
Diagnosis and Treatment of Acute Pancreatitis

 , ,
, ,
Abstract
:1. Introduction
2. Classification of Acute Pancreatitis
3. Diagnosis of Acute Pancreatitis
3.1. Laboratory Test and Indicator Enzymes
3.2. Laboratory Tests
3.2.1. Serum Lipase and Amylase
3.2.2. Urinary Trypsinogen-2
3.2.3. Urinary Amylase
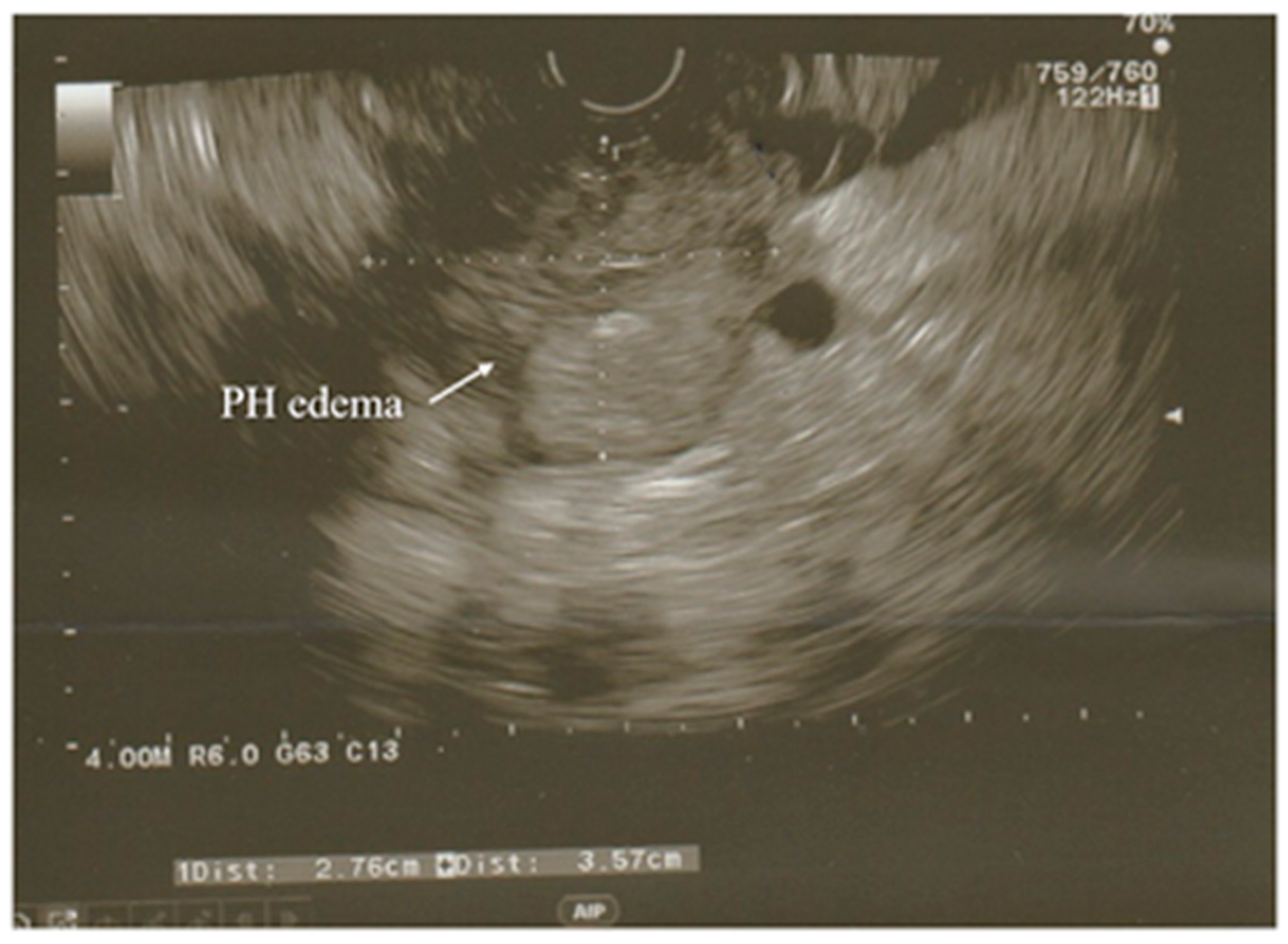
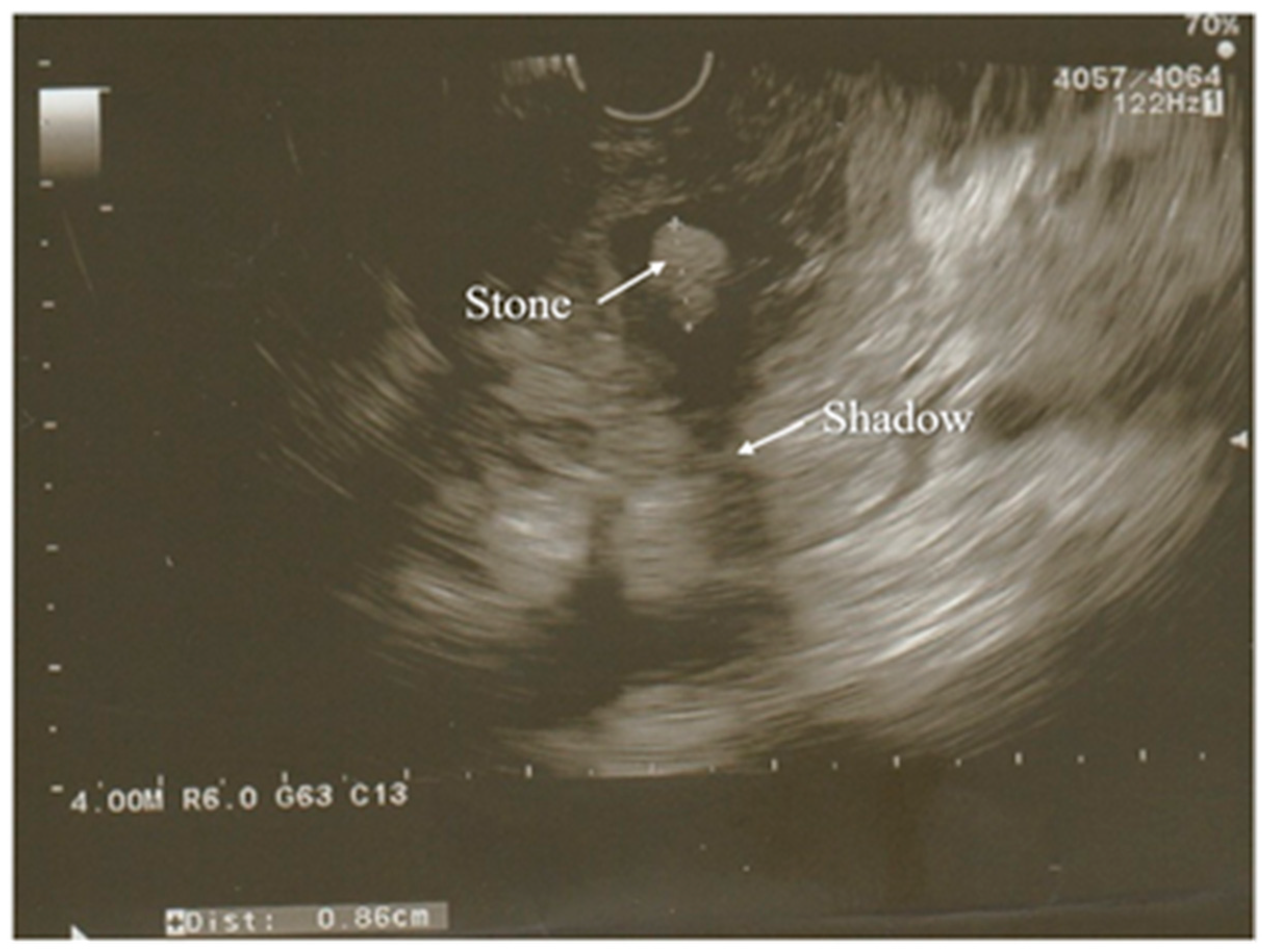
3.3. Ultrasonography
3.4. Magnetic Resonance Imaging
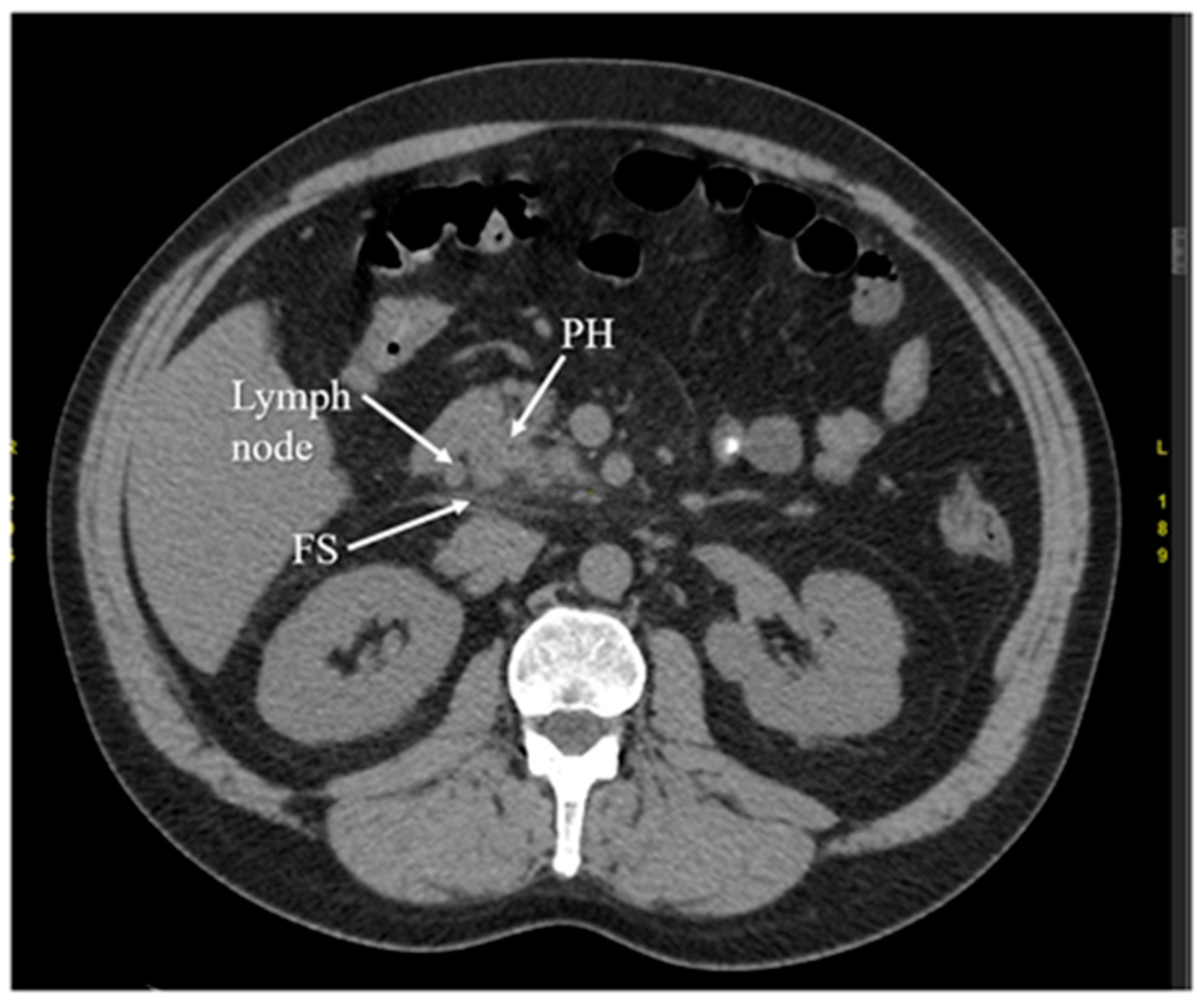
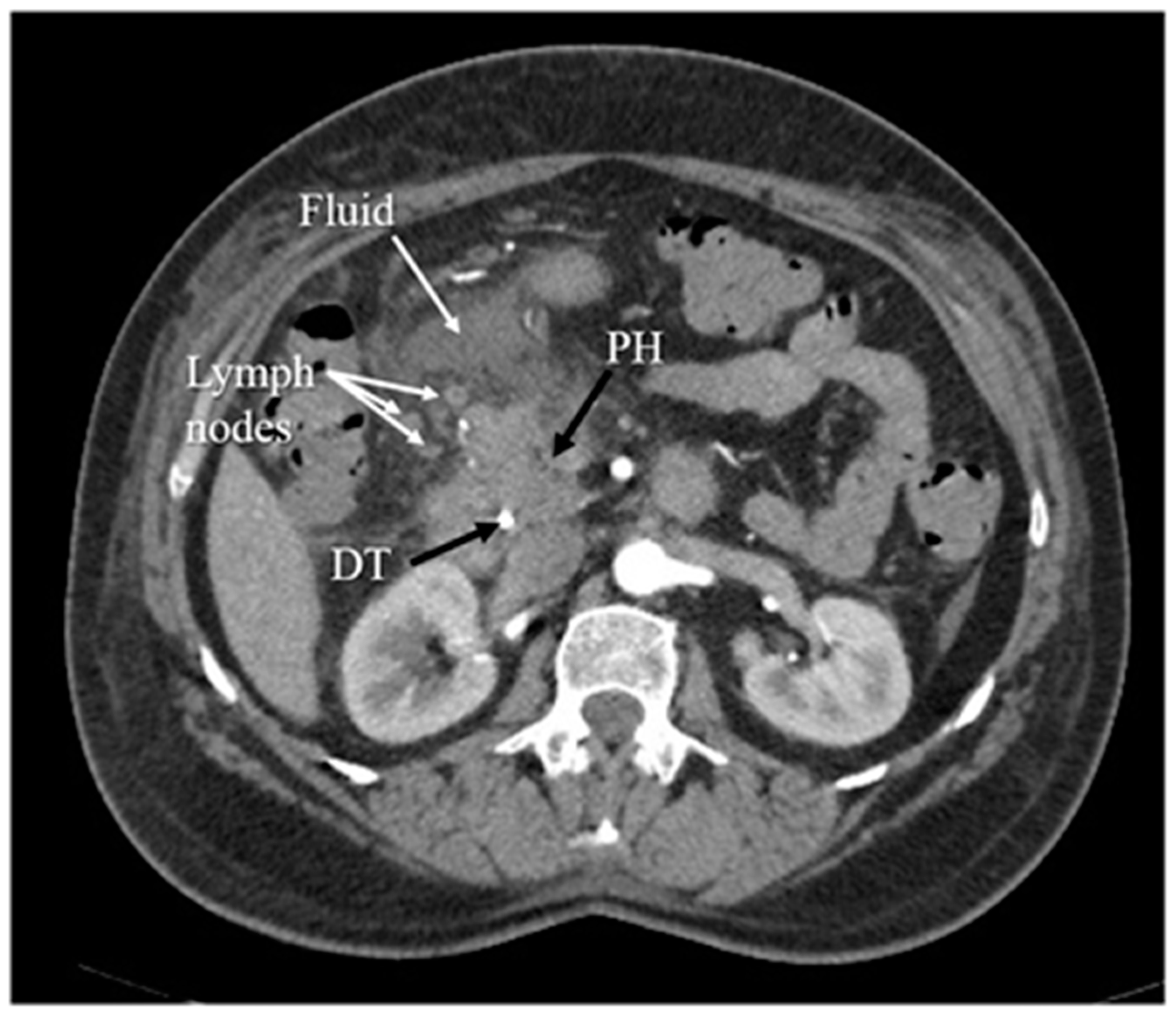
3.5. Computed Tomography
4. Etiology of Acute Pancreatitis
5. Assessment of Severity of Acute Pancreatitis
5.1. Serum C-Reactive Protein and Other Laboratory Assays
5.2. Severity-of-Disease Rating Systems
5.3. Assessment of Organ Failure
6. Management of Acute Pancreatitis
6.1. Supportive Care
6.2. Improvement of Laboratory Parameters
6.3. Nutrition
6.4. Pharmacological and Antimicrobial Treatment
6.5. Surgical and Operative Treatment
7. Prevention of Acute Pancreatitis
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Classification of acute pancreatitis—2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.A.; Hsu, J.; Bawazeer, M.; Marshall, J.; Friedrich, J.O.; Nathens, A.; Coburn, N.; May, G.R.; Pearsall, E.; McLeod, R.S. Clinical practice guideline: Management of acute pancreatitis. Can. J. Surg. 2016, 59, 128–140. [Google Scholar] [CrossRef]
- Leppäniemi, A.; Tolonen, M.; Tarasconi, A.; Lohse, H.A.S.; Gamberini, E.; Kirkpatrick, A.W.; Ball, C.G.; Parry, N.; Sartelli, M.; Wolbrink, D.R.J.; et al. WSES guidelines for the management of severe acute pancreatitis. World J. Emerg. Surg. 2019, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Besselink, M.; van Santvoort, H.; Freeman, M.; Gardner, T.; Mayerle, J.; Vege, S.S.; Werner, J.; Banks, P.; McKay, C.; Fernandez-del Castillo, C.; et al. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, E1–E15. [Google Scholar]
- Machicado, J.D.; Yadav, D. Epidemiology of Recurrent Acute and Chronic Pancreatitis: Similarities and Differences. Dig. Dis. Sci. 2017, 62, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Párniczky, A.; Kui, B.; Szentesi, A.; Balázs, A.; Szűcs, A.; Mosztbacher, D.; Czimmer, J.; Sarlós, P.; Bajor, J.; Gódi, S.; et al. Prospective, Multicentre, Nationwide Clinical Data from 600 Cases of Acute Pancreatitis. PLoS ONE 2016, 11, e0165309. [Google Scholar] [CrossRef]
- Ali, U.A.; Issa, Y.; Hagenaars, J.C.; Bakker, O.J.; van Goor, H.; Nieuwenhuijs, V.B.; Bollen, T.L.; van Ramshorst, B.; Witteman, B.J.; Brink, M.A.; et al. Risk of Recurrent Pancreatitis and Progression to Chronic Pancreatitis After a First Episode of Acute Pancreatitis. Clin. Gastroenterol. Hepatol. 2016, 14, 738–746. [Google Scholar]
- Gao, Y.J.; Li, Y.Q.; Wang, Q.; Li, S.L.; Li, G.Q.; Ma, J.; Zeng, X.Z.; Huang, L.Y.; Yuan, S.A.; Liu, C.A.; et al. Analysis of the clinical features of recurrent acute pancreatitis in China. J. Gastroenterol. 2006, 41, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.; O’Connell, M.; Papachristou, G.I. Natural history following the first attack of acute pancreatitis. Am. J. Gastroenterol. 2012, 107, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Yi, F.; Ge, L.; Zhao, J.; Lei, Y.; Zhou, F.; Chen, Z.; Zhu, Y.; Xia, B. Meta-analysis: Total parenteral nutrition versus total enteral nutrition in predicted severe acute pancreatitis. Intern. Med. 2012, 51, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Basnayake, C.; Ratnam, D. Blood tests for acute pancreatitis. Aust. Prescr. 2015, 38, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Pitchumoni, C.S.; Sivaprasad, A.V. Evaluating tests for acute pancreatitis. Am. J. Gastroenterol. 1990, 85, 1. [Google Scholar]
- Brizi, M.G.; Perillo, F.; Cannone, F.; Tuzza, L.; Manfredi, R. The role of imaging in acute pancreatitis. Radiol. Med. 2021, 126, 1017–1029. [Google Scholar] [CrossRef] [PubMed]
- Chase, C.W.; Barker, D.E.; Russell, W.L.; Burns, R.P. Serum amylase and lipase in the evaluation of acute abdominal pain. Am. Surg. 1996, 62, 1028–1033. [Google Scholar]
- Al-Bahrani, A.Z.; Ammori, B.J. Clinical laboratory assessment of acute pancreatitis. Clin. Chim. Acta 2005, 362, 26–48. [Google Scholar] [CrossRef]
- Párniczky, A.; Abu-El-Haija, M.; Husain, S.; Lowe, M.; Oracz, G.; Sahin-Tóth, M.; Szabó, F.K.; Uc, A.; Wilschanski, M.; Witt, H.; et al. EPC/HPSG evidence-based guidelines for the management of pediatric pancreatitis. Pancreatology 2018, 18, 146–160. [Google Scholar] [CrossRef]
- Rompianesi, G.; Hann, A.; Komolafe, O.; Pereira, S.P.; Davidson, B.R.; Gurusamy, K.S. Serum amylase and lipase and urinary trypsinogen and amylase for diagnosis of acute pancreatitis. Cochrane Database Syst. Rev. 2017, 2017, 5. [Google Scholar] [CrossRef]
