
Quantitative Assessment of the Restoration of Original Anatomy after 3D Virtual Reduction of Long Bone Fractures

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
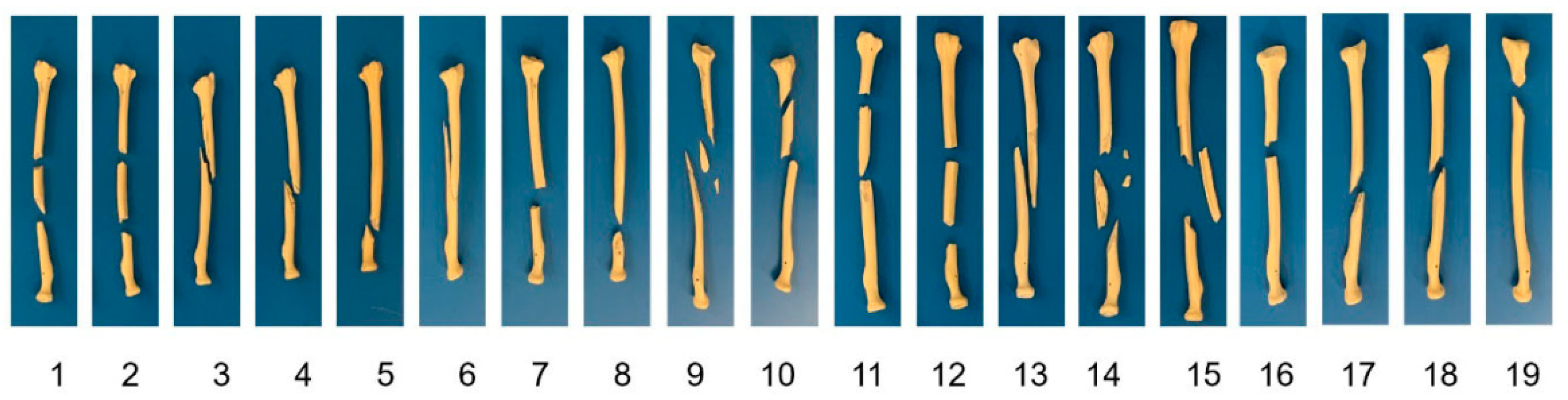
2.1. Material Preparation and CT Scanning
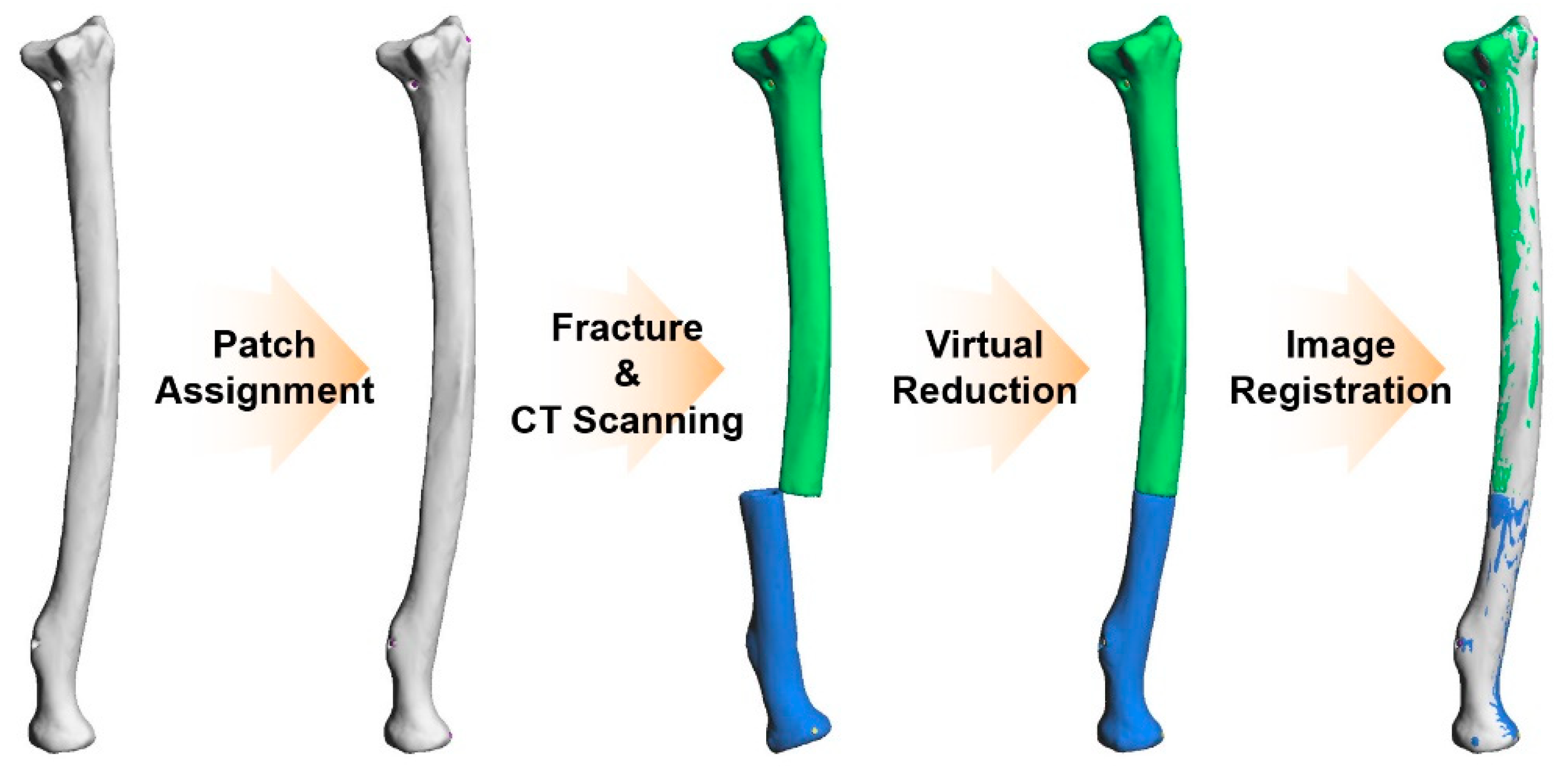
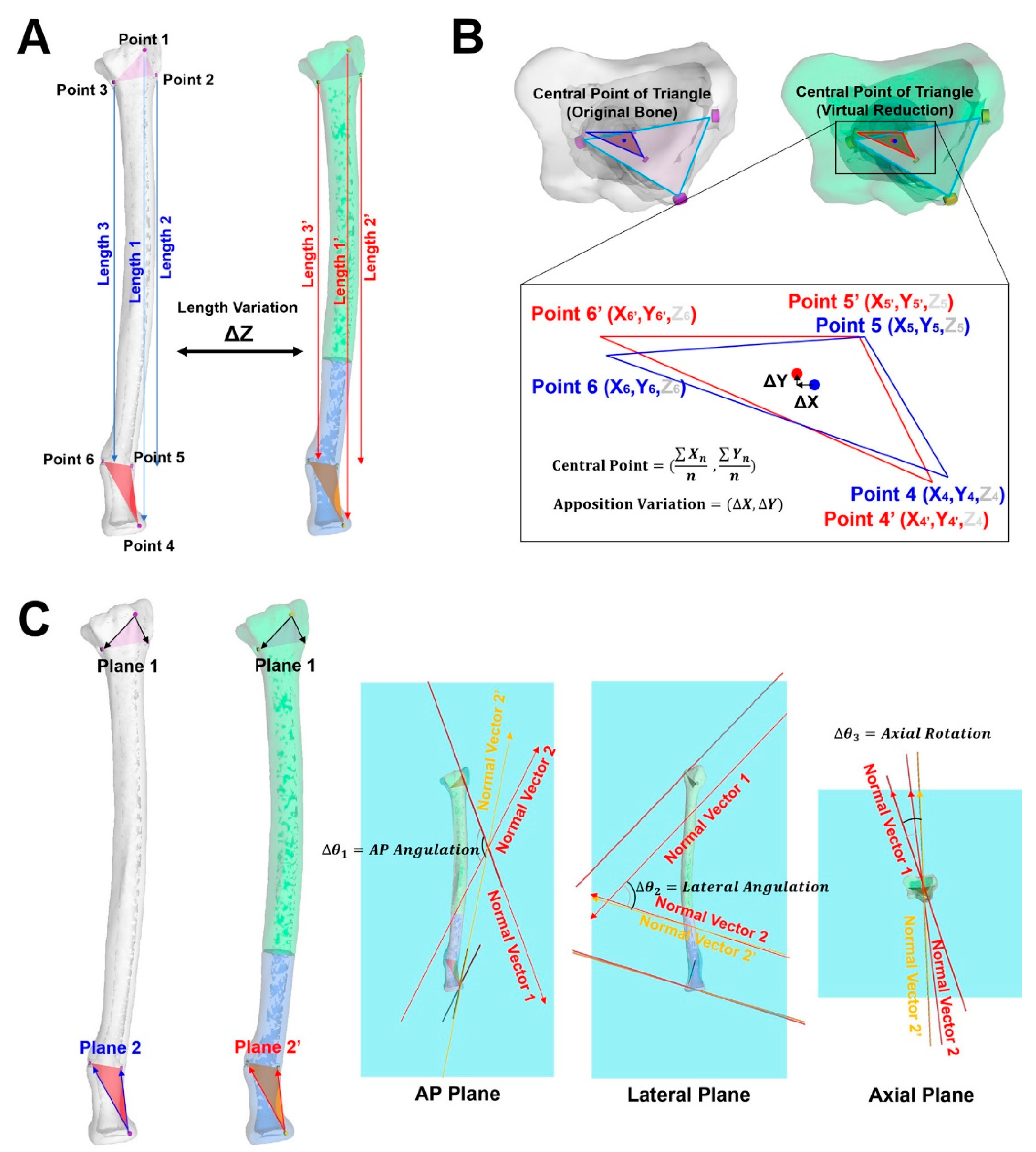
2.2. Virtual Reduction and Accuracy Evaluation
2.3. Statistical Analysis
3. Results
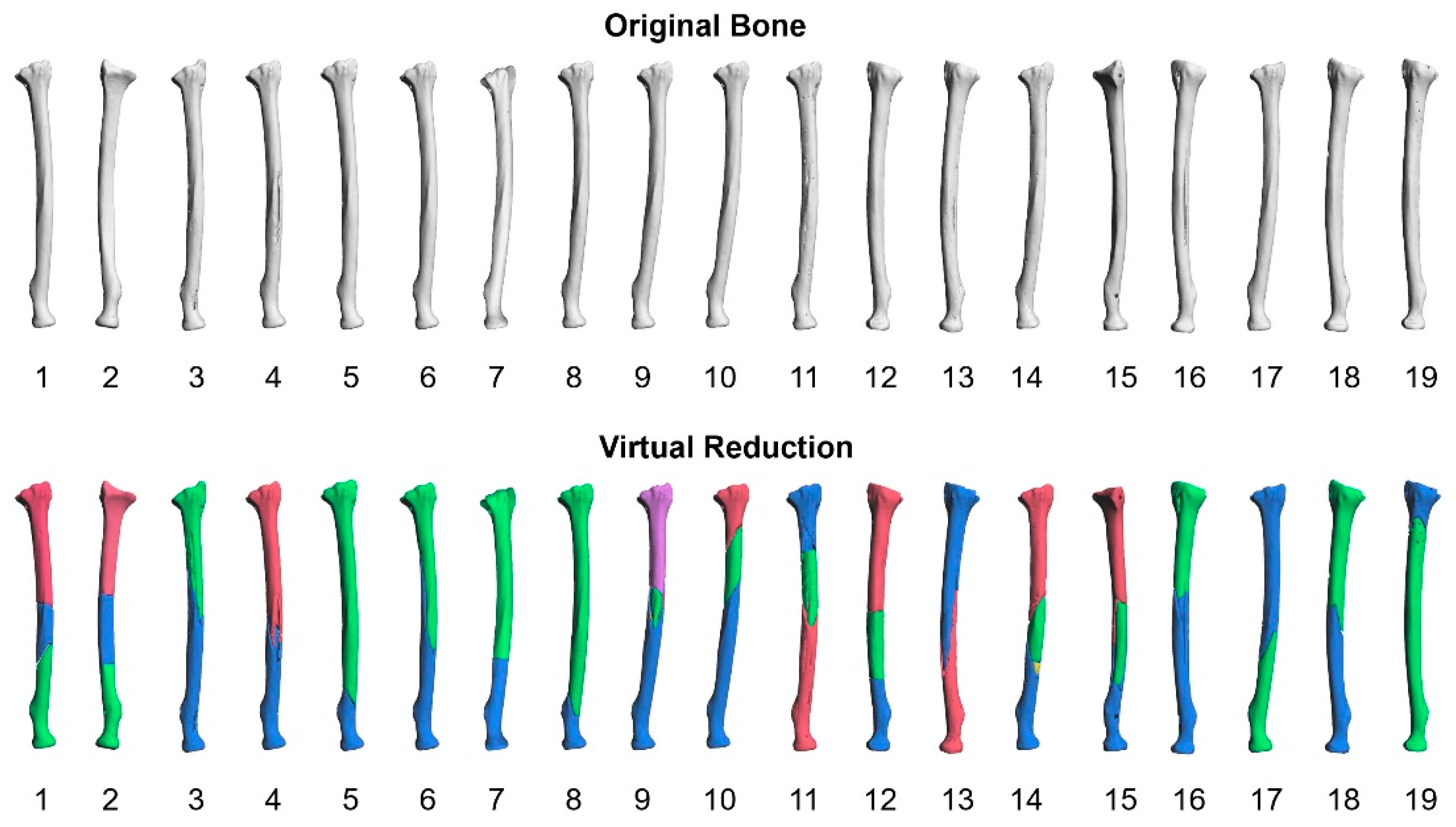
3.1. Ultimate Shape of the Virtual Reduction
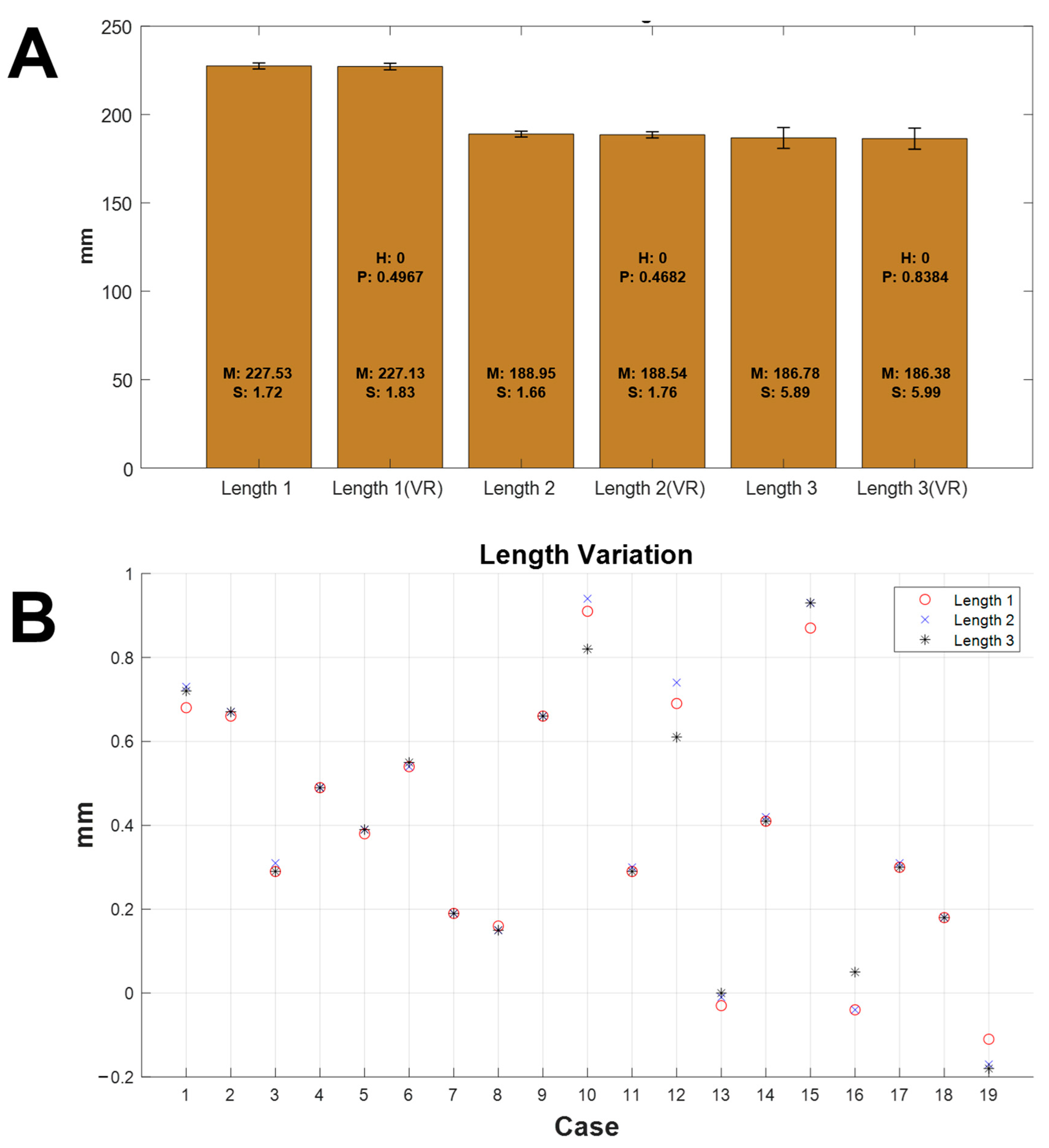
3.2. Length Variation
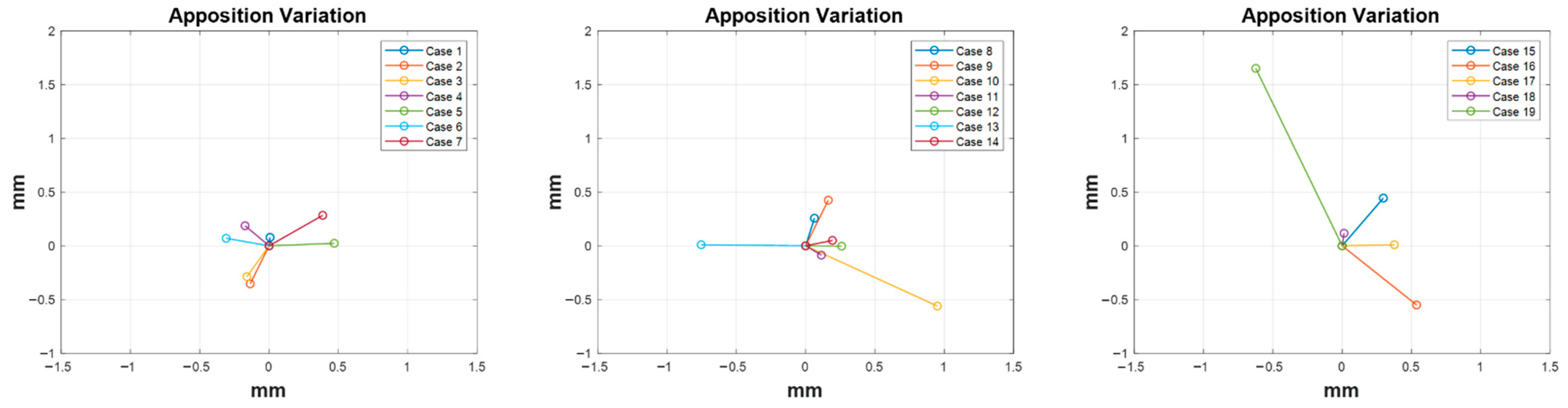
3.3. Apposition Variation
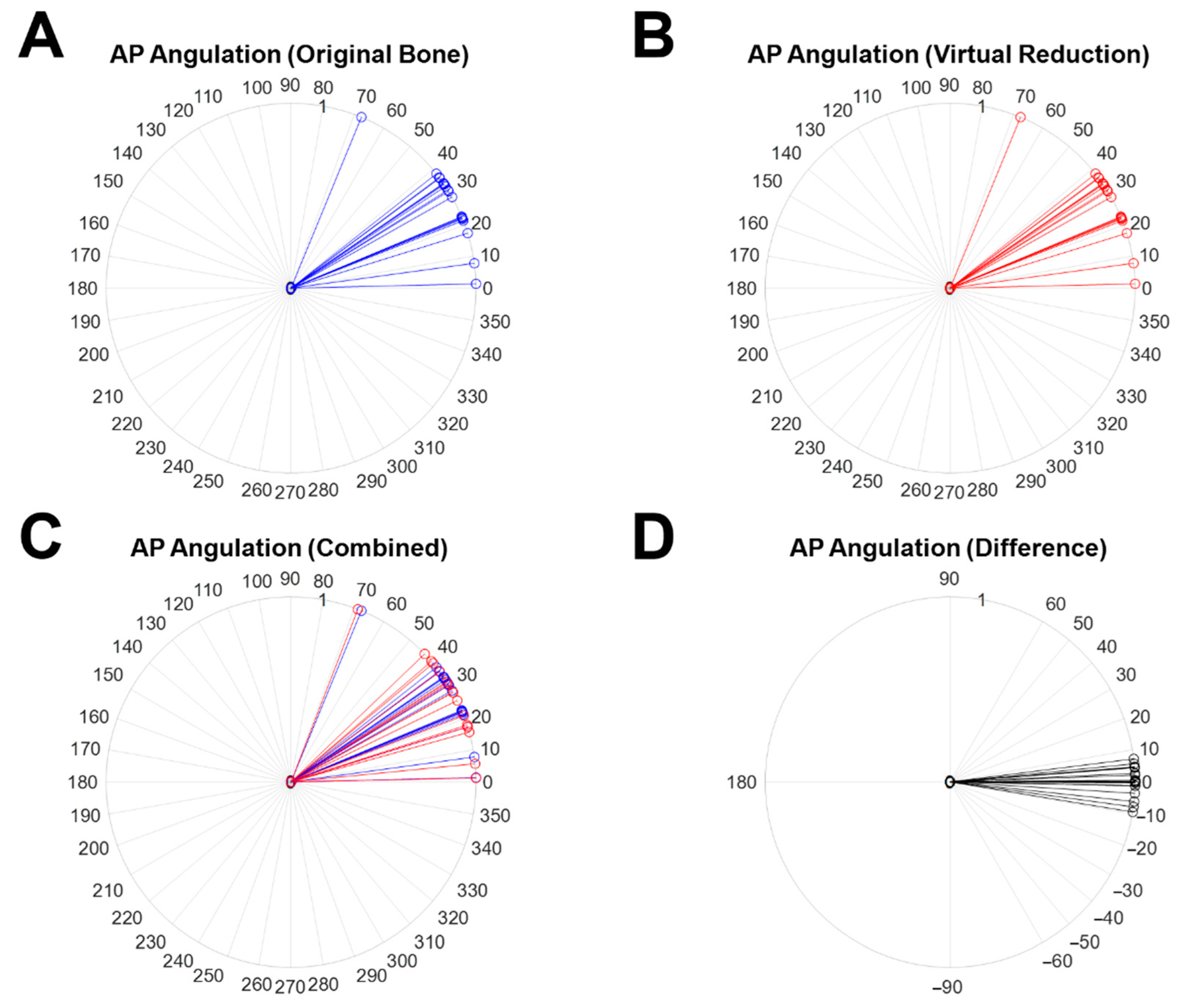
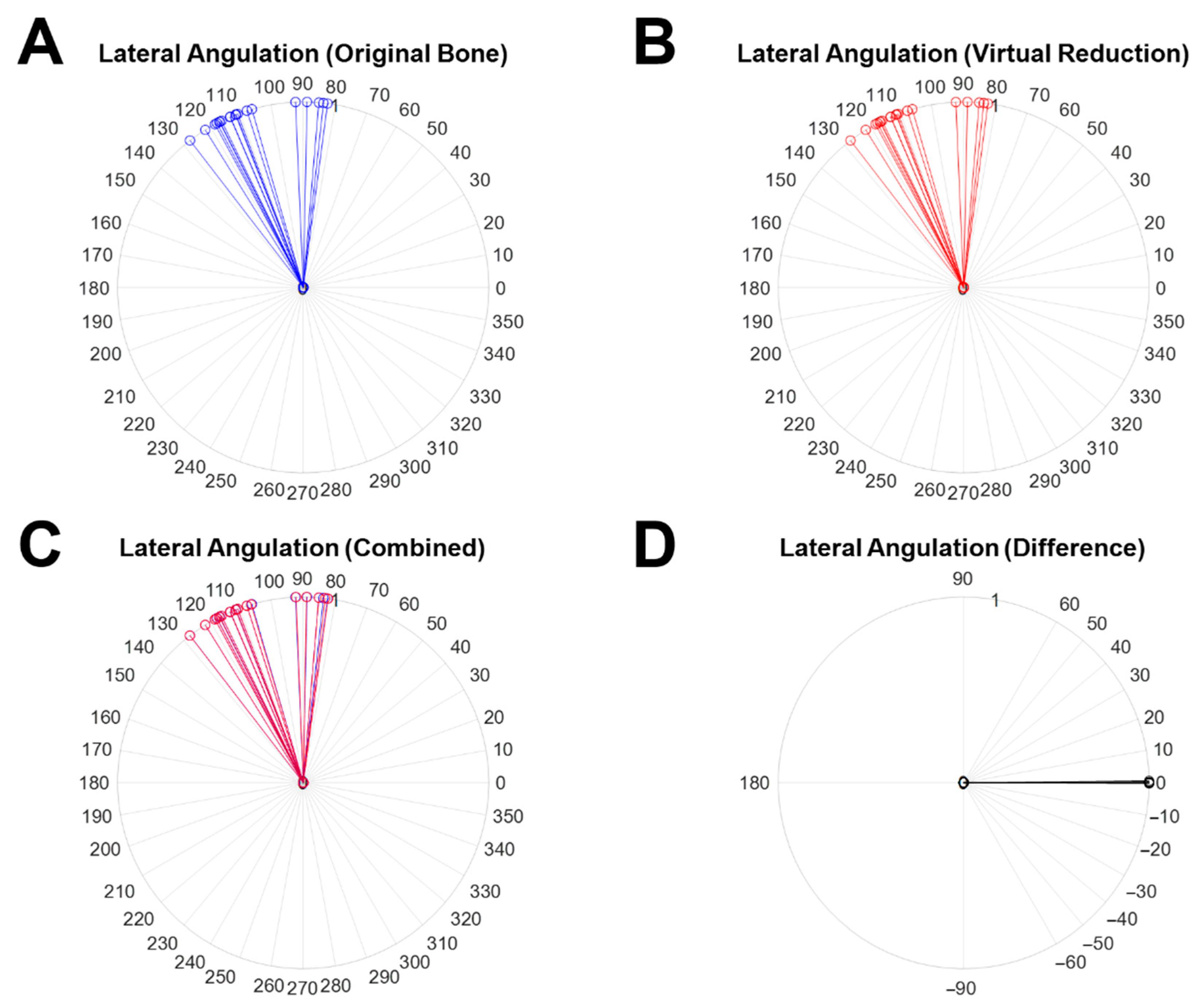
3.4. Alignment Variation
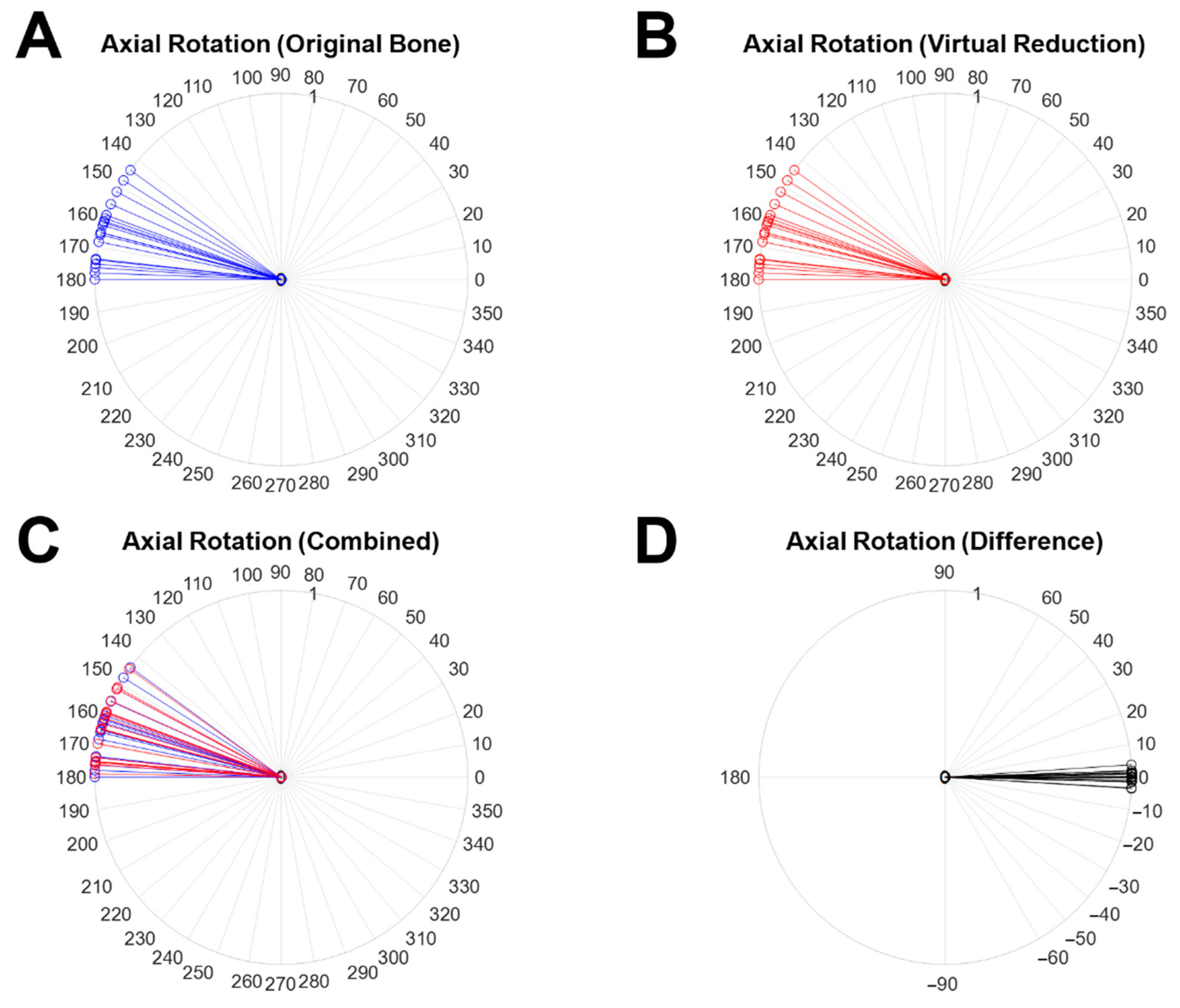
3.5. Rotation Variation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fazzalari, N. Bone fracture and bone fracture repair. Osteoporos. Int. 2011, 22, 2003–2006. [Google Scholar] [CrossRef] [PubMed]
- Braziulis, K.; Rimdeika, R.; Kregždytė, R.; Tarasevičius, Š. Associations between the fracture type and functional outcomes after distal radial fractures treated with a volar locking plate. Medicina 2013, 49, 62. [Google Scholar] [CrossRef] [Green Version]
- Noble, B.S.; Reeve, J. Osteocyte function, osteocyte death and bone fracture resistance. Mol. Cell. Endocrinol. 2000, 159, 7–13. [Google Scholar] [CrossRef]
- Engelhardt, L.; Niemeyer, F.; Christen, P.; Müller, R.; Stock, K.; Blauth, M.; Urban, K.; Ignatius, A.; Simon, U. Simulating metaphyseal fracture healing in the distal radius. Biomechanics 2021, 1, 29–42. [Google Scholar] [CrossRef]
