
Subtypes of the Completely Reversed Flow Waveform in Vertebral Artery Can Help to Differentiate Subclavian Artery Occlusion from Severe Stenosis

Abstract
:1. Introduction
2. Methods
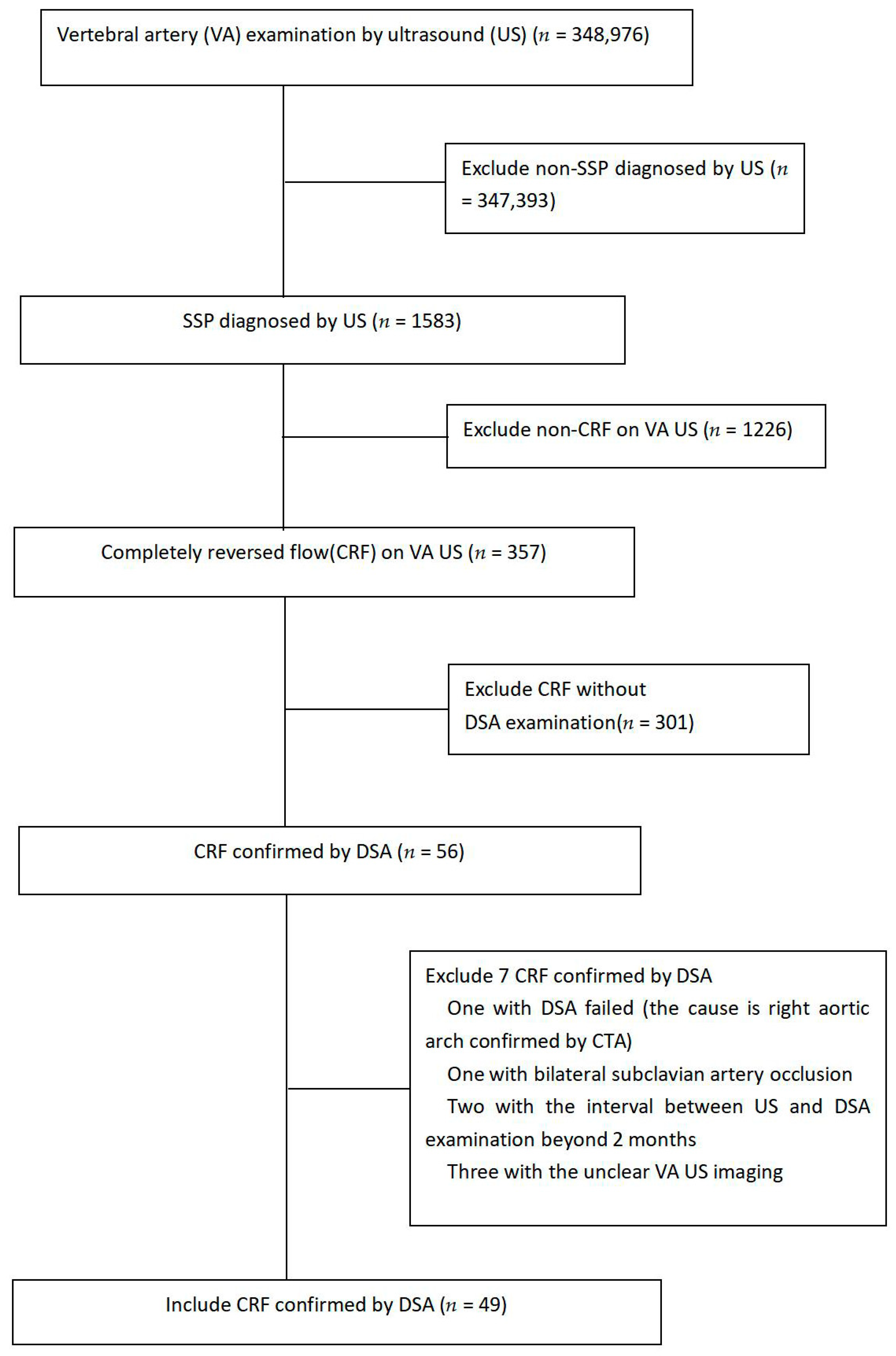
2.1. Patients
2.2. Doppler Sonography
2.3. Angiography
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients with CRF and SA Stenosis
3.2. Correlation of CRF Waveform and VA Parameters with Ipsilateral SA Occlusion or Severe Stenosis
3.3. Diagnostic Values of VA US Parameters in 27 Patients with VA CCRF
3.4. Diagnostic Values of VA US Parameters in 22 Patients with VA ICRF
3.5. Diagnostic Value of CCRF Combined with the Diameter of the Target VA with ICRF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savitz, S.I.; Caplan, L.R. Vertebrobasilar disease. N. Engl. J. Med. 2005, 352, 2618–2626. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Suri, M.F.; Ziai, W.C.; Yahia, A.M.; Mohammad, Y.; Sen, S.; Agarwal, P.; Zaidat, O.O.; Suarez, J.I.; Wityk, R.J. Stroke-free survival and its determinants in patients with symptomatic vertebrobasilar stenosis: A multicenter study. Neurosurgery 2003, 52, 1033–1040. [Google Scholar]
- Jahic, E.; Avdagic, H.; Iveljic, I.; Krdzalic, A. Percutaneous Transluminal Angioplasty of Subclavian Artery Lesions. Med. Arch. 2019, 73, 28–31. [Google Scholar] [CrossRef]
- Kablak-Ziembicka, A.; Przewlocki, T.; Pieniazek, P.; Musialek, P.; Kozanecki, A.; Stopa, I.; Zalewski, J.; Tracz, W. Doppler Ultrasonography in Suspected Subclavian Artery Obstruction and in Patient Monitoring after Subclavian Stenting. Cardiovasc. Interv. Radiol. 2007, 30, 894–900. [Google Scholar] [CrossRef]
- Sixt, S.; Rastan, A.; Schwarzwälder, U.; Bürgelin, K.; Noory, E.; Schwarz, T.; Beschorner, U.; Frank, U.; Müller, C.; Hauk, M.; et al. Results after balloon angioplasty or stenting of atherosclerotic subclavian artery obstruction. Catheter. Cardiovasc. Interv. 2009, 73, 395–403. [Google Scholar] [CrossRef]
