
Prediction of Intraparenchymal Hemorrhage Progression and Neurologic Outcome in Traumatic Brain Injury Patients Using Radiomics Score and Clinical Parameters

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
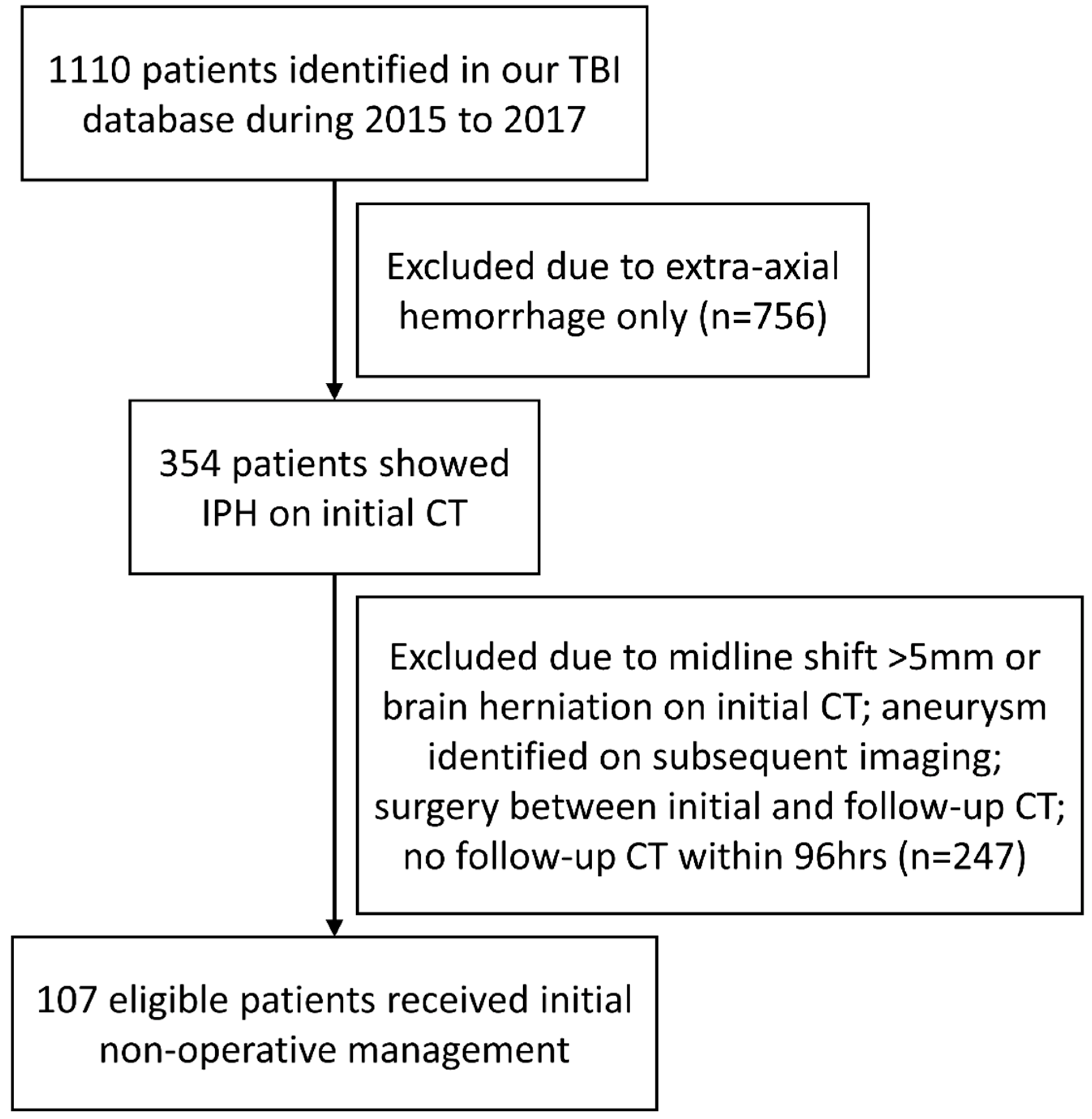
2.1. Patient Identification, Baseline Parameters, and Outcomes’ Definitions
2.2. CT Protocols
