
Diagnostic Yield of Xpert MTB/RIF Assay Using Bronchoalveolar Lavage Fluid in Detecting Mycobacterium tuberculosis among the Sputum-Scarce Suspected Pulmonary TB Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
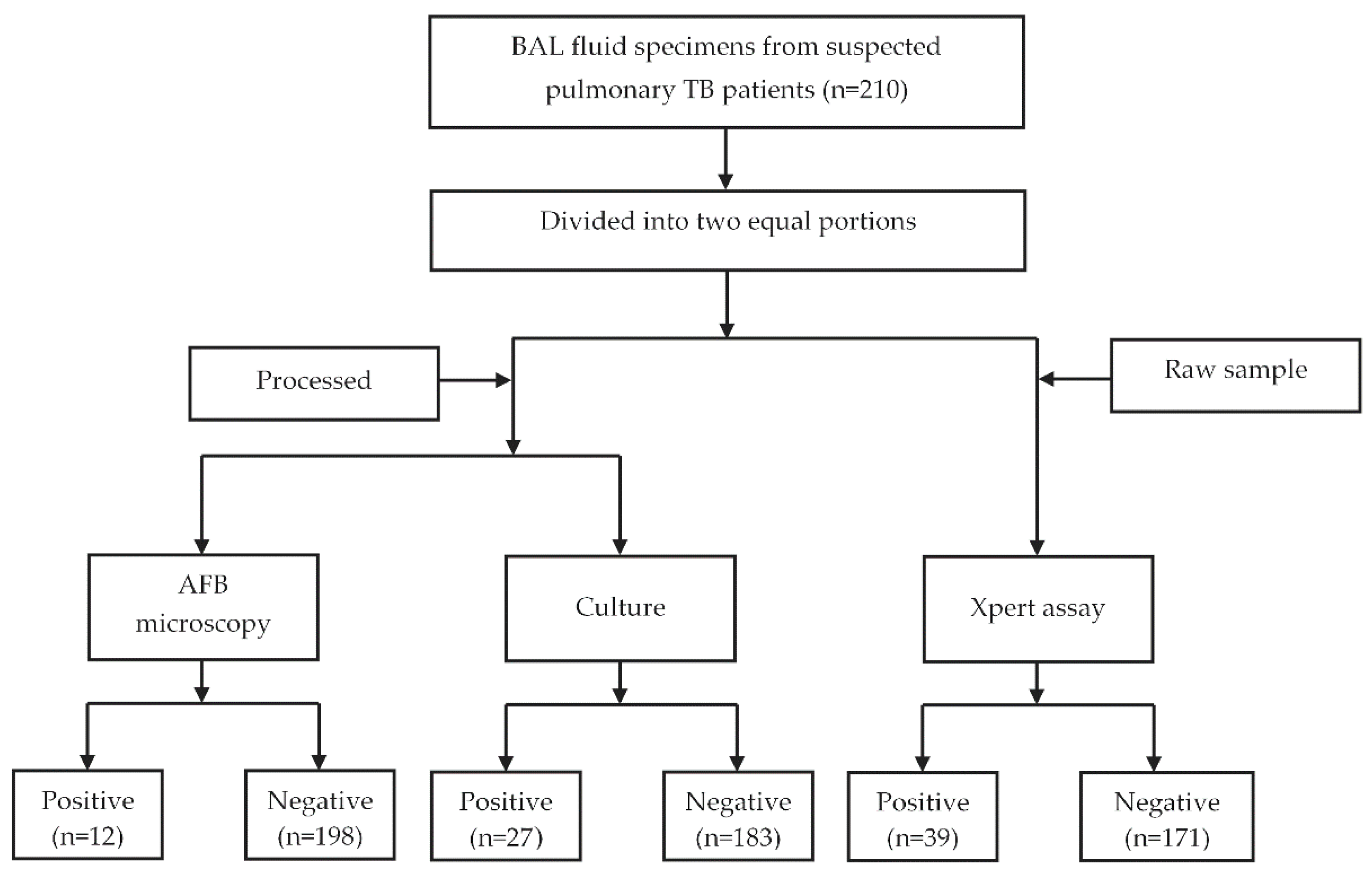
2.1. Specimen Collection
2.2. Specimen Processing
2.3. Culture and AFB Microscopy
2.4. Insertion Sequence 6110 (IS6110) PCR
2.5. Xpert MTB/RIF Assay
2.6. Data Analysis