- Keim, V.; Teich, N.; Fiedler, F.; Hartig, W.; Thiele, G.; Mössner, J. A comparison of lipase and amylase in the diagnosis of acute pancreatitis in patients with abdominal pain. Pancreas 1998, 16, 45–49. [Google Scholar] [CrossRef]
- Gwozdz, G.P.; Steinberg, W.M.; Werner, M.; Henry, J.P.; Pauley, C. Comparative evaluation of the diagnosis of acute pancreatitis based on serum and urine enzyme assays. Clin. Chim. Acta 1990, 187, 243–254. [Google Scholar] [CrossRef]
- Logie, J.J.; Cox, M.; Sharkey, J.; Williams, A. A multidisciplinary approach to an unusual cause of hyperamylasaemia. BMJ Case Rep. 2015, 2015, bcr2015209780. [Google Scholar] [CrossRef]
- Windsor, A.; Kanwar, S.; Li, A.G.K.; Barnes, E.; Guthrie, J.A.; Spark, J.I.; Welsh, F.; Guillou, P.J.; Reynolds, J.V. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. Gut 1998, 42, 431–435. [Google Scholar] [CrossRef]
- Matull, W.R.; Pereira, S.P.; O’Donohue, J.W. Biochemical markers of acute pancreatitis. J. Clin. Pathol. 2006, 59, 340–344. [Google Scholar] [CrossRef]
- Mayumi, T.; Inui, K.; Maetani, I.; Yokoe, M.; Sakamoto, T.; Yoshida, M.; Ko, S.; Hirata, K.; Takada, T. Validity of the urinary trypsinogen-2 test in the diagnosis of acute pancreatitis. Pancreas 2012, 41, 869–875. [Google Scholar] [CrossRef]
- Al-Omran, M.; AlBalawi, Z.H.; Tashkandi, M.F.; Al-Ansary, L.A. Enteral versus parenteral nutrition for acute pancreatitis (Review) Enteral versus parenteral nutrition for acute pancreatitis. Health Care 2010, 1, 4–6. [Google Scholar]
- Baillie, J. Rapid measurement of urinary trypsinogen-2 as a screening test for acute pancreatitis. Gastrointest. Endosc. 1997, 46, 385–386. [Google Scholar]
- Hedström, J.; Sainio, V.; Kemppainen, E.; Puolakkainen, P.; Haapiainen, R.; Kivilaakso, E.; Schauman, K.O.; Stenman, U.H. Urine trypsinogen-2 as marker of acute pancreatitis. Clin. Chem. 1996, 42, 685–690. [Google Scholar] [CrossRef]
- Kylänpää-Bäck, M.L.; Kemppainen, E.; Puolakkainen, P.; Hedström, J.; Haapiainen, R.; Korvuo, A.; Stenman, U.H. Comparison of urine trypsinogen-2 test strip with serum lipase in the diagnosis of acute pancreatitis. Hepato-Gastroenterol. 2002, 49, 1130–1134. [Google Scholar]
- Yasuda, H.; Kataoka, K.; Takeyama, Y.; Takeda, K.; Ito, T.; Mayumi, T.; Isaji, S.; Mine, T.; Kitagawa, M.; Kiriyama, S.; et al. Usefulness of urinary trypsinogen-2 and trypsinogen activation peptide in acute pancreatitis: A multicenter study in Japan. World J. Gastroenterol. 2019, 25, 107–117. [Google Scholar] [CrossRef]
- Hegewald, M.J.; Isenberg, G.; Sterling, R.K.; Cooper, G.S.; Chak, A.; Sivak, M.V. Evaluation of a rapid urine amylase test using post-ERCP hyperamylasemia as a model. Am. J. Gastroenterol. 2001, 96, 2640–2645. [Google Scholar] [CrossRef]
- Terui, K.; Hishiki, T.; Saito, T.; Mitsunaga, T.; Nakata, M.; Yoshida, H. Urinary amylase/urinary creatinine ratio (uAm/uCr)-a less-invasive parameter for management of hyperamylasemia. BMC Pediatrics 2013, 13, 205. [Google Scholar] [CrossRef]
- Bree, R.L.; Ralls, P.W.; Balfe, D.M.; DiSantis, D.J.; Glick, S.N.; Levine, M.S.; Megibow, A.; Saini, S.; Shuman, W.P.; Greene, F.L.; et al. Evaluation of patients with acute right upper quadrant pain. American College of Radiology. ACR Appropr. Criteria. Radiol. 2000, 215, 153–157. [Google Scholar]
- Bar-Meir, S. Gallstones: Prevalence, diagnosis and treatment. Isr. Med. Assoc. J. IMAJ. 2001, 3, 111–113. [Google Scholar]
- Benarroch-Gampel, J.; Boyd, C.A.; Sheffield, K.M.; Townsend, C.M.; Riall, T.S. Overuse of ct in patients with complicated gallstone disease. J. Am. Coll. Surg. 2011, 213, 524–530. [Google Scholar] [CrossRef]
- Brown, A.; Baillargeon, J.D.; Hughes, M.D.; Banks, P.A. Can fluid resuscitation prevent pancreatic necrosis in severe acute pancreatitis? Pancreatology 2002, 2, 104–107. [Google Scholar] [CrossRef]
- Portincasa, P.; Moschetta, A.; Petruzzelli, M.; Palasciano, G.; di Ciaula, A.; Pezzolla, A. Symptoms and diagnosis of gallbladder stones. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 1017–1029. [Google Scholar] [CrossRef]
- Sun, H.; Zuo, H.-D.; Lin, Q.; Yang, D.-D.; Zhou, T.; Tang, M.-Y.; Wáng, Y.X.J.; Zhang, X.-M. MR imaging for acute pancreatitis: The current status of clinical applications. Ann. Transl. Med. 2019, 7, 269. [Google Scholar] [CrossRef]
- Thevenot, A.; Bournet, B.; Otal, P.; Canevet, G.; Moreau, J.; Buscail, L. Endoscopic ultrasound and magnetic resonance cholangiopancreatography in patients with idiopathic acute pancreatitis. Dig. Dis. Sci. 2013, 58, 2361–2368. [Google Scholar] [CrossRef]