- Schillinger, M.; Haumer, M.; Schillinger, S.; Ahmadi, R.; Minar, E. Risk stratification for subclavian artery angioplasty: Is there an increased rate of restenosis after stent implantation? J. Endovasc Ther. 2001, 8, 550–557. [Google Scholar] [CrossRef]
- Mrad, I.B.; Miri, R.; Mazzaccaro, D.; Mrad, M.B.; Mleyhi, S.; Zairi, I.; Hammami, R.; Nano, G.; Kraiem, S.; Denguir, R. Endovascular therapy for steno-occlusive subclavian artery disease early and long-term outcomes in a multicentric Tunisian study. Ann. Ital. Chir. 2022, 93, 470–475. [Google Scholar]
- Zhang, J.; Wang, L.; Chen, Y.; Wang, S.; Xing, Y.; Cui, L. Color Doppler Ultrasonography for the Evaluation of Subclavian Artery Stenosis. Front. Neurol. 2022, 13, 804039. [Google Scholar] [CrossRef]
- Gunabushanam, G.; Kummant, L.; Scoutt, L.M. Vertebral Artery Ultrasound. Radiologic Clinics of North America. Elsevier Health Sci. 2019, 57, 519–533. [Google Scholar]
- Nicolau, C.; Gilabert, R.; Chamorro, A.; Vázquez, F.; Bargalló, N.; Brú, C. Doppler sonography of the intertransverse segment of the vertebral artery. J. Ultrasound Med. 2000, 19, 47–53. [Google Scholar] [CrossRef]
- Buckenham, T.M. Wright IA:Ultrasound of the extracranial vertebral artery. Br. J. Radiol. 2004, 77, 15–20. [Google Scholar] [CrossRef]
- Psychogios, K.; Magoufis, G.; Kargiotis, O.; Safouris, A.; Bakola, E.; Chondrogianni, M.; Zis, P.; Stamboulis, E.; Tsivgoulis, G. Ultrasound Assessment of Extracranial Carotids and Vertebral Arteries in Acute Cerebral Ischemia. Medicina 2020, 56, 711. [Google Scholar] [CrossRef]
- Cheng, P.; Liu, B.; Yu, D.; Xu, J. The value of color Doppler sonography in diagnosis and hemodynamic analysis of innominate artery occlusion. J. Clin. Ultrasound. 2022, 50, 351–353. [Google Scholar] [CrossRef]