- Stramazzo, L.; Rovere, G.; Cioffi, A.; Vigni, G.E.; Galvano, N.; D’Arienzo, A.; Letizia Mauro, G.; Camarda, L.; D’Arienzo, M. Peri-Implant Distal Radius Fracture: Proposal of a New Classification. J. Clin. Med. 2022, 11, 2628. [Google Scholar] [CrossRef] [PubMed]
- Wähnert, D.; Greiner, J.; Brianza, S.; Kaltschmidt, C.; Vordemvenne, T.; Kaltschmidt, B. Strategies to Improve Bone Healing: Innovative Surgical Implants Meet Nano-/Micro-Topography of Bone Scaffolds. Biomedicines 2021, 9, 746. [Google Scholar] [CrossRef] [PubMed]
- Chaya, A.; Yoshizawa, S.; Verdelis, K.; Myers, N.; Costello, B.J.; Chou, D.-T.; Pal, S.; Maiti, S.; Kumta, P.N.; Sfeir, C. In vivo study of magnesium plate and screw degradation and bone fracture healing. Acta Biomater. 2015, 18, 262–269. [Google Scholar] [CrossRef]
- El Haj, M.; Khoury, A.; Mosheiff, R.; Liebergall, M.; Weil, Y.A. Orthogonal double plate fixation for long bone fracture nonunion. Acta Chir. Orthop. Traumatol. Cech. 2013, 80, 131–137. [Google Scholar]
- Nadkarni, B.; Srivastav, S.; Mittal, V.; Agarwal, S. Use of locking compression plates for long bone nonunions without removing existing intramedullary nail: Review of literature and our experience. J. Trauma 2008, 65, 482–486. [Google Scholar] [CrossRef]
- Ellis, E., III; Muniz, O.; Anand, K. Treatment considerations for comminuted mandibular fractures. J. Oral Maxillofac. Surg. 2003, 61, 861–870. [Google Scholar] [CrossRef]
