
The Value of APTw CEST MRI in Routine Clinical Assessment of Human Brain Tumor Patients at 3T

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Magnetic Resonance Imaging (MRI) Acquisition
2.3. Chemical Exchange Saturation Transfer (CEST) Data Post-Processing and Analysis
2.4. Statistics
3. Results
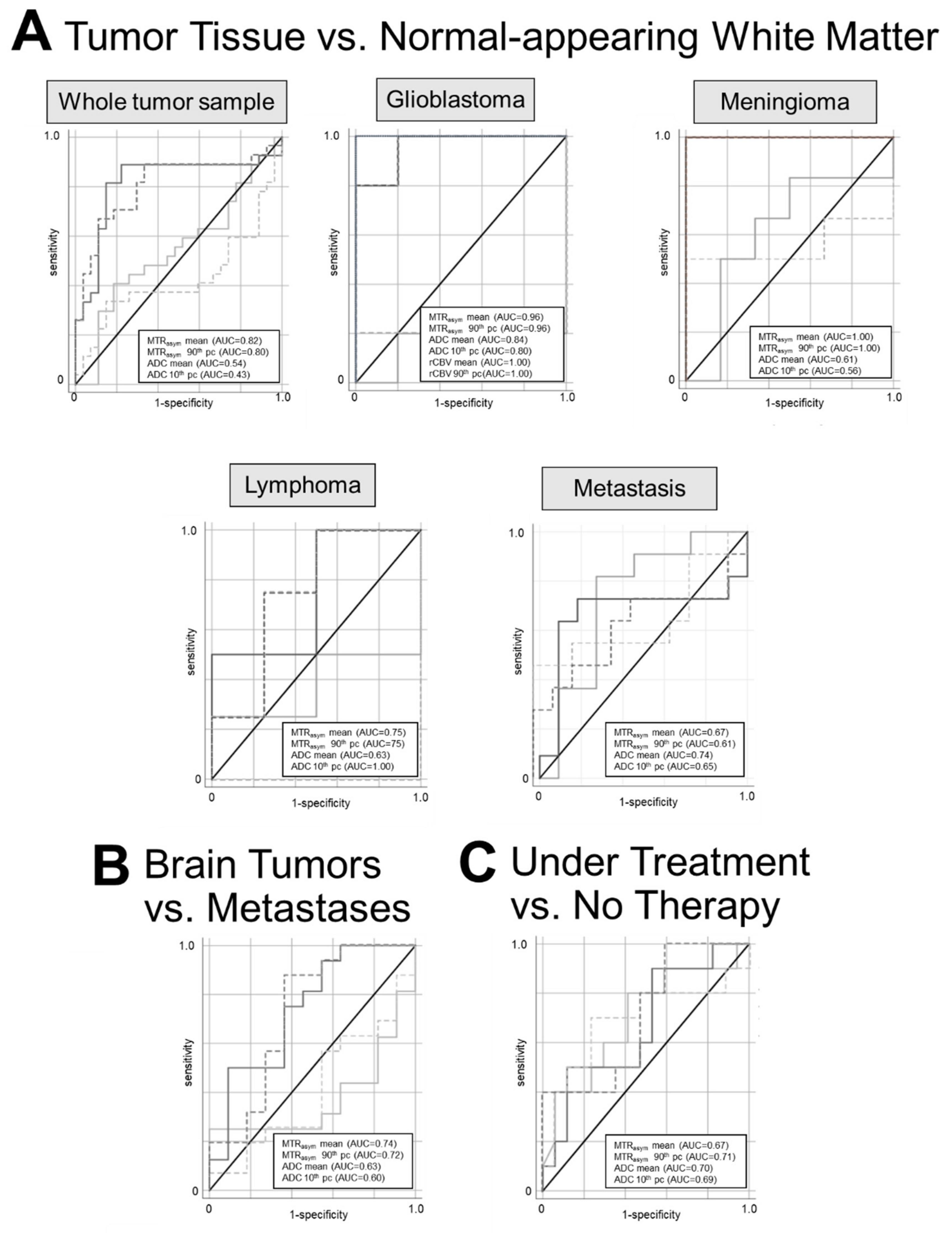
3.1. Differentiation between Tumor Tissue versus Normal-Appearing White Matter (NAWM)
3.2. Differentiation between Primary Brain Tumor vs. Brain Metastases
3.3. Differentiation between Patients with vs. without Ongoing Oncological Therapy
4. Discussion
4.1. Brain Tumor Tissue vs. NAWM
4.2. Primary Brain Tumors vs. Brain Metastases
4.3. Patients with vs. without Ongoing Oncological Therapy
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stupp, R.; Roila, F. ESMO Guidelines Working Group Malignant glioma: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2009, 20 (Suppl. S4), 126–128. [Google Scholar] [CrossRef] [PubMed]
- Mehrabian, H.; Detsky, J.; Soliman, H.; Sahgal, A.; Stanisz, G.J. Advanced Magnetic Resonance Imaging Techniques in Management of Brain Metastases. Front. Oncol. 2019, 9, 440. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Chang, S.M.; Van den Bent, M.J.; Vogelbaum, M.A.; Macdonald, D.R.; Lee, E.Q. Response Assessment in Neuro-Oncology Clinical Trials. J. Clin. Oncol. 2017, 35, 2439–2449. [Google Scholar] [CrossRef] [PubMed]
- Brandsma, D.; Stalpers, L.; Taal, W.; Sminia, P.; van den Bent, M.J. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol. 2008, 9, 453–461. [Google Scholar] [CrossRef]
- Zaiss, M.; Bachert, P. Chemical exchange saturation transfer (CEST) and MR Z-spectroscopy in vivo: A review of theoretical approaches and methods. Phys. Med. Biol. 2013, 58, R221–R269. [Google Scholar] [CrossRef]