- Sakima, H.; Wakugawa, Y.; Isa, K.; Yasaka, M.; Ogata, T.; Saitoh, M.; Shimada, H.; Yasumori, K.; Inoue, T.; Ohya, Y.; et al. Correlation between the Degree of Left Subclavian Artery Stenosis and the Left Vertebral Artery Waveform by Pulse Doppler Ultrasonography. Cerebrovasc. Dis. 2011, 31, 64–67. [Google Scholar] [CrossRef]
- Chen, S.P.; Hu, Y.P. Waveform Patterns and Peak Reversed Velocity in Vertebral Arteries Predict Severe Subclavian Artery Stenosis and Occlusion. J. Ultrasound Med. Biol. 2015, 41, 1328–1333. [Google Scholar] [CrossRef]
- Kliewer, M.A.; Hertzberg, B.S.; Kim, D.H.; Bowie, J.D.; Courneya, D.L.; Carroll, B.A. Vertebral Artery Doppler Waveform Changes Indicating Subclavian Steal Physiology. Am. J. Roentgenol. 2000, 174, 815–819. [Google Scholar] [CrossRef] [Green Version]
- Labropoulos, N.; Nandivada, P.; Bekelis, K. Prevalence and Impact of the Subclavian Steal Syndrome. Ann. Surg. 2010, 252, 166–170. [Google Scholar] [CrossRef]
- Päivänsalo, M.; kkilä, O.; Tikkakoski, T.; Leinonen, S.; Merikantoet, J.; Suramo, I. Duplex ultrasound in the subclavian steal syndrome. Acta Radiol. 1998, 39, 183–188. [Google Scholar] [CrossRef]
- Hua, Y.; Jia, L.; Li, L.; Ling, C.; Miao, Z.; Jiao, L. Evaluation of Severe Subclavian Artery Stenosis by Color Doppler Flow Imaging. Ultrasound Med. Biol. 2011, 37, 358–363. [Google Scholar] [CrossRef]
- Mousa, A.Y.; Morkous, R.; Broce, M.; Yacoub, M.; Sticco, A.; Viradia, R.; Bates, M.C.; AbuRahma, A.F. Validation of subclavian duplex velocity criteria to grade severity of subclavianartery stenosis. J. Vasc Surg. 2017, 65, 1779–1785. [Google Scholar] [CrossRef] [Green Version]
- Shao, Q.Q.; Zhao, T.; Ren, J.H.; Wang, B.; Sun, H.J. Color doppler flow imaging evaluates the influence on subclavian artery steal caused by vertebral artery hypoplasia. J. Biol. Regul. Homeost. Agents. 2021, 35, 331–336. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Datum |
