
Criteria for Diagnosis of Polycystic Ovary Syndrome during Adolescence: Literature Review


Abstract
:1. Introduction
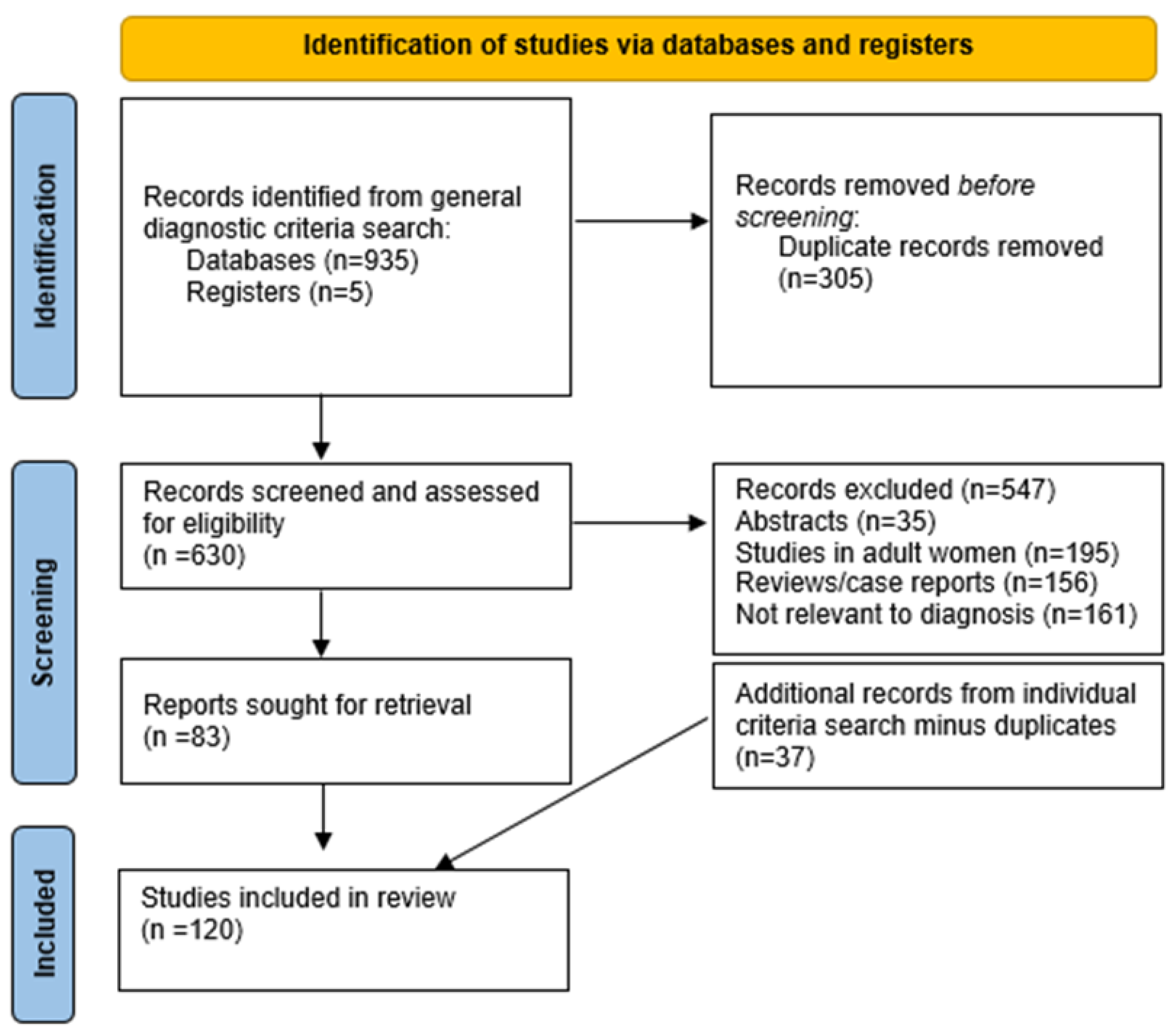
2. Search Strategy
3. Main Criteria to Diagnose PCOS during Adolescence
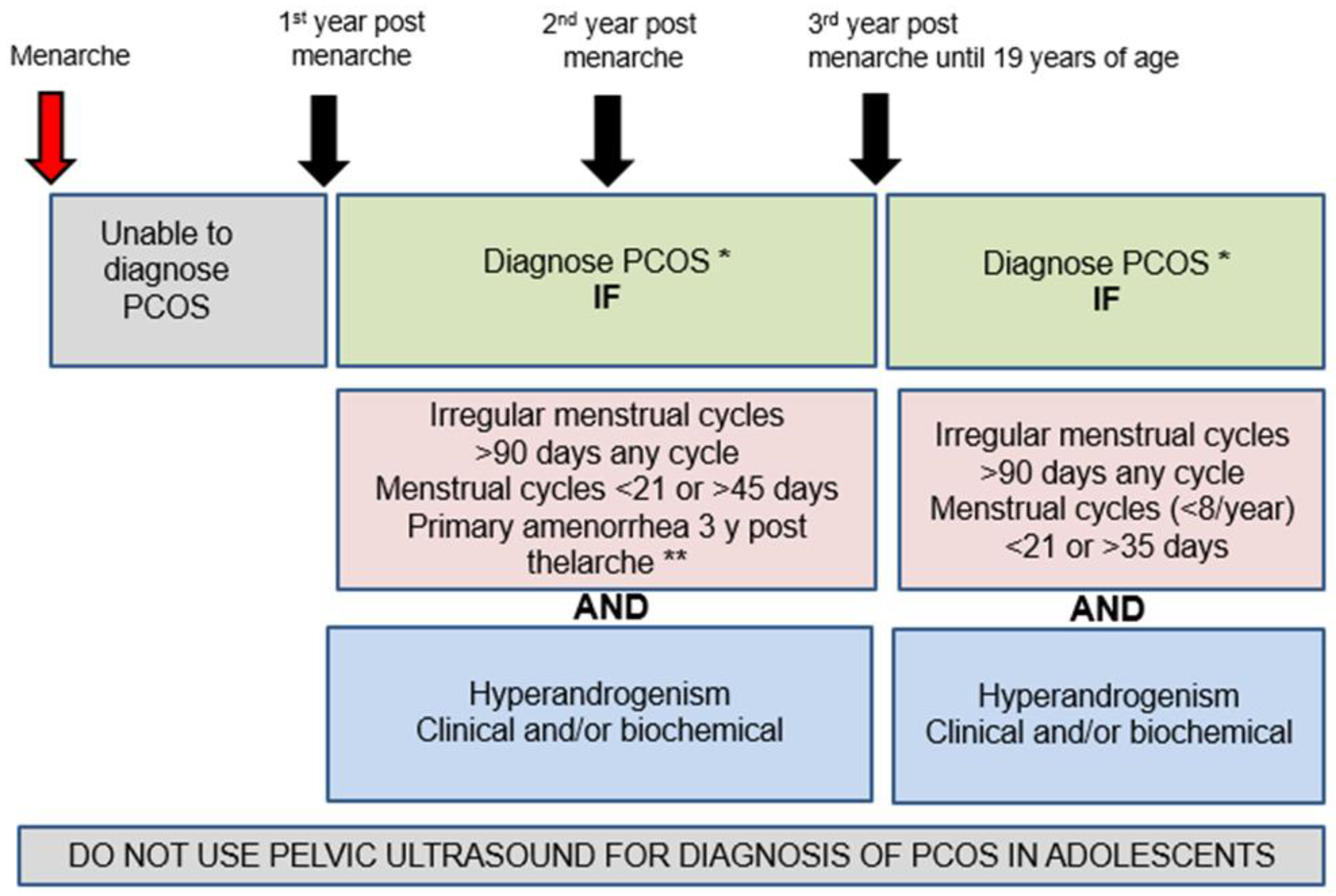
3.1. Menstrual Cycle Irregularity and Ovulatory Dysfunction
3.2. Hyperandrogenism
3.3. Other Investigations and/or Features Not Part of the Diagnostic Criteria
3.3.1. Pelvic Ultrasound to Evaluate PCOM
3.3.2. Anti-Müllerian Hormone (AMH)
3.3.3. Insulin Resistance
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategies for Diagnosis as Run 4 March 2022
- Database: Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily <1946 to 2 March 2022>
- Polycystic ovary syndrome/ 16279
- polycystic ovar*.mp. 21744
- poly-cystic ovar*.mp. 51
- (PCOS or PCOD).mp. 13672
- (stein-leventhal or leventhal).mp. 911
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 21864
- or/1-6 22558
- Young Adult/ 981588
- Adolescent/ 2161302
- 1Child/ 1819791
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1120473
- or/8-11 3870344
- *Diagnosis/ 13392
- Missed Diagnosis/ 258
- Delayed Diagnosis/ 7701
- Diagnostic Errors/ 39204
- diagnos*.ti,kf. 738538
- (diagnos* adj6 controver*).ab. 3416
- (diagnos* adj6 dilemma*).ab. 5049
- (diagnos* adj6 experience*).ab. 14386
- (diagnos* adj6 dissatisf*).ab. 150
- (diagnos* adj6 satisf*).ab. 3611
- (diagnos* adj6 challeng*).ab. 40293
- (diagnos* adj2 miss*).ab. 4865
- (diagnos* adj2 delay*).ab. 24809
- misdiagnos*.ti,ab,kf. 38867
- or/13-26 863236
- 7 and 12 and 27 377
- limit 28 to english language 326
- Database: Embase <1974 to 2 March 2022>
- ovary polycystic disease/ 31017
- polycystic ovar*.mp. 27051
- poly-cystic ovar*.mp. 185
- (PCOS or PCOD).mp. 20618
- (stein-leventhal or leventhal).mp. 605
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 34194
- or/1-6 36308
- young adult/ 448275
- adolescent/ 1651934
- child/ 1907656
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1512100
- or/8-11 3624844
- *diagnosis/ 62017
- missed diagnosis/ 928
- delayed diagnosis/ 15408
- diagnostic error/ 64671
- diagnos*.ti,kf. 861099
- (diagnos* adj6 controver*).ab. 4754
- (diagnos* adj6 dilemma*).ab. 7606
- (diagnos* adj6 experience*).ab. 22581
- (diagnos* adj6 dissatisf*).ab. 227
- (diagnos* adj6 satisf*).ab. 5542
- (diagnos* adj6 challeng*).ab. 62196
- (diagnos* adj2 miss*).ab. 7740
- (diagnos* adj2 delay*).ab. 39406
- misdiagnos*.ti,ab,kf. 55961
- or/13-26 1055751
- 7 and 12 and 27 513
- limit 28 to english language 454
- Database: EBM Reviews-Cochrane Central Register of Controlled Trials <January 2022>
- Polycystic ovary syndrome/ 1649
- polycystic ovar*.mp. 4330
- poly-cystic ovar*.mp. 125
- (PCOS or PCOD).mp. 3508
- (stein-leventhal or leventhal).mp. 57
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 4491
- or/1-6 4858
- Young Adult/ 73866
- Adolescent/ 110345
- Child/ 52129
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 125810
- or/8-11 262647
- Diagnosis/ 69
- Missed Diagnosis/ 9
- Delayed Diagnosis/ 28
- Diagnostic Errors/ 286
- diagnos*.ti,kw. 64022
- (diagnos* adj6 controver*).ab. 189
- (diagnos* adj6 dilemma*).ab. 59
- (diagnos* adj6 experience*).ab. 1344
- (diagnos* adj6 dissatisf*).ab. 14
- (diagnos* adj6 satisf*).ab. 775
- (diagnos* adj6 challeng*).ab. 1224
- (diagnos* adj2 miss*).ab. 300
- (diagnos* adj2 delay*).ab. 746
- misdiagnos*.ti,ab,kw. 599
- or/13-26 67044
- 7 and 12 and 27 51
- limit 28 to english language 48
- Database: EBM Reviews-Cochrane Database of Systematic Reviews <2005 to 2 March 2022>
- polycystic ovar*.mp. 149
- poly-cystic ovar*.mp. 0
- (PCOS or PCOD).mp. 84
- (stein-leventhal or leventhal).mp. 39
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 150
- or/1-5 174
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or paediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1241
- diagnos*.ti,kw. 629
- (diagnos* adj6 controver*).ab. 1
- (diagnos* adj6 dilemma*).ab. 0
- (diagnos* adj6 experience*).ab. 15
- (diagnos* adj6 dissatisf*).ab. 0
- (diagnos* adj6 satisf*).ab. 1
- (diagnos* adj6 challeng*).ab. 11
- (diagnos* adj2 miss*).ab. 1
- (diagnos* adj2 delay*).ab. 10
- misdiagnos*.ti,ab,kw. 6
- or/8-17 648
- 6 and 7 and 18 0
- Database: CINAHL Plus with Full Text
- (MH “Polycystic Ovary Syndrome”) 4,429
- polycystic ovar* 5,698
- poly-cystic ovar* 26
- PCOS or PCOD 4,958
- “stein-leventhal” or Leventhal 1,267
- ovar* N6 (sclerocystic or polycystic or poly-cystic) 5,705
- S1 OR S2 OR S3 OR S4 OR S5 OR S6 7,733
- (MH “Adolescence+”) 575,454
- (MH “Child”) 503,695
- adolescen* or teen* or child* or school-age* or schoolage* or youth* or juvenile* or pediatric* or paediatric* or girl* 1,294,856
- S8 OR S9 OR S10 1,294,856
- (MM “Diagnosis”) 4,700
- (MH “Failure to Diagnose”) 1,465
- (MH “Diagnosis, Delayed”) 4,904
- (MH “Diagnostic Errors”) 12,392
- TI diagnos* 137,514
- AB diagnos* N7 controver* OR AB diagnos* N7 dilemma* OR AB diagnos* N7 experience* OR AB diagnos* N7 dissatisf* OR AB diagnos* N7 satisf* OR AB diagnos* N7 challeng* OR AB diagnos* N7 miss* OR AB diagnos* N7 delay* OR TI misdiagnos* OR AB misdiagnos* 42,186
- S12 OR S13 OR S14 OR S15 OR S16 OR S17 184,345
- S7 AND S11 AND S18 108
- S7 AND S11 AND S18 Limiters-English Language 107
- Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily <1946 to 13 May 2022>
- 1.