- Somani, P.; Sunkara, T.; Sharma, M. Role of endoscopic ultrasound in idiopathic pancreatitis. World J. Gastroenterol. 2017, 23, 6952–6961. [Google Scholar] [CrossRef]
- Liu, C.-L.; Lo, C.-M.; Chan, J.K.-F.; Poon, R.T.-P.; Lam, C.-M.; Fan, S.-T.; Wong, J. Detection of choledocholithiasis by EUS in acute pancreatitis: A prospective evaluation in 100 consecutive patients. Gastrointest. Endosc. 2001, 54, 325–330. [Google Scholar] [CrossRef]
- Sirli, R.; Sporea, I. Ultrasound examination of the normal pancreas. Med. Ultrason. 2010, 12, 62–65. [Google Scholar]
- Rizk, M.K.; Gerke, H. Utility of endoscopic ultrasound in pancreatitis: A review. World J. Gastroenterol. 2007, 13, 6321. [Google Scholar] [CrossRef]
- Kotwal, V.; Talukdar, R.; Levy, M.; Vege, S.S. Role of endoscopic ultrasound during hospitalization for acute pancreatitis. World J. Gastroenterol. 2010, 16, 4888. [Google Scholar] [CrossRef]
- Guda, N.M.; Trikudanathan, G.; Freeman, M.L. Idiopathic recurrent acute pancreatitis. Lancet Gastroenterol. Hepatol. 2018, 3, 720–728. [Google Scholar] [CrossRef]
- Somani, P.; Navaneethan, U. Role of ERCP in Patients With Idiopathic Recurrent Acute Pancreatitis. Curr. Treat. Options Gastroenterol. 2016, 14, 327–339. [Google Scholar]
- Uhl, W.; Warshaw, A.; Imrie, C.; Bassi, C.; McKay, C.J.; Lankisch, P.G.; Carter, R.; Di Magno, E.; Banks, P.A.; Whitcomb, D.C.; et al. IAP guidelines for the surgical management of acute pancreatitis. Pancreatology 2002, 2, 565–573. [Google Scholar] [CrossRef]
- Romagnuolo, J.; Bardou, M.; Rahme, E.; Joseph, L.; Reinhold, C.; Barkun, A.N. Magnetic Resonance Cholangiopancreatography: A Meta-Analysis of Test Performance in Suspected Biliary Disease. Annals of Internal Medicine. 2003, 139, 547–557. [Google Scholar] [CrossRef]
- Duncan, C.B.; Riall, T.S. Evidence-Based Current Surgical Practice: Calculous Gallbladder Disease. J. Gastrointest. Surg. 2012, 16, 2011–2025. [Google Scholar] [CrossRef]
- Raghuwanshi, S.; Gupta, R.; Vyas, M.M.; Sharma, R. CT evaluation of acute pancreatitis and its prognostic correlation with CT severity index. J. Clin. Diagn. Res. 2016, 10, TC06. [Google Scholar] [CrossRef]
- Balthazar, E.J. Acute pancreatitis: Assessment of severity with clinical and CT evaluation. Radiology 2002, 223, 603–613. [Google Scholar] [CrossRef]
- Beger, H.G.; Bittner, R.; Block, S.; Büchler, M. Bacterial contamination of pancreatic necrosis. A prospective clinical study. Gastroenterology 1986, 91, 433–438. [Google Scholar] [CrossRef]
- Johnson, C.D. UK guidelines for the management of acute pancreatitis. Gut 2005, 54, iii1. [Google Scholar]
- Nordback, I.; Pelli, H.; Lappalainen–Lehto, R.; Järvinen, S.; Räty, S.; Sand, J. The Recurrence of Acute Alcohol-Associated Pancreatitis Can Be Reduced: A Randomized Controlled Trial. Gastroenterology 2009, 136, 848–855. [Google Scholar] [CrossRef]
- James, T.W.; Crockett, S.D. Management of acute pancreatitis in the first 72 hours. Curr. Opin. Gastroenterol. 2018, 34, 330–335. [Google Scholar] [CrossRef]
- Johnson, C.; Lévy, P. Detection of gallstones in acute pancreatitis: When and how? Pancreatology 2010, 10, 27–32. [Google Scholar] [CrossRef]
- Lankisch, P.G.; Lowenfels, A.B.; Maisonneuve, P.; Oría, A. What is the risk of alcoholic pancreatitis in heavy drinkers? Pancreas 2002, 25, 411–412. [Google Scholar] [CrossRef]
- Yadav, D.; Eigenbrodt, M.L.; Briggs, M.J.; Williams, D.K.; Wiseman, E.J. Pancreatitis: Prevalence and risk factors among male veterans in a detoxification program. Pancreas 2007, 34, 390–398. [Google Scholar] [CrossRef]
- Garg, R.; Rustagi, T. Management of Hypertriglyceridemia Induced Acute Pancreatitis. BioMed Res. Int. 2018, 2018, 4721357. [Google Scholar] [CrossRef]
- Yadav, D.; Pitchumoni, C.S. Issues in Hyperlipidemic Pancreatitis. J. Clin. Gastroenterol. 2003, 36, 54–62. [Google Scholar] [CrossRef]
- Badalov, N.; Baradarian, R.; Iswara, K.; Li, J.; Steinberg, W.; Tenner, S. Drug-Induced Acute Pancreatitis: An Evidence-Based Review. Clin. Gastroenterol. Hepatol. 2007, 5, 648–661. [Google Scholar] [CrossRef]
- Wolfe, D.; Kanji, S.; Yazdi, F.; Barbeau, P.; Rice, D.; Beck, A.; Butler, C.; Esmaeilisaraji, L.; Skidmore, B.; Moher, D.; et al. Drug induced pancreatitis: A systematic review of case reports to determine potential drug associations. PLoS ONE 2020, 15, e0231883. [Google Scholar] [CrossRef]
- Kochar, B.; Akshintala, V.S.; Afghani, E.; Elmunzer, B.J.; Kim, K.J.; Lennon, A.M.; Khashab, M.A.; Kalloo, A.N.; Singh, V.K. Incidence, severity, and mortality of post-ERCP pancreatitis: A systematic review by using randomized, controlled trials. Gastrointest. Endosc. 2015, 81, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekhara, V.; Khashab, M.A.; Muthusamy, V.R.; Acosta, R.D.; Agrawal, D.; Bruining, D.H.; Eloubeidi, M.A.; Fanelli, R.D.; Faulx, A.L.; Gurudu, S.R.; et al. Adverse events associated with ERCP. Gastrointest. Endosc. 2017, 85, 32–47. [Google Scholar] [CrossRef] [PubMed]
