
Impact of Selected Serum Factors on Metastatic Potential of Gastric Cancer Cells

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Description of Patient Cohort: Inclusion and Exclusion Criteria
2.2. Collection and Preservation of Serum Samples
2.3. Cells and Culture Conditions
2.4. Enzyme-Linked Immunoassay
2.5. Online Databases and Analysis
2.6. Chemotaxis Assay
2.7. Cell Adhesion
2.8. Cell Proliferation
2.9. Statistical Analysis
3. Results
3.1. Detailed Patient Characteristics
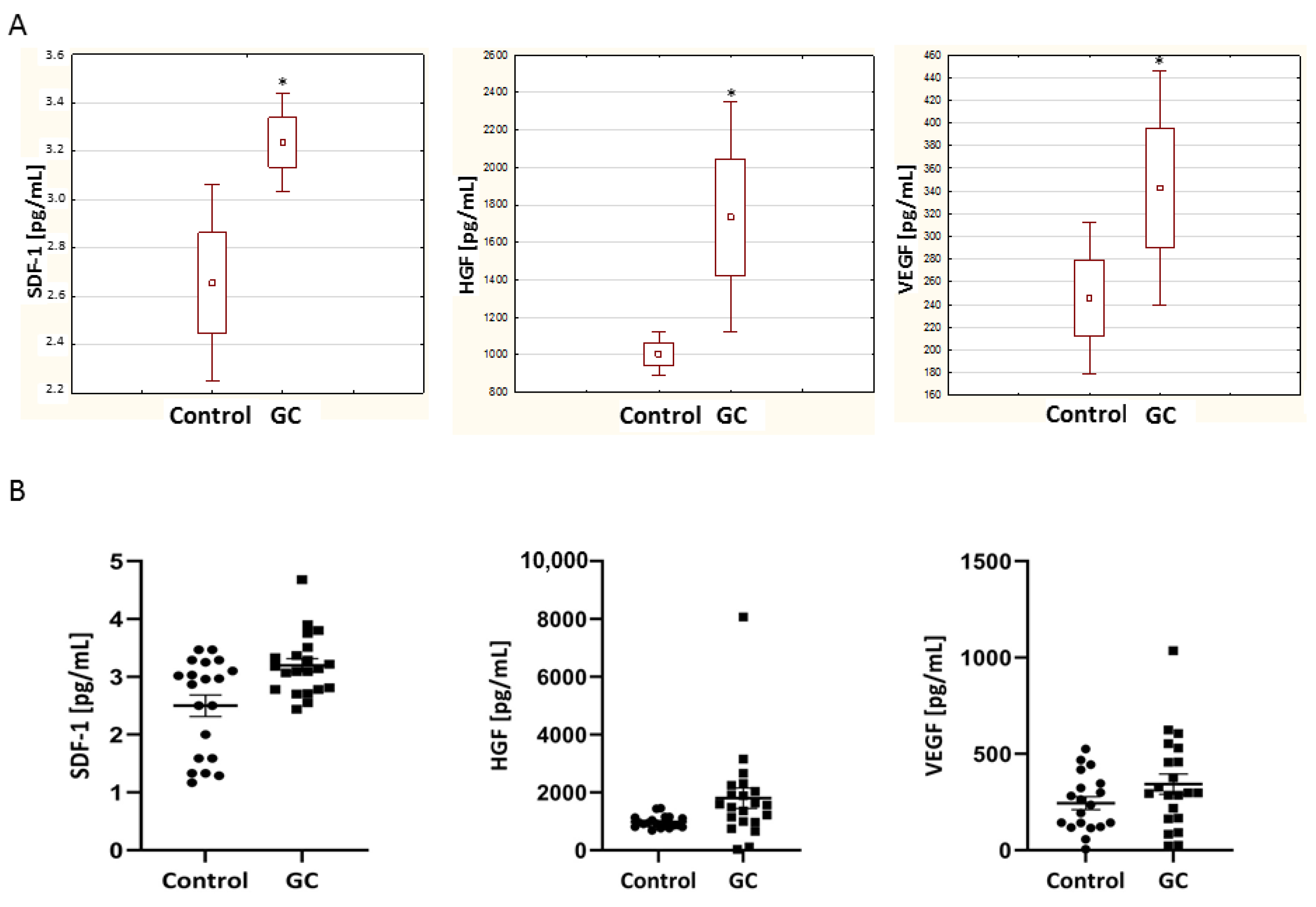
3.2. High Level of SDF-1, HGF and VEGF in Gastric Cancer Patients’ Serum
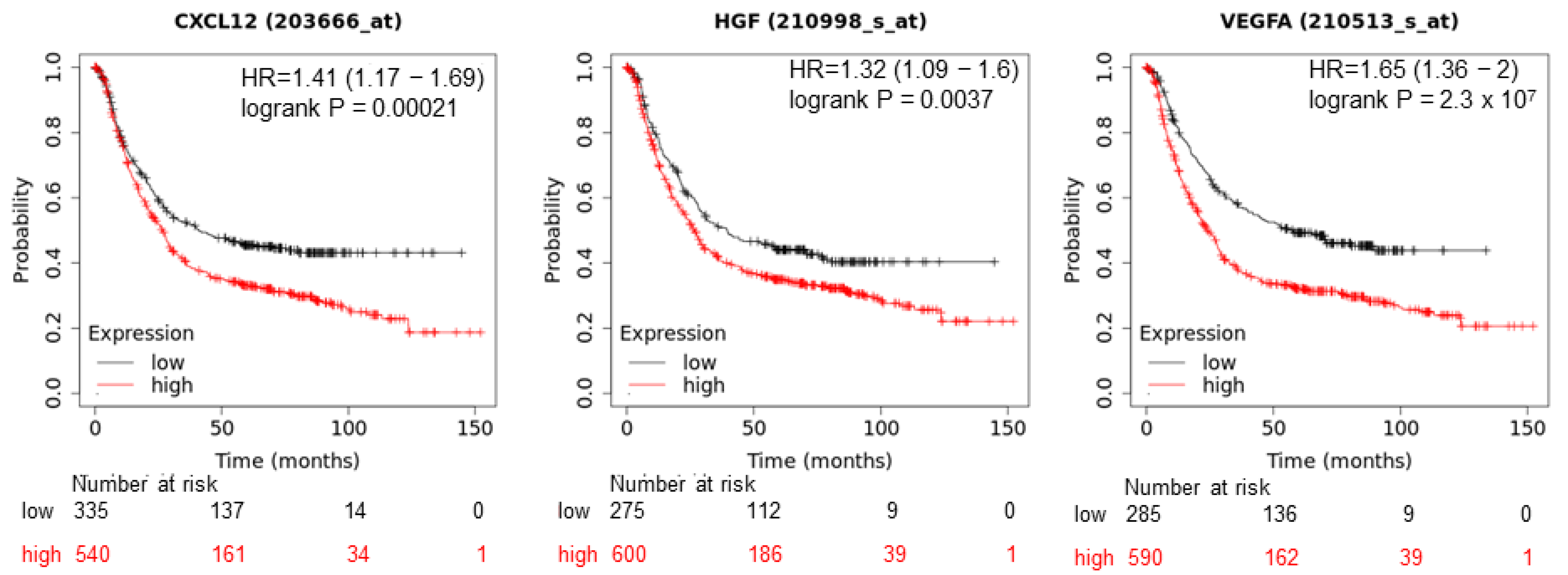
3.3. High Expression of SDF-1, HGF and VEGF-A in Tumor Tissues Decreases Gastric Cancer Patients’ Overall Survival
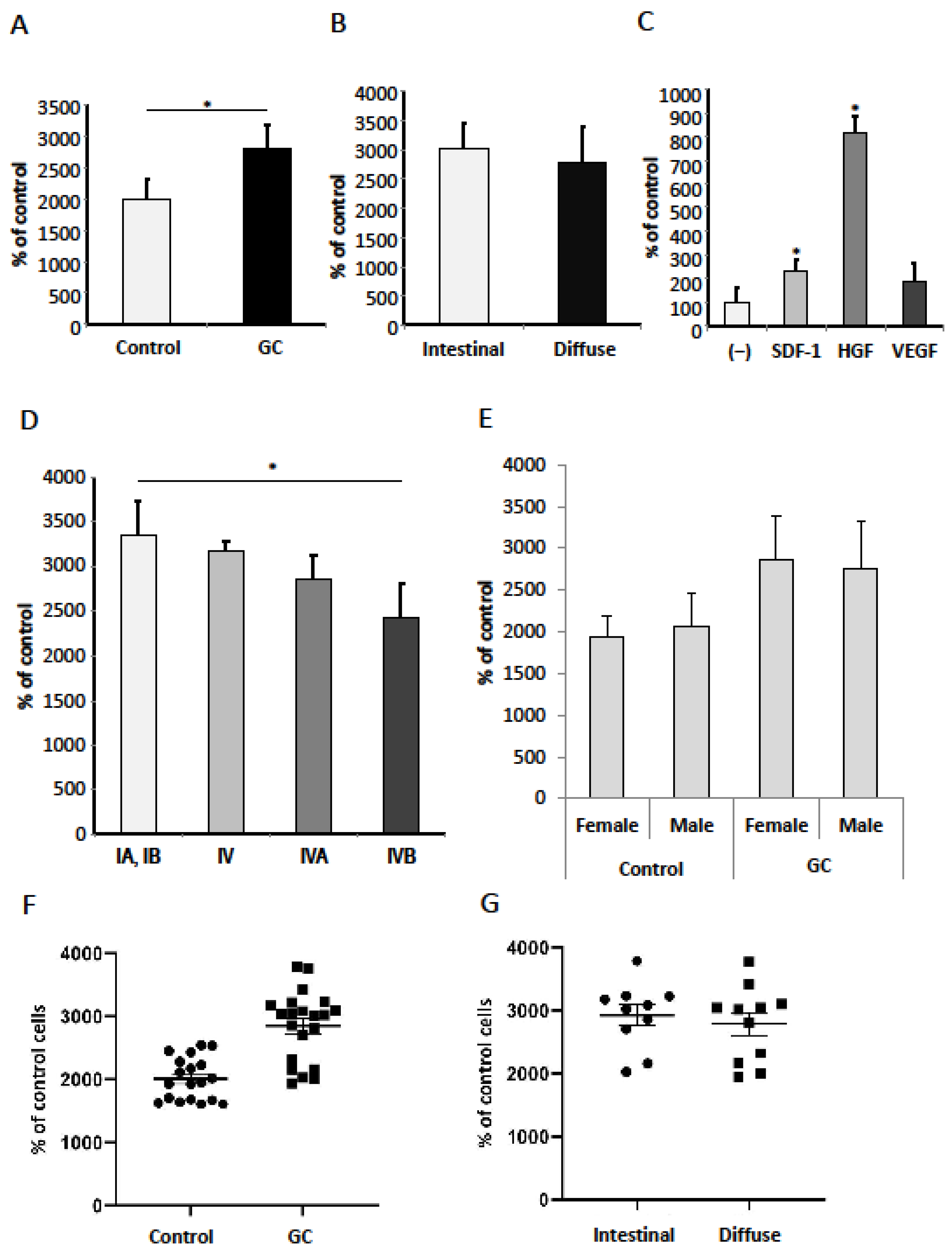
3.4. SDF-1, HGF, VEGF-A and Serum from Gastric Cancer Patients Promote Migration of Gastric Cancer Cells
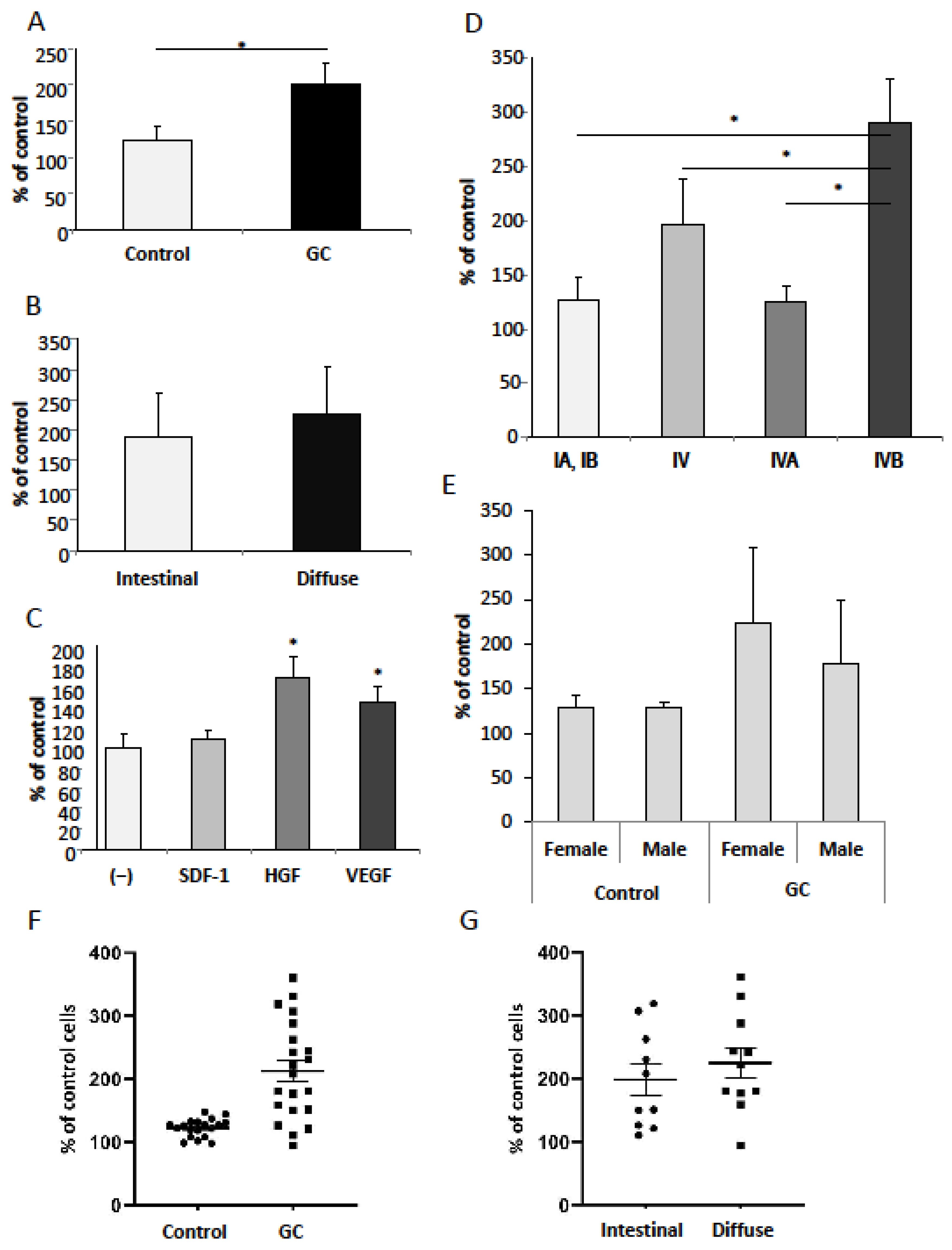
3.5. SDF-1, HGF, VEGF-A and Serum from Gastric Cancer Patients Promote Adhesion of Gastric Cancer Cells
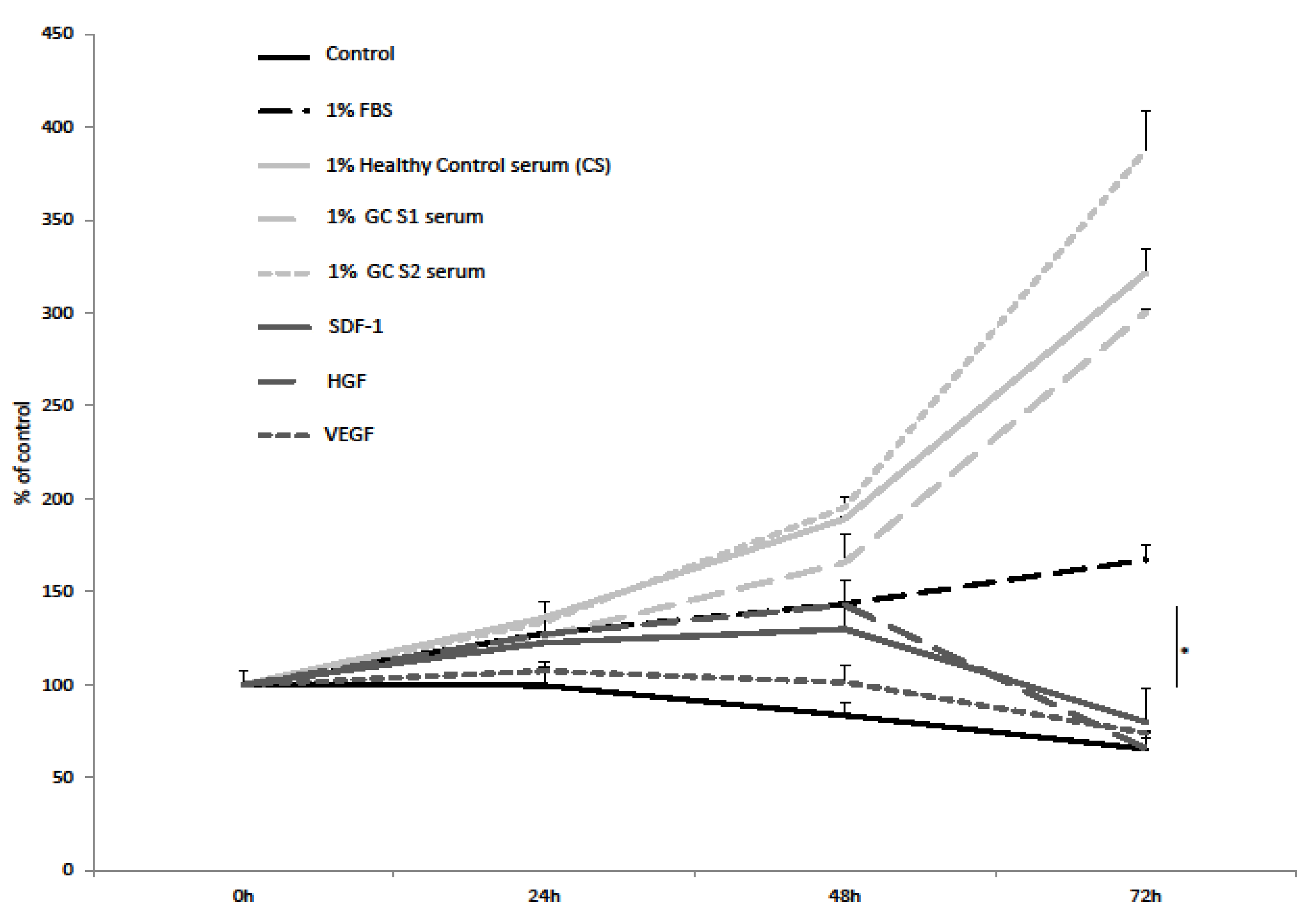
3.6. SDF-1, HGF, VEGF-A and Serum from Gastric Cancer Patients Promote Proliferation of Gastric Cancer Cells
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamashima, C. The burden of gastric cancer. Ann. Transl. Med. 2020, 8, 734. [Google Scholar] [CrossRef]
- Yusefi, A.R.; Lankarani, K.B.; Bastani, P.; Radinmanesh, M.; Kavosi, Z. Risk Factors for Gastric Cancer: A Systematic Review. Asian Pac. J. Cancer Prev. 2018, 19, 591–603. [Google Scholar] [CrossRef]
- Ang, T.L.; Fock, K.M. Clinical epidemiology of gastric cancer. Singap. Med. J. 2014, 55, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Nagini, S. Carcinoma of the stomach: A review of epidemiology, pathogenesis, molecular genetics and chemoprevention. World J. Gastrointest. Oncol. 2012, 4, 156–169. [Google Scholar] [CrossRef]
