
Clinical Applications of Quantitative Perfusion Imaging with a C-Arm Flat-Panel Detector—A Systematic Review
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
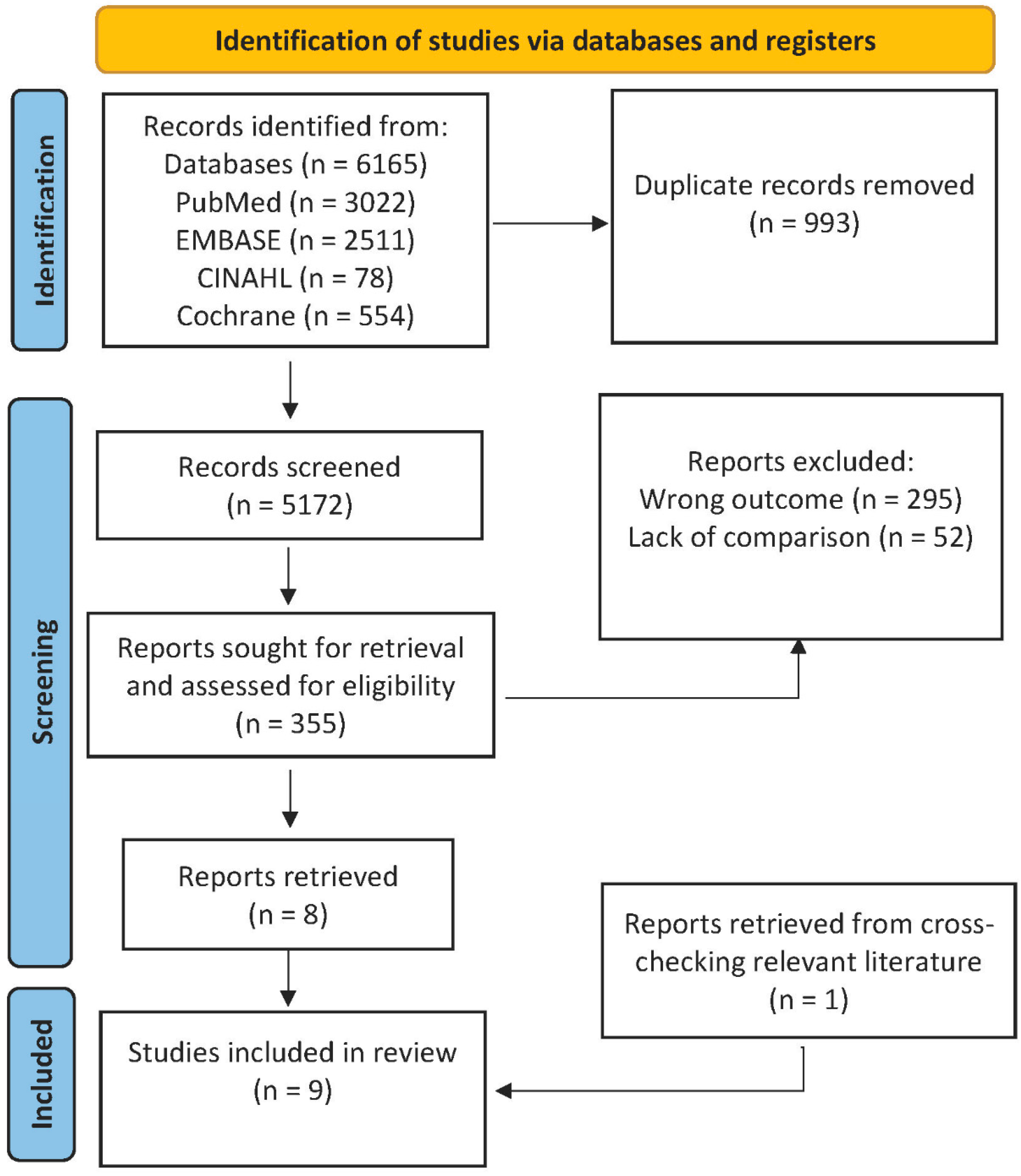
2.1. Literature Search
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
3. Results
3.1. 2D Perfusion Angiography
3.1.1. Description of the Technique
3.1.2. Clinical Applications
3.2. Dual-Phase CBCT Perfusion
3.2.1. Description of the Technique
3.2.2. Clinical Applications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Orth, R.C.; Wallace, M.J.; Kuo, M.D. C-arm Cone-beam CT: General principles and technical considerations for use in interventional radiology. J. Vasc. Interv. Radiol. 2008, 19, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Gyánó, M.; Góg, I.; Óriás, V.I.; Ruzsa, Z.; Nemes, B.; Csobay-Novák, C.; Oláh, Z.; Nagy, Z.; Merkely, B.; Szigeti, K.; et al. Kinetic imaging in lower extremity arteriography: Comparison to digital subtraction angiography. Radiology 2019, 290, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Hochmuth, A.; Spetzger, U.; Schumacher, M. Comparison of three-dimensional rotational angiography with digital subtraction angiography in the assessment of ruptured cerebral aneurysms. Am. J. Neuroradiol. 2002, 23, 1199–1205. [Google Scholar]
- Missler, U.; Hundt, C.; Wiesmann, M.; Mayer, T.; Brückmann, H. Three-dimensional reconstructed rotational digital subtraction angiography in planning treatment of intracranial aneurysms. Eur. Radiol. 2000, 10, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Song, J.K.; Niimi, Y.; Brisman, J.L.; Berenstein, A. Simultaneous bilateral internal carotid artery 3d rotational angiography. Am. J. Neuroradiol. 2004, 25, 1787–1789. [Google Scholar] [PubMed]
- Feldkamp, L.A.; Davis, L.C.; Kress, J.W. Practical cone-beam algorithm. J. Opt. Soc. Am. A 1984, 1, 612. [Google Scholar] [CrossRef] [Green Version]
- Ning, R.; Chen, B.; Yu, R.; Conover, D.; Tang, X.; Ning, Y. Flat panel detector-based cone-beam volume CT angi-ography imaging: System evaluation. IEEE Trans. Med. Imaging 2000, 19, 949–963. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Hatsukami, T.S.; Mossa-Basha, M. Vessel Based Imaging Techniques: Diagnosis, Treatment, and Prevention; Springer Nature: Cham, Switzerland, 2019. [Google Scholar]
- Harrigan, M.; Deveikis, J. Handbook of cerebrovascular disease and neurointerventional technique. Am. J. Neuroradiol. 2009, 30, E135. [Google Scholar] [CrossRef]
- Sun, Z. Digital variance angiography: A promising alternative technology to traditional angiography for improvement of image quality with reduction of radiation and contrast medium doses. Cardiovasc. Interv. Radiol. 2021, 44, 460–461. [Google Scholar] [CrossRef]
- Strother, C.; Bender, F.; Deuerling-Zheng, Y.; Royalty, K.; Pulfer, K.; Baumgart, J.; Zellerhoff, M.; Aagaard-Kienitz, B.; Niemann, D.; Lindstrom, M. Parametric color coding of digital subtraction angiography. Am. J. Neuroradiol. 2010, 31, 919–924. [Google Scholar] [CrossRef] [Green Version]