|---|---|
| Clinical characteristics | |
| Age (y) | 54–86 (68.2 ± 7.8) |
| Gender (male/female) | 39/10 |
| Hypertension | 27 (55%) |
| Hyperlipidemia | 7 (14.3%) |
| Diabetes | 15 (30.6(%) |
| Smoking habit | 11 (22.4%) |
| Obesity | 15 (30.6%) |
| Concomitant diseases | |
| Coronary artery diseases | 3 (6.1%) |
| Previous myocardial infarction | 1 (2%) |
| Previous stroke/TIA | 7 (14.3%) |
| Clinical symptoms and physical examination | |
| Asymptomatic patients | 10 (20.4%) |
| Symptomatic patients | 39 (79.6%) |
| Symptoms of posterior fossa ischemia | 22 (44.9%) |
| Upper limb claudication | 9 (18.4%) |
| Pulse weakness | 33 (67.3%) |
| Mean SBP difference (mmHg) * | 33 (16–46) |
| Mean DBP difference (mmHg) * | 9 (5.5–18) |
| Events | CCRF Group (n = 27) | ICRF Group (n = 22) | p-Value |
|---|---|---|---|
| Carotid artery occlusion | 3 | 3 | 0.805 |
| Vertebral artery occlusion | 2 | 3 | 0.497 |
| Carotid and vertebral artery occlusion | 1 | 1 | 0.885 |
| Parameters | Occlusion (n = 33) | Severe Stenosis (n = 16) | p-Value |
|---|---|---|---|
| Age (years) | 67.7 ± 7.8 | 69.2 ± 8.0 | 0.585 |
| Gender (male/female) | 25/8 | 14/2 | 0.464 |
| Site (left/right) | 28/5 | 16/0 | 0.158 |
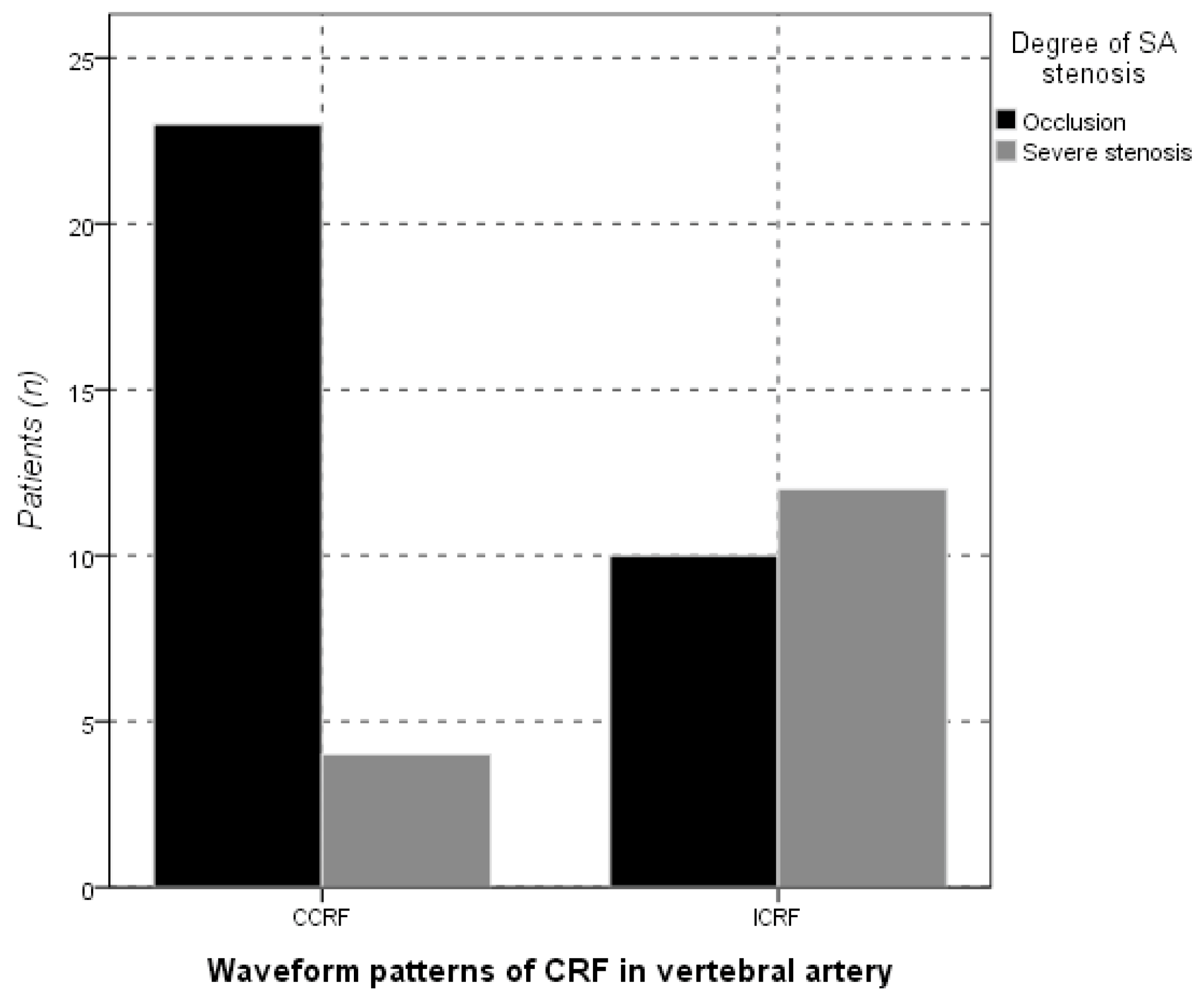
| Waveform type | 0.005 | ||
| CCRF | 23 | 4 | |
| ICRF | 10 | 12 | |
| Diameter (mm) | |||
| TVA | 3.4 ± 0.7 | 3. 3 ± 0.7 | 0.807 |
| CVA | 3.8 ± 0.8 | 3.7 ± 0.6 | 0.411 |
| PSV (cm/s) | |||
| TVA (PRV) | 63 (41–84) | 50 (40–77.25) | 0.337 |
| CVA | 76 (60.5–101) | 79.5 (61–91.25) | 0.725 |
| Resistant index (RI) | |||
| TVA | 0.88 ± 0.11 | 0.96 ± 0.07 | 0.051 |
| CVA | 0.73 ± 0.10 | 0.74 ± 0.12 | 0.492 |
| Parameters | Occlusion Group (n = 23) | Severe Stenosis Group (n = 4) | p-Value |