- Ushijima, T.; Sasako, M. Focus on gastric cancer. Cancer Cell 2004, 5, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Narita, Y.; Muro, K. Challenges in molecular targeted therapy for gastric cancer: Considerations for efficacy and safety. Expert Opin. Drug Saf. 2016, 16, 319–327. [Google Scholar] [CrossRef]
- Wang, T.; Hou, J.; Li, Z.; Zheng, Z.; Wei, J.; Song, D.; Hu, T.; Wu, Q.; Yang, J.Y.; Cai, J.-C. miR-15a-3p and miR-16-1-3p Negatively Regulate Twist1 to Repress Gastric Cancer Cell Invasion and Metastasis. Int. J. Biol. Sci. 2017, 13, 122–134. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.-Y.; Lee, K.-G.; Suh, Y.-S.; Kim, M.A.; Kong, S.-H.; Lee, H.-J.; Kim, W.H.; Yang, H.-K. Lymph Node Metastasis in Mucosal Gastric Cancer. Ann. Surg. 2017, 265, 137–142. [Google Scholar] [CrossRef]
- Yu, S.; Yu, Y.; Zhang, W.; Yuan, W.; Zhao, N.; Li, Q.; Cui, Y.; Wang, Y.; Li, W.; Sun, Y.; et al. FOXO3a promotes gastric cancer cell migration and invasion through the induction of cathepsin L. Oncotarget 2016, 7, 34773–34784. [Google Scholar] [CrossRef] [Green Version]
- Szala, S. Cells of the tumor microenvironment: The purpose of antitumor therapy. J. Oncol. 2007, 57, 633–645. [Google Scholar]
- Louault, K.; Li, R.-R.; Declerck, Y.A. Cancer-Associated Fibroblasts: Understanding Their Heterogeneity. Cancers 2020, 12, 3108. [Google Scholar] [CrossRef]
- Ichikawa, J.; Matsumoto, S.; Shimoji, T.; Tanizawa, T.; Gokita, T.; Hayakawa, K.; Aoki, K.; Ina, S.; Kanda, H. Intraneural metastasis of gastric carcinoma leads to sciatic nerve palsy. BMC Cancer 2012, 12, 313. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Wu, N.-D.; Liu, B.-R. Regional but fatal: Intraperitoneal metastasis in gastric cancer. World J. Gastroenterol. 2016, 22, 7478–7485. [Google Scholar] [CrossRef]