- Struffert, T.; Deuerling-Zheng, Y.; Engelhorn, T.; Kloska, S.; Gölitz, P.; Bozzato, A.; Kapsreiter, M.; Strother, C.M.; Doerfler, A. Monitoring of balloon test occlusion of the internal carotid artery by parametric color coding and perfusion imaging within the Angio suite: First results. Clin. Neuroradiol. 2013, 23, 285–292. [Google Scholar] [CrossRef]
- Gölitz, P.; Struffert, T.; Lücking, H.; Rösch, J.; Knossalla, F.; Ganslandt, O.; Deuerling-Zheng, Y.; Doerfler, A. Parametric color coding of digital subtraction angiography in the evaluation of carotid cavernous fistulas. Clin. Neuroradiol. 2013, 23, 113–120. [Google Scholar] [CrossRef]
- Lin, C.-J.; Luo, C.-B.; Hung, S.-C.; Guo, W.-Y.; Chang, F.-C.; Beilner, J.; Kowarschik, M.; Chu, W.-F.; Chang, C.-Y. Application of color-coded digital subtraction angiography in treatment of indirect carotid-cavernous fistulas: Initial experience. J. Chin. Med. Assoc. 2013, 76, 218–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, S.-C.; Liang, M.-L.; Lin, C.-F.; Lin, C.-J.; Guo, W.-Y.; Chang, F.-C.; Wong, T.-T.; Chang, C.-Y. New grading of moyamoya disease using color-coded parametric quantitative digital subtraction angiography. J. Chin. Med. Assoc. 2014, 77, 437–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.; Hung, S.; Guo, W.; Chang, F.; Luo, C.; Beilner, J.; Kowarschik, M.; Chu, W.; Chang, C. Monitoring peri-therapeutic cerebral circulation time: A feasibility study using color-coded quantitative DSA in patients with steno-occlusive arterial disease. Am. J. Neuroradiol. 2012, 33, 1685–1690. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.J.; Chang, F.C.; Tsai, F.Y.; Guo, W.Y.; Hung, S.C.; Chen, D.Y.T.; Chang, C.Y. Stenotic transverse sinus predisposes to poststenting hyperperfusion syndrome as evidenced by quantitative analysis of peritherapeutic cerebral circulation time. Am. J. Neuroradiol. 2014, 35, 1132–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jens, S.; Marquering, H.A.; Koelemay, M.J.W.; Reekers, J.A. Perfusion angiography of the foot in patients with critical limb ischemia: Description of the technique. Cardiovasc. Interv. Radiol. 2015, 38, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Reekers, J.A.; Koelemay, M.J.W.; Marquering, H.A.; van Bavel, E.T. Functional imaging of the foot with perfusion angiography in critical limb ischemia. Cardiovasc. Interv. Radiol. 2016, 39, 183–189. [Google Scholar] [CrossRef] [Green Version]
- Murray, T.; Rodt, T.; Lee, M.J. Two-dimensional perfusion angiography of the foot. J. Endovasc. Ther. 2016, 23, 58–64. [Google Scholar] [CrossRef]
- Ganguly, A.; Fieselmann, A.; Marks, M.; Rosenberg, J.; Boese, J.; Deuerling-Zheng, Y.; Straka, M.; Zaharchuk, G.; Bammer, R.; Fahrig, R. Cerebral CT perfusion using an interventional C-Arm imaging system: Cerebral blood flow measurements. Am. J. Neuroradiol. 2011, 32, 1525–1531. [Google Scholar] [CrossRef] [Green Version]