- Blaho, M.; Dítě, P.; Kunovský, L.; Kianička, B. Autoimmune pancreatitis—An ongoing challenge. Adv. Med. Sci. 2020, 65, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, A.; Inoue, D.; Takahashi, N. Autoimmune pancreatitis: An update. Abdom. Radiol. 2020, 45, 1359–1370. [Google Scholar] [CrossRef] [PubMed]
- Kamisawa, T.; Chari, S.T.; Lerch, M.M.; Kim, M.-H.; Gress, T.M.; Shimosegawa, T. Recent advances in autoimmune pancreatitis: Type 1 and type 2. Postgrad. Med. J. 2014, 90, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, K.; Zamboni, G. IgG4-related disease. Pathologica 2012, 104, 1–3. [Google Scholar]
- Pieringer, H.; Parzer, I.; Wöhrer, A.; Reis, P.; Oppl, B.; Zwerina, J. IgG4- related disease: An orphan disease with many faces. Orphanet J. Rare Dis. 2014, 9, 110. [Google Scholar] [CrossRef]
- Hart, P.A.; Zen, Y.; Chari, S.T. Recent Advances in Autoimmune Pancreatitis. Gastroenterology 2015, 149, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Mitsuyama, T.; Uchida, K.; Sumimoto, K.; Fukui, Y.; Ikeura, T.; Fukui, T.; Nishio, A.; Shikata, N.; Uemura, Y.; Satoi, S.; et al. Comparison of neutrophil infiltration between type 1 and type 2 autoimmune pancreatitis. Pancreatology 2015, 15, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, M.; Wallace, M.B. Diagnostic approach to patients with acute idiopathic and recurrent pancreatitis, what should be done? World J. Gastroenterol. 2008, 14, 1007. [Google Scholar] [CrossRef]
- Gurusamy, K.S.; Debray, T.; Rompianesi, G. Prognostic models for predicting the severity and mortality in people with acute pancreatitis. Cochrane Database Syst. Rev. 2018, 2018, CD013026. [Google Scholar] [CrossRef]
- Fei, Y.; Gao, K.; Tu, J.; Wang, W.; Zong, G.-Q.; Li, W.-Q. Predicting and evaluation the severity in acute pancreatitis using a new modeling built on body mass index and intra-abdominal pressure. Am. J. Surg. 2018, 216, 304–309. [Google Scholar] [CrossRef]
- Wang, S.-Q.; Li, S.-J.; Feng, Q.-X.; Feng, X.-Y.; Xu, L.; Zhao, Q.-C. Overweight is an additional prognostic factor in acute pancreatitis: A meta-analysis. Pancreatology 2011, 11, 92–98. [Google Scholar] [CrossRef]
- Mayer, J.M.; Raraty, M.; Slavin, J.; Kemppainen, E.; Fitzpatrick, J.; Hietaranta, A.; Puolakkainen, P.; Beger, H.G.; Neoptolemos, J.P. Serum amyloid A is a better early predictor of severity than C-reactive protein in acute pancreatitis. Br. J. Surg. 2002, 89, 163–171. [Google Scholar]
- WWu, X.; Zheng, R.; Lin, H.; Zhuang, Z.; Zhang, M.; Yan, P. Effect of transpulmonary pressure-directed mechanical ventilation on respiration in severe acute pancreatitis patient with intraabdominal hypertension. Natl. Med. J. China 2015, 95, 3168–3172. [Google Scholar]
- Farkas, N.; Hanák, L.; Mikó, A.; Bajor, J.; Sarlós, P.; Czimmer, J.; Vincze; Gódi, S.; Pécsi, D.; Varjú, P.; et al. A Multicenter, International Cohort Analysis of 1435 Cases to Support Clinical Trial Design in Acute Pancreatitis. Front. Physiol. 2019, 10, 1092. [Google Scholar] [CrossRef] [PubMed]
- Arif, A.; Jaleel, F.; Rashid, K. Accuracy of BISAP score in prediction of severe acute pancreatitis. Pak. J. Med. Sci. 2019, 35, 1008–1012. [Google Scholar] [CrossRef]
- Jones, J.; Gaillard, F. Ranson Criteria. In Radiopaedia.org; StatPearls: Treasure Island, FL, USA, 2009. [Google Scholar]
- Ma, X.; Li, L.; Jin, T.; Xia, Q. Harmless acute pancreatitis score on admission can accurately predict mild acute pancreatitis. Nan Fang Yi Ke Da Xue Xue Bao 2020, 40, 190–195. [Google Scholar] [PubMed]
- Sayraç, A.V.; Cete, Y.; Sayrac, N. Utility of HAPS for predicting prognosis in acute pancreatitis. Ulus. Travma Ve Acil Cerrahi Derg. 2018, 24, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Al-Qahtani, H.H.; Alam, M.K.; Waheed, M. Comparison of harmless acute pancreatitis score with Ranson’s score in predicting the severity of acute pancreatitis. J. Coll. Physicians Surg. Pak. 2017, 27, 75–79. [Google Scholar] [PubMed]
- Godinjak, A.; Iglica, A.; Rama, A.; Tančica, I.; Jusufović, S.; Ajanović, A.; Kukuljac, A. Predictive value of SAPS II and APACHE II scoring systems for patient outcome in a medical intensive care unit. Acta Med. Acad 2016, 45, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Le Mee, J.; Paye, F.; Sauvanet, A.; O’Toole, D.; Hammel, P.; Marty, J.; Ruszniewski, P.; Belghiti, J. Incidence and reversibility of organ failure in the course of sterile or infected necrotizing pancreatitis. Arch. Surg. 2001, 136, 1386–1390. [Google Scholar] [CrossRef]