- Bugyik, E.; Renyi-Vamos, F.; Szabo, V.; Dezso, K.; Ecker, N.; Rokusz, A.; Nagy, P.; Dome, B.; Paku, S. Mechanisms of vascularization in murine models of primary and metastatic tumor growth. Chin. J. Cancer 2016, 35, 19. [Google Scholar] [CrossRef] [Green Version]
- Yu, B.; Chen, X.; Li, J.; Qu, Y.; Su, L.; Peng, Y.; Huang, J.; Yan, J.; Yu, Y.; Gu, Q.; et al. Stromal fibroblasts in the microenvironment of gastric carcinomas promote tumor metastasis via upregulating TAGLN expression. BMC Cell Biol. 2013, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kitadai, Y. Cancer-Stromal Cell Interaction and Tumor Angiogenesis in Gastric Cancer. Cancer Microenviron. 2009, 3, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Chen, X.; Zhou, Q.; Li, P.; Yu, B.; Li, J.; Qu, Y.; Yan, J.; Yu, Y.; Yan, M.; et al. Hepatocyte growth factor activates tumor stromal fibroblasts to promote tumorigenesis in gastric cancer. Cancer Lett. 2013, 335, 128–135. [Google Scholar] [CrossRef]
- Baj, J.; Korona-Głowniak, I.; Forma, A.; Maani, A.; Sitarz, E.; Rahnama-Hezavah, M.; Radzikowska, E.; Portincasa, P. Mechanisms of the Epithelial–Mesenchymal Transition and Tumor Microenvironment in Helicobacter pylori-Induced Gastric Cancer. Cells 2020, 9, 1055. [Google Scholar] [CrossRef] [Green Version]
- Grymula, K.; Tarnowski, M.; Wysoczynski, M.; Drukala, J.; Barr, F.G.; Ratajczak, J.; Kucia, M. Overlapping and distinct role of CXCR7-SDF-1/ITAC and CXCR4-SDF-1 axes in regulating metastatic behavior of human rhabdomyosarcomas. Int. J. Cancer 2010, 127, 2554–2568. [Google Scholar] [CrossRef]
- Zhao, B.-C.; Wang, Z.-J.; Mao, W.-Z.; Ma, H.-C.; Han, J.-G.; Zhao, B.; Xu, H.-M. CXCR4/SDF-1 axis is involved in lymph node metastasis of gastric carcinoma. World J. Gastroenterol. 2011, 17, 2389–2396. [Google Scholar] [CrossRef]
- Stuelten, C.; Parent, C.A.; Montell, D.J. Cell motility in cancer invasion and metastasis: Insights from simple model organisms. Nat. Cancer 2018, 18, 296–312. [Google Scholar] [CrossRef]
