure-wise quality control. NeuroImage 2019, 195, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Lakshminarayanan, B.; Pritzel, A.; Blundell, C. Simple and Scalable Predictive Uncertainty Estimation using Deep Ensembles. arXiv 2016, arXiv:1612.01474. [Google Scholar]
- Jungo, A.; Balsiger, F.; Reyes, M. Analyzing the Quality and Challenges of Uncertainty Estimations for Brain Tumor Segmentation. Front. Neurosci. 2020, 14, 282. [Google Scholar] [CrossRef] [PubMed]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef]
- Gal, Y.; Ghahramani, Z. Dropout as a Bayesian Approximation: Representing Model Uncertainty in Deep Learning. In Proceedings of the 33rd International Conference on Machine Learning, New York, NY, USA, 19–24 June 2015. [Google Scholar]
- Schisterman, E.F.; Faraggi, D.; Reiser, B.; Hu, J. Youden Index and the optimal threshold for markers with mass at zero. Statist. Med. 2008, 27, 297–315. [Google Scholar] [CrossRef]
- Audigé, L.; Bucher, H.C.C.; Aghlmandi, S.; Stojanov, T.; Schwappach, D.; Hunziker, S.; Candrian, C.; Cunningham, G.; Durchholz, H.; Eid, K.; et al. Swiss-wide multicentre evaluation and prediction of core outcomes in arthroscopic rotator cuff repair: Protocol for the ARCR_Pred cohort study. BMJ Open 2021, 11, e045702. [Google Scholar] [CrossRef]
- Zeng, G.; Schmaranzer, F.; Degonda, C.; Gerber, N.; Gerber, K.; Tannast, M.; Burger, J.; Siebenrock, K.A.; Zheng, G.; Lerch, T.D. MRI-based 3D models of the hip joint enables radiation-free computer-assisted planning of periacetabular osteotomy for treatment of hip dysplasia using deep learning for automatic segmentation. Eur. J. Radiol. Open 2021, 8, 100303. [Google Scholar] [CrossRef]
- Sander, J.; de Vos, B.D.; Išgum, I. Automatic segmentation with detection of local segmentation failures in cardiac MRI. Sci. Rep. 2020, 10, 21769. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Training Dataset | Test Dataset |
|---|---|---|
| Image datasets, no. | 111 T1-MRI | 60 T1-MRI |
| Shoulders (Patients), no. | 37 (37) | 39 (38) |
| Age (years; mean ± std) | 57 ± 13 | 57 ± 10 |
| Female sex, no. (%) | 16 (43) | 13 (33) |
| Left side, no. (%) | 15 (41) | 14 (36) |
| Anatomical orientation, no. | 37 coronal 37 sagittal 37 transversal | 20 coronal 20 sagittal 20 transversal |
| Institutions, no. | 7 | 9 |
| Vendor no. (%) | 35 (95) Siemens 2 (5) Philipps | 32 (82) Siemens 7 (18) Philipps |
| Magnetic field strength no. (%) | 21 (57) 1.5 Tesla 16 (43) 3.0 Tesla | 14 (36) 1.5 Tesla 25 (64) 3.0 Tesla |
| In-plane resolution (mm) | 0.2–0.5 | 0.2–0.5 |
| Slice thickness (mm) | 2.5–4.0 | 2.5–4.0 |
| Spacing between slices (mm) | 3.3–4.6 | 2.75–4.8 |
| Network | Humerus | Scapula | SSP | SSC | ISP | TM | Overall |
|---|---|---|---|---|---|---|---|
| 2D | 0.96 ± 0.03 | 0.91 ± 0.05 | 0.90 ± 0.06 | 0.90 ± 0.09 | 0.89 ± 0.06 | 0.83 ± 0.09 | 0.90 ± 0.08 |
| 3D | 0.97 ± 0.02 | 0.92 ± 0.05 | 0.92 ± 0.06 | 0.91 ± 0.07 | 0.91 ± 0.05 | 0.86 ± 0.07 | 0.91 ± 0.06 |
| Ensemble | 0.96 ± 0.02 | 0.92 ± 0.05 | 0.91 ± 0.05 | 0.91 ± 0.08 | 0.91 ± 0.05 | 0.85 ± 0.08 | 0.91 ± 0.07 |
| Label | DCM TTA | DCA no TTA | DCA TTA | DCA TTA N = 10, p = 0.05 | DCA TTA N = 15, p = 0.05 |
|---|---|---|---|---|---|
| Humerus | 0.98 | 1.00 | 1.00 | 1.00 | 1.00 |
| Scapula | 0.41 | 0.76 | 0.57 | 0.54 | 0.54 |
| Supraspinatus | 0.91 | 0.93 | 0.98 | 0.98 | 0.98 |
| Subscapularis | 0.92 | 0.94 | 0.94 | 0.96 | 0.98 |
| Infraspinatus | 0.84 | 0.84 | 0.84 | 0.84 | 0.82 |
| Teres minor | 0.59 | 0.50 | 0.53 | 0.50 | 0.53 |
| Average | 0.77 | 0.83 | 0.81 | 0.80 | 0.81 |
| Label | Sensitivity | Specificity | TP | TN | FP | FN | Threshold |
|---|---|---|---|---|---|---|---|
| Humerus | 1.00 | 1.00 | 3 | 60 | 0 | 0 | 0.97 |
| Scapula | 1.00 | 0.98 | 3 | 59 | 1 | 0 | 0.94 |
| Supraspinatus | 1.00 | 0.97 | 2 | 59 | 2 | 0 | 0.92 |
| Subscapularis | 1.00 | 0.97 | 3 | 58 | 2 | 0 | 0.91 |
| Infraspinatus | 1.00 | 0.98 | 4 | 58 | 1 | 0 | 0.93 |
| Teres Minor | 1.00 | 0.72 | 3 | 43 | 17 | 0 | 0.94 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hess, H.; Ruckli, A.C.; Bürki, F.; Gerber, N.; Menzemer, J.; Burger, J.; Schär, M.; Zumstein, M.A.; Gerber, K. Deep-Learning-Based Segmentation of the Shoulder from MRI with Inference Accuracy Prediction. Diagnostics 2023, 13, 1668. https://doi.org/10.3390/diagnostics13101668
Hess H, Ruckli AC, Bürki F, Gerber N, Menzemer J, Burger J, Schär M, Zumstein MA, Gerber K. Deep-Learning-Based Segmentation of the Shoulder from MRI with Inference Accuracy Prediction. Diagnostics. 2023; 13(10):1668. https://doi.org/10.3390/diagnostics13101668
Chicago/Turabian StyleHess, Hanspeter, Adrian C. Ruckli, Finn Bürki, Nicolas Gerber, Jennifer Menzemer, Jürgen Burger, Michael Schär, Matthias A. Zumstein, and Kate Gerber. 2023. "Deep-Learning-Based Segmentation of the Shoulder from MRI with Inference Accuracy Prediction" Diagnostics 13, no. 10: 1668. https://doi.org/10.3390/diagnostics13101668