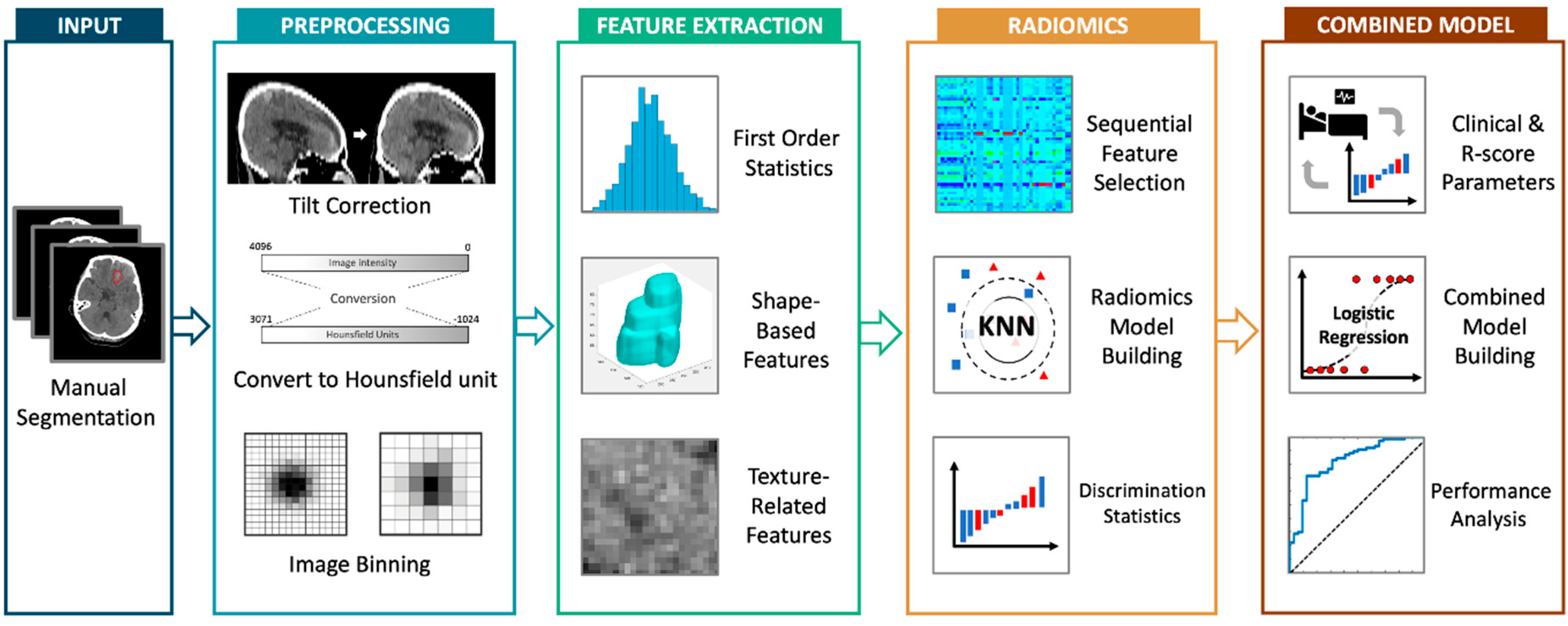
2.3. Image Segmentation
2.4. Radiomics Features’ Extraction and Selection
2.5. Radiomics Score and Performance Evaluation
2.6. Building of Combined Clinical–Radiomics Model
3. Results
3.1. Baseline Patient Characteristics
3.2. Repeatability of Segmentations
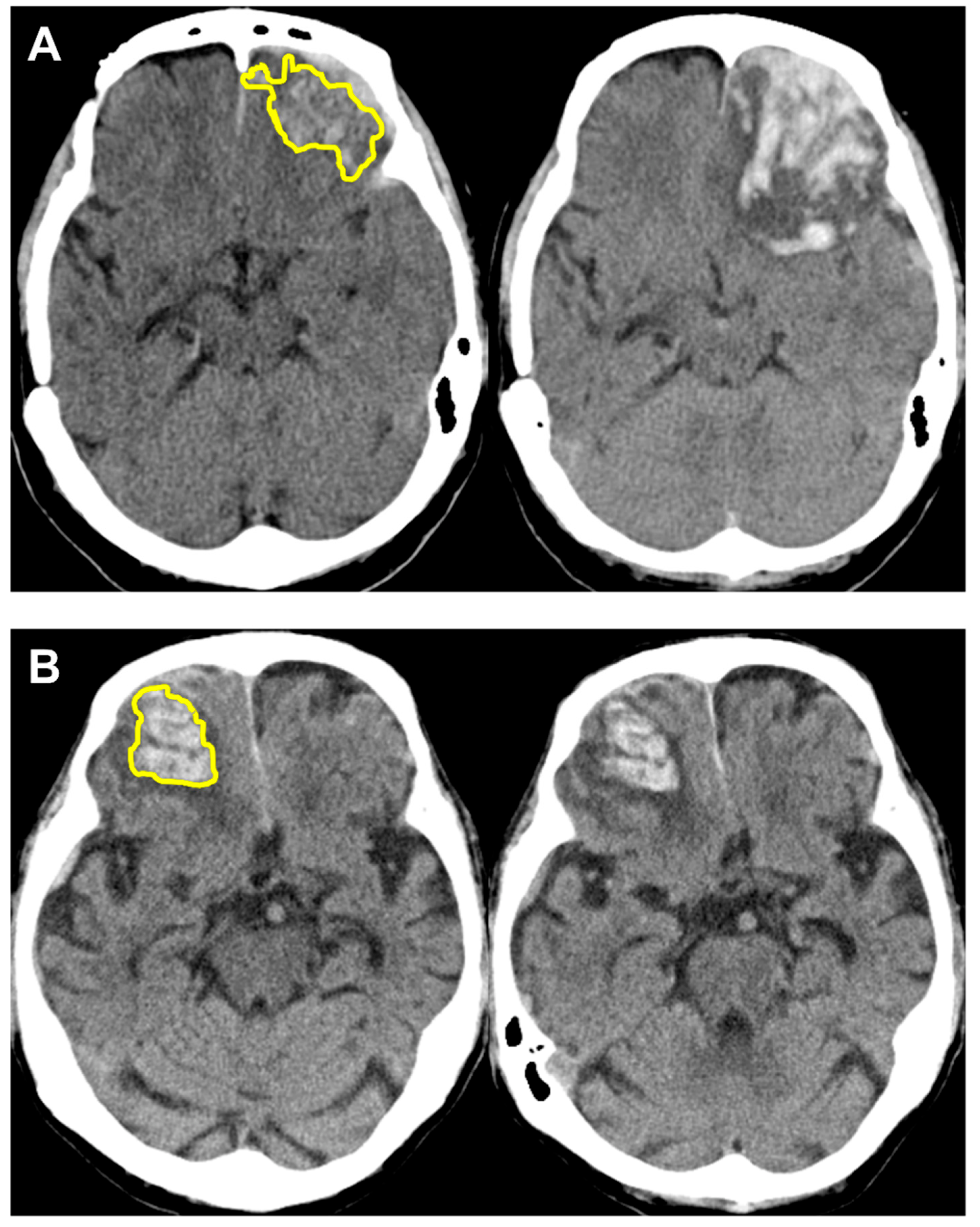