- Isenmann, R.; Rau, B.; Beger, H.G. Bacterial infection and extent of necrosis are determinants of organ failure in patients with acute necrotizing pancreatitis. Br. J. Surg. 1999, 86, 1020–1024. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.; Whang, E.E.; Brooks, D.C.; Moore, F.D.; Hughes, M.D.; Sica, G.T.; Zinner, M.J.; Ashley, S.W.; Banks, P.A. Is severity of necrotizing pancreatitis increased in extended necrosis and infected necrosis? Pancreas 2002, 25, 229–233. [Google Scholar] [CrossRef]
- Kumar, A.H.; Griwan, M.S. A comparison of APACHE II, BISAP, Ranson’s score and modified CTSI in predicting the severity of acute pancreatitis based on the 2012 revised Atlanta Classification. Gastroenterol. Rep. 2018, 6, 127–131. [Google Scholar] [CrossRef]
- Balthazar, E.J.; Robinson, D.L.; Megibow, A.J.; Ranson, J.H.C. Acute pancreatitis: Value of CT in establishing prognosis. Radiology 1990, 174, 331–336. [Google Scholar] [CrossRef]
- Mortelé, K.J.; Mergo, P.J.; Taylor, H.M.; Wiesner, W.; Cantisani, V.; Ernst, M.D.; Kalantari, B.N.; Ros, P.R. Peripancreatic vascular abnormalities complicating acute pancreatitis: Contrast-enhanced helical CT findings. Eur. J. Radiol. 2004, 52, 67–72. [Google Scholar] [CrossRef]
- Bollen, T.L.; Singh, V.K.; Maurer, R.; Repas, K.; van Es, H.W.; Banks, P.A.; Mortele, K.J. Comparative evaluation of the modified CT severity index and CT severity index in assessing severity of acute pancreatitis. Am. J. Roentgenol. 2011, 197, 386–392. [Google Scholar] [CrossRef]
- Banday, I.A.; Gattoo, I.; Khan, A.M.; Javeed, J.; Gupta, G.; Latief, M. Modified computed tomography severity index for evaluation of acute pancreatitis and its correlation with clinical outcome: A tertiary care hospital based observational study. J. Clin. Diagn. Res. 2015, 9, TC01. [Google Scholar] [CrossRef]
- Kui, B.; Pintér, J.; Molontay, R.; Nagy, M.; Farkas, N.; Gede, N.; Vincze; Bajor, J.; Gódi, S.; Czimmer, J.; et al. EASY-APP: An artificial intelligence model and application for early and easy prediction of severity in acute pancreatitis. Clin. Transl. Med. 2022, 12, e842. [Google Scholar] [CrossRef]
- Chang, K.; Lu, W.; Zhang, K.; Jia, S.; Li, F.; Wang, F.; Deng, S.; Chen, M. Rapid urinary trypsinogen-2 test in the early diagnosis of acute pancreatitis: A meta-analysis. Clin. Biochem. 2012, 45, 1051–1056. [Google Scholar] [CrossRef]
- Johnson, C.D.; Abu-Hilal, M. Persistent organ failure during the first week as a marker of fatal outcome in acute pancreatitis. Gut 2004, 53, 1340–1344. [Google Scholar] [CrossRef] [PubMed]
- Mofidi, R.; Duff, M.D.; Wigmore, S.J.; Madhavan, K.K.; Garden, O.J.; Parks, R.W. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. Br. J. Surg. 2006, 93, 738–744. [Google Scholar] [CrossRef]
- De-Madaria, E.; Soler-Sala, G.; Sánchez-Payá, J.; López-Font, I.; Martínez, J.; Gómez-Escolar, L.; Sempere, L.; Sánchez-Fortún, C.; Pérez-Mateo, M. Influence of fluid therapy on the prognosis of acute pancreatitis: A prospective cohort study. Am. J. Gastroenterol. 2011, 106, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Basurto Ona, X.; Rigau Comas, D.; Urrútia, G. Opioids for acute pancreatitis pain. Cochrane Database Syst. Rev. 2013, 2013, 13–14. [Google Scholar] [CrossRef]
- Meng, W.; Yuan, J.; Zhang, C.; Bai, Z.; Zhou, W.; Yan, J.; Li, X. Parenteral analgesics for pain relief in acute pancreatitis: A systematic review. Pancreatology 2013, 13, 201–206. [Google Scholar] [CrossRef]
- Stigliano, S.; Sternby, H.; de Madaria, E.; Capurso, G.; Petrov, M.S. Early management of acute pancreatitis: A review of the best evidence. Dig. Liver Dis. 2017, 49, 585–594. [Google Scholar] [CrossRef]
- Sun, S.; Yang, K.; He, X.; Tian, J.; Ma, B.; Jiang, L. Probiotics in patients with severe acute pancreatitis: A meta-analysis. Langenbeck’s Arch. Surg. 2008, 394, 171–177. [Google Scholar] [CrossRef]
- Buter, A.; Imrie, C.W.; Carter, C.R.; Evans, S.; McKay, C.J. Dynamic nature of early organ dysfunction determines outcome in acute pancreatitis. British Journal of Surgery. 2002, 89, 298–302. [Google Scholar] [CrossRef]
- Nathens, A.B.; Curtis, J.R.; Beale, R.J.; Cook, D.J.; Moreno, R.P.; Romand, J.A.; Skerrett, S.J.; Stapleton, R.D.; Ware, L.B.; Waldmann, C.S. Management of the critically ill patient with severe acute pancreatitis. Crit. Care Med. 2004, 32, 2524–2536. [Google Scholar] [CrossRef]
- Zhao, X.; Huang, W.; Li, J.; Liu, Y.; Wan, M.; Xue, G.; Zhu, S.; Guo, H.; Xia, Q.; Tang, W. Noninvasive Positive-Pressure Ventilation in Acute Respiratory Distress Syndrome in Patients with Acute Pancreatitis: A Retrospective Cohort Study. Pancreas 2016, 45, 58–63. [Google Scholar] [CrossRef]