3. Results
3.1. Demographic Characteristics and Clinical Presentations of the Enrolled Patients
3.2. Diagnostic Performances of Different Tests Methods
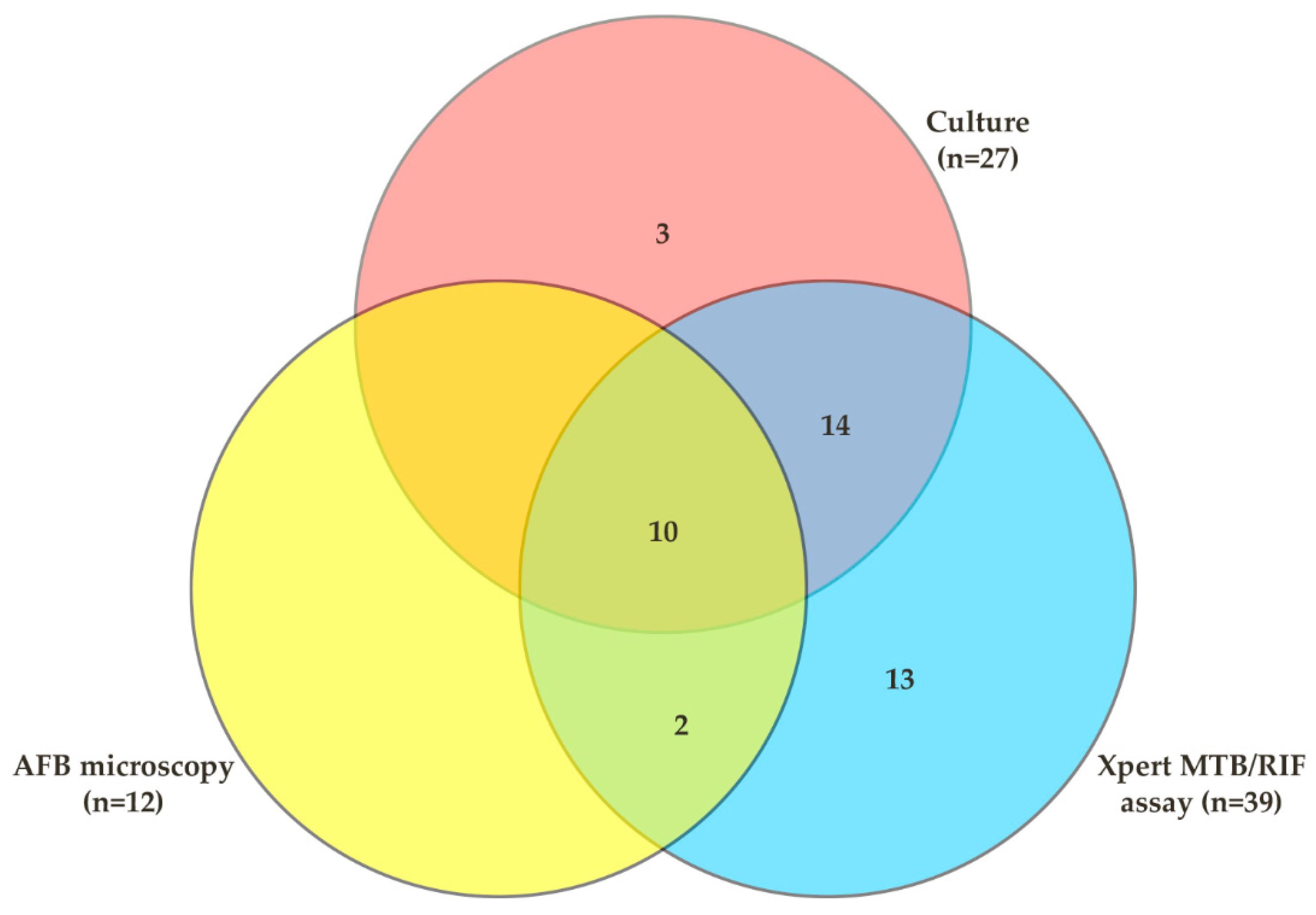
3.3. Comparative Analysis of Different Test Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Tuberculosis Report. 2021. Available online: https://www.who.int/publications/i/item/9789240037021 (accessed on 20 February 2022).