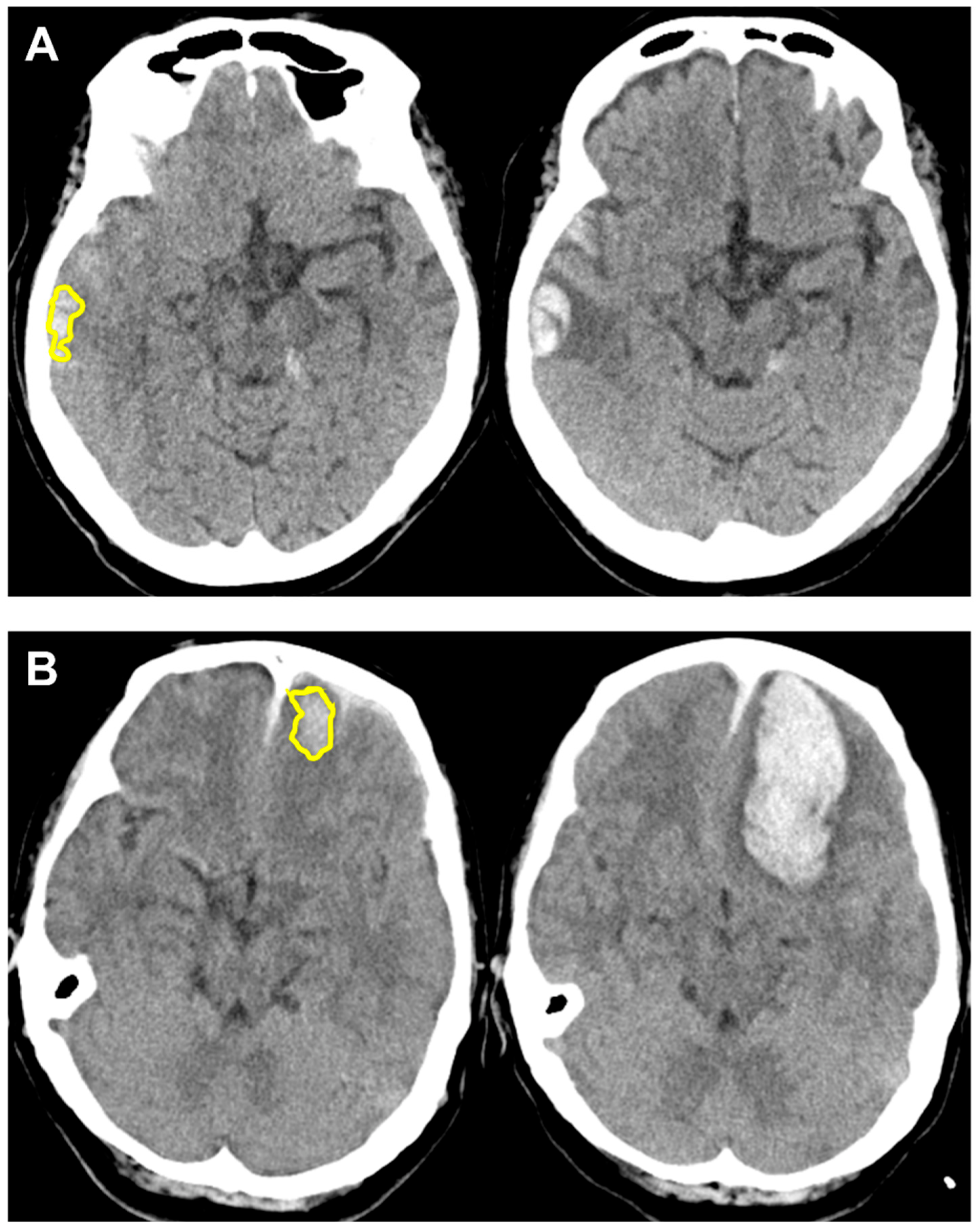
3.3. Performance of Radiomics Score with Case Examples
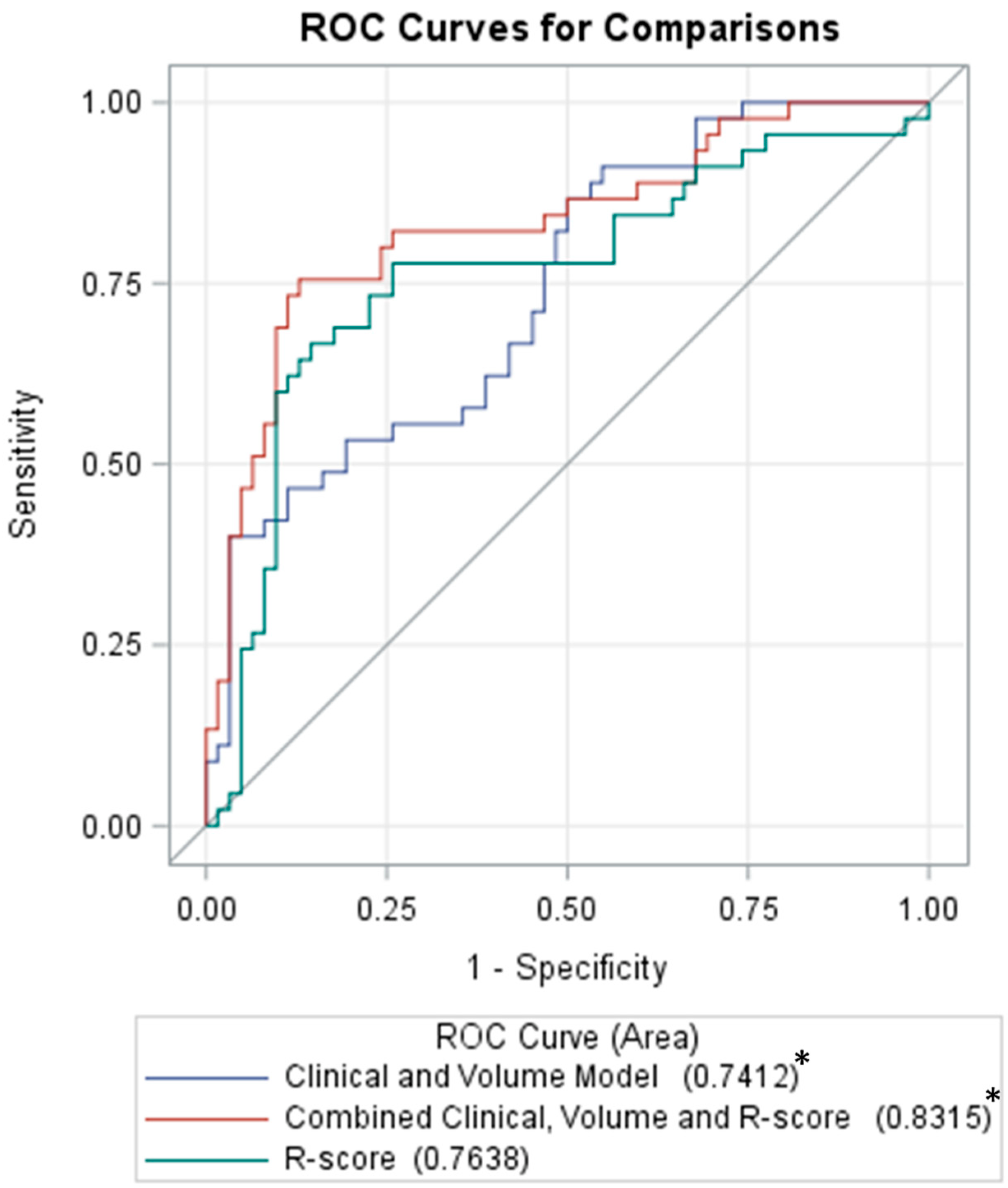
3.4. Combined Clinical–Radiomics Model for Prediction of Hemorrhagic Progression
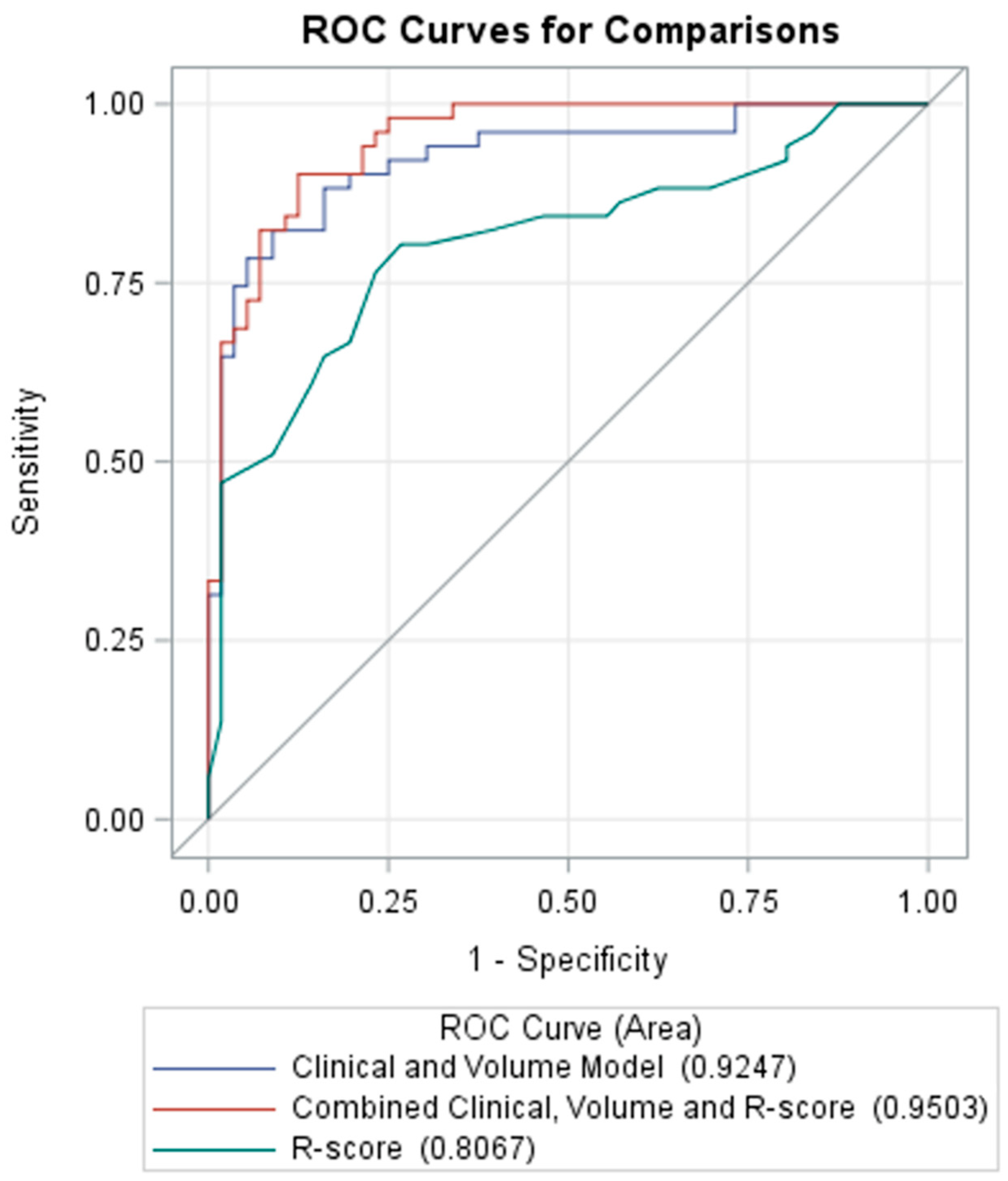
3.5. Prediction of Poor Neurologic Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peterson, A.B.; Zhou, H.; Thomas, K.E.; Daugherty, J. Surveillance Report of Traumatic Brain Injury-related Hospitalizations and Deaths by Age Group, Sex, and Mechanism of Injury—United States, 2016 and 2017. 2021. Available online: https://www.cdc.gov/traumaticbraininjury/pdf/TBI-surveillance-report-2016-2017-508.pdf (accessed on 21 September 2021).