- Noguchi, E.; Saito, N.; Kobayashi, M.; Kameoka, S. Clinical significance of hepatocyte growth factor/c-Met expression in the assessment of gastric cancer progression. Mol. Med. Rep. 2015, 11, 3423–3431. [Google Scholar] [CrossRef] [Green Version]
- Sasahira, T.; Kirita, T. Hallmarks of Cancer-Related Newly Prognostic Factors of Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2018, 19, 2413. [Google Scholar] [CrossRef] [Green Version]
- Carmeliet, P.; Ferreira, V.; Breier, G.; Pollefeyt, S.; Kieckens, L.; Gertsenstein, M.; Fahrig, M.; Vandenhoeck, A.; Harpal, K.; Eberhardt, C.; et al. Abnormal blood vessel development and lethality in embryos lacking a single VEGF allele. Nat. Cell Biol. 1996, 380, 435–439. [Google Scholar] [CrossRef]
- Sousa Moreira, I.; Alexandrino Fernandes, P.; Joao Ramos, M. Vascular Endothelial Growth Factor (VEGF) Inhibition—A Critical Review. Anti-Cancer Agents Med. Chem. 2007, 7, 223–245. [Google Scholar] [CrossRef]
- Kędzierska, L.; Madej-Michniewicz, A.; Marczuk, N.; Dołęgowska, B.; Starzyńska, T.; Błogowski, W. Clinical significance of var-ious growth factors in patients with different gastric neoplasms. Am. J. Transl. Res. 2020, 12, 118–129. [Google Scholar]
- Saharinen, P.; Eklund, L.; Pulkki, K.; Bono, P.; Alitalo, K. VEGF and angiopoietin signaling in tumor angiogenesis and metastasis. Trends Mol. Med. 2011, 17, 347–362. [Google Scholar] [CrossRef]
- Sun, F.; Feng, M.; Guan, W. Mechanisms of peritoneal dissemination in gastric cancer (Review). Oncol. Lett. 2017, 14, 6991–6998. [Google Scholar] [CrossRef] [Green Version]
- Hassan, S.; Baccarelli, A.; Salvucci, O.; Basik, M. Plasma Stromal Cell-Derived Factor-1: Host Derived Marker Predictive of Distant Metastasis in Breast Cancer. Clin. Cancer Res. 2008, 14, 446–454. [Google Scholar] [CrossRef] [Green Version]