- WHO. Global Tuberculosis Report. 2020. Available online: https://www.who.int/publications/i/item/9789240013131 (accessed on 28 January 2022).
- WHO. Global Tuberculosis Report. 2019. Available online: https://www.who.int/publications/i/item/9789241565714 (accessed on 10 February 2022).
- Van Cutsem, G.; Isaakidis, P.; Farley, J.; Nardell, E.; Volchenkov, G.; Cox, H. Infection control for drug-resistant tuberculosis: Early diagnosis and treatment is the key. Clin. Infect. Dis. 2016, 62, S238–S243. [Google Scholar] [CrossRef] [Green Version]
- Mathew, P.; Kuo, Y.-H.; Vazirani, B.; Eng, R.H.; Weinstein, M.P. Are three sputum acid-fast bacillus smears necessary for discontinuing tuberculosis isolation? J. Clin. Microbiol. 2002, 40, 3482–3484. [Google Scholar]
- Uddin, M.K.M.; Chowdhury, M.R.; Ahmed, S.; Rahman, M.T.; Khatun, R.; van Leth, F.; Banu, S. Comparison of direct versus concentrated smear microscopy in detection of pulmonary tuberculosis. BMC Res. Notes 2013, 6, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, P.; Pai, M. The diagnosis and misdiagnosis of tuberculosis [State of the art series. Tuberculosis. Edited by ID Rusen. Number 1 in the series]. Int. J. Tuberc. Lung Dis. 2008, 12, 1226–1234. [Google Scholar]
- Agrawal, M.; Bajaj, A.; Bhatia, V.; Dutt, S. Comparative study of GeneXpert with ZN stain and culture in samples of suspected pulmonary tuberculosis. J. Clin. Diagn. Res. JCDR 2016, 10, DC09. [Google Scholar] [CrossRef]
- Zeka, A.N.; Tasbakan, S.; Cavusoglu, C. Evaluation of the GeneXpert MTB/RIF assay for rapid diagnosis of tuberculosis and detection of rifampin resistance in pulmonary and extrapulmonary specimens. J. Clin. Microbiol. 2011, 49, 4138–4141. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Updated guidelines for the use of nucleic acid amplification tests in the diagnosis of tuberculosis. Morb. Mortal. Wkly. Rep. 2009, 58, 7–10. [Google Scholar]
- Bajrami, R.; Mulliqi, G.; Kurti, A.; Lila, G.; Raka, L. Comparison of GeneXpert MTB/RIF and conventional methods for the diagnosis of tuberculosis in Kosovo. J. Infect. Dev. Ctries. 2016, 10, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Raviglione, M.; Marais, B.; Floyd, K.; Lönnroth, K.; Getahun, H.; Migliori, G.B.; Harries, A.D.; Nunn, P.; Lienhardt, C.; Graham, S.; et al. Scaling up interventions to achieve global tuberculosis control: Progress and new developments. Lancet 2012, 379, 1902–1913. [Google Scholar] [CrossRef]
- Uddin, M.K.M.; Rahman, A.; Ather, M.F.; Ahmed, T.; Rahman, S.M.M.; Ahmed, S.; Banu, S. Distribution and Frequency of rpoB Mutations Detected by Xpert MTB/RIF Assay Among Beijing and Non-Beijing Rifampicin Resistant Mycobacterium tuberculosis Isolates in Bangladesh. Infect. Drug Resist. 2020, 13, 789–797. [Google Scholar] [CrossRef] [Green Version]
- Pai, M.; Minion, J.; Sohn, H.; Zwerling, A.; Perkins, M.D. Novel and improved technologies for tuberculosis diagnosis: Progress and challenges. Clin. Chest Med. 2009, 30, 701–716. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB; 9241506334; World Health Organization: Geneva, Switzerland, 2013.