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurland, D.; Hong, C.; Aarabi, B.; Gerzanich, V.; Simard, J.M. Hemorrhagic progression of a contusion after traumatic brain injury: A review. J. Neurotrauma 2012, 29, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, A.D.; Niogi, S.N.; Whitlow, C.T.; Tsiouris, A.J. Traumatic Brain Injury: Imaging Patterns and Complications. In Radiographics: A Review; Publication of the Radiological Society of North America, Inc.: Chicago, IL, USA, 2019; Volume 39, pp. 1571–1595. [Google Scholar] [CrossRef]
- Adatia, K.; Newcombe, V.F.J.; Menon, D.K. Contusion Progression Following Traumatic Brain Injury: A Review of Clinical and Radiological Predictors, and Influence on Outcome. Neurocritical Care 2021, 34, 312–324. [Google Scholar] [CrossRef] [PubMed]
- McGinn, M.J.; Povlishock, J.T. Pathophysiology of Traumatic Brain Injury. Neurosurg. Clin. North Am. 2016, 27, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Cepeda, S.; Gómez, P.A.; Castaño-Leon, A.M.; Munarriz, P.M.; Paredes, I.; Lagares, A. Contrecoup Traumatic Intracerebral Hemorrhage: A Geometric Study of the Impact Site and Association with Hemorrhagic Progression. J. Neurotrauma 2016, 33, 1034–1046. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Malik, A.A.; Adil, M.M.; Defillo, A.; Sherr, G.T.; Suri, M.F. Hematoma Enlargement Among Patients with Traumatic Brain Injury: Analysis of a Prospective Multicenter Clinical Trial. J. Vasc. Interv. Neurol. 2015, 8, 42–49. [Google Scholar]
- Iaccarino, C.; Schiavi, P.; Picetti, E.; Goldoni, M.; Cerasti, D.; Caspani, M.; Servadei, F. Patients with brain contusions: Predictors of outcome and relationship between radiological and clinical evolution. J. Neurosurg. 2014, 120, 908–918. [Google Scholar] [CrossRef]
- White, C.L.; Griffith, S.; Caron, J.L. Early progression of traumatic cerebral contusions: Characterization and risk factors. J. Trauma 2009, 67, 508–514, discussion 514–505. [Google Scholar] [CrossRef] [Green Version]
- Alahmadi, H.; Vachhrajani, S.; Cusimano, M.D. The natural history of brain contusion: An analysis of radiological and clinical progression. J. Neurosurg. 2010, 112, 1139–1145. [Google Scholar] [CrossRef]
- Chang, E.F.; Meeker, M.; Holland, M.C. Acute traumatic intraparenchymal hemorrhage: Risk factors for progression in the early post-injury period. Neurosurgery 2006, 58, 647–656. [Google Scholar] [CrossRef]
- Carnevale, J.A.; Segar, D.J.; Powers, A.Y.; Shah, M.; Doberstein, C.; Drapcho, B.; Morrison, J.F.; Williams, J.R.; Collins, S.; Monteiro, K.; et al. Blossoming contusions: Identifying factors contributing to the expansion of traumatic intracerebral hemorrhage. J. Neurosurg. 2018, 129, 1305–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, Y.R.; Basoor, A.; Jain, G.; Nelson, A. Expanding traumatic intracerebral contusion/hematoma. Neurol. India 2006, 54, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Rehman, L.; Afzal, A.; Aziz, H.F.; Akbar, S.; Abbas, A.; Rizvi, R. Radiological Parameters to Predict Hemorrhagic Progression of Traumatic Contusional Brain Injury. J. Neurosci. Rural. Pract. 2019, 10, 212–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allison, R.Z.; Nakagawa, K.; Hayashi, M.; Donovan, D.J.; Koenig, M.A. Derivation of a Predictive Score for Hemorrhagic Progression of Cerebral Contusions in Moderate and Severe Traumatic Brain Injury. Neurocritical Care 2017, 26, 80–86. [Google Scholar] [CrossRef]
- Sharma, M.; Mittal, R.S.; Sharma, A.; Gandhi, A. Posttraumatic Contusion: Clinical and Radiologic Factors for Progression in Early Postinjury Period. Indian J. Neurotrauma 2016, 13, 1–6. [Google Scholar]
- Wan, X.; Fan, T.; Wang, S.; Zhang, S.; Liu, S.; Yang, H.; Shu, K.; Lei, T. Progressive hemorrhagic injury in patients with traumatic intracerebral hemorrhage: Characteristics, risk factors and impact on management. Acta Neurochir. 2017, 159, 227–235. [Google Scholar] [CrossRef]
- Cepeda, S.; Gómez, P.A.; Castaño-Leon, A.M.; Martínez-Pérez, R.; Munarriz, P.M.; Lagares, A. Traumatic Intracerebral Hemorrhage: Risk Factors Associated with Progression. J. Neurotrauma 2015, 32, 1246–1253. [Google Scholar] [CrossRef]