- Polycystic ovary syndrome/ 16686
- 2.
- polycystic ovar*.mp. 22098
- 3.
- poly-cystic ovar*.mp. 52
- 4.
- (PCOS or PCOD).mp. 13942
- 5.
- (stein-leventhal or leventhal).mp. 912
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 22219
- 7.
- or/1-6 22911
- 8.
- Young Adult/ 990846
- 9.
- Adolescent/ 2175898
- 10.
- Child/ 1841609
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kf. 1140005
- 12.
- or/8-11 3904962
- 13.
- Diagnosis/ 17514
- 14.
- Diagnosis, Differential/ 465318
- 15.
- Missed Diagnosis/ 280
- 16.
- Delayed Diagnosis/ 7853
- 17.
- Diagnostic Errors/ 39330
- 18.
- diagnos*.ti,kf. 746831
- 19.
- clinical diagnosis.ab. 48824
- 20.
- differential diagnosis.ab. 103778
- 21.
- (diagnos* adj3 criteria).ab. 63792
- 22.
- (diagnos* adj6 controver*).ab. 3445
- 23.
- (diagnos* adj6 dilemma*).ab. 5122
- 24.
- (diagnos* adj6 experience*).ab. 14665
- 25.
- (diagnos* adj6 dissatisf*).ab. 151
- 26.
- (diagnos* adj6 satisf*).ab. 3659
- 27.
- (diagnos* adj6 challeng*).ab. 41398
- 28.
- (diagnos* adj2 miss*).ab. 4989
- 29.
- (diagnos* adj2 delay*).ab. 25305
- 30.
- undiagnos*.ti,ab,kf. 22874
- 31.
- or/13-30 1348101
- 32.
- Menstrual Cycle/ 13873
- 33.
- Menstruation Disturbances/ 7386
- 34.
- Amenorrhea/ 10053
- 35.
- Oligomenorrhea/ 741
- 36.
- (menstru* or menses or period*).ti,ab,kf. 1913338
- 37.
- (amenorrhea or amenorrhoea).ti,ab,kf. 14826
- 38.
- (oligomenorrhea or oligomenorrhoea).ti,ab,kf. 1399
- 39.
- or/32-38 1932211
- 40.
- 7 and 12 and 31 and 39 311
- 41.
- limit 40 to (english or spanish) 274
- Embase <1974 to 13 May 2022>
- 1.
- ovary polycystic disease/ 31705
- 2.
- polycystic ovar*.mp. 27648
- 3.
- poly-cystic ovar*.mp. 189
- 4.
- (PCOS or PCOD).mp. 21164
- 5.
- (stein-leventhal or leventhal).mp. 607
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 34931
- 7.
- or/1-6 37109
- 8.
- young adult/ 457981
- 9.
- adolescent/ 1668346
- 10.
- child/ 1930245
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1531909
- 12.
- or/8-11 3666415
- 13.
- diagnosis/ 1370526
- 14.
- differential diagnosis/ 356015
- 15.
- missed diagnosis/ 991
- 16.
- delayed diagnosis/ 15697
- 17.
- diagnostic error/ 65252
- 18.
- diagnos*.ti,kf. 871654
- 19.
- clinical diagnosis.ab. 72479
- 20.
- differential diagnosis.ab. 150575
- 21.
- (diagnos* adj3 criteria).ab. 103665
- 22.
- (diagnos* adj6 controver*).ab. 4794
- 23.
- (diagnos* adj6 dilemma*).ab. 7711
- 24.
- (diagnos* adj6 experience*).ab. 22955
- 25.
- (diagnos* adj6 dissatisf*).ab. 229
- 26.
- (diagnos* adj6 satisf*).ab. 5604
- 27.
- (diagnos* adj6 challeng*).ab. 63546
- 28.
- (diagnos* adj2 miss*).ab. 7918
- 29.
- (diagnos* adj2 delay*).ab. 40023
- 30.
- undiagnos*.ti,ab,kf. 35267
- 31.
- or/13-30 2596598
- 32.
- menstrual cycle/ 38625
- 33.
- menstruation/ 20937
- 34.
- exp menstruation disorder/ 69557
- 35.
- (menstru* or menses or period*).ti,ab,kf. 2625182
- 36.
- (amenorrhea or amenorrhoea).ti,ab,kf. 18642
- 37.
- (oligomenorrhea or oligomenorrhoea).ti,ab,kf. 2181
- 38.
- or/32-37 2687373
- 39.
- 7 and 12 and 31 and 38 656
- 40.
- limit 39 to (english or spanish) 606
- EBM Reviews-Cochrane Central Register of Controlled Trials <April 2022>
- 1.
- Polycystic ovary syndrome/ 1679
- 2.
- polycystic ovar*.mp. 4297
- 3.
- poly-cystic ovar*.mp. 132
- 4.
- (PCOS or PCOD).mp. 3496
- 5.
- (stein-leventhal or leventhal).mp. 57
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 4464
- 7.
- or/1-6 4827
- 8.
- Young Adult/ 74694
- 9.
- Adolescent/ 111127
- 10.
- Child/ 52868
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 125587
- 12.
- or/8-11 263322
- 13.
- Diagnosis/ 68
- 14.
- Diagnosis, Differential/ 1490
- 15.
- Missed Diagnosis/ 11
- 16.
- Delayed Diagnosis/ 28
- 17.
- Diagnostic Errors/ 288
- 18.
- diagnos*.ti,kw. 65057
- 19.
- clinical diagnosis.ab. 5116
- 20.
- differential diagnosis.ab. 788
- 21.
- (diagnos* adj3 criteria).ab. 16717
- 22.
- (diagnos* adj6 controver*).ab. 105
- 23.
- (diagnos* adj6 dilemma*).ab. 45
- 24.
- (diagnos* adj6 experience*).ab. 760
- 25.
- (diagnos* adj6 dissatisf*).ab. 6
- 26.
- (diagnos* adj6 satisf*).ab. 474
- 27.
- (diagnos* adj6 challeng*).ab. 806
- 28.
- (diagnos* adj2 miss*).ab. 204
- 29.
- (diagnos* adj2 delay*).ab. 560
- 30.
- undiagnos*.ti,ab,kw. 1143
- 31.
- or/13-30 87378
- 32.
- Menstrual Cycle/ 869
- 33.
- Menstruation Disturbances/ 235
- 34.
- Amenorrhea/ 343
- 35.
- Oligomenorrhea/ 46
- 36.
- (menstru* or menses or period*).ti,ab,kw. 281778
- 37.
- (amenorrhea or amenorrhoea).ti,ab,kw. 2311
- 38.
- (oligomenorrhea or oligomenorrhoea).ti,ab,kw. 361
- 39.
- or/32-38 283399
- 40.
- 7 and 12 and 31 and 39 30
- 41.
- limit 40 to (english or spanish) 29
- EBM Reviews-Cochrane Database of Systematic Reviews <2005 to 11 May 2022>
- 1.
- polycystic ovar*.mp. 149
- 2.
- poly-cystic ovar*.mp. 0
- 3.
- (PCOS or PCOD).mp. 84
- 4.
- (stein-leventhal or leventhal).mp. 39
- 5.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 150
- 6.
- or/1-5 174
- 7.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1253
- 8.
- diagnos*.ti,ab,kw. 1727
- 9.
- undiagnos*.ti,ab,kw. 16
- 10.
- or/8-9 1731
- 11.
- (menstru* or menses or period*).ti,ab,kw. 1345
- 12.
- (amenorrhea or amenorrhoea).ti,ab,kw. 44
- 13.
- (oligomenorrhea or oligomenorrhoea).ti,ab,kw. 2
- 14.
- or/11-13 1353
- 15.
- 6 and 7 and 10 and 14 3
- Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily <1946 to 13 May 2022>
- 1.
- Polycystic ovary syndrome/ 16686
- 2.
- polycystic ovar*.mp. 22098
- 3.
- poly-cystic ovar*.mp. 52
- 4.