- Norrman, E.; Keistinen, T.; Uddenfeldt, M.; Rydström, P.-O.; Lundgren, R. Bronchoalveolar lavage is better than gastric lavage in the diagnosis of pulmonary tuberculosis. Scand. J. Infect. Dis. 1988, 20, 77–80. [Google Scholar] [CrossRef]
- Dickson, S.J.; Brent, A.; Davidson, R.N.; Wall, R. Comparison of bronchoscopy and gastric washings in the investigation of smear-negative pulmonary tuberculosis. Clin. Infect. Dis. 2003, 37, 1649–1653. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Kwon, B.; Lim, S.; Lee, Y.; Cho, Y.-J.; Yoon, H.; Lee, J.; Lee, C.-T.; Park, J. Diagnostic value of bronchoalveolar lavage and bronchial washing in sputum-scarce or smear-negative cases with suspected pulmonary tuberculosis: A randomized study. Clin. Microbiol. Infect. 2020, 26, 911–916. [Google Scholar] [CrossRef]
- Brown, M.; Varia, H.; Bassett, P.; Davidson, R.N.; Wall, R.; Pasvol, G. Prospective study of sputum induction, gastric washing, and bronchoalveolar lavage for the diagnosis of pulmonary tuberculosis in patients who are unable to expectorate. Clin. Infect. Dis. 2007, 44, 1415–1420. [Google Scholar] [CrossRef]
- Soo, P.-C.; Horng, Y.-T.; Hsueh, P.-R.; Shen, B.-J.; Wang, J.-Y.; Tu, H.-H.; Wei, J.-R.; Hsieh, S.-C.; Huang, C.-C.; Lai, H.-C. Direct and simultaneous identification of Mycobacterium tuberculosis complex (MTBC) and Mycobacterium tuberculosis (MTB) by rapid multiplex nested PCR-ICT assay. J. Microbiol. Methods 2006, 66, 440–448. [Google Scholar] [CrossRef]
- Uddin, M.K.M.; Ahmed, M.; Islam, M.R.; Rahman, A.; Khatun, R.; Hossain, M.A.; Maug, A.K.J.; Banu, S. Molecular characterization and drug susceptibility profile of Mycobacterium tuberculosis isolates from Northeast Bangladesh. Infect. Genet. Evol. 2018, 65, 136–143. [Google Scholar] [CrossRef]
- Narayanan, S.; Parandaman, V.; Narayanan, P.; Venkatesan, P.; Girish, C.; Mahadevan, S.; Rajajee, S. Evaluation of PCR using TRC4 and IS6110 primers in detection of tuberculous meningitis. J. Clin. Microbiol. 2001, 39, 2006. [Google Scholar] [CrossRef] [Green Version]
- Deng, Y.; Duan, Y.-F.; Gao, S.-P.; Wang, J.-M. Comparison of LAMP, GeneXpert, Mycobacterial Culture, Smear Microscopy, TSPOT. TB, TBAg/PHA Ratio for Diagnosis of Pulmonary Tuberculosis. Curr. Med. Sci. 2021, 41, 1023–1028. [Google Scholar] [CrossRef]
- Denkinger, C.M.; Schumacher, S.G.; Boehme, C.C.; Dendukuri, N.; Pai, M.; Steingart, K.R. Xpert MTB/RIF assay for the diagnosis of extrapulmonary tuberculosis: A systematic review and meta-analysis. Eur. Respir. J. 2014, 44, 435–446. [Google Scholar] [CrossRef] [Green Version]
- e Castro, A.T.; Mendes, M.; Freitas, S.; Roxo, P. Diagnostic yield of sputum microbiological analysis in the diagnosis of pulmonary tuberculosis in a period of 10 years. Rev. Port. Pneumol. 2015, 21, 185–191. [Google Scholar] [CrossRef]