- Fantner, G.E.; Hassenkam, T.; Kindt, J.H.; Weaver, J.C.; Birkedal, H.; Pechenik, L.; Cutroni, J.A.; Cidade, G.A.G.; Stucky, G.D.; Morse, D.E. Sacrificial bonds and hidden length dissipate energy as mineralized fibrils separate during bone fracture. Nat. Mater. 2005, 4, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Geris, L.; Gerisch, A.; Vander Sloten, J.; Weiner, R.; Van Oosterwyck, H. Angiogenesis in bone fracture healing: A bioregulatory model. J. Theor. Biol. 2008, 251, 137–158. [Google Scholar] [CrossRef] [PubMed]
- Knitschke, M.; Sonnabend, S.; Roller, F.C.; Pons-Kühnemann, J.; Schmermund, D.; Attia, S.; Streckbein, P.; Howaldt, H.-P.; Böttger, S. Osseous Union after Mandible Reconstruction with Fibula Free Flap Using Manually Bent Plates vs. Patient-Specific Implants: A Retrospective Analysis of 89 Patients. Curr. Oncol. 2022, 29, 3375–3392. [Google Scholar] [CrossRef] [PubMed]
- Ghiasi, M.S.; Chen, J.; Vaziri, A.; Rodriguez, E.K.; Nazarian, A. Bone fracture healing in mechanobiological modeling: A review of principles and methods. Bone Rep. 2017, 6, 87–100. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Einhorn, T.A.; Marsh, D. Fracture healing: The diamond concept. Injury 2007, 38, S3–S6. [Google Scholar] [CrossRef]
- Mast, J.; Jakob, R.; Ganz, R. Planning and Reduction Technique in Fracture Surgery; Springer Science & Business Media: Berlin, Germany, 2012. [Google Scholar]
- Wood, G.W. General principles of fracture treatment. In Campbell’s Operative Orthoaedics, 10th ed.; Canale, S.T., Ed.; Mosby: St. Louis, MO, USA, 2003; p. 2714. [Google Scholar]