- (PCOS or PCOD).mp. 13942
- 5.
- (stein-leventhal or leventhal).mp. 912
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 22219
- 7.
- or/1-6 22911
- 8.
- Young Adult/ 990846
- 9.
- Adolescent/ 2175898
- 10.
- Child/ 1841609
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kf. 1140005
- 12.
- or/8-11 3904962
- 13.
- Diagnosis/ 17514
- 14.
- Diagnostic Techniques, Endocrine/ 1071
- 15.
- Biomarkers/ 329596
- 16.
- Diagnosis, Differential/ 465318
- 17.
- Missed Diagnosis/ 280
- 18.
- Delayed Diagnosis/ 7853
- 19.
- Diagnostic Errors/ 39330
- 20.
- diagnos*.ti,kf. 746831
- 21.
- (biomarker* or marker*).ti,ab,kf. 1148168
- 22.
- clinical diagnosis.ab. 48824
- 23.
- differential diagnosis.ab. 103778
- 24.
- diagnostic definition*.ab. 312
- 25.
- (diagnos* adj3 criteria).ab. 63792
- 26.
- (diagnos* adj6 controver*).ab. 3445
- 27.
- (diagnos* adj6 dilemma*).ab. 5122
- 28.
- (diagnos* adj6 experience*).ab. 14665
- 29.
- (diagnos* adj6 dissatisf*).ab. 151
- 30.
- (diagnos* adj6 satisf*).ab. 3659
- 31.
- (diagnos* adj6 challeng*).ab. 41398
- 32.
- (diagnos* adj2 miss*).ab. 4989
- 33.
- (diagnos* adj2 delay*).ab. 25305
- 34.
- undiagnos*.ti,ab,kf. 22874
- 35.
- or/13-34 2541274
- 36.
- Hyperandrogenism/ 2277
- 37.
- exp Dehydroepiandrosterone/ 11984
- 38.
- hyperandrogen*.ti,ab,kf. 6042
- 39.
- ((androgen or testosterone) adj2 (increas* or elevate* or raise* or high*)).ti,ab,kf. 10782
- 40.
- Hirsutism/ 4159
- 41.
- hirsutism.ti,kf. 1908
- 42.
- Acne Vulgaris/ 12765
- 43.
- (acne adj2 (severe or vulgaris)).ti,kf. 3481
- 44.
- Alopecia/ 12264
- 45.
- alopecia.ti,kf. 10073
- 46.
- or/36-45 59877
- 47.
- 7 and 12 and 35 and 46 638
- 48.
- limit 47 to (english or spanish) 597
- Embase <1974 to 13 May 2022>
- 1.
- ovary polycystic disease/ 31705
- 2.
- polycystic ovar*.mp. 27648
- 3.
- poly-cystic ovar*.mp. 189
- 4.
- (PCOS or PCOD).mp. 21164
- 5.
- (stein-leventhal or leventhal).mp. 607
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 34931
- 7.
- or/1-6 37109
- 8.
- young adult/ 457981
- 9.
- adolescent/ 1668346
- 10.
- child/ 1930245
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1531909
- 12.
- or/8-11 3666415
- 13.
- diagnosis/ 1370526
- 14.
- endocrine system examination/ 545
- 15.
- biological marker/ 381458
- 16.
- differential diagnosis/ 356015
- 17.
- missed diagnosis/ 991
- 18.
- delayed diagnosis/ 15697
- 19.
- diagnostic error/ 65252
- 20.
- diagnos*.ti,kf. 871654
- 21.
- (biomarker* or marker*).ti,ab,kf. 1654043
- 22.
- clinical diagnosis.ab. 72479
- 23.
- differential diagnosis.ab. 150575
- 24.
- (diagnos* adj3 criteria).ab. 103665
- 25.
- (diagnos* adj6 controver*).ab. 4794
- 26.
- (diagnos* adj6 dilemma*).ab. 7711
- 27.
- (diagnos* adj6 experience*).ab. 22955
- 28.
- (diagnos* adj6 dissatisf*).ab. 229
- 29.
- (diagnos* adj6 satisf*).ab. 5604
- 30.
- (diagnos* adj6 challeng*).ab. 63546
- 31.
- (diagnos* adj2 miss*).ab. 7918
- 32.
- (diagnos* adj2 delay*).ab. 40023
- 33.
- undiagnos*.ti,ab,kf. 35267
- 34.
- or/13-33 4124534
- 35.
- hyperandrogenism/ 8276
- 36.
- prasterone/ 15819
- 37.
- hyperandrogen*.ti,ab,kf. 9102
- 38.
- ((androgen or testosterone) adj2 (increas* or elevate* or raise* or high*)).ti,ab,kf. 13861
- 39.
- hirsutism/ 12014
- 40.
- hirsutism.ti,kf. 2388
- 41.
- acne vulgaris/ 11465
- 42.
- (acne adj2 (severe or vulgaris)).ti,kf. 4583
- 43.
- Alopecia/ 45479
- 44.
- alopecia.ti,kf. 12487
- 45.
- or/35-44 109088
- 46.
- 7 and 12 and 34 and 45 900
- 47.
- limit 46 to (english or spanish) 845
- EBM Reviews-Cochrane Central Register of Controlled Trials <April 2022>
- 1.
- Polycystic ovary syndrome/ 1679
- 2.
- polycystic ovar*.mp. 4297
- 3.
- poly-cystic ovar*.mp. 132
- 4.
- (PCOS or PCOD).mp. 3496
- 5.
- (stein-leventhal or leventhal).mp. 57
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 4464
- 7.
- or/1-6 4827
- 8.
- Young Adult/ 74694
- 9.
- Adolescent/ 111127
- 10.
- Child/ 52868
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 125587
- 12.
- or/8-11 263322
- 13.
- Diagnosis/ 68
- 14.
- Diagnostic Techniques, Endocrine/ 47
- 15.
- Biomarkers/ 15881
- 16.
- Diagnosis, Differential/ 1490
- 17.
- Missed Diagnosis/ 11
- 18.
- Delayed Diagnosis/ 28
- 19.
- Diagnostic Errors/ 288
- 20.
- diagnos*.ti,kw. 65057
- 21.
- (biomarker* or marker*).ti,ab,kw. 84953
- 22.
- clinical diagnosis.ab. 5116
- 23.
- differential diagnosis.ab. 788
- 24.
- diagnostic definition*.ab. 9
- 25.
- (diagnos* adj3 criteria).ab. 16717
- 26.
- (diagnos* adj6 controver*).ab. 105
- 27.
- (diagnos* adj6 dilemma*).ab. 45
- 28.
- (diagnos* adj6 experience*).ab. 760
- 29.
- (diagnos* adj6 dissatisf*).ab. 6
- 30.
- (diagnos* adj6 satisf*).ab. 474
- 31.
- (diagnos* adj6 challeng*).ab. 806
- 32.
- (diagnos* adj2 miss*).ab. 204
- 33.
- (diagnos* adj2 delay*).ab. 560
- 34.
- undiagnos*.ti,ab,kw. 1143
- 35.
- or/13-34 172054
- 36.
- Hyperandrogenism/ 146
- 37.
- exp Dehydroepiandrosterone/ 694
- 38.
- hyperandrogen*.ti,ab,kw. 859
- 39.
- ((androgen or testosterone) adj2 (increas* or elevate* or raise* or high*)).ti,ab,kw. 1044
- 40.
- Hirsutism/ 204
- 41.
- hirsutism.ti,kw. 449
- 42.
- Acne Vulgaris/ 1473
- 43.
- (acne adj2 (severe or vulgaris)).ti,kw. 1985
- 44.
- Alopecia/ 630
- 45.
- alopecia.ti,kw. 2918
- 46.
- or/36-45 8608
- 47.
- 7 and 12 and 35 and 46 65
- 48.
- limit 47 to (english or spanish) 62
- EBM Reviews-Cochrane Database of Systematic Reviews <2005 to 11 May 2022>
- 1.
- polycystic ovar*.mp. 149
- 2.
- poly-cystic ovar*.mp. 0
- 3.
- (PCOS or PCOD).mp. 84
- 4.
- (stein-leventhal or leventhal).mp. 39
- 5.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 150
- 6.
- or/1-5 174
- 7.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1253
- 8.
- diagnos*.ti,ab,kw. 1727
- 9.
- undiagnos*.ti,ab,kw. 16
- 10.
- or/8-9 1731
- 11.
- hyperandrogen*.ti,ab,kw. 6
- 12.
- ((androgen or testosterone) adj2 (increas* or elevate* or raise* or high*)).ti,ab,kw. 1
- 13.
- hirsutism.ti,kw. 8
- 14.
- (acne adj2 (severe or vulgaris)).ti,kw. 14
- 15.
- alopecia.ti,kw. 6
- 16.
- or/11-14 22
- 17.
- 6 and 7 and 10 and 16 1
- Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily <1946 to 22 March 2022>
- 1.
- Polycystic ovary syndrome/ 16385
- 2.
- polycystic ovar*.mp. 21847
- 3.
- poly-cystic ovar*.mp. 52
- 4.
- (PCOS or PCOD).mp. 13742
- 5.
- (stein-leventhal or leventhal).mp. 911
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 21969
- 7.
- or/1-6 22659
- 8.
- Young Adult/ 985418
- 9.
- Adolescent/ 2166028
- 10.
- Child/ 1825339
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kf. 1128017
- 12.
- or/8-11 3881789
- 13.
- Diagnosis/ 17509
- 14.
- Diagnostic Techniques, Endocrine/ 1070
- 15.
- Diagnosis, Differential/ 464734
- 16.
- Missed Diagnosis/ 267
- 17.
- Delayed Diagnosis/ 7754
- 18.
- Diagnostic Errors/ 39243
- 19.
- diagnos*.ti,kf. 740720
- 20.
- clinical diagnosis.ab. 48220
- 21.
- differential diagnosis.ab. 103059
- 22.
- diagnostic technique*.ab. 10773
- 23.
- (diagnos* adj3 criteria).ab. 63184
- 24.
- (diagnos* adj6 controver*).ab. 3425
- 25.
- (diagnos* adj6 dilemma*).ab. 5065
- 26.
- (diagnos* adj6 experience*).ab. 14465
- 27.
- (diagnos* adj6 dissatisf*).ab. 150
- 28.
- (diagnos* adj6 satisf*).ab. 3625
- 29.
- (diagnos* adj6 challeng*).ab. 40566
- 30.
- (diagnos* adj2 miss*).ab. 4898
- 31.
- (diagnos* adj2 delay*).ab. 24943
- 32.
- undiagnos*.ti,ab,kf. 22641
- 33.
- or/13-32 1346318
- 34.
- Ultrasonography/ 193782
- 35.
- Ultrasonography, Doppler/ 16855
- 36.
- Imaging, Three-Dimensional/ 78894
- 37.
- ultraso*.ti,ab,kf. 423835
- 38.
- doppler.ti,ab,kf. 110117
- 39.
- echograph*.ti,ab,kf. 10075
- 40.
- sonogra*.ti,ab,kf. 59806
- 41.
- imaging.ti,ab,kf. 952478
- 42.
- polycystic ovarian morphology.ti,ab,kf. 256
- 43.