- Cordemans, C.; De Laet, I.; Van Regenmortel, N.; Schoonheydt, K.; Dits, H.; Huber, W.; Malbrain, M.L. Fluid management in critically ill patients: The role of extravascular lung water, Abdominal hypertension, Capillary leak, And fluid balance. Ann. Intensive Care 2012, 2, S1. [Google Scholar] [CrossRef]
- Komolafe, O.; Pereira, S.P.; Davidson, B.R.; Gurusamy, K.S. Serum C-reactive protein, procalcitonin, and lactate dehydrogenase for the diagnosis of pancreatic necrosis. Cochrane Database Syst. Rev. 2017, 2017, CD012645. [Google Scholar] [CrossRef]
- Li, S.; Zhang, Y.; Li, M.; Xie, C.; Wu, H. Serum albumin, a good indicator of persistent organ failure in acute pancreatitis. BMC Gastroenterol. 2017, 17, 59. [Google Scholar]
- Valverde-López, F.; Matas-Cobos, A.M.; Alegría-Motte, C.; Jiménez-Rosales, R.; Úbeda-Muñoz, M.; Redondo-Cerezo, E. BISAP, RANSON, lactate and others biomarkers in prediction of severe acute pancreatitis in a European cohort. J. Gastroenterol. Hepatol. 2017, 32, 1649–1656. [Google Scholar] [CrossRef]
- Zádori, N.; Párniczky, A.; Szentesi, A.; Hegyi, P. Insufficient implementation of the IAP/APA guidelines on aetiology in acute pancreatitis: Is there a need for implementation managers in pancreatology? United Eur. Gastroenterol. J. 2020, 8, 246–248. [Google Scholar] [CrossRef]
- Staubli, S.M.; Oertli, D.; Nebiker, C.A. Laboratory markers predicting severity of acute pancreatitis. Crit. Rev. Clin. Lab. Sci. 2015, 52, 273–283. [Google Scholar] [CrossRef]
- Koutroumpakis, E.; Wu, B.U.; Bakker, O.J.; Dudekula, A.; Singh, V.K.; Besselink, M.G.; Yadav, D.; van Santvoort, H.C.; Whitcomb, D.C.; Gooszen, H.G.; et al. Admission hematocrit and rise in blood urea nitrogen at 24 h outperform other laboratory markers in predicting persistent organ failure and pancreatic necrosis in acute pancreatitis: A post hoc analysis of three large prospective databases. Am. J. Gastroenterol. 2015, 110, 1707–1716. [Google Scholar] [CrossRef]
- Brown, A.; James-Stevenson, T.; Dyson, T.; Grunkenmeier, D. The Panc 3 score: A rapid and accurate test for predicting severity on presentation in acute pancreatitis. J. Clin. Gastroenterol. 2007, 41, 855–858. [Google Scholar] [CrossRef]
- Yang, C.J.; Chen, J.; Phillips, A.R.J.; Windsor, J.A.; Petrov, M.S. Predictors of severe and critical acute pancreatitis: A systematic review. Dig. Liver Dis. 2014, 46, 446–451. [Google Scholar] [CrossRef]
- Zeng, Y.B.; Zhan, X.B.; Guo, X.R.; Zhang, H.G.; Chen, Y.; Cai, Q.C.; Li, Z.S. Risk factors for pancreatic infection in patients with severe acute pancreatitis: An analysis of 163 cases. J. Dig. Dis. 2014, 15, 377–385. [Google Scholar] [CrossRef]
- Zhao, Z.; Yu, Y.; Xie, R.; Yang, K.; Xu, D.; Li, L.; Lin, J.; Zheng, L.; Zhang, C.; Xu, X.; et al. Prognostic value of the creatinine-albumin ratio in acute pancreatitis debridement. BMC Surg. 2020, 20, 322. [Google Scholar] [CrossRef]
- Lipinski, M.; Rydzewski, A.; Rydzewska, G. Early changes in serum creatinine level and estimated glomerular filtration rate predict pancreatic necrosis and mortality in acute pancreatitis Creatinine and eGFR in acute pancreatitis. Pancreatology 2013, 13, 207–211. [Google Scholar] [CrossRef]
- Abou-Assi, S.; O’Keefe, S.J. Nutrition support during acute pancreatitis. Nutrition 2002, 18, 938–943. [Google Scholar] [CrossRef]
- Yadav, D.; Agarwal, N.; Pitchumoni, C.S. A critical evaluation of laboratory tests in acute pancreatitis. Am. J. Gastroenterol. 2002, 97, 1309–1318. [Google Scholar] [CrossRef]
- Eckerwall, G.E.; Tingstedt, B.B.Å.; Bergenzaun, P.E.; Andersson, R.G. Immediate oral feeding in patients with mild acute pancreatitis is safe and may accelerate recovery-A randomized clinical study. Clin. Nutr. 2007, 26, 758–763. [Google Scholar] [CrossRef]
- Petrov, M.S.; Pylypchuk, R.D.; Uchugina, A.F. A systematic review on the timing of artificial nutrition in acute pancreatitis. Br. J. Nutr. 2009, 101, 787–793. [Google Scholar] [CrossRef]
- Jacobson, B.C.; vander Vliet, M.B.; Hughes, M.D.; Maurer, R.; McManus, K.; Banks, P.A. A Prospective, Randomized Trial of Clear Liquids Versus Low-Fat Solid Diet as the Initial Meal in Mild Acute Pancreatitis. Clin. Gastroenterol. Hepatol. 2007, 5, 946–951. [Google Scholar] [CrossRef]
- Sathiaraj, E.; Murthy, S.; Mansard, M.J.; Rao, G.V.; Mahukar, S.; Reddy, D.N. Clinical trial: Oral feeding with a soft diet compared with clear liquid diet as initial meal in mild acute pancreatitis. Aliment. Pharmacol. Ther. 2008, 28, 777–781. [Google Scholar] [CrossRef]
- Moraes, J.M.M.; Felga, G.E.G.; Chebli, L.A.; Franco, M.B.; Gomes, C.A.; Gaburri, P.D.; Zanini, A.; Chebli, J.M.F. A full solid diet as the initial meal in mild acute pancreatitis is safe and result in a shorter length of hospitalization: Results from a prospective, randomized, controlled, double-blind clinical trial. J. Clin. Gastroenterol. 2010, 44, 517–522. [Google Scholar] [CrossRef]