- Worodria, W.; Davis, J.L.; Cattamanchi, A.; Andama, A.; Den Boon, S.; Yoo, S.D.; Hopewell, P.C.; Huang, L. Bronchoscopy is useful for diagnosing smear-negative tuberculosis in HIV-infected patients. Eur. Respir. J. 2010, 36, 446–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, P.R.; Lodha, R.; Singh, U.; Kabra, S.K. A prospective assessment of the role of bronchoscopy and bronchoalveolar lavage in evaluation of children with pulmonary tuberculosis. J. Trop. Pediatr. 2010, 57, 363–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnard, D.A.; Irusen, E.M.; Bruwer, J.W.; Plekker, D.; Whitelaw, A.C.; Deetlefs, J.D.; Koegelenberg, C.F. The utility of Xpert MTB/RIF performed on bronchial washings obtained in patients with suspected pulmonary tuberculosis in a high prevalence setting. BMC Pulm. Med. 2015, 15, 103. [Google Scholar] [CrossRef] [Green Version]
- Khalil, K.F.; Butt, T. Diagnostic yield of bronchoalveolar lavage gene Xpert in smear-negative and sputum-scarce pulmonary tuberculosis. J. Coll. Physicians Surg. Pak. 2015, 25, 115–118. [Google Scholar] [PubMed]
- Le Palud, P.; Cattoir, V.; Malbruny, B.; Magnier, R.; Campbell, K.; Oulkhouir, Y.; Zalcman, G.; Bergot, E. Retrospective observational study of diagnostic accuracy of the Xpert® MTB/RIF assay on fiberoptic bronchoscopy sampling for early diagnosis of smear-negative or sputum-scarce patients with suspected tuberculosis. BMC Pulm. Med. 2014, 14, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.Y.; Seong, M.-W.; Park, S.S.; Hwang, S.-S.; Lee, J.; Park, Y.S.; Lee, C.H.; Lee, S.-M.; Yoo, C.-G.; Kim, Y.W.; et al. Diagnostic accuracy of Xpert® MTB/RIF on bronchoscopy specimens in patients with suspected pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2013, 17, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Soneja, M.; Gowda, N.C.; Ray, A.; Khanna, A.; Sinha, S. Evaluation of Xpert® Mycobacterium tuberculosis/rifampin in sputum-smear negative and sputum-scarce patients with pulmonary tuberculosis using bronchoalveolar lavage fluid. Lung India Off. Organ Indian Chest Soc. 2018, 35, 295–300. [Google Scholar] [CrossRef]
- Dunlap, N.E.; Bass, J.; Fujiwara, P.; Hopewell, P.; Horsburgh, C.; Salfinger, M.; Simone, P. Diagnostic standards and classification of tuberculosis in adults and children. Am. J. Respir. Crit. Care Med. 2000, 161, 1376–1395. [Google Scholar]
- Helb, D.; Jones, M.; Story, E.; Boehme, C.; Wallace, E.; Ho, K.; Kop, J.; Owens, M.R.; Rodgers, R.; Banada, P. Rapid detection of Mycobacterium tuberculosis and rifampin resistance by use of on-demand, near-patient technology. J. Clin. Microbiol. 2010, 48, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Meyer, A.J.; Atuheire, C.; Worodria, W.; Kizito, S.; Katamba, A.; Sanyu, I.; Andama, A.; Ayakaka, I.; Cattamanchi, A.; Bwanga, F.; et al. Sputum quality and diagnostic performance of GeneXpert MTB/RIF among smear-negative adults with presumed tuberculosis in Uganda. PLoS ONE 2017, 12, e0180572. [Google Scholar] [CrossRef] [Green Version]
- Walters, E.; Goussard, P.; Bosch, C.; Hesseling, A.C.; Gie, R.P. GeneXpert MTB/RIF on bronchoalveolar lavage samples in children with suspected complicated intrathoracic tuberculosis: A pilot study. Pediatric Pulmonol. 2014, 49, 1133–1137. [Google Scholar] [CrossRef]
- Lawson, L.; Emenyonu, N.; Abdurrahman, S.T.; Lawson, J.O.; Uzoewulu, G.N.; Sogaolu, O.M.; Ebisike, J.N.; Parry, C.M.; Yassin, M.A.; Cuevas, L.E. Comparison of Mycobacterium tuberculosis drug susceptibility using solid and liquid culture in Nigeria. BMC Res. Notes 2013, 6, 215. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Categories | Numbers (n) | Frequency (%) | |