- PCOM.ti,ab,kf. 316
- 44.
- or/34-43 1470075
- 45.
- 7 and 12 and 33 and 44 197
- 46.
- limit 45 to (english or spanish) 180
- Embase <1974 to 22 March 2022>
- 1.
- ovary polycystic disease/ 31135
- 2.
- polycystic ovar*.mp. 27137
- 3.
- poly-cystic ovar*.mp. 185
- 4.
- (PCOS or PCOD).mp. 20677
- 5.
- (stein-leventhal or leventhal).mp. 605
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 34324
- 7.
- or/1-6 36441
- 8.
- young adult/ 451020
- 9.
- adolescent/ 1656206
- 10.
- child/ 1913414
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1516782
- 12.
- or/8-11 3635590
- 13.
- diagnosis/ 1367804
- 14.
- differential diagnosis/ 354368
- 15.
- missed diagnosis/ 941
- 16.
- delayed diagnosis/ 15509
- 17.
- diagnostic error/ 64843
- 18.
- diagnos*.ti,kf. 863628
- 19.
- clinical diagnosis.ab. 71731
- 20.
- differential diagnosis.ab. 149450
- 21.
- diagnostic technique*.ab. 13979
- 22.
- (diagnos* adj3 criteria).ab. 102817
- 23.
- (diagnos* adj6 controver*).ab. 4766
- 24.
- (diagnos* adj6 dilemma*).ab. 7622
- 25.
- (diagnos* adj6 experience*).ab. 22680
- 26.
- (diagnos* adj6 dissatisf*).ab. 227
- 27.
- (diagnos* adj6 satisf*).ab. 5564
- 28.
- (diagnos* adj6 challeng*).ab. 62534
- 29.
- (diagnos* adj2 miss*).ab. 7784
- 30.
- (diagnos* adj2 delay*).ab. 39586
- 31.
- undiagnos*.ti,ab,kf. 34880
- 32.
- or/13-31 2589857
- 33.
- echography/ 351726
- 34.
- ultrasound/ 203032
- 35.
- doppler ultrasonography/ 8482
- 36.
- three-dimensional imaging/ 104412
- 37.
- ultraso*.ti,ab,kf. 624906
- 38.
- doppler.ti,ab,kf. 165439
- 39.
- echograph*.ti,ab,kf. 13252
- 40.
- sonogra*.ti,ab,kf. 84906
- 41.
- imaging.ti,ab,kf. 1338544
- 42.
- polycystic ovarian morphology.ti,ab,kf. 356
- 43.
- PCOM.ti,ab,kf. 502
- 44.
- or/33-43 2148774
- 45.
- 7 and 12 and 32 and 44 422
- 46.
- limit 45 to (english or spanish) 395
- EBM Reviews-Cochrane Central Register of Controlled Trials <January 2022>
- 1.
- Polycystic ovary syndrome/ 1649
- 2.
- polycystic ovar*.mp. 4330
- 3.
- poly-cystic ovar*.mp. 125
- 4.
- (PCOS or PCOD).mp. 3508
- 5.
- (stein-leventhal or leventhal).mp. 57
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 4491
- 7.
- or/1-6 4858
- 8.
- Young Adult/ 73866
- 9.
- Adolescent/ 110345
- 10.
- Child/ 52129
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 125810
- 12.
- or/8-11 262647
- 13.
- Diagnosis/ 69
- 14.
- Diagnostic Techniques, Endocrine/ 47
- 15.
- Diagnosis, Differential/ 1491
- 16.
- Missed Diagnosis/ 9
- 17.
- Delayed Diagnosis/ 28
- 18.
- Diagnostic Errors/ 286
- 19.
- diagnos*.ti,kw. 64022
- 20.
- diagnostic technique*.ab. 225
- 21.
- (diagnos* adj6 controver*).ab. 189
- 22.
- (diagnos* adj6 dilemma*).ab. 59
- 23.
- (diagnos* adj6 experience*).ab. 1344
- 24.
- (diagnos* adj6 dissatisf*).ab. 14
- 25.
- (diagnos* adj6 satisf*).ab. 775
- 26.
- (diagnos* adj6 challeng*).ab. 1224
- 27.
- (diagnos* adj2 miss*).ab. 300
- 28.
- (diagnos* adj2 delay*).ab. 746
- 29.
- undiagnos*.ti,ab,kw. 1141
- 30.
- or/13-29 68839
- 31.
- Ultrasonography/ 5104
- 32.
- Ultrasonography, Doppler/ 610
- 33.
- Imaging, Three-Dimensional/ 1198
- 34.
- ultraso*.ti,ab,kw. 45636
- 35.
- doppler.ti,ab,kw. 11283
- 36.
- echograph*.ti,ab,kw. 6197
- 37.
- sonogra*.ti,ab,kw. 4359
- 38.
- imaging.ti,ab,kw. 53978
- 39.
- polycystic ovarian morphology.ti,ab,kw. 27
- 40.
- PCOM.ti,ab,kw. 20
- 41.
- or/31-40 105019
- 42.
- 7 and 12 and 30 and 41 14
- 43.
- limit 42 to english language 13
- EBM Reviews-Cochrane Database of Systematic Reviews <2005 to 16 March 2022>
- 1.
- polycystic ovar*.mp. 149
- 2.
- poly-cystic ovar*.mp. 0
- 3.
- (PCOS or PCOD).mp. 84
- 4.
- (stein-leventhal or leventhal).mp. 39
- 5.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 150
- 6.
- or/1-5 174
- 7.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1243
- 8.
- diagnos*.ti,ab,kw. 1715
- 9.
- ultraso*.ti,ab,kw. 240
- 10.
- doppler.ti,ab,kw. 37
- 11.
- echograph*.ti,ab,kw. 0
- 12.
- sonogra*.ti,ab,kw. 9
- 13.
- imaging.ti,ab,kw. 230
- 14.
- polycystic ovarian morphology.ti,ab,kw. 0
- 15.
- PCOM.ti,ab,kw. 0
- 16.
- or/9-15 413
- 17.
- 6 and 7 and 8 and 16 0
- Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily <1946 to 13 May 2022>
- 1.
- Polycystic ovary syndrome/ 16686
- 2.
- polycystic ovar*.mp. 22098
- 3.
- poly-cystic ovar*.mp. 52
- 4.
- (PCOS or PCOD).mp. 13942
- 5.
- (stein-leventhal or leventhal).mp. 912
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 22219
- 7.
- or/1-6 22911
- 8.
- Young Adult/ 990846
- 9.
- Adolescent/ 2175898
- 10.
- Child/ 1841609
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kf. 1140005
- 12.
- or/8-11 3904962
- 13.
- Diagnosis/ 17514
- 14.
- Diagnostic Techniques, Endocrine/ 1071
- 15.
- Biomarkers/ 329596
- 16.
- Diagnosis, Differential/ 465318
- 17.
- Missed Diagnosis/ 280
- 18.
- Delayed Diagnosis/ 7853
- 19.
- Diagnostic Errors/ 39330
- 20.
- diagnos*.ti,kf. 746831
- 21.
- (biomarker* or marker*).ti,ab,kf. 1148168
- 22.
- clinical diagnosis.ab. 48824
- 23.
- differential diagnosis.ab. 103778
- 24.
- (diagnos* adj3 criteria).ab. 63792
- 25.
- (diagnos* adj6 controver*).ab. 3445
- 26.
- (diagnos* adj6 dilemma*).ab. 5122
- 27.
- (diagnos* adj6 experience*).ab. 14665
- 28.
- (diagnos* adj6 dissatisf*).ab. 151
- 29.
- (diagnos* adj6 satisf*).ab. 3659
- 30.
- (diagnos* adj6 challeng*).ab. 41398
- 31.
- (diagnos* adj2 miss*).ab. 4989
- 32.
- (diagnos* adj2 delay*).ab. 25305
- 33.
- undiagnos*.ti,ab,kf. 22874
- 34.
- or/13-33 2541115
- 35.
- Anti-Mullerian Hormone/ 3755
- 36.
- Anti-Mullerian Hormone.ti,ab,kf. 4463
- 37.
- antimullerian hormone.ti,ab,kf. 582
- 38.
- AMH.ti,ab,kf. 5049
- 39.
- Mullerian inhibiting substance.ti,ab,kf. 579
- 40.
- or/35-39 7018
- 41.
- 7 and 12 and 34 and 40 171
- 42.
- limit 41 to (english or spanish) 167
- Embase <1974 to 13 May 2022>
- 1.
- ovary polycystic disease/ 31705
- 2.
- polycystic ovar*.mp. 27648
- 3.
- poly-cystic ovar*.mp. 189
- 4.
- (PCOS or PCOD).mp. 21164
- 5.
- (stein-leventhal or leventhal).mp. 607
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 34931
- 7.
- or/1-6 37109
- 8.
- young adult/ 457981
- 9.
- adolescent/ 1668346
- 10.
- child/ 1930245
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1531909
- 12.
- or/8-11 3666415
- 13.
- diagnosis/ 1370526
- 14.
- endocrine system examination/ 545
- 15.
- biological marker/ 381458
- 16.
- differential diagnosis/ 356015
- 17.
- missed diagnosis/ 991
- 18.
- delayed diagnosis/ 15697
- 19.
- diagnostic error/ 65252
- 20.
- diagnos*.ti,kf. 871654
- 21.
- (biomarker* or marker*).ti,ab,kf. 1654043
- 22.
- clinical diagnosis.ab. 72479
- 23.
- differential diagnosis.ab. 150575
- 24.
- (diagnos* adj3 criteria).ab. 103665
- 25.
- (diagnos* adj6 controver*).ab. 4794
- 26.
- (diagnos* adj6 dilemma*).ab. 7711
- 27.
- (diagnos* adj6 experience*).ab. 22955
- 28.
- (diagnos* adj6 dissatisf*).ab. 229
- 29.
- (diagnos* adj6 satisf*).ab. 5604
- 30.
- (diagnos* adj6 challeng*).ab. 63546
- 31.
- (diagnos* adj2 miss*).ab. 7918
- 32.
- (diagnos* adj2 delay*).ab. 40023
- 33.
- undiagnos*.ti,ab,kf. 35267
- 34.
- or/13-33 4124534
- 35.
- Muellerian inhibiting factor/ 8673
- 36.
- Anti-Mullerian Hormone.ti,ab,kf. 6977
- 37.
- antimullerian hormone.ti,ab,kf. 996
- 38.
- AMH.ti,ab,kf. 9618
- 39.
- Mullerian inhibiting substance.ti,ab,kf. 716
- 40.
- or/35-39 13778
- 41.
- 7 and 12 and 34 and 40 192
- 42.
- limit 41 to (english or spanish) 186
- EBM Reviews-Cochrane Central Register of Controlled Trials <April 2022>
- 1.
- Polycystic ovary syndrome/ 1679
- 2.
- polycystic ovar*.mp. 4297
- 3.
- poly-cystic ovar*.mp. 132
- 4.
- (PCOS or PCOD).mp. 3496
- 5.
- (stein-leventhal or leventhal).mp. 57
- 6.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 4464
- 7.
- or/1-6 4827
- 8.