- Mizue, F.; Shirai, Y.; Ito, H. Surgical treatment of comminuted fractures of the distal clavicle using Wolter clavicular plates. J. Nippon Med. Sch. 2000, 67, 32–34. [Google Scholar] [CrossRef] [Green Version]
- Ingrassia, T.; Nigrelli, V.; Pecorella, D.; Bragonzoni, L.; Ricotta, V. Influence of the Screw Positioning on the Stability of Locking Plate for Proximal Tibial Fractures: A Numerical Approach. Appl. Sci. 2020, 10, 4941. [Google Scholar] [CrossRef]
- Orbay, J.L.; Castaneda, J.E.; Kortenbach, J.A. Bone Fracture Fixation Plate Shaping System. U.S. Patent 7,771,433, 10 August 2010. [Google Scholar]
- Fawcett, T. An introduction to ROC analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Florin, M.; Arzdorf, M.; Linke, B.; Auer, J.A. Assessment of stiffness and strength of 4 different implants available for equine fracture treatment: A study on a 20° oblique long-bone fracture model using a bone substitute. Vet. Surg. 2005, 34, 231–238. [Google Scholar] [CrossRef]
- Wagner, M.; Frenk, A.; Frigg, R. New concepts for bone fracture treatment and the Locking Compression Plate. Surg. Technol. Int. 2004, 12, 271–277. [Google Scholar]
- Watts, A.; Weinhold, P.; Kesler, W.; Dahners, L. A biomechanical comparison of short segment long bone fracture fixation techniques: Single large fragment plate versus 2 small fragment plates. J. Orthop. Trauma 2012, 26, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Bizzotto, N.; Sandri, A.; Regis, D.; Romani, D.; Tami, I.; Magnan, B. Three-dimensional printing of bone fractures: A new tangible realistic way for preoperative planning and education. Surg. Innov. 2015, 22, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Grützner, P.A.; Suhm, N. Computer aided long bone fracture treatment. Injury 2004, 35, S57–S64. [Google Scholar] [CrossRef]