- Kalfarentzos, F.; Kehagias, J.; Mead, N.; Kokkinis, K.; Gogos, C.A. Enteral nutrition is superior to parenteral nutrition in severe acute pancreatitis: Results of a randomized prospective trial. Br. J. Surg. 1997, 84, 1665–1669. [Google Scholar] [CrossRef]
- Petrov, M.S.; van Santvoort, H.C.; Besselink, M.G.H.; van der Heijden, G.J.M.G.; Windsor, J.A.; Gooszen, H.G. Enteral nutrition and the risk of mortality and infectious complications in patients with severe acute pancreatitis: A meta-analysis of randomized trials. Arch. Surg. 2008, 143, 1111–1117. [Google Scholar] [CrossRef]
- Gupta, R.; Patel, K.; Calder, P.C.; Yaqoob, P.; Primrose, J.N.; Johnson, C.D. A randomised clinical trial to assess the effect of total enteral and total parenteral nutritional support on metabolic, inflammatory and oxidative markers in patients with predicted severe acute pancreatitis (APACHE II ≥ 6). Pancreatology 2003, 3, 406–413. [Google Scholar] [CrossRef]
- Petrov, M.S.; Correia, M.I.T.D.; Windsor, J.A. Nasogastric tube feeding in predicted severe acute pancreatitis. A systematic review of the literature to determine safety and tolerance. J. Pancreas 2008, 9, 440–448. [Google Scholar]
- Chang, Y.S.; Fu, H.Q.; Xiao, Y.M.; Liu, J.C. Nasogastric or nasojejunal feeding in predicted severe acute pancreatitis: A meta-analysis. Crit. Care 2013, 17, R118. [Google Scholar] [CrossRef]
- Petrov, M.S.; Loveday, B.P.T.; Pylypchuk, R.D.; McIlroy, K.; Phillips, A.R.J.; Windsor, J.A. Systematic review and meta-analysis of enteral nutrition formulations in acute pancreatitis. Br. J. Surg. 2009, 96, 1243–1252. [Google Scholar] [CrossRef]
- Büchler, M.; Malfertheiner, P.; Uhl, W.; Schölmerich, J.; Stöckmann, F.; Adler, G.; Gaus, W.; Rolle, K.; Beger, H.G.; German Pancreatitis Study Group. Gabexate mesilate in human acute pancreatitis. German Pancreatitis Study Group. Gastroenterology 1993, 104, 1165–1170. [Google Scholar] [CrossRef]
- Johnson, C.D.; Kingsnorth, A.N.; Imrie, C.W.; McMahon, M.J.; Neoptolemos, J.P.; McKay, C.; Toh, S.K.C.; Skaife, P.; Leeder, P.C.; Wilson, P.; et al. Double blind, randomised, placebo controlled study of a platelet activating factor antagonist, lexipafant, in the treatment and prevention of organ failure in predicted severe acute pancreatitis. Gut 2001, 48, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Vissers, R.J.; Abu-Laban, R.B.; McHugh, D.F. Amylase and lipase in the emergency department evaluation of acute pancreatitis. J. Emerg. Med. 1999, 17, 1027–1037. [Google Scholar] [CrossRef]
- Reuken, P.A.; Albig, H.; Rödel, J.; Hocke, M.; Will, U.; Stallmach, A.; Bruns, T. Fungal Infections in Patients with Infected Pancreatic Necrosis and Pseudocysts: Risk Factors and Outcome. Pancreas 2018, 47, 92–98. [Google Scholar] [CrossRef]
- Büchler, M.; Malfertheiner, P.; Frieβ, H.; Isenmann, R.; Vanek, E.; Grimm, H.; Schlegel, P.; Friess, T.; Beger, H.G. Human pancreatic tissue concentration of bactericidal antibiotics. Gastroenterology 1992, 103, 1902–1908. [Google Scholar] [CrossRef]
- Otto, W.; Komorzycki, K.; Krawczyk, M. Efficacy of antibiotic penetration into pancreatic necrosis. HPB 2006, 8, 43–48. [Google Scholar] [CrossRef]
- Schubert, S.; Dalhoff, A. Activity of moxifloxacin, imipenem, and ertapenem against Escherichia coli, Enterobacter cloacae, Enterococcus faecalis, and Bacteroides fragilis in monocultures and mixed cultures in an in vitro pharmacokinetic/pharmacodynamic model simulating concentrations in the human pancreas. Antimicrob. Agents Chemother. 2012, 56, 6434–6436. [Google Scholar] [PubMed]
- Schwender, B.J.; Gordon, S.R.; Gardner, T.B. Risk Factors for the Development of Intra-Abdominal Fungal Infections in Acute Pancreatitis. Pancreas 2015, 44, 805. [Google Scholar] [CrossRef]
- Mowery, N.T.; Bruns, B.R.; MacNew, H.G.; Agarwal, S.; Enniss, T.M.; Khan, M.; Guo, W.A.; Cannon, J.W.; Lissauer, M.E.; Duane, T.M.; et al. Surgical management of pancreatic necrosis: A practice management guideline from the Eastern Association for the Surgery of Trauma. J. Trauma Acute Care Surg. 2017, 83, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.K.; Adler, G. From acinar cell damage to systemic inflammatory response: Current concepts in pancreatitis. Pancreatology 2001, 1, 356–362. [Google Scholar] [CrossRef]
- Dervenis, C.; Johnson, C.D.; Bassi, C.A.; Bradley, E.; Imrie, C.W.; McMahon, M.J.; Modlin, I. Diagnosis, objective assessment of severity, and management of acute pancreatitis: Santorini consensus conference. Int. J. Pancreatol. 1999, 25, 195–210. [Google Scholar] [CrossRef]