- Young Adult/ 74694
- 9.
- Adolescent/ 111127
- 10.
- Child/ 52868
- 11.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 125587
- 12.
- or/8-11 263322
- 13.
- Diagnosis/ 68
- 14.
- Diagnostic Techniques, Endocrine/ 47
- 15.
- Biomarkers/ 15881
- 16.
- Diagnosis, Differential/ 1490
- 17.
- Missed Diagnosis/ 11
- 18.
- Delayed Diagnosis/ 28
- 19.
- Diagnostic Errors/ 288
- 20.
- diagnos*.ti,kw. 65057
- 21.
- (biomarker* or marker*).ti,ab,kw. 84953
- 22.
- clinical diagnosis.ab. 5116
- 23.
- differential diagnosis.ab. 788
- 24.
- (diagnos* adj3 criteria).ab. 16717
- 25.
- (diagnos* adj6 controver*).ab. 105
- 26.
- (diagnos* adj6 dilemma*).ab. 45
- 27.
- (diagnos* adj6 experience*).ab. 760
- 28.
- (diagnos* adj6 dissatisf*).ab. 6
- 29.
- (diagnos* adj6 satisf*).ab. 474
- 30.
- (diagnos* adj6 challeng*).ab. 806
- 31.
- (diagnos* adj2 miss*).ab. 204
- 32.
- (diagnos* adj2 delay*).ab. 560
- 33.
- undiagnos*.ti,ab,kw. 1143
- 34.
- or/13-33 172052
- 35.
- Anti-Mullerian Hormone/ 134
- 36.
- Anti-Mullerian Hormone.ti,ab,kw. 580
- 37.
- antimullerian hormone.ti,ab,kw. 106
- 38.
- AMH.ti,ab,kw. 1005
- 39.
- Mullerian inhibiting substance.ti,ab,kw. 7
- 40.
- or/35-39 1214
- 41.
- 7 and 12 and 34 and 40 18
- 42.
- limit 41 to (english or spanish) 18
- EBM Reviews-Cochrane Database of Systematic Reviews <2005 to 11 May 2022>
- 1.
- polycystic ovar*.mp. 149
- 2.
- poly-cystic ovar*.mp. 0
- 3.
- (PCOS or PCOD).mp. 84
- 4.
- (stein-leventhal or leventhal).mp. 39
- 5.
- (ovar* adj5 (sclerocystic or polycystic or poly-cystic)).mp. 150
- 6.
- or/1-5 174
- 7.
- (adolescen* or teen* or school-age* or schoolage* or youth* or juvenile* or p?ediatric* or girl* or (young adj3 (adult* or person* or people* or wom#n))).ti,ab,kw. 1253
- 8.
- diagnos*.ti,ab,kw. 1727
- 9.
- undiagnos*.ti,ab,kw. 16
- 10.
- or/8-9 1731
- 11.
- Anti-Mullerian Hormone.ti,ab,kw. 2
- 12.
- antimullerian hormone.ti,ab,kw. 0
- 13.
- AMH.ti,ab,kw. 2
- 14.
- Mullerian inhibiting substance.ti,ab,kw. 0
- 15.
- or/11-14 2
- 16.
- 6 and 7 and 10 and 15 0
References
- Bozdag, G.; Mumusoglu, S.; Zengin, D.; Karabulut, E.; Yildiz, B.O. The prevalence and phenotypic features of polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. (Oxf. Engl.) 2016, 31, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Naz, M.S.G.; Tehrani, F.R.; Majd, H.A.; Ahmadi, F.; Ozgoli, G.; Fakari, F.R.; Ghasemi, V. The prevalence of polycystic ovary syndrome in adolescents: A systematic review and meta-analysis. Int. J. Reprod. Biomed. (Yazd Iran) 2019, 17, 533–542. [Google Scholar]
- Akgul, S.; Duzceker, Y.; Kanbur, N.; Derman, O. Do Different Diagnostic Criteria Impact Polycystic Ovary Syndrome Diagnosis for Adolescents? J. Pediatric Adolesc. Gynecol. 2018, 31, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Kostroun, K.E.; Goldrick, K.M.; Mondshine, J.N.; Robinson, R.D.; Brown, C.C.; Knudtson, J.F. Impact Of New 2018 International Diagnostic Criteria For The Diagnosis Of Polycystic Ovary Syndrome. Fertil. Steril. 2020, 114 (Suppl. S3), e401. [Google Scholar] [CrossRef]
- Yu, O.; Covey, J.; Grafton, J.; Cronkite, D.; Kelley, A.; Hansen, K.; Hilpert, J.; Schulze-Rath, R.; Reed, S.D. Identification of a diagnostically complex condition, polycystic ovarian syndrome, in a population-based cohort using electronic health record data. Pharmacoepidemiol. Drug Saf. 2021, 30 (Suppl. S1), 240–241. [Google Scholar]
- Cioana, M.; Deng, J.; Nadarajah, A.; Hou, M.; Qiu, Y.; Chen, S.S.J.; Rivas, A.; Banfield, L.; Alfaraidi, H.; Alotaibi, A.; et al. Prevalence of Polycystic Ovary Syndrome in Patients With Pediatric Type 2 Diabetes: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2147454. [Google Scholar] [CrossRef]
- Vink, J.M.; Sadrzadeh, S.; Lambalk, C.B.; Boomsma, D.I. Heritability of polycystic ovary syndrome in a Dutch twin-family study. J. Clin. Endocrinol. Metab. 2006, 91, 2100–2104. [Google Scholar] [CrossRef] [Green Version]
- Kocaay, P.; Siklar, Z.; Buyukfirat, S.; Berberoglu, M. The Diagnostic Value of Anti-Mullerian Hormone in Early Post Menarche Adolescent Girls with Polycystic Ovarian Syndrome. J. Pediatric Adolesc. Gynecol. 2018, 31, 362–366. [Google Scholar] [CrossRef]
- Tunc, S.; Ozkan, B. Analysis of New Biomarkers for the Diagnosis of Polycystic Ovary Syndrome in Adolescents. Guncel Pediatri 2021, 19, 311–318. [Google Scholar] [CrossRef]
- Hayes, M.G.; Urbanek, M.; Ehrmann, D.A.; Armstrong, L.L.; Lee, J.Y.; Sisk, R.; Karaderi, T.; Barber, T.M.; McCarthy, M.I.; Franks, S.; et al. Genome-wide association of polycystic ovary syndrome implicates alterations in gonadotropin secretion in European ancestry populations. Nat. Commun. 2015, 6, 7502. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Lv, Y.; Li, L.; Chen, Z.J. Genetic Studies on Polycystic Ovary Syndrome. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 37, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Day, F.; Karaderi, T.; Jones, M.R.; Meun, C.; He, C.; Drong, A.; Kraft, P.; Lin, N.; Huang, H.; Broer, L.; et al. Large-scale genome-wide meta-analysis of polycystic ovary syndrome suggests shared genetic architecture for different diagnosis criteria. PLoS Genet. 2018, 14, e1007813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Ho, K.; Keaton, J.M.; Hartzel, D.N.; Day, F.; Justice, A.E.; Josyula, N.S.; Pendergrass, S.A.; Actkins, K.E.; Davis, L.K.; et al. A genome-wide association study of polycystic ovary syndrome identified from electronic health records. Am. J. Obstet. Gynecol. 2020, 223, 559. [Google Scholar] [CrossRef] [PubMed]
- Risal, S.; Pei, Y.; Lu, H.; Manti, M.; Fornes, R.; Pui, H.P.; Zhao, Z.; Massart, J.; Ohlsson, C.; Lindgren, E.; et al. Prenatal androgen exposure and transgenerational susceptibility to polycystic ovary syndrome. Nat. Med. 2019, 25, 1894–1904. [Google Scholar] [CrossRef]
- Pena, A.S.; Metz, M. What is adolescent polycystic ovary syndrome? J. Paediatr. Child Health 2018, 54, 351–355. [Google Scholar] [CrossRef] [Green Version]
- Vassalou, H.; Sotiraki, M.; Michala, L. PCOS diagnosis in adolescents: The timeline of a controversy in a systematic review. J. Pediatric Endocrinol. Metab. 2019, 32, 549–559. [Google Scholar] [CrossRef]
- Peña, A.S.; Witchel, S.F.; Hoeger, K.M.; Oberfield, S.E.; Vogiatzi, M.G.; Misso, M.; Garad, R.; Dabadghao, P.; Teede, H. Adolescent polycystic ovary syndrome according to the international evidence-based guideline. BMC Med. 2020, 18, 72. [Google Scholar] [CrossRef]
- Rosenfield, R.L. Perspectives on the International Recommendations for the Diagnosis and Treatment of Polycystic Ovary Syndrome in Adolescence. J. Pediatric Adolesc. Gynecol. 2020, 33, 445–447. [Google Scholar] [CrossRef]
- Zawadski, J.; Dunaif, A. Diagnostic Criteria for Polycystic Ovary Syndrome. In Polycystic Ovary Syndrome; Dunaif, A., Givens, J., Haseltine, F., Eds.; Blackwell Scientific: Boston, MA, USA, 1992; pp. 377–384. [Google Scholar]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef]
- Azziz, R.; Carmina, E.; Dewailly, D.; Diamanti-Kandarakis, E.; Escobar-Morreale, H.F.; Futterweit, W.; Janssen, O.E.; Legro, R.S.; Norman, R.J.; Taylor, A.E.; et al. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: The complete task force report. Fertil. Steril. 2009, 91, 456–488. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Deeks, A.A.; Moran, L.J.; Stuckey, B.G.; Wong, J.L.; Norman, R.J.; Costello, M.F. Assessment and management of polycystic ovary syndrome: Summary of an evidence-based guideline. Med. J. Aust. 2011, 195, S65–S112. [Google Scholar] [CrossRef] [Green Version]
- Legro, R.S.; Arslanian, S.A.; Ehrmann, D.A.; Hoeger, K.M.; Murad, M.H.; Pasquali, R.; Welt, C.K.; Endocrine, S. Diagnosis and treatment of polycystic ovary syndrome: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2013, 98, 4565–4592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Wattar, B.H.; Fisher, M.; Bevington, L.; Talaulikar, V.; Davies, M.; Conway, G.; Yasmin, E. Clinical Practice Guidelines on the Diagnosis and Management of Polycystic Ovary Syndrome: A Systematic Review and Quality Assessment Study. J. Clin. Endocrinol. Metab. 2021, 106, 2436–2446. [Google Scholar] [CrossRef] [PubMed]
- Witchel, S.F.; Oberfield, S.; Rosenfield, R.L.; Codner, E.; Bonny, A.; Ibanez, L.; Pena, A.; Horikawa, R.; Gomez-Lobo, V.; Joel, D.; et al. The Diagnosis of Polycystic Ovary Syndrome during Adolescence. Horm. Res. Paediatr. 2015, 83, 376–389. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, L.; Oberfield, S.E.; Witchel, S.; Auchus, R.J.; Chang, R.J.; Codner, E.; Dabadghao, P.; Darendeliler, F.; Elbarbary, N.S.; Gambineri, A.; et al. An International Consortium Update: Pathophysiology, Diagnosis, and Treatment of Polycystic Ovarian Syndrome in Adolescence. Horm. Res. Paediatr. 2017, 88, 371–395. [Google Scholar] [CrossRef]
- Sebastian, M.R.; Wiemann, C.M.; Bacha, F.; Alston Taylor, S.J. Diagnostic Evaluation, Comorbidity Screening, and Treatment of Polycystic Ovary Syndrome in Adolescents in 3 Specialty Clinics. J. Pediatric Adolesc. Gynecol. 2018, 31, 367–371. [Google Scholar] [CrossRef]