- Rogers, W.; Thulasi Seetha, S.; Refaee, T.A.G.; Lieverse, R.I.Y.; Granzier, R.W.Y.; Ibrahim, A.; Keek, S.A.; Sanduleanu, S.; Primakov, S.P.; Beuque, M.P.L.; et al. Radiomics: From qualitative to quantitative imaging. Br. J. Radiol. 2020, 93, 20190948. [Google Scholar] [CrossRef]
- Xie, H.; Ma, S.; Wang, X.; Zhang, X. Noncontrast computer tomography-based radiomics model for predicting intracerebral hemorrhage expansion: Preliminary findings and comparison with conventional radiological model. Eur. Radiol. 2020, 30, 87–98. [Google Scholar] [CrossRef]
- Xu, W.; Ding, Z.; Shan, Y.; Chen, W.; Feng, Z.; Pang, P.; Shen, Q. A Nomogram Model of Radiomics and Satellite Sign Number as Imaging Predictor for Intracranial Hematoma Expansion. Front. Neurosci. 2020, 14, 491. [Google Scholar] [CrossRef]
- Chen, Q.; Zhu, D.; Liu, J.; Zhang, M.; Xu, H.; Xiang, Y.; Zhan, C.; Zhang, Y.; Huang, S.; Yang, Y. Clinical-radiomics Nomogram for Risk Estimation of Early Hematoma Expansion after Acute Intracerebral Hemorrhage. Acad. Radiol. 2021, 28, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Pszczolkowski, S.; Manzano-Patrón, J.P.; Law, Z.K.; Krishnan, K.; Ali, A.; Bath, P.M.; Sprigg, N.; Dineen, R.A. Quantitative CT radiomics-based models for prediction of haematoma expansion and poor functional outcome in primary intracerebral haemorrhage. Eur. Radiol. 2021, 31, 7945–7959. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Guo, D.; Tang, Z.; Liu, H.; Li, X.; Luo, S.; Yao, X.; Song, W.; Song, J.; Zhou, Z. Noncontrast Computed Tomography-Based Radiomics Analysis in Discriminating Early Hematoma Expansion after Spontaneous Intracerebral Hemorrhage. Korean J. Radiol. 2021, 22, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.P.; Qureshi, A.I.; Jain, A.; Tharmaseelan, H.; Berson, E.R.; Zeevi, T.; Majidi, S.; Filippi, C.G.; Iseke, S.; Gross, M.; et al. Admission computed tomography radiomic signatures outperform hematoma volume in predicting baseline clinical severity and functional outcome in the ATACH-2 trial intracerebral hemorrhage population. Eur. J. Neurol. 2021, 28, 2989–3000. [Google Scholar] [CrossRef]
- Nawabi, J.; Kniep, H.; Elsayed, S.; Friedrich, C.; Sporns, P.; Rusche, T.; Böhmer, M.; Morotti, A.; Schlunk, F.; Dührsen, L.; et al. Imaging-Based Outcome Prediction of Acute Intracerebral Hemorrhage. Transl. Stroke Res. 2021, 12, 958–967. [Google Scholar] [CrossRef]
- Song, Z.; Tang, Z.; Liu, H.; Guo, D.; Cai, J.; Zhou, Z. A clinical-radiomics nomogram may provide a personalized 90-day functional outcome assessment for spontaneous intracerebral hemorrhage. Eur. Radiol. 2021, 31, 4949–4959. [Google Scholar] [CrossRef]
- Xu, X.; Zhang, J.; Yang, K.; Wang, Q.; Chen, X.; Xu, B. Prognostic prediction of hypertensive intracerebral hemorrhage using CT radiomics and machine learning. Brain Behav. 2021, 11, e02085. [Google Scholar] [CrossRef]
- Zhan, C.; Chen, Q.; Zhang, M.; Xiang, Y.; Chen, J.; Zhu, D.; Chen, C.; Xia, T.; Yang, Y. Radiomics for intracerebral hemorrhage: Are all small hematomas benign? Br. J. Radiol. 2021, 94, 20201047. [Google Scholar] [CrossRef]
- Zhang, L.; Zhuang, Q.; Wu, G.; Yu, J.; Shi, Z.; Yuan, Q.; Yu, J.; Hu, J. Combined Radiomics Model for Prediction of Hematoma Progression and Clinical Outcome of Cerebral Contusions in Traumatic Brain Injury. Neurocritical Care 2021, 36, 441–451. [Google Scholar] [CrossRef]
- Sheng, J.; Chen, W.; Zhuang, D.; Li, T.; Yang, J.; Cai, S.; Chen, X.; Liu, X.; Tian, F.; Huang, M.; et al. A Clinical Predictive Nomogram for Traumatic Brain Parenchyma Hematoma Progression. Neurol. Ther. 2022, 11, 185–203. [Google Scholar] [CrossRef]