- Zellerhoff, M.; Deuerling-Zheng, Y.; Strother, C.M.; Ahmed, A.; Pulfer, K.; Redel, T.; Royalty, K.; Grinde, J.; Consigny, D. Measurement of cerebral blood volume using angiographic C-arm systems. In Proceedings of the Medical Imaging 2009: Biomedical Applications in Molecular, Structural, and Functional Imaging, Lake Buena Vista (Orlando Area), FL, USA, 27 February 2009; Volume 7262, pp. 121–128. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Hinrichs, J.B.; Murray, T.; Akin, M.; Lee, M.; Brehm, M.U.; Wilhelmi, M.; Wacker, F.K.; Rodt, T. Evaluation of a novel 2D perfusion angiography technique independent of pump injections for assessment of interventional treatment of peripheral vascular disease. Int. J. Cardiovasc. Imaging 2017, 33, 295–301. [Google Scholar] [CrossRef]
- Ng, J.J.; Papadimas, E.; Dharmaraj, R.B. Assessment of flow after lower extremity endovascular revascularisation: A feasibility study using time attenuation curve analysis of digital subtraction angiography. EJVES Short Rep. 2019, 45, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lou, W.-S.; Su, H.-B.; Huang, K.-Y.; He, X.; Chen, L.; Chen, G.-P.; Shi, W.-Y.; Han, J.-F.; Gu, J.-P. Evaluation of distal hemodynamic changes of lower extremity after endovascular treatment: Correlation between measurements of color-coded quantitative digital subtraction angiography and ankle-brachial index. J. Vasc. Interv. Radiol. 2016, 27, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Lou, W.; Gu, J. Clinical values of hemodynamics assessment by parametric color coding of digital sub-traction angiography before and after endovascular therapy for critical limb ischaemia. Zhonghua Yi Xue Za Zhi 2015, 95, 3036–3040. [Google Scholar] [PubMed]
- Troisi, N.; Michelagnoli, S.; Panci, S.; Bacchi, S.; Incerti, D.; Vecchio, L.L.; Dedola, G.L.; Chisci, E. Association of 2D perfusion angiography and wound healing rate in combined femoro-popliteal and below-the-knee lesions in ischemic patients undergoing isolated femoro-popliteal endovascular revascularization. Int. J. Low. Extrem. Wounds 2021. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Z.-G.; Zhang, X.-B.; Han, J.-F.; Beilner, J.; Deuerling-Zheng, Y.; Chi, J.-C.; Wang, J.; Qian, L.-J.; Zhou, Y.; Xu, J.-R. Hepatic blood volume imaging with the use of flat-detector CT perfusion in the angiography suite: Comparison with results of conventional multislice CT perfusion. J. Vasc. Interv. Radiol. 2014, 25, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Peynircioğlu, B.; Hızal, M.; Cil, B.; Deuerling-Zheng, Y.; Von Roden, M.; Hazirolan, T.; Akata, D.; Ozmen, M.N.; Balkanci, F.; Hizal, M.; et al. Quantitative liver tumor blood volume measurements by a C-arm CT post-processing software before and after hepatic arterial embolization therapy: Comparison with MDCT perfusion. Diagn. Interv. Radiol. 2015, 21, 71–77. [Google Scholar] [CrossRef]
- Rathmann, N.; Kara, K.; Budjan, J.; Henzler, T.; Smakic, A.; Schoenberg, S.O.; Diehl, S.J. Parenchymal liver blood volume and dynamic volume perfusion CT measurements of hepatocellular carcinoma in patients undergoing transarterial chemoembolization. Anticancer Res. 2017, 37, 5681–5685. Available online: http://ar.iiarjournals.org/content/37/10/5681. [PubMed]