- Pena, A.S.; Teede, H.; Hewawasam, E.; Hull, M.L.; Gibson-Helm, M. Diagnosis experiences of adolescents with polycystic ovary syndrome: Cross-sectional study. Clin. Endocrinol. 2022, 96, 62–69. [Google Scholar] [CrossRef]
- Li, L.; Feng, Q.; Ye, M.; He, Y.; Yao, A.; Shi, K. Metabolic effect of obesity on polycystic ovary syndrome in adolescents: A meta-analysis. J. Obstet. Gynaecol. 2017, 37, 1036–1047. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International, P.N. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Clin. Endocrinol. 2018, 89, 251–268. [Google Scholar] [CrossRef] [Green Version]
- Witchel, S.F.; Teede, H.J.; Peña, A.S. Curtailing PCOS. Pediatric Res. 2020, 87, 353–361. [Google Scholar] [CrossRef]
- Tay, C.T.; Hart, R.J.; Hickey, M.; Moran, L.J.; Earnest, A.; Doherty, D.A.; Teede, H.J.; Joham, A.E. Updated adolescent diagnostic criteria for polycystic ovary syndrome: Impact on prevalence and longitudinal body mass index trajectories from birth to adulthood. BMC Med. 2020, 18, 389. [Google Scholar] [CrossRef] [PubMed]
- Huguelet, P.S.; Olson, E.; Sass, A.; Bartz, S.; Hsu, S.; Cree-Green, M. Application of a Standard Cross-Specialty Workup for Diagnosis and Metabolic Screening of Obese Adolescents With Polycystic Ovary Syndrome. J. Adolesc. Health 2021, 68, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Torres, O.A.; Miller, E.; Witchel, S.F. Quality Improvement in the Evaluation and Diagnosis of Polycystic Ovary Syndrome in Adolescent Girls. J. Pediatric Adolesc. Gynecol. 2021, 34, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Legro, R.S.; Lin, H.M.; Demers, L.M.; Lloyd, T. Rapid maturation of the reproductive axis during perimenarche independent of body composition. J. Clin. Endocrinol. Metab. 2000, 85, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.Z.; Kangarloo, T.; Adams, J.M.; Sluss, P.M.; Welt, C.K.; Chandler, D.W.; Zava, D.T.; McGrath, J.A.; Umbach, D.M.; Hall, J.E.; et al. Healthy Post-Menarchal Adolescent Girls Demonstrate Multi-Level Reproductive Axis Immaturity. J. Clin. Endocrinol. Metab. 2019, 104, 613–623. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Pollack, S.; Ghods, A.; Dicken, C.; Isaac, B.; Adel, G.; Zeitlian, G.; Santoro, N. Onset of ovulation after menarche in girls: A longitudinal study. J. Clin. Endocrinol. Metab. 2008, 93, 1186–1194. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics; Committee on Adolescence; American College of Obstetricians and Gynecologists; Committee on Adolescent Health Care. Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign. Pediatrics 2006, 118, 2245–2250. [Google Scholar] [CrossRef] [Green Version]
- ACOG Committee on Adolescent Health Care. ACOG Committee Opinion No. 349, November 2006: Menstruation in girls and adolescents: Using the menstrual cycle as a vital sign. Obstet. Gynecol. 2006, 108, 1323–1328. [Google Scholar] [CrossRef]
- Widholm, O.; Kantero, R.L. A statistical analysis of the menstrual patterns of 8,000 Finnish girls and their mothers. Acta Obstet. Gynecol. Scand. Suppl. 1971, 14 (Suppl. S14), 1–36. [Google Scholar]
- Flug, D.; Largo, R.H.; Prader, A. Menstrual patterns in adolescent Swiss girls: A longitudinal study. Ann. Hum. Biol. 1984, 11, 495–508. [Google Scholar] [CrossRef]
- Varnell, R.R.; Arnold, T.J.; Quandt, S.A.; Talton, J.W.; Chen, H.; Miles, C.M.; Daniel, S.S.; Sandberg, J.C.; Anderson, K.A.; Arcury, T.A. Menstrual Cycle Patterns and Irregularities in Hired Latinx Child Farmworkers. J. Occup. Environ. Med. 2021, 63, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Treloar, A.E.; Boynton, R.E.; Behn, B.G.; Brown, B.W. Variation of the human menstrual cycle through reproductive life. Int. J. Fertil. 1967, 12 Pt 2, 77–126. [Google Scholar] [CrossRef]
- De Sanctis, V.; Bernasconi, S.; Bianchin, L.; Bona, G.; Bozzola, M.; Buzi, F.; De Sanctis, C.; Rigon, F.; Tatò, L.; Tonini, G.; et al. Onset of menstrual cycle and menses features among secondary school girls in Italy: A questionnaire study on 3,783 students. Indian J. Endocrinol. Metab. 2014, 18 (Suppl. S1), S84–S92. [Google Scholar] [PubMed]
- Assens, M.; Dyre, L.; Henriksen, L.S.; Brocks, V.; Sundberg, K.; Jensen, L.N.; Pedersen, A.T.; Main, K.M. Menstrual Pattern, Reproductive Hormones, and Transabdominal 3D Ultrasound in 317 Adolescent Girls. J. Clin. Endocrinol. Metab. 2020, 105, dgaa355. [Google Scholar] [CrossRef]
- Gruber, N.; Modan-Moses, D. Menstrual Cycle in Adolescents: Updating the Normal Pattern. J. Clin. Endocrinol. Metab. 2021, 106, e372–e374. [Google Scholar] [CrossRef] [PubMed]
- van Hooff, M.H.; Voorhorst, F.J.; Kaptein, M.B.; Hirasing, R.A.; Koppenaal, C.; Schoemaker, J. Predictive value of menstrual cycle pattern, body mass index, hormone levels and polycystic ovaries at age 15 years for oligo-amenorrhoea at age 18 years. Hum. Reprod. (Oxf. Engl.) 2004, 19, 383–392. [Google Scholar] [CrossRef] [Green Version]
- West, S.; Lashen, H.; Bloigu, A.; Franks, S.; Puukka, K.; Ruokonen, A.; Järvelin, M.R.; Tapanainen, J.S.; Morin-Papunen, L. Irregular menstruation and hyperandrogenaemia in adolescence are associated with polycystic ovary syndrome and infertility in later life: Northern Finland Birth Cohort 1986 study. Hum. Reprod. (Oxf. Engl.) 2014, 29, 2339–2351. [Google Scholar] [CrossRef] [Green Version]
- Fraser, I.S.; Critchley, H.O.; Munro, M.G.; Broder, M. Can we achieve international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding? Hum. Reprod. (Oxf. Engl.) 2007, 22, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Hale, G.E.; Zhao, X.; Hughes, C.L.; Burger, H.G.; Robertson, D.M.; Fraser, I.S. Endocrine features of menstrual cycles in middle and late reproductive age and the menopausal transition classified according to the Staging of Reproductive Aging Workshop (STRAW) staging system. J. Clin. Endocrinol. Metab. 2007, 92, 3060–3067. [Google Scholar] [CrossRef]
- O’Connor, K.A.; Ferrell, R.; Brindle, E.; Trumble, B.; Shofer, J.; Holman, D.J.; Weinstein, M. Progesterone and ovulation across stages of the transition to menopause. Menopause 2009, 16, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Codner, E.; Villarroel, C.; Eyzaguirre, F.C.; Lopez, P.; Merino, P.M.; Perez-Bravo, F.; Iniguez, G.; Cassorla, F. Polycystic ovarian morphology in postmenarchal adolescents. Fertil. Steril. 2011, 95, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, M.G.; Skidmore, D.S.; Lowry, G.F.; Mackenzie, J.A. Incidence of ovulation in the years after the menarche. J. Endocrinol. 1983, 97, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Apter, D.; Bolton, N.J.; Hammond, G.L.; Vihko, R. Serum sex hormone-binding globulin during puberty in girls and in different types of adolescent menstrual cycles. Acta Endocrinol. (Copenh.) 1984, 107, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Seidman, L.C.; Brennan, K.M.; Rapkin, A.J.; Payne, L.A. Rates of Anovulation in Adolescents and Young Adults with Moderate to Severe Primary Dysmenorrhea and Those without Primary Dysmenorrhea. J. Pediatric Adolesc. Gynecol. 2018, 31, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Pena, A.S.; Doherty, D.A.; Atkinson, H.C.; Hickey, M.; Norman, R.J.; Hart, R. The majority of irregular menstrual cycles in adolescence are ovulatory: Results of a prospective study. Arch. Dis. Child. 2018, 103, 235–239. [Google Scholar] [CrossRef] [Green Version]
- Codner, E.; Eyzaguirre, F.C.; Iñiguez, G.; López, P.; Pérez-Bravo, F.; Torrealba, I.M.; Cassorla, F.; Chilean Group for the Study of Ovarian Function in Type 1 Diabetes. Ovulation rate in adolescents with type 1 diabetes mellitus. Fertil. Steril. 2011, 95, 197–202.e1. [Google Scholar] [CrossRef]
- Morrison, J.A.; Glueck, C.J.; Daniels, S.; Wang, P.; Stroop, D. Ramifications of adolescent menstrual cycles ≥ 42 days in young adults. Fertil. Steril. 2011, 96, 236–240.e1. [Google Scholar] [CrossRef] [Green Version]
- Pinola, P.; Morin-Papunen, L.C.; Bloigu, A.; Puukka, K.; Ruokonen, A.; Jarvelin, M.R.; Franks, S.; Tapanainen, J.S.; Lashen, H. Anti-Mullerian hormone: Correlation with testosterone and oligo- Or amenorrhoea in female adolescence in a population-based cohort study. Hum. Reprod. 2014, 29, 2317–2325. [Google Scholar] [CrossRef] [Green Version]
- van Hooff, M.H.; Voorhorst, F.J.; Kaptein, M.B.; Hirasing, R.A.; Koppenaal, C.; Schoemaker, J. Endocrine features of polycystic ovary syndrome in a random population sample of 14–16 year old adolescents. Hum. Reprod. (Oxf. Engl.) 1999, 14, 2223–2229. [Google Scholar] [CrossRef]
- Davis-Kankanamge, C.N.; Strickland, J.; Carnahan, M.; Higgins, J.; Dowlut-McElroy, T. The association between body mass index and androgen levels in adolescent girls with irregular menses or amenorrhea. Fertil. Steril. 2016, 106 (Suppl. S3), e255. [Google Scholar] [CrossRef]