|---|---|---|---|
| Sex | Male | 140 | 66.7 |
| Female | 70 | 33.3 | |
| Age Ranges | 1–20 | 10 | 4.7 |
| 21–50 | 109 | 52 | |
| >50 | 91 | 43.3 | |
| TB History | Yes | 14 | 6.7 |
| No | 196 | 93.3 | |
| Diabetes | Yes | 31 | 14.8 |
| No | 179 | 85.2 | |
| Occupations | Service holders | 43 | 20.5 |
| Business | 18 | 8.5 | |
| Housewife | 43 | 20.5 | |
| Student | 17 | 8.1 | |
| Unemployed | 20 | 9.5 | |
| Others * | 69 | 32.9 | |
| Test Methods | Xpert Assay (n = 210) | AFB Microscopy (n = 210) | Culture (n = 210) | ||
|---|---|---|---|---|---|
| Positive | Negative | Positive | Negative | ||
| Test Results | Detected High-1 | 1 | 0 | 1 | 0 |
| Detected Medium-9 | 5 | 4 | 8 | 1 | |
| Detected Low-12 | 1 | 11 | 6 | 6 | |
| Detected Very Low-17 | 5 | 12 | 9 | 8 | |
| Not Detected-171 | 0 | 171 | 3 | 168 | |
| Frequency to Positivity | 18.6% | 5.7% | 12.8% | ||
| Variables (95% CI) | Compared to Culture (n = 27) | Compared to CRS (n = 42) | |||
|---|---|---|---|---|---|
| Xpert MTB/RIF Assay | AFB Microscopy | Xpert MTB/RIF Assay | Culture | AFB Microscopy | |
| TB Positive Cases (n) | 24 | 10 | 39 | 27 | 12 |
| Sensitivity | 88.9 * (70.8–97.6) | 37.0 (19.4–57.6) | 92.9 † (80.5–98.5) | 64.3 (48.0–78.4) | 28.6 ‡ (15.7–44.6) |
| Specificity | 91.8 (86.8–95.3) | 98.9 (96.1–99.9) | 100 (97.8–100.0) | 100 (97.8–100.0) | 100 (97.8–100.0) |
| PPV | 61.5 (44.6–76.6) | 83.3 (51.6–97.9) | 100 (91.0–100.0) | 100 (87.2–100.0) | 100 (73.5–100.0) |
| NPV | 98.2 (95.06–99.6) | 91.4 (86.6–94.9) | 98.2 (95.0–99.6) | 91.8 (86.8–95.3) | 84.8 (79.1–89.5) |
| Variables | Compared to Culture (n = 27) | Compared to CRS (n = 42) | |||
|---|---|---|---|---|---|
| Xpert MTB/RIF Assay | AFB Microscopy | Xpert MTB/RIF Assay | Culture | AFB Microscopy | |
| AUC | 0.904 | 0.698 | 0.964 | 0.821 | 0.655 |
| Standard error | 0.033 | 0.048 | 0.02 | 0.037 | 0.036 |
| p value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| 95% CI * | 0.840–0.967 | 0.640–0.793 | 0.925–1.000 | 0.748–0.895 | 0.548–0.726 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uddin, M.K.M.; Ather, M.F.; Akter, S.; Nasrin, R.; Rahman, T.; Kabir, S.N.; Rahman, S.M.M.; Pouzol, S.; Hoffmann, J.; Banu, S. Diagnostic Yield of Xpert MTB/RIF Assay Using Bronchoalveolar Lavage Fluid in Detecting Mycobacterium tuberculosis among the Sputum-Scarce Suspected Pulmonary TB Patients. Diagnostics 2022, 12, 1676. https://doi.org/10.3390/diagnostics12071676
Uddin MKM, Ather MF, Akter S, Nasrin R, Rahman T, Kabir SN, Rahman SMM, Pouzol S, Hoffmann J, Banu S. Diagnostic Yield of Xpert MTB/RIF Assay Using Bronchoalveolar Lavage Fluid in Detecting Mycobacterium tuberculosis among the Sputum-Scarce Suspected Pulmonary TB Patients. Diagnostics. 2022; 12(7):1676. https://doi.org/10.3390/diagnostics12071676
Chicago/Turabian StyleUddin, Mohammad Khaja Mafij, Md. Fahim Ather, Sharmin Akter, Rumana Nasrin, Tanjina Rahman, Sk Nazmul Kabir, S. M. Mazidur Rahman, Stephane Pouzol, Jonathan Hoffmann, and Sayera Banu. 2022. "Diagnostic Yield of Xpert MTB/RIF Assay Using Bronchoalveolar Lavage Fluid in Detecting Mycobacterium tuberculosis among the Sputum-Scarce Suspected Pulmonary TB Patients" Diagnostics 12, no. 7: 1676. https://doi.org/10.3390/diagnostics12071676