- Syha, R.; Gatidis, S.; Grözinger, G.; Grosse, U.; Maurer, M.; Zender, L.; Horger, M.; Nikolaou, K.; Ketelsen, D. C-arm computed tomography and volume perfusion computed tomography (VPCT)-based assessment of blood volume changes in hepatocellular carcinoma in prediction of midterm tumor response to transarterial chemoembolization: A single center retrospective trial. Cancer Imaging 2016, 16, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crummy, A.; Strother, C.; Sackett, J.; Ergun, D.; Shaw, C.; Kruger, R.; Mistretta, C.; Turnipseed, W.; Lieberman, R.; Myerowitz, P.; et al. Computerized fluoroscopy: Digital subtraction for intravenous angiocardiography and arteriography. Am. J. Roentgenol. 1980, 135, 1131–1140. [Google Scholar] [CrossRef]
- Kruger, R.A.; Mistretta, C.A.; Houk, T.L.; Riederer, S.J.; Shaw, C.G.; Goodsitt, M.M.; Crummy, A.B.; Zwiebel, W.; Lancaster, J.C.; Rowe, G.G.; et al. Computerized fluoroscopy in real time for noninvasive visualization of the cardiovascular system. Radiology 1979, 130, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Meaney, T.; Weinstein, M.; Buonocore, E.; Pavlicek, W.; Borkowski, G.; Gallagher, J.; Sufka, B.; MacIntyre, W. Digital subtraction angiography of the human cardiovascular system. Am. J. Roentgenol. 1980, 135, 1153–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ovitt, T.; Capp, M.P.; Christenson, P.; Fisher, H.D.; Frost, M.M.; Nudelman, S.; Roehrig, H.; Seeley, G. The Development of a digital video subtraction system for intravenous angiography. In Noninvasive Cardiovascular Measurements; Proc. SPIE 0167: Palo Alto, USA, 1979; pp. 61–66. [Google Scholar]
- Mistretta, C.A. Digital videoangiography. Diagn. Imaging 1981, 3, 14–25. [Google Scholar]
- Ipema, J.; Heinen, S.G.; Janssens, A.J.; Potters, F.H.; Ünlü, Ç.; de Vries, J.-P.P.; Heuvel, D.A.V.D. Repeatability, and intra-observer and interobserver agreement of two dimensional perfusion angiography in patients with chronic limb threatening Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 980–987. [Google Scholar] [CrossRef]
- Syha, R.; Grözinger, G.; Grosse, U.; Maurer, M.; Zender, L.; Horger, M.; Nikolaou, K.; Ketelsen, D. C-arm computed tomography parenchymal blood volume measurement in evaluation of hepatocellular carcinoma before transarterial chemoembolization with drug eluting beads. Cancer Imaging 2015, 15, 22. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. In Seminars in Liver Disease; Thieme Medical Publishers, Inc.: New York, NY, USA, 1999; Volume 19, pp. 329–338. [Google Scholar]
- Sommer, C.; Stampfl, U.; Kauczor, H.; Pereira, P. Nationale S3-leitlinie hepatozelluläres karzinom. Der Radiol. 2014, 54, 642–653. [Google Scholar] [CrossRef]
- Vogl, T.J.; Lammer, J.; Lencioni, R.; Malagari, K.; Watkinson, A.; Pilleul, F.; Denys, A.; Lee, C. Liver, gastrointestinal, and cardiac toxicity in intermediate hepatocellular carcinoma treated with PRECISION TACE with drug-eluting beads: Results from the PRECISION V randomized trial. Am. J. Roentgenol. 2011, 197, W562–W570. [Google Scholar] [CrossRef]