- Cicchetti, D. Guidelines, Criteria, and Rules of Thumb for Evaluating Normed and Standardized Assessment Instrument in Psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Lohmann, P.; Bousabarah, K.; Hoevels, M.; Treuer, H. Radiomics in radiation oncology-basics, methods, and limitations. Strahlenther. Onkol. 2020, 196, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Arba, F.; Boulouis, G.; Charidimou, A. Noncontrast CT markers of intracerebral hemorrhage expansion and poor outcome: A meta-analysis. Neurology 2020, 95, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Lustenberger, T.; Kern, M.; Relja, B.; Wutzler, S.; Störmann, P.; Marzi, I. The effect of brain injury on the inflammatory response following severe trauma. Immunobiology 2016, 221, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Melamed, E.; Lavy, S.; Bentin, S.; Cooper, G.; Rinot, Y. Reduction in regional cerebral blood flow during normal aging in man. Stroke 1980, 11, 31–35. [Google Scholar] [CrossRef] [Green Version]
- Park, J.E.; Kim, S.H.; Yoon, S.H.; Cho, K.G.; Kim, S.H. Risk Factors Predicting Unfavorable Neurological Outcome during the Early Period after Traumatic Brain Injury. J. Korean Neurosurg. Soc. 2009, 45, 90–95. [Google Scholar] [CrossRef]
- McIntyre, A.; Mehta, S.; Aubut, J.; Dijkers, M.; Teasell, R.W. Mortality among older adults after a traumatic brain injury: A meta-analysis. Brain Inj. 2013, 27, 31–40. [Google Scholar] [CrossRef]
- Ostermann, R.C.; Joestl, J.; Tiefenboeck, T.M.; Lang, N.; Platzer, P.; Hofbauer, M. Risk factors predicting prognosis and outcome of elderly patients with isolated traumatic brain injury. J. Orthop. Surg. Res. 2018, 13, 277. [Google Scholar] [CrossRef] [Green Version]
- Kinoshita, K. Traumatic brain injury: Pathophysiology for neurocritical care. J. Intensive Care 2016, 4, 29. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Dong, B.; Mao, Y.; Guan, W.; Cao, J.; Zhu, R.; Wang, S. Review: Traumatic brain injury and hyperglycemia, a potentially modifiable risk factor. Oncotarget 2016, 7, 71052–71061. [Google Scholar] [CrossRef] [Green Version]
- Hermanides, J.; Plummer, M.P.; Finnis, M.; Deane, A.M.; Coles, J.P.; Menon, D.K. Glycaemic control targets after traumatic brain injury: A systematic review and meta-analysis. Crit. Care 2018, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, M.; Newcombe, V.F.J.; Mathieu, F.; Adatia, K.; Kamnitsas, K.; Ferrante, E.; Das, T.; Whitehouse, D.; Rueckert, D.; Menon, D.K.; et al. Multiclass semantic segmentation and quantification of traumatic brain injury lesions on head CT using deep learning: An algorithm development and multicentre validation study. Lancet Digit. Health 2020, 2, e314–e322. [Google Scholar] [CrossRef]
- Phaphuangwittayakul, A.; Guo, Y.; Ying, F.; Dawod, A.Y.; Angkurawaranon, S.; Angkurawaranon, C. An optimal deep learning framework for multi-type hemorrhagic lesions detection and quantification in head CT images for traumatic brain injury. Appl. Intell. 2022, 52, 7320–7338. [Google Scholar] [CrossRef] [PubMed]
- Inkeaw, P.; Angkurawaranon, S.; Khumrin, P.; Inmutto, N.; Traisathit, P.; Chaijaruwanich, J.; Angkurawaranon, C.; Chitapanarux, I. Automatic hemorrhage segmentation on head CT scan for traumatic brain injury using 3D deep learning model. Comput. Biol. Med. 2022, 146, 105530. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HPC | |||
|---|---|---|---|
| No (n = 62) | Yes (n = 45) | p-Value | |
| Age (years), mean ± SD | 52.82 ± 20.50 | 55.89 ± 18.31 | 0.426 |
| <45 | 21 (33.87) | 10 (22.22) | 0.404 |
| 45–65 | 22 (35.48) | 18 (40.00) | |
| ≥65 | 19 (30.65) | 17 (37.78) | |
| Sex, male (%) | 42 (67.74) | 32 (71.11) | 0.833 |
| Injury—Falling | 25 (40.32) | 18 (40.00) | 1.000 |
| Injury—Motor vehicle collision | 37 (59.68) | 27 (60.00) | |
| IPH volume (cc), mean ± SD | 5.79 ± 8.19 | 11.32 ± 11.82 | 0.009 * |
| Multiple IPH, n (%) | 37 (59.68) | 34 (75.56) | 0.100 |
| EDH, n (%) | 17 (27.42) | 9 (20.00) | 0.494 |
| SDH, n (%) | 41 (66.13) | 37 (82.22) | 0.080 |
| SAH, n (%) | 50 (80.65) | 41 (91.11) | 0.174 |
| IVH, n (%) | 8 (12.90) | 5 (11.11) | 1.000 |
| PLT (count/μL), mean ± SD | 239.52 ± 81.91 | 217.09 ± 56.28 | 0.096 |
| <150 K | 8 (12.90) | 5 (11.11) | 1.000 |
| ≥150 K | 54 (87.10) | 40 (88.89) | |
| Antiplatelet usage, n (%) | 5 (8.06) | 4 (8.89) | 1.000 |
| INR, mean ± SD | 1.00 ± 0.13 | 1.02 ± 0.09 | 0.468 |