- Karabulut, S.; Taş, F.; Akyüz, F.; Ormeci, A.C.; Serilmez, M.; Soydinc, H.O.; Vatansever, S.; Yasasever, V. Clinical significance of serum hepatocyte growth factor (HGF) levels in hepatocellular carcinoma. Tumor Biol. 2013, 35, 2327–2333. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, Y.; Hosaka, K.; Andersson, P.; Wang, J.; Tholander, F.; Cao, Z.; Morikawa, H.; Tegnér, J.; Yang, Y.; et al. VEGF-B promotes cancer metastasis through a VEGF-A–independent mechanism and serves as a marker of poor prognosis for cancer patients. Proc. Natl. Acad. Sci. USA 2015, 112, E2900–E2909. [Google Scholar] [CrossRef] [Green Version]
- Ding, S.; Lin, S.; Dong, X.; Yang, X.; Qu, H.; Huang, S.; Liu, W.; Zhou, L.; Liu, D. Potential prognostic value of circulating levels of vascular endothelial growth factor-A in patients with gastric cancer. In Vivo 2005, 19, 793–795. [Google Scholar]
- Macedo, F.; Ladeira, K.; Longatto-Filho, A.; Martins, S.F. Gastric Cancer and Angiogenesis: Is VEGF a Useful Biomarker to Assess Progression and Remission? J. Gastric Cancer 2017, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Shen, H.; Kapesa, L.; Zeng, S. Lauren classification and individualized chemotherapy in gastric cancer. Oncol. Lett. 2016, 11, 2959–2964. [Google Scholar] [CrossRef] [Green Version]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Lánczky, A.; Győrffy, B. Web-Based Survival Analysis Tool Tailored for Medical Research (KMplot): Development and Implementation. J. Med. Internet Res. 2021, 23, e27633. [Google Scholar] [CrossRef]
- Tarnowski, M.; Schneider, G.; Amann, G.; Clark, G.; Houghton, P.; Barr, F.G.; Kenner, L.; Ratajczak, M.Z.; Kucia, M. RasGRF1 regulates proliferation and metastatic behavior of human alveolar rhabdomyosarcomas. Int. J. Oncol. 2012, 41, 995–1004. [Google Scholar] [CrossRef] [Green Version]
- Iwasa, S.; Yanagawa, T.; Fan, J.; Katoh, R. Expression of CXCR4 and its ligand SDF-1 in intestinal–type gastric cancer is associated with lumphe node and liver metastasis. Anticancer Res. 2009, 29, 4751–4758. [Google Scholar]