- Umehara, H.; Okazaki, K.; Kawa, S.; Takahashi, H.; Goto, H.; Matsui, S.; Ishizaka, N.; Akamizu, T.; Sato, Y.; Kawano, M. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod. Rheumatol. 2021, 31, 529–533. [Google Scholar] [CrossRef]
- Uchida, K.; Okazaki, K. Clinical and pathophysiological aspects of type 1 autoimmune pancreatitis. J. Gastroenterol. 2018, 53, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Márta, K.; Gede, N.; Szakács, Z.; Solymár, M.; Hegyi, P.J.; Tél, B.; Erőss, B.; Vincze; Arvanitakis, M.; Boškoski, I.; et al. Combined use of indomethacin and hydration is the best conservative approach for post-ERCP pancreatitis prevention: A network meta-analysis. Pancreatology 2021, 21, 1247–1255. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severity of Acute Pancreatitis | Characteristics |
|---|---|
| Mild acute pancreatitis | The most frequent form No organ failure No local or systemic complications Usually resolves in the first week |
| Moderately severe acute pancreatitis | Transient organ failure resolving within 48 h Local or systemic complications without persistent organ failure Exacerbation of co-morbid disease |
| Severe acute pancreatitis | Persistent organ failure > 48 h |
| Criterion of Acute Pancreatitis | Characteristics |
| Organ failure and systemic complications of acute pancreatitis | Respiratory System: Pao2/FiO2 ≤ 300 Cardiovascular System: systolic blood pressure < 90 mm Hg (off inotropic support) not fluid responsive or pH < 7.3 Urinary System: serum creatinine ≥ 170 μmol/L |
| Local complications of acute pancreatitis | Acute peripancreatic fluid collections Pancreatic and peripancreatic necrosis (sterile or infected) Pancreatic pseudocyst Walled-off pancreatic necrosis (sterile or infected) |
| Assay | Serum Lipase | Serum Amylase |
|---|---|---|
| Origin of the enzyme | Pancreas [14] | Pancreas, salivary glands, small intestine, ovaries, adipose tissue, skeletal muscle [14] |
| The normal range of the enzyme | 5-208 U/L [18] | 30-110 U/L [18] |
| The dynamics of enzyme level |
|
|
| A common threshold | Three times the normal limit [1] | Three times the normal limit [1] |
| Radiological Test | Advantages | Limitations | |
|---|---|---|---|
| US |
|
| |
| EUS |
| ||
| MRI |
|
| |
| CT |
|
| |
| Grade, Points | Characteristics |
|---|---|
| Grade A, 0 points | Normal pancreas. |
| Grade B, 1 point | Focal or diffuse enlargement of the pancreas (including contour irregularities, non-homogenous attenuation of the gland, dilation of the pancreatic duct, and foci of small fluid collections within the gland, as long as there was no evidence of peri-pancreatic disease. |
| Grade C, 2 points | Intrinsic pancreatic abnormalities associated with hazy streaky densities representing inflammatory changes in the peri-pancreatic fat. |
| Grade D, 3 points | Single ill-defined fluid collection (phlegmon). |
| Grade E, 4 points | Two or multiple poorly defined fluid collections or presence of gas in or adjacent to the pancreas. |
| The presence and extent of necrosis | Points |
| Necrosis absent | 0 points |
| < 30% necrosis | 2 points |
| 30–50% necrosis | 4 points |
| >50% necrosis | 6 points |
| Severity of AP | CTSI score |
| Mild pancreatitis | 0–3 |
| Moderate pancreatitis | 4–6 |
| Severe pancreatitis | 7–10 |
| Points | Characteristics |
|---|---|
| 0 points | Normal pancreas |
| 2 points | Intrinsic pancreatic abnormalities with or without inflammatory changes in peripancreatic fat. |
| 4 points | Pancreatic or peripancreatic fluid collection or peripancreatic fat necrosis. |
| The presence and extent of necrosis | Points |
| Necrosis absent | 0 points |
| <30% necrosis | 2 points |
| >30% necrosis | 4 points |
| Severity of AP | Modified CTSI score |
| Mild pancreatitis | 0–2 |
| Moderate pancreatitis | 4–6 |
| Severe pancreatitis | 8–10 |
| Impaired Organ | Symptoms |
|---|---|
| Respiratory |
|
| Cardiovascular |
|
| Renal |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walkowska, J.; Zielinska, N.; Tubbs, R.S.; Podgórski, M.; Dłubek-Ruxer, J.; Olewnik, Ł. Diagnosis and Treatment of Acute Pancreatitis. Diagnostics 2022, 12, 1974. https://doi.org/10.3390/diagnostics12081974
Walkowska J, Zielinska N, Tubbs RS, Podgórski M, Dłubek-Ruxer J, Olewnik Ł. Diagnosis and Treatment of Acute Pancreatitis. Diagnostics. 2022; 12(8):1974. https://doi.org/10.3390/diagnostics12081974
Chicago/Turabian StyleWalkowska, Julia, Nicol Zielinska, R. Shane Tubbs, Michał Podgórski, Justyna Dłubek-Ruxer, and Łukasz Olewnik. 2022. "Diagnosis and Treatment of Acute Pancreatitis" Diagnostics 12, no. 8: 1974. https://doi.org/10.3390/diagnostics12081974