| <1.05 | 53 (85.48) | 31 (68.89) | 0.056 |
| ≥1.05 | 9 (14.52) | 14 (31.11) | |
| APTT ratio, mean ± SD | 0.93 ± 0.11 | 0.93 ± 0.12 | 0.922 |
| <1.05 | 54 (87.10) | 39 (86.67) | 1.000 |
| ≥1.05 | 8 (12.90) | 6 (13.33) | |
| SBP at ER (mmHg), mean ± SD | 149.65 ± 32.87 | 156.51 ± 34.25 | 0.297 |
| <180 | 51 (82.26) | 33 (73.33) | 0.342 |
| ≥180 | 11 (17.74) | 12 (26.67) | |
| GCS at ER, mean ± SD | 12.23 ± 3.25 | 11.31 ± 3.65 | 0.175 |
| <9 | 10 (16.13) | 11 (24.44) | 0.422 |
| 9–14 | 19 (30.65) | 15 (33.33) | |
| ≥14 | 33 (53.23) | 19 (42.22) | |
| ISS score, mean ± SD | 21.47 ± 10.45 | 25.24 ± 11.35 | 0.078 |
| <16 | 9 (14.52) | 4 (8.89) | 0.009 * |
| 16–25 | 33 (53.23) | 13 (28.89) | |
| ≥25 | 20 (32.26) | 28 (62.22) | |
| HTN, n (%) | 14 (22.58) | 14 (31.11) | 0.376 |
| DM, n (%) | 9 (14.52) | 10 (22.22) | 0.318 |
| GOS | |||
| Good (4–5) (n = 56) | Poor (1–3) (n = 51) | p-Value | |
| Age (years), mean ± SD | 46.16 ± 17.90 | 62.84 ± 17.65 | <0.001 * |
| <45 | 24 (42.86) | 7 (13.73) | <0.001 * |
| 45–65 | 25 (44.64) | 15 (29.41) | |
| ≥65 | 7 (12.50) | 29 (56.86) | |
| Sex, male (%) | 36 (64.29) | 38 (74.51) | 0.298 |
| Injury—Falling | 16 (28.57) | 27 (52.94) | 0.017 * |
| Injury—Motor vehicle collision | 40 (71.43) | 24 (47.06) | |
| IPH volume (cc), mean ± SD | 6.15 ± 7.01 | 10.28 ± 12.56 | 0.042 * |
| Multiple IPH, n (%) | 33 (58.93) | 38 (74.51) | 0.104 |
| EDH, n (%) | 16 (28.57) | 10 (19.61) | 0.368 |
| SDH, n (%) | 38 (67.86) | 40 (78.43) | 0.278 |
| SAH, n (%) | 42 (75.00) | 49 (96.08) | 0.002 * |
| IVH, n (%) | 2 (3.57) | 11 (21.57) | 0.006 * |
| PLT (count/μL), mean ± SD | 234.71 ± 65.50 | 225.00 ± 80.41 | 0.493 |
| <150 K | 3 (5.36) | 10 (19.61) | 0.036 * |
| ≥150 K | 53 (94.64) | 41 (80.39) | |
| Antiplatelet usage, n (%) | 2 (3.57) | 7 (13.73) | 0.083 |
| INR, mean ± SD | 0.98 ± 0.05 | 1.04 ± 0.15 | 0.006 * |
| <1.05 | 51 (91.07) | 33 (64.71) | 0.002 * |
| ≥1.05 | 5 (8.93) | 18 (35.29) | |
| APTT ratio, mean ± SD | 0.90 ± 0.09 | 0.97 ± 0.13 | 0.004 * |
| <1.05 | 52 (92.86) | 41 (80.39) | 0.084 |
| ≥1.05 | 4 (7.14) | 10 (19.61) | |
| SBP at ER (mmHg), mean ± SD | 149.16 ± 26.70 | 156.24 ± 39.55 | 0.286 |
| <180 | 47 (83.93) | 37 (72.55) | 0.166 |
| ≥180 | 9 (16.07) | 14 (27.45) | |
| GCS at ER, mean ± SD | 12.95 ± 2.56 | 10.63 ± 3.87 | <0.001 * |
| <9 | 5 (8.93) | 16 (31.37) | 0.007 * |
| 9–14 | 18 (32.14) | 16 (31.37) | |
| ≥14 | 33 (58.93) | 19 (37.25) | |
| ISS score, mean ± SD | 19.16 ± 7.31 | 27.33 ± 12.63 | <0.001 * |
| <16 | 10 (17.86) | 3 (5.88) | <0.001 * |
| 16–25 | 32 (57.14) | 14 (27.45) | |
| ≥25 | 14 (25.00) | 34 (66.67) | |
| HTN, n (%) | 5 (8.93) | 23 (45.10) | <0.001 * |
| DM, n (%) | 7 (12.50) | 12 (23.53) | 0.205 |
| AUC | Accuracy | Sensitivity | Specificity | |
|---|---|---|---|---|
| R-score for hemorrhagic progression | 0.7638 | 0.7757 | 0.6222 | 0.8871 |
| R-score for poor outcome (GOS 1–3) | 0.8067 | 0.7664 | 0.7647 | 0.7679 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, Y.-J.; Liu, Y.-L.; Chen, J.-H.; Ho, C.-H.; Yang, C.-C.; Chen, T.-Y.; Wu, T.-C.; Ko, C.-C.; Zhou, J.T.; Zhang, Y.; et al. Prediction of Intraparenchymal Hemorrhage Progression and Neurologic Outcome in Traumatic Brain Injury Patients Using Radiomics Score and Clinical Parameters. Diagnostics 2022, 12, 1677. https://doi.org/10.3390/diagnostics12071677
Shih Y-J, Liu Y-L, Chen J-H, Ho C-H, Yang C-C, Chen T-Y, Wu T-C, Ko C-C, Zhou JT, Zhang Y, et al. Prediction of Intraparenchymal Hemorrhage Progression and Neurologic Outcome in Traumatic Brain Injury Patients Using Radiomics Score and Clinical Parameters. Diagnostics. 2022; 12(7):1677. https://doi.org/10.3390/diagnostics12071677
Chicago/Turabian StyleShih, Yun-Ju, Yan-Lin Liu, Jeon-Hor Chen, Chung-Han Ho, Cheng-Chun Yang, Tai-Yuan Chen, Te-Chang Wu, Ching-Chung Ko, Jonathan T. Zhou, Yang Zhang, and et al. 2022. "Prediction of Intraparenchymal Hemorrhage Progression and Neurologic Outcome in Traumatic Brain Injury Patients Using Radiomics Score and Clinical Parameters" Diagnostics 12, no. 7: 1677. https://doi.org/10.3390/diagnostics12071677