- Lee, H.J.; Kim, S.W.; Kim, H.Y.; Li, S.; Yun, H.J.; Song, K.S.; Kim, S.; Jo, D.Y. Chemokine receptor CXCR4 expression, function, and clinical implications in gastric cancer. Int. J. Oncol. 2009, 34, 473–480. [Google Scholar]
- Tarnowski, M.; Grymuła, K.; Tkacz, M.; Czerewaty, M.; Poniewierska-Baran, A.; Ratajczak, M.Z. Molecular mechanisms regulating metastasis of cancer cells with special emphasis on rhabdomyosarcoma. Postepy Hig. Med. Dosw. (Online) 2014, 68, 258–270. [Google Scholar] [CrossRef]
- Kwak, M.K.; Hur, K.; Park, D.J.; Lee, H.J.; Kim, W.H.; Lee, K.U.; Choe, K.J.; Yang, H.K. Expression of chemokine receptors in human gastric cancer. Tumour Biol. 2005, 26, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Ji, J.; Jiang, J.; Cai, Q.; Wang, C.; Shi, M.; Yu, Y.; Zhu, Z.; Zhang, J. HGF-mediated crosstalk between cancer-associated fibroblasts and MET-unamplified gastric cancer cells activates coordinated tumorigenesis and metastasis. Cell Death Dis. 2018, 9, 867. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-Y.; Hsieh, J.-S.; Chen, C.-C.; Tzou, W.-S.; Cheng, T.-L.; Chen, F.-M.; Huang, T.-J.; Huang, Y.-S.; Huang, S.-Y.; Yang, T.; et al. Alterations of APC, c-met, and p53 genes in tumor tissue and serum of patients with gastric cancers. J. Surg. Res. 2004, 120, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xi, W.; Ji, J.; Cai, Q.; Zhao, Q.; Jiang, J.; Zhou, C.; Shi, M.; Zhang, H.; Zhu, Z.; et al. The prognostic value of HGF-c-MET signaling pathway in Gastric Cancer: A study based on TCGA and GEO databases. Int. J. Med. Sci. 2020, 17, 1946–1955. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y. Molecular therapy for gastric cancer. Chin. Clin. Oncol. 2013, 2. [Google Scholar] [CrossRef]