- Lass, N.; Kleber, M.; Winkel, K.; Wunsch, R.; Reinehr, T. Effect of lifestyle intervention on features of polycystic ovarian syndrome, metabolic syndrome, and intima-media thickness in obese adolescent girls. J. Clin. Endocrinol. Metab. 2011, 96, 3533–3540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caanen, M.R.; Peters, H.E.; van de Ven, P.M.; Juttner, A.M.F.M.; Laven, J.S.E.; van Hooff, M.H.A.; Lambalk, C.B. Anti-Mullerian Hormone Levels in Adolescence in Relation to Long-term Follow-up for Presence of Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, e1084–e1095. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, B.O.; Bolour, S.; Woods, K.; Moore, A.; Azziz, R. Visually scoring hirsutism. Hum. Reprod. Update 2010, 16, 51–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeUgarte, C.M.; Woods, K.S.; Bartolucci, A.A.; Azziz, R. Degree of facial and body terminal hair growth in unselected black and white women: Toward a populational definition of hirsutism. J. Clin. Endocrinol. Metab. 2006, 91, 1345–1350. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Ni, R.; Li, L.; Mo, Y.; Huang, J.; Huang, M.; Azziz, R.; Yang, D. Defining hirsutism in Chinese women: A cross-sectional study. Fertil. Steril. 2011, 96, 792–796. [Google Scholar] [CrossRef]
- Chan, J.L.; Pall, M.; Ezeh, U.; Mathur, R.; Pisarska, M.D.; Azziz, R. Screening for Androgen Excess in Women: Accuracy of Self-Reported Excess Body Hair Growth and Menstrual Dysfunction. J. Clin. Endocrinol. Metab. 2020, 105, e3688–e3695. [Google Scholar] [CrossRef]
- Asanidze, E.; Kristesashvili, J.; Parunashvili, N.; Karelishvili, N.; Etsadashvili, N. Challenges in diagnosis of polycystic ovary syndrome in adolescence. Gynecol. Endocrinol. 2021, 37, 819–822. [Google Scholar] [CrossRef]
- Taylor, A.E.; Ware, M.A.; Breslow, E.; Pyle, L.; Severn, C.; Nadeau, K.J.; Chan, C.L.; Kelsey, M.M.; Cree-Green, M. 11-Oxyandrogens in Adolescents With Polycystic Ovary Syndrome. J. Endocr. Soc. 2022, 6, bvac037. [Google Scholar] [CrossRef]
- Zore, T.; Lizneva, D.; Brakta, S.; Walker, W.; Suturina, L.; Azziz, R. Minimal difference in phenotype between adolescents and young adults with polycystic ovary syndrome. Fertil. Steril. 2019, 111, 389–396. [Google Scholar] [CrossRef]
- Hickey, M.; Doherty, D.A.; Atkinson, H.; Sloboda, D.M.; Franks, S.; Norman, R.J.; Hart, R. Clinical, ultrasound and biochemical features of polycystic ovary syndrome in adolescents: Implications for diagnosis. Hum. Reprod. 2011, 26, 1469–1477. [Google Scholar] [CrossRef] [Green Version]
- Gambineri, A.; Fanelli, F.; Prontera, O.; Repaci, A.; Di Dalmazi, G.; Zanotti, L.; Pagotto, U.; Flacco, M.E.; Guidi, J.; Fava, G.A.; et al. Prevalence of hyperandrogenic states in late adolescent and young women: Epidemiological survey on italian high-school students. J. Clin. Endocrinol. Metab. 2013, 98, 1641–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Zegarra, C.; Sundararajan, D.; Benson, J.; Seagle, H.; Witten, M.; Walders-Abramson, N.; Simon, S.L.; Huguelet, P.; Nokoff, N.J.; Cree-Green, M. Care for Adolescents with PCOS: Development and prescribing patterns of a multidisciplinary clinic. J. Pediatric Adolesc. Gynecol. 2021, 34, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Ramezani Tehrani, F.; Behboudi-Gandevani, S.; Bidhendi Yarandi, R.; Saei Ghare Naz, M.; Carmina, E. Prevalence of acne vulgaris among women with polycystic ovary syndrome: A systemic review and meta-analysis. Gynecol. Endocrinol. 2021, 37, 392–405. [Google Scholar] [CrossRef] [PubMed]
- Carmina, E.; Azziz, R.; Bergfeld, W.; Escobar-Morreale, H.F.; Futterweit, W.; Huddleston, H.; Lobo, R.; Olsen, E. Female Pattern Hair Loss and Androgen Excess: A Report From the Multidisciplinary Androgen Excess and PCOS Committee. J. Clin. Endocrinol. Metab. 2019, 104, 2875–2891. [Google Scholar] [CrossRef]
- Ucar, M.; Ata, A.; Barutcuoglu, B.; Ak, G.; Habif, S.; Parildar, Z.; Goksen, D.; Darcan, S.; Ozen, S. Plasma steroid panel with liquid chromotographymass spectrometry (LC/MS-MS) method: Utilization in differential diagnosis of hyperandrogenism. Horm. Res. Paediatr. 2021, 94 (Suppl. S1), 124. [Google Scholar]
- Nicolaides, N.C.; Matheou, A.; Vlachou, F.; Neocleous, V.; Skordis, N. Polycystic ovarian syndrome in adolescents: From diagnostic criteria to therapeutic management. Acta Biomed. 2020, 91, e2020085. [Google Scholar]
- Khashchenko, E.; Uvarova, E.; Vysokikh, M.; Ivanets, T.; Krechetova, L.; Tarasova, N.; Sukhanova, I.; Mamedova, F.; Borovikov, P.; Balashov, I.; et al. The Relevant Hormonal Levels and Diagnostic Features of Polycystic Ovary Syndrome in Adolescents. J. Clin. Med. 2020, 9, 1831. [Google Scholar] [CrossRef]
- Pignatelli, D. Non-classic adrenal hyperplasia due to the deficiency of 21-hydroxylase and its relation to polycystic ovarian syndrome. Front. Horm. Res. 2013, 40, 158–170. [Google Scholar]
- Esquivel-Zuniga, M.R.; Kirschner, C.K.; McCartney, C.R.; Burt Solorzano, C.M. Non-PCOS Hyperandrogenic Disorders in Adolescents. Semin. Reprod. Med. 2022, 40, 42–52. [Google Scholar] [CrossRef]
- Demirci, T.; Cengiz, H.; Varim, C.; Cetin, S. The role and importance of auxiliary tests in differential diagnosis in patients with mildly high basal 17-OH-progesterone levels in the evaluation of hirsutism. Turk. J. Med. Sci. 2020, 50, 1976–1982. [Google Scholar] [CrossRef]
- Lidaka, L.; Bekere, L.; Rota, A.; Isakova, J.; Lazdane, G.; Kivite-Urtane, A.; Dzivite-Krisane, I.; Kempa, I.; Dobele, Z.; Gailite, L. Role of Single Nucleotide Variants in FSHR, GNRHR, ESR2 and LHCGR Genes in Adolescents with Polycystic Ovary Syndrome. Diagnostics 2021, 11, 2327. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.H.; Rizvi, S.A.; Shahid, R.; Manzoor, R. Dehydroepiandrosterone Sulfate (DHEAS) levels in Polycystic Ovary Syndrome (PCOS). J. Coll. Physicians Surg. Pak. 2021, 31, 253–257. [Google Scholar] [PubMed]
- Turcu, A.F.; Rege, J.; Auchus, R.J.; Rainey, W.E. 11-Oxygenated androgens in health and disease. Nat. Rev. Endocrinol. 2020, 16, 284–296. [Google Scholar] [CrossRef]
- Fulghesu, A.M.; Canu, E.; Casula, L.; Melis, F.; Gambineri, A. Polycystic Ovarian Morphology in Normocyclic Non-hyperandrogenic Adolescents. J. Pediatric Adolesc. Gynecol. 2021, 34, 612–616. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, D.; Li, L.; Chen, X. The role of ovarian volume as a diagnostic criterion for Chinese adolescents with polycystic ovary syndrome. J. Pediatric Adolesc. Gynecol. 2008, 21, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Fu, Q. Three-dimensional transrectal ultrasonography in adolescent patients with polycystic ovarian syndrome. Int. J. Gynaecol. Obstet. 2007, 98, 34–38. [Google Scholar] [CrossRef]
- Senaldi, L.; Gopi, R.P.; Milla, S.; Shah, B. Is ultrasound useful in the diagnosis of adolescents with polycystic ovary syndrome? J. Pediatric Endocrinol. Metab. 2015, 28, 605–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fondin, M.; Rachas, A.; Huynh, V.; Franchi-Abella, S.; Teglas, J.P.; Duranteau, L.; Adamsbaum, C. Polycystic ovary syndrome in adolescents: Which MR Imaging-based diagnostic criteria? Radiology 2017, 285, 961–970. [Google Scholar] [CrossRef] [Green Version]
- Kayemba-Kay’s, S.; Pambou, A.; Heron, A.; Benosman, S.M. Polycystic ovary syndrome: Pelvic MRI as alternative to pelvic ultrasound for the diagnosis in overweight and obese adolescent girls. Int. J. Pediatrics Adolesc. Med. 2017, 4, 147–152. [Google Scholar] [CrossRef]
- Venturoli, S.; Porcu, E.; Fabbri, R.; Pluchinotta, V.; Ruggeri, S.; Macrelli, S.; Paradisi, R.; Flamigni, C. Longitudinal change of sonographic ovarian aspects and endocrine parameters in irregular cycles of adolescence. Pediatric Res. 1995, 38, 974–980. [Google Scholar] [CrossRef] [Green Version]
- Merino, P.M.; Villarroel, C.; Jesam, C.; Lopez, P.; Codner, E. New Diagnostic Criteria of Polycystic Ovarian Morphology for Adolescents: Impact on Prevalence and Hormonal Profile. Horm. Res. Paediatr. 2017, 88, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Radivojevic, U.D.; Lazovic, G.B.; Kravic-Stevovic, T.K.; Puzigaca, Z.D.; Canovic, F.M.; Nikolic, R.R.; Milicevic, S.M. Differences in anthropometric and ultrasonographic parameters between adolescent girls with regular and irregular menstrual cycles: A case-study of 835 cases. J. Pediatric Adolesc. Gynecol. 2014, 27, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.L.; Ramlau-Hansen, C.H.; Ernst, E.; Olsen, S.F.; Bonde, J.P.; Vested, A.; Toft, G. A very large proportion of young Danish women have polycystic ovaries: Is a revision of the Rotterdam criteria needed? Hum. Reprod. (Oxf. Engl.) 2010, 25, 3117–3122. [Google Scholar] [CrossRef] [Green Version]
- Dewailly, D.; Lujan, M.E.; Carmina, E.; Cedars, M.I.; Laven, J.; Norman, R.J.; Escobar-Morreale, H.F. Definition and significance of polycystic ovarian morphology: A task force report from the Androgen Excess and Polycystic Ovary Syndrome Society. Hum. Reprod. Update 2014, 20, 334–352. [Google Scholar] [CrossRef] [PubMed]
- Pecchioli, Y.; Oyewumi, L.; Allen, L.M.; Kives, S. The Utility of Routine Ultrasound in the Diagnosis and Management of Adolescents with Abnormal Uterine Bleeding. J. Pediatric Adolesc. Gynecol. 2017, 30, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Jopling, H.; Yates, A.; Burgoyne, N.; Hayden, K.; Chaloner, C.; Tetlow, L. Paediatric Anti-Mullerian Hormone measurement: Male and female reference intervals established using the automated Beckman Coulter Access AMH assay. Endocrinol. Diabetes Metab. 2018, 1, e00021. [Google Scholar] [CrossRef] [Green Version]