|---|---|---|---|
| Age (years) | 67.0 ± 7.2 | 71.3 ± 6.7 | 0.284 |
| Gender (male/female) | 18/5 | 3/1 | 1.000 |
| Site (left/right) | 18/5 | 4/0 | 0.561 |
| Diameter (mm) | |||
| TVA | 3.2 ± 0.7 | 3. 8 ± 0.5 | 0.096 |
| CVA | 3.8 ± 0.8 | 3.9 ± 0.6 | 0.825 |
| PSV (cm/s) | |||
| TVA (PRV) | 60 (40–84) | 76 (47.25–84) | 0.473 |
| CVA | 76 (59–99) | 84 (68.75–97.25) | 0.682 |
| Resistant index (RI) | |||
| TVA | 0.83 ± 0.09 | 0.84 ± 0.04 | 0.800 |
| CVA | 0.71 ± 0.09 | 0.75 ± 0.09 | 0.441 |
| Parameters | Occlusion (n = 10) | Severe Stenosis (n = 12) | p-Value |
|---|---|---|---|
| Age (years) | 69.3 ± 9.1 | 68.5 ± 8.5 | 0.833 |
| Gender (male/female) | 7/3 | 10/2 | 0.624 |
| Diameter (mm) | |||
| TVA | 3.8 ± 0.7 | 3. 2 ± 0.7 | 0.041 |
| CVA | 3.7 ± 0.9 | 3.6 ± 0.6 | 0.849 |
| PSV (cm/s) | |||
| TVA (PRV) | 66 (47.25–98.25) | 46 (40–65.5) | 0.099 |
| CVA | 75.5 (67.75–114) | 78 (58.75–90.5) | 0.664 |
| Resistant index (RI) | |||
| CVA | 0.79 ± 0.12 | 0.74 ± 0.13 | 0.363 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.-P.; Zhong, Z.; Tu, D.-P. Subtypes of the Completely Reversed Flow Waveform in Vertebral Artery Can Help to Differentiate Subclavian Artery Occlusion from Severe Stenosis. Diagnostics 2023, 13, 146. https://doi.org/10.3390/diagnostics13010146
Chen S-P, Zhong Z, Tu D-P. Subtypes of the Completely Reversed Flow Waveform in Vertebral Artery Can Help to Differentiate Subclavian Artery Occlusion from Severe Stenosis. Diagnostics. 2023; 13(1):146. https://doi.org/10.3390/diagnostics13010146
Chicago/Turabian StyleChen, Shun-Ping, Zhen Zhong, and Dong-Pei Tu. 2023. "Subtypes of the Completely Reversed Flow Waveform in Vertebral Artery Can Help to Differentiate Subclavian Artery Occlusion from Severe Stenosis" Diagnostics 13, no. 1: 146. https://doi.org/10.3390/diagnostics13010146