- Fuessinger, M.A.; Gass, M.; Woelm, C.; Cornelius, C.-P.; Zimmerer, R.M.; Poxleitner, P.; Schlager, S.; Metzger, M.C. Analyzing the Fitting of Novel Preformed Osteosynthesis Plates for the Reduction and Fixation of Mandibular Fractures. J. Clin. Med. 2021, 10, 5975. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.K.; Chao, E.Y.S.; Mak, A.F.T. Development and validation of a new approach for computer-aided long bone fracture reduction using unilateral external fixator. J. Biomech. 2006, 39, 2104–2112. [Google Scholar] [CrossRef]
- Shefelbine, S.J.; Augat, P.; Claes, L.; Simon, U. Trabecular bone fracture healing simulation with finite element analysis and fuzzy logic. J. Biomech. 2005, 38, 2440–2450. [Google Scholar] [CrossRef] [PubMed]
- Caligiana, P.; Liverani, A.; Ceruti, A.; Santi, G.M.; Donnici, G.; Osti, F. An Interactive Real-Time Cutting Technique for 3D Models in Mixed Reality. Technologies 2020, 8, 23. [Google Scholar] [CrossRef]
- Cimerman, M.; Kristan, A. Preoperative planning in pelvic and acetabular surgery: The value of advanced computerised planning modules. Injury 2007, 38, 442–449. [Google Scholar] [CrossRef]
- Giovinco, N.A.; Dunn, S.P.; Dowling, L.; Smith, C.; Trowell, L.; Ruch, J.A.; Armstrong, D.G. A novel combination of printed 3-dimensional anatomic templates and computer-assisted surgical simulation for virtual preoperative planning in Charcot foot reconstruction. J. Foot Ankle Surg. 2012, 51, 387–393. [Google Scholar] [CrossRef]