- Prager, M.G.; Lackner, E.-M.; Krauth, M.-T.; Unseld, M.; Pöttler, M.; Laffer, S.; Cerny-Reiterer, S.; Lamm, W.; Kornek, G.V.; Binder, B.R.; et al. Targeting of VEGF-dependent transendothelial migration of cancer cells by bevacizumab. Mol. Oncol. 2010, 4, 150–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, H.; Kobayashi, M.; Sakamoto, J. Evaluation and treatment of malignant ascites secondary to gastric cancer. World J. Gastroenterol. 2015, 21, 10936–10947. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wei, Z.; Wang, C.; Chen, W.; He, Y.; Zhang, C. Gender Differences in Gastric Cancer Survival: 99,922 Cases Based on the SEER Database. J. Gastrointest. Surg. 2020, 24, 1747–1757. [Google Scholar] [CrossRef] [PubMed]
- Roussos, E.T.; Condeelis, J.S.; Patsialou, A. Chemotaxis in cancer. Nat. Cancer 2011, 11, 573–587. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Parameters | Cases (n = 21) | Healthy Controls (n = 19) |
|---|---|---|
| Age (years) | 64.8 (3.15) 1 | 59.6 (1.88) 1 |
| Gender | ||
| 11 (52.4%) | 10 (52.6%) |
| 10 (47.6%) | 9 (47.4%) |
| Tumor histology | ||
| 10 (47.6%) | |
| 11 (52.4%) | |
| TNM stage | ||
| 3 (14.3%) | |
| 2 (9.5%) | |
| 3 (14.3%) | |
| 1 (4.8%) | |
| 4 (19.0%) | |
| 2 (9.5%) | |
| 6 (28.6%) | |
| Serum levels (pg/mL) | ||
| 3.2 (0.11) 1 | 2.66 (0.20) 1 |
| 1808.59 (356.38) 1 | 1003.74 (46.78) 1 |
| 345.59 (52.54) 1 | 245.6 (32.22) 1 |
| Control | p | Intestinal (IA and IB) | p | Intestinal (IV-IVB) | p | Diffuse (IA, IB, II) | p | Diffuse (III, IV-IVB) | p | Total Intestinal | p | Total Diffuse | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 19 | n = 3 | n = 7 | n = 4 | n = 7 | n= 10 | n= 11 | ||||||||
| Male, n (%) | 10 (52.63) | ref | 1 (33.33) | 0.53 | 5 (71.43) | 0.39 | 1 (25.00) | 0.31 | 3 (42.86) | 0.66 | 6 (60.00) | 0.7 | 4 (36.36) | 0.39 |
| Female, n (%) | 9 (47.37) | 2 (66.67) | 2 (28.57) | 3 (75.00) | 4 (57.14) | 4 (40.00) | 7 (63.64) | |||||||
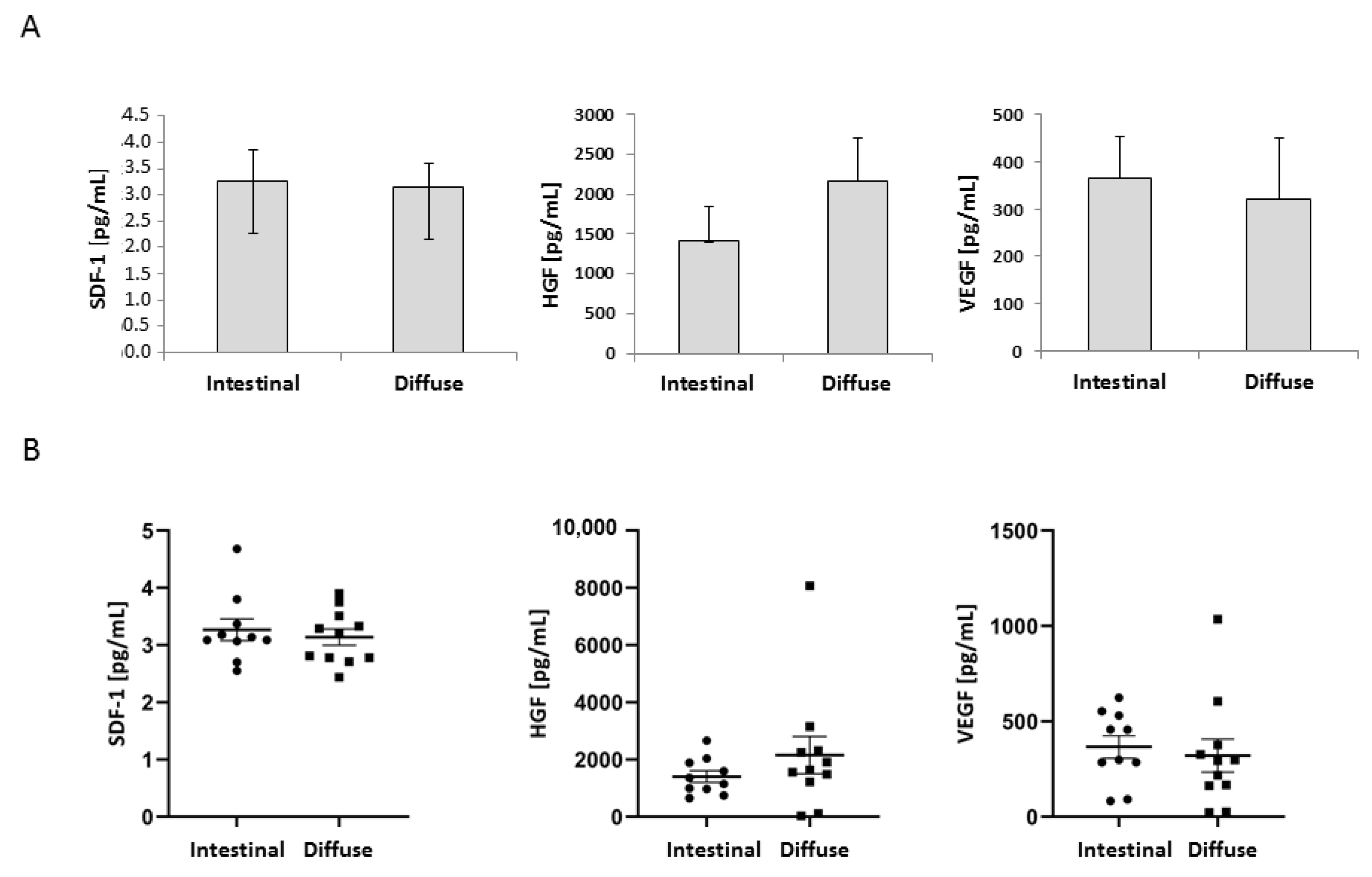
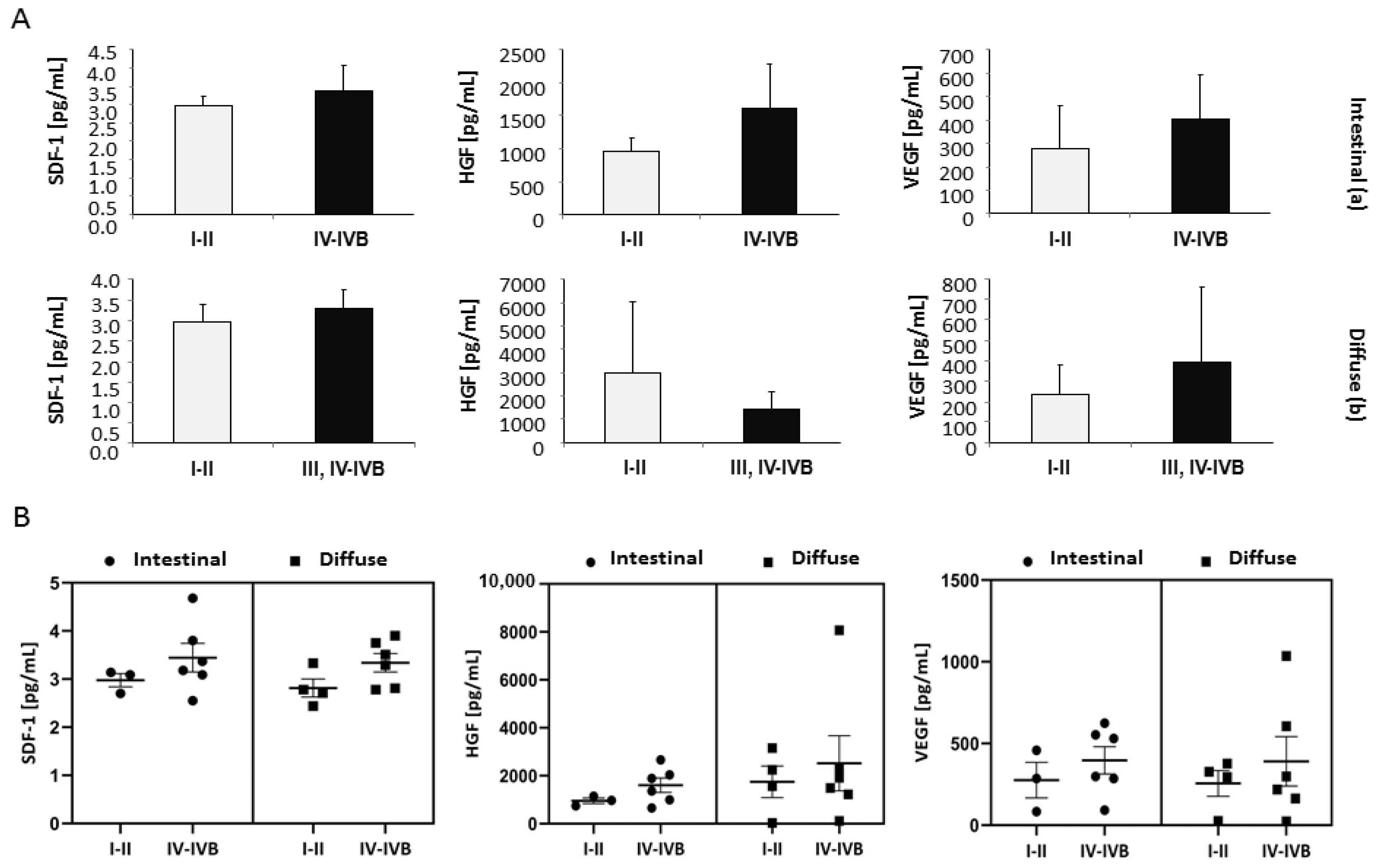