- Van Helden, J.; Weiskirchen, R.; Evliyaoglu, O. Age-specific Reference Values for the Roche Elecsys AMH assay and its Diagnostic Performance in PCOS. J. Lab. Med. 2019, 43, eA26. [Google Scholar]
- Evliyaoglu, O.; Imohl, M.; Weiskirchen, R.; Van Helden, J. Age-specific reference values improve the diagnostic performance of AMH in polycystic ovary syndrome. Clin. Chem. Lab. Med. 2020, 58, 1291–1301. [Google Scholar] [CrossRef]
- Song, J.; Park, Y.; Cho, H.W.; Lee, S.G.; Kim, S.; Lim, J.B. Age-group-specific reference intervals for anti-Mullerian hormone and its diagnostic performance for polycystic ovary syndrome in a Korean population. J. Clin. Lab. Anal. 2021, 35, e23861. [Google Scholar] [CrossRef]
- Smith, M.; Ho, J.R.; Ma, L.; Lee, M.; Czerwinski, S.A.; Glenn, T.; Cool, D.R.; Gagneux, P.; Frank, S.; Lindheim, S.R. Does anti-mullerian hormone (AMH) predict biochemical hyperandrogenism, oligo-anovulation (OA), metabolic dysfunction (MD), and metabolic syndrome (METS)?: Results from a longitudinal study. Fertil. Steril. 2019, 111 (Suppl. S4), e37. [Google Scholar] [CrossRef] [Green Version]
- Villarroel, C.; Merino, P.M.; Lopez, P.; Eyzaguirre, F.C.; Van Velzen, A.; Iniguez, G.; Codner, E. Polycystic ovarian morphology in adolescents with regular menstrual cycles is associated with elevated anti-Mullerian hormone. Hum. Reprod. (Oxf. Engl.) 2011, 26, 2861–2868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teede, H.; Misso, M.; Tassone, E.C.; Dewailly, D.; Ng, E.H.; Azziz, R.; Norman, R.J.; Andersen, M.; Franks, S.; Hoeger, K.; et al. Anti-Müllerian Hormone in PCOS: A Review Informing International Guidelines. Trends Endocrinol. Metab. 2019, 30, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.W.; Brill, S.; Shanazarian, M.; Samonte, K. Anti-Mullerian Hormone As A Diagnostic Tool For Polycystic Ovarian Syndrome In Adolescent Population. J. Adolesc. Health 2019, 64 (Suppl. S2), S48–S49. [Google Scholar] [CrossRef]
- Hart, R.; Doherty, D.A.; Norman, R.J.; Franks, S.; Dickinson, J.E.; Hickey, M.; Sloboda, D.M. Serum antimullerian hormone (AMH) levels are elevated in adolescent girls with polycystic ovaries and the polycystic ovarian syndrome (PCOS). Fertil. Steril. 2010, 94, 1118–1121. [Google Scholar] [CrossRef]
- Tokmak, A.; Timur, H.; Aksoy, R.T.; Cinar, M.; Yilmaz, N. Is anti-Mullerian hormone a good diagnostic marker for adolescent and young adult patients with Polycystic ovary syndrome? Turk. J. Obstet. Gynecol. 2015, 12, 199–204. [Google Scholar] [CrossRef]
- Yetim, A.; Yetim, C.; Bas, F.; Erol, O.B.; Cig, G.; Ucar, A.; Darendeliler, F. Anti-Mullerian Hormone and Inhibin-A, but not Inhibin-B or Insulin-Like Peptide-3, may be Used as Surrogates in the Diagnosis of Polycystic Ovary Syndrome in Adolescents: Preliminary Results. J. Clin. Res. Pediatric Endocrinol. 2016, 8, 288–297. [Google Scholar] [CrossRef]
- Hristova, D.; Kirilov, G. Hormonal status and bone turnover in adolescents with polycystic ovarian syndrome. Clin. Exp. Obstet. Gynecol. 2022, 49, 56. [Google Scholar] [CrossRef]
- Sopher, A.B.; Grigoriev, G.; Laura, D.; Cameo, T.; Lerner, J.P.; Chang, R.J.; McMahon, D.J.; Oberfield, S.E. Anti-Mullerian hormone may be a useful adjunct in the diagnosis of polycystic ovary syndrome in nonobese adolescents. J. Pediatric Endocrinol. Metab. 2014, 27, 1175–1179. [Google Scholar] [CrossRef] [Green Version]
- Savas-Erdeve, S.; Keskin, M.; Sagsak, E.; Cenesiz, F.; Cetinkaya, S.; Aycan, Z. Do the Anti-Mullerian Hormone Levels of Adolescents with Polycystic Ovary Syndrome, Those Who Are at Risk for Developing Polycystic Ovary Syndrome, and Those Who Exhibit Isolated Oligomenorrhea Differ from Those of Adolescents with Normal Menstrual Cycles? Horm. Res. Paediatr. 2016, 85, 406–411. [Google Scholar] [CrossRef]
- Kim, J.Y.; Tfayli, H.; Michaliszyn, S.F.; Lee, S.; Nasr, A.; Arslanian, S. Anti-Mullerian Hormone in Obese Adolescent Girls With Polycystic Ovary Syndrome. J. Adolesc. Health 2017, 60, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Pankhurst, M.W.; Dillingham, P.W.; Pena, A.S. Proteolytic activation of anti-Mullerian hormone is suppressed in adolescent girls. Endocrine 2022, 76, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Siow, Y.; Kives, S.; Hertweck, P.; Perlman, S.; Fallat, M.E. Serum Mullerian-inhibiting substance levels in adolescent girls with normal menstrual cycles or with polycystic ovary syndrome. Fertil. Steril. 2005, 84, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Kulle, A.; Rothermel, J.; Knop, C.; Lass, N.; Bosse, C.; Holterhus, P.M. Weight loss in obese girls with polycystic ovarian syndrome is associated with a decrease in Anti-Muellerian Hormone concentrations. Clin. Endocrinol. 2017, 87, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Dursun, F.; Guven, A.; Yildiz, M. Assessment of Anti-Mullerian Hormone Level in Management of Adolescents with Polycystic Ovary Syndrome. J. Clin. Res. Pediatric Endocrinol. 2016, 8, 55–60. [Google Scholar] [CrossRef]
- Li, M.; Ruan, X.; Ju, R.; Min, M.; Xu, Z.; Luo, S.; Wang, H.; Mueck, A.O. Is anti-Mullerian hormone a useful biomarker in the diagnosis of polycystic ovary syndrome in Chinese adolescents? Gynecol. Endocrinol. 2022, 38, 148–152. [Google Scholar] [CrossRef]
- Ramezani Tehrani, F.; Rahmati, M.; Mahboobifard, F.; Firouzi, F.; Hashemi, N.; Azizi, F. Age-specific cut-off levels of anti-Mullerian hormone can be used as diagnostic markers for polycystic ovary syndrome. Reprod. Biol. Endocrinol. 2021, 19, 76. [Google Scholar] [CrossRef]
- Peña, A.S.; Curran, J.A.; Fuery, M.; George, C.; Jefferies, C.A.; Lobley, K.; Ludwig, K.; Maguire, A.M.; Papadimos, E.; Peters, A.; et al. Screening, assessment and management of type 2 diabetes mellitus in children and adolescents: Australasian Paediatric Endocrine Group guidelines. Med. J. Aust. 2020, 213, 30–43. [Google Scholar] [CrossRef]
- Hudnut-Beumler, J.; Kaar, J.L.; Taylor, A.; Kelsey, M.M.; Nadeau, K.J.; Zeitler, P.; Snell-Bergeon, J.; Pyle, L.; Cree-Green, M. Development of type 2 diabetes in adolescent girls with polycystic ovary syndrome and obesity. Pediatric Diabetes 2021, 22, 699–706. [Google Scholar] [CrossRef]
- Benson, J.; Severn, C.; Hudnut-Beumler, J.; Simon, S.L.; Abramson, N.; Shomaker, L.B.; Gulley, L.D.; Taylor, A.; Kelsey, M.M.; Nadeau, K.J.; et al. Depression in Girls With Obesity and Polycystic Ovary Syndrome and/or Type 2 Diabetes. Can. J. Diabetes 2020, 44, 507–513. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Criteria Definition | Witchel S et al. 2015 [25] | Ibanez L et al. 2017 [26] | Pena AS et al. 2020 [17] |
|---|---|---|---|
| Menstrual Irregularity Ovulatory dysfunction | Menstrual cycles < 20 days and >45 days two years post-menarche | Irregular cycles two years post-menarche | Strict definition according to time post-menarche Irregular cycles are normal 1st year post-menarche Menstrual cycles < 21 and >45 days 1–3 years post-menarche Menstrual cycles < 21 days and >35 days 3 years post-menarche (<8 cycles per year) |
| Menstrual cycles > 90 days 1 year post-menarche | Menstrual cycles > 90 days 1 year post-menarche | Menstrual cycles > 90 days 1 year post-menarche | |
| Primary amenorrhea by 15 years or after 2–3 years post thelarche | Primary amenorrhea in girls that completed puberty | Primary amenorrhea by 15 years or after 3 years post thelarche | |
| Hyperandrogenism | Clinical: moderate to severe hirsutism (no definition provided) and/or persistent acne unresponsive to topical therapy Rarely alopecia Biochemical: confirmation test in girls with hyperandrogenism Persistent elevation of total testosterone and/or free testosterone A single androgen test two standard deviations above the mean for the assay | Clinical: progressive hirsutism and/or moderate to severe acne unresponsive to topical therapy (severe cystic acne) Rarely alopecia Biochemical: confirmation test in girls with hyperandrogenism using high quality assays. No clear cut off for testosterone given | Clinical: hirsutism defined as modified Ferriman Gellway score. 4–6 and/or severe acne Rarely alopecia Biochemical: In females with irregular cycles yet without hyperandrogenism testosterone, free testosterone of free androgen index can assist with diagnosis. No cut offs given |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña, A.S.; Codner, E.; Witchel, S. Criteria for Diagnosis of Polycystic Ovary Syndrome during Adolescence: Literature Review. Diagnostics 2022, 12, 1931. https://doi.org/10.3390/diagnostics12081931
Peña AS, Codner E, Witchel S. Criteria for Diagnosis of Polycystic Ovary Syndrome during Adolescence: Literature Review. Diagnostics. 2022; 12(8):1931. https://doi.org/10.3390/diagnostics12081931
Chicago/Turabian StylePeña, Alexia S., Ethel Codner, and Selma Witchel. 2022. "Criteria for Diagnosis of Polycystic Ovary Syndrome during Adolescence: Literature Review" Diagnostics 12, no. 8: 1931. https://doi.org/10.3390/diagnostics12081931