- Girod, S.; Teschner, M.; Schrell, U.; Kevekordes, B.; Girod, B. Computer-aided 3-D simulation and prediction of craniofacial surgery: A new approach. J. Craniomaxillofac. Surg. 2001, 29, 156–158. [Google Scholar] [CrossRef]
- Iorio, R.; Siegel, J.; Specht, L.M.; Tilzey, J.F.; Hartman, A.; Healy, W.L. A comparison of acetate vs digital templating for preoperative planning of total hip arthroplasty: Is digital templating accurate and safe? J. Arthroplast. 2009, 24, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Jamali, A.A. Digital templating and preoperative deformity analysis with standard imaging software. Clin. Orthop. Relat. Res. 2009, 467, 2695–2704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosashvilim, Y.; Shasha, N.; Olschewski, E.; Safir, O.; White, L.; Gross, A.; Backstein, D. Digital versus conventional templating techniques in preoperative planning for total hip arthroplasty. Can. J. Surg. 2009, 52, 6–11. [Google Scholar]
- Noble, P.C.; Sugano, N.; Johnston, J.D.; Thompson, M.T.; Conditt, M.A.; Engh Sr, C.A.; Mathis, K.B. Computer simulation: How can it help the surgeon optimize implant position? Clin. Orthop. Relat. Res. 2003, 417, 242–252. [Google Scholar] [CrossRef]
- Kohyama, S.; Nishiura, Y.; Hara, Y.; Ogawa, T.; Ikumi, A.; Okano, E.; Totoki, Y.; Yoshii, Y.; Yamazaki, M. Preoperative Evaluation and Surgical Simulation for Osteochondritis Dissecans of the Elbow Using Three-Dimensional MRI-CT Image Fusion Images. Diagnostics 2021, 11, 2337. [Google Scholar] [CrossRef] [PubMed]