| Serum level of SDF-1 (pg/mL), median | 2.96 | ref | 3.09 | 0.7 | 3.18 | 0.73 | 2.75 | 0.97 | 3.29 | 0.06 | 3.11 | 0.1 | 3.22 | 0.16 |
| (IQR) | (1.59–3.27) | (2.89–3.11) | (3.08–3.59) | (2.64–2.92) | (3.02–3.63) | (3.07–3.32) | (2.78–3.42) | |||||||
| Serum level of HGF (ng/mL), median | 0.92 | ref | 0.97 | 1 | 1.60 | 0.03 * | 1.90 | 0.13 | 1.64 | 0.01 * | 1.26 | 0.08 | 1.64 | 0.006 * |
| (IQR) | (0.82–1.12) | (0.86–1.06) | (1.18–1.96) | (1.18–2.47) | (1.35–2.11) | (0.97–1.82) | (1.35–2.28) | |||||||
| Serum level of VEGF (pg/mL), median | 235.18 | ref | 285.19 | 0.85 | 457.40 | 0.06 | 310.50 | 0.78 | 218.00 | 0.6 | 377.80 | 0.1 | 293.90 | 0.58 |
| (IQR) | (131.88–335.22) | (184.04–371.59) | (291.69–541–750 | (226.95–339.45) | (164.85–451–77) | (285.19–512.22) | (164.85–351.80) | |||||||
| Age at diagnosis, median years | 59 | ref | 73 | 0.01 * | 69 | 0.39 | 56 | 0.49 | 59 | 0.69 | 72 | 0.06 | 59 | 0.97 |
| (IQR) | (54–65) | (72–79) | (53–81) | (49–62) | (52–75) | (59–83) | (49–71) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tkacz, M.; Tarnowski, M.; Poniewierska-Baran, A.; Serwin, K.; Madej-Michniewicz, A.; Deskur, A.; Czerny, B.; Starzyńska, T. Impact of Selected Serum Factors on Metastatic Potential of Gastric Cancer Cells. Diagnostics 2022, 12, 700. https://doi.org/10.3390/diagnostics12030700
Tkacz M, Tarnowski M, Poniewierska-Baran A, Serwin K, Madej-Michniewicz A, Deskur A, Czerny B, Starzyńska T. Impact of Selected Serum Factors on Metastatic Potential of Gastric Cancer Cells. Diagnostics. 2022; 12(3):700. https://doi.org/10.3390/diagnostics12030700
Chicago/Turabian StyleTkacz, Marta, Maciej Tarnowski, Agata Poniewierska-Baran, Karol Serwin, Anna Madej-Michniewicz, Anna Deskur, Bogusław Czerny, and Teresa Starzyńska. 2022. "Impact of Selected Serum Factors on Metastatic Potential of Gastric Cancer Cells" Diagnostics 12, no. 3: 700. https://doi.org/10.3390/diagnostics12030700