- Reed, G.W.; Salehi, N.; Giglou, P.R.; Kafa, R.; Malik, U.; Maier, M.; Shishehbor, M.H. Time to wound healing and major adverse limb events in patients with critical limb ischemia treated with endovascular revascularization. Ann. Vasc. Surg. 2016, 36, 190–198. [Google Scholar] [CrossRef]
- Bradbury, A.W.; Adam, D.J.; Bell, J.; Forbes, J.F.; Fowkes, F.G.R.; Gillespie, I.; Raab, G.; Ruckley, C.V. Multicentre randomised controlled trial of the clinical and cost-effectiveness of a by-pass-surgery-first versus a balloon-angioplasty-first revascularisation strategy for severe limb ischaemia due to in-frainguinal disease. The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial. Health Technol. Assess. 2010, 14, 1–236. [Google Scholar]
- Reed, G.W.; Raeisi-Giglou, P.; Kafa, R.; Malik, U.; Salehi, N.; Shishehbor, M.H. Hospital readmissions following endovascular therapy for critical limb ischemia: Associations with wound healing, major adverse limb events, and mortality. J. Am. Heart Assoc. 2016, 5, e003168. [Google Scholar] [CrossRef] [Green Version]
- Rajebi, M.R.; Benenati, M.J.; Schernthaner, M.B.; Walker, G.; Gandhi, R.T.; Pena, C.S.; Katzen, B.T. Reliability and accuracy of simple visual estimation in assessment of peripheral arterial stenosis. J. Vasc. Interv. Radiol. 2015, 26, 890–896. [Google Scholar] [CrossRef]
- Cossman, D.V.; Ellison, J.E.; Wagner, W.H.; Carroll, R.M.; Treiman, R.L.; Foran, R.F.; Levin, P.M.; Cohen, J. Comparison of contrast arteriography to arterial mapping with color-flow duplex imaging in the lower extremities. J. Vasc. Surg. 1989, 10, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Cooper, K.; Peña, C.; Benenati, J. Determining end points for critical limb ischemia interventions. Technol. Vasc. Interv. Radiol. 2016, 19, 104–112. [Google Scholar] [CrossRef]
- Boezeman, R.P.E.; Becx, B.P.; Van den Heuvel, D.A.F.; Ünlü, Ç.; Vos, J.A.; de Vries, J.P.P.M. Monitoring of foot oxy-genation with near-infrared spectroscopy in patients with critical limb ischemia undergoing percutaneous translu-minal angioplasty: A pilot study. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 650–656. [Google Scholar] [CrossRef] [Green Version]
- Schreuder, S.M.; Nieuwdorp, M.; Koelemay, M.J.W.; Bipat, S.; AReekers, J. Testing the sympathetic nervous system of the foot has a high predictive value for early amputation in patients with diabetes with a neuroischemic ulcer. BMJ Open Diabetes Res. Care 2018, 6, e000592. [Google Scholar] [CrossRef] [Green Version]
- Salem, R.; Sangro, B. Transarterial chemoembolization and radioembolization. Semin. Liver Dis. 2014, 34, 435–443. [Google Scholar] [CrossRef]
- Llovet, J.M.; Montal, R.; Villanueva, A. Randomized trials and endpoints in advanced HCC: Role of PFS as a surrogate of survival. J. Hepatol. 2019, 70, 1262–1277. [Google Scholar] [CrossRef] [Green Version]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef]
- Bauknecht, H.-C.; Romano, V.C.; Rogalla, P.; Klingebiel, R.; Wolf, C.; Bornemann, L.; Hamm, B.; Hein, P.A. Intra- and interobserver variability of linear and volumetric measurements of brain metastases using contrast-enhanced magnetic resonance imaging. Investig. Radiol. 2010, 45, 49–56. [Google Scholar] [CrossRef]