- Tucker, S.; Cevidanes, L.H.S.; Styner, M.; Kim, H.; Reyes, M.; Proffit, W.; Turvey, T. Comparison of actual surgical outcomes and 3-dimensional surgical simulations. J. Oral Maxillofac. Surg. 2010, 68, 2412–2421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suetenkov, D.; Ivanov, D.; Dol, A.; Diachkova, E.; Vasil’ev, Y.; Kossovich, L. Construction of Customized Palatal Orthodontic Devices on Skeletal Anchorage Using Biomechanical Modeling. Bioengineering 2022, 9, 12. [Google Scholar] [CrossRef]
- Egol, K.A.; Koval, K.J.; Zuckerman, J.D. Handbook of Fractures, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Kim, M.-S.; Shin, H.-B.; Kim, S.; Shim, J.G.; Yoon, D.-K.; Suh, T.-S. SPECT Image analysis using computational ROC curve based on threshold setup. Prog. Med. Phys. 2017, 28, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Camblor, P.; Pardo-Fernández, J.C. The Youden index in the generalized receiver operating characteristic curve context. Int. J. Biostat. 2019, 15, 20180060. [Google Scholar] [CrossRef]
- Gao, W.; Wang, W. Analysis of k-partite ranking algorithm in area under the receiver operating characteristic curve criterion. Int. J. Comput. Math. 2018, 95, 1527–1547. [Google Scholar] [CrossRef]
- Cho, H.; Matthews, G.J.; Harel, O. Confidence intervals for the area under the receiver operating characteristic curve in the presence of ignorable missing data. Int. Stat. Rev. 2019, 87, 152–177. [Google Scholar] [CrossRef] [PubMed]
- Al-Ayyoub, M.; Al-Zghool, D. Determining the type of long bone fractures in x-ray images. WSEAS Trans. Inf. Sci. Appl. 2013, 10, 261–270. [Google Scholar]
- Dobbe, J.G.G.; du Pré, K.J.; Kloen, P.; Blankevoort, L.; Streekstra, G.J. Computer-assisted and patient-specific 3-D planning and evaluation of a single-cut rotational osteotomy for complex long-bone deformities. Med. Biol. Eng. Comput. 2011, 49, 1363–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neill, M.C.; Ruff, C.B. Estimating human long bone cross-sectional geometric properties: A comparison of noninvasive methods. J. Hum. Evol. 2004, 47, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, G.; Müller, U.; Wentzensen, A. The value of laboratory and imaging studies in the evaluation of long-bone non-unions. Injury 2007, 38, S33–S37. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.-S.; Yoon, D.-K.; Shin, S.-H.; Choe, B.-Y.; Rhie, J.-W.; Chung, Y.-G.; Suh, T.S. Quantitative Assessment of the Restoration of Original Anatomy after 3D Virtual Reduction of Long Bone Fractures. Diagnostics 2022, 12, 1372. https://doi.org/10.3390/diagnostics12061372
Kim M-S, Yoon D-K, Shin S-H, Choe B-Y, Rhie J-W, Chung Y-G, Suh TS. Quantitative Assessment of the Restoration of Original Anatomy after 3D Virtual Reduction of Long Bone Fractures. Diagnostics. 2022; 12(6):1372. https://doi.org/10.3390/diagnostics12061372
Chicago/Turabian StyleKim, Moo-Sub, Do-Kun Yoon, Seung-Han Shin, Bo-Young Choe, Jong-Won Rhie, Yang-Guk Chung, and Tae Suk Suh. 2022. "Quantitative Assessment of the Restoration of Original Anatomy after 3D Virtual Reduction of Long Bone Fractures" Diagnostics 12, no. 6: 1372. https://doi.org/10.3390/diagnostics12061372