- Tognolini, A.; Louie, J.D.; Hwang, G.L.; Hofmann, L.V.; Sze, D.Y.; Kothary, N. Utility of C-arm CT in patients with hepatocellular carcinoma undergoing transhepatic arterial chemoembolization. J. Vasc. Interv. Radiol. 2010, 21, 339–347. [Google Scholar] [CrossRef]
- Kakeda, S.; Korogi, Y.; Ohnari, N.; Moriya, J.; Oda, N.; Nishino, K.; Miyamoto, W. Usefulness of cone-beam volume CT with flat panel detectors in conjunction with catheter angiography for transcatheter arterial embolization. J. Vasc. Interv. Radiol. 2007, 18, 1508–1516. [Google Scholar] [CrossRef]
- Miyayama, S.; Yamashiro, M.; Ikuno, M.; Okumura, K.; Yoshida, M. Ultraselective transcatheter arterial che-moembolization for small hepatocellular carcinoma guided by automated tumor-feeders detection software: Tech-nical success and short-term tumor response. Abdom Imaging 2014, 39, 645–656. [Google Scholar] [CrossRef]
- Syha, R.; Grünwald, L.; Horger, T.; Spira, D.; Ketelsen, D.; Vogel, W.; Claussen, C.D.; Horger, M. Assessment of the nature of residual masses at end of treatment in lymphoma patients using volume perfusion computed tomography. Eur. Radiol. 2014, 24, 770–779. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study, Year, and Design | Cohort | Reference Technique | Variables Measured from C-Arm CT |
|---|---|---|---|
| Technique: 2D perfusion angiography | |||
| Hinrichs 2016 [26], retrospective | PAD 1, n = 21 | ABI 2 | TTP 3, PD 4, and AUC 5 |
| Ng 2019 [27], retrospective | PAD 1, n = 47 | ABI 2, TBI 6 | TTP 3, Imax 7, and washin 8 and washout 9 gradients |
| Lou 2016 [28], retrospective | PAD 1, n = 19 | ABI 2 | TTP 3 |
| Su 2015 [29], prospective | PAD 1, n = 21 | ABI 2, TcPO2 10 | TTP 3 |
| Troisi 2021 [30], prospective | PAD 1, n = 24 | TcPO2 10 | TDC 11 |
| Technique: Dual-phase CBCT 12 perfusion | |||
| Zhuang 2014 [31], prospective | HCC 13, n = 20 | CTP 14 (CBV) 15 | PBV 16 |
| Peynircioğlu 2014 [32], prospective | HCC 13, n = 14 | CTP 14 (CBV) 15 | PBV 16 |
| Rathmann 2017 [33], prospective | HCC 13, n = 16 | CTP 14 (CBV) 15 | PBV 16 |
| Syha 2016 [34], retrospective | HCC 13, n = 25 | CTP 14 (CBV) 15 | PBV 16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaid Al-Kaylani, A.H.A.; Schuurmann, R.C.L.; Maathuis, W.D.; Slart, R.H.J.A.; De Vries, J.-P.P.M.; Bokkers, R.P.H. Clinical Applications of Quantitative Perfusion Imaging with a C-Arm Flat-Panel Detector—A Systematic Review. Diagnostics 2023, 13, 128. https://doi.org/10.3390/diagnostics13010128
Zaid Al-Kaylani AHA, Schuurmann RCL, Maathuis WD, Slart RHJA, De Vries J-PPM, Bokkers RPH. Clinical Applications of Quantitative Perfusion Imaging with a C-Arm Flat-Panel Detector—A Systematic Review. Diagnostics. 2023; 13(1):128. https://doi.org/10.3390/diagnostics13010128
Chicago/Turabian StyleZaid Al-Kaylani, Abdallah H. A., Richte C. L. Schuurmann, Wouter D. Maathuis, Riemer H. J. A. Slart, Jean-Paul P. M. De Vries, and Reinoud P. H. Bokkers. 2023. "Clinical Applications of Quantitative Perfusion Imaging with a C-Arm Flat-Panel Detector—A Systematic Review" Diagnostics 13, no. 1: 128. https://doi.org/10.3390/diagnostics13010128