- Dou, W.; Lin, C.Y.E.; Ding, H.; Shen, Y.; Dou, C.; Qian, L.; Wen, B.; Wu, B. Chemical exchange saturation transfer magnetic resonance imaging and its main and potential applications in pre-clinical and clinical studies. Quant. Imaging Med. Surg. 2019, 9, 1747–1766. [Google Scholar] [CrossRef]
- Wu, B.; Warnock, G.; Zaiss, M.; Lin, C.; Chen, M.; Zhou, Z.; Mu, L.; Nanz, D.; Tuura, R.; Delso, G. An overview of CEST MRI for non-MR physicists. EJNMMI Phys. 2016, 3, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Lal, B.; Wilson, D.A.; Laterra, J.; van Zijl, P.C.M. Amide proton transfer (APT) contrast for imaging of brain tumors. Magn. Reson. Med. 2003, 50, 1120–1126. [Google Scholar] [CrossRef]
- Zhou, J.; Payen, J.-F.; Wilson, D.A.; Traystman, R.J.; van Zijl, P.C.M. Using the amide proton signals of intracellular proteins and peptides to detect pH effects in MRI. Nat. Med. 2003, 9, 1085–1090. [Google Scholar] [CrossRef]
- Zhou, J.; Heo, H.Y.; Knutsson, L.; van Zijl, P.C.M.; Jiang, S. APT-weighted MRI: Techniques, current neuro applications, and challenging issues. J. Magn. Reson. Imaging 2019, 50, 347–364. [Google Scholar] [CrossRef]
- Kamimura, K.; Nakajo, M.; Yoneyama, T.; Takumi, K.; Kumagae, Y.; Fukukura, Y.; Yoshiura, T. Amide proton transfer imaging of tumors: Theory, clinical applications, pitfalls, and future directions. Jpn. J. Radiol. 2019, 37, 109–116. [Google Scholar] [CrossRef]
- Jin, T.; Wang, P.; Zong, X.; Kim, S.-G. MR imaging of the amide-proton transfer effect and the pH-insensitive nuclear overhauser effect at 9.4 T. Magn. Reson. Med. 2013, 69, 760–770. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Yu, H.; Wang, X.; Lu, S.; Li, Y.; Feng, L.; Zhang, Y.; Heo, H.-Y.; Lee, D.-H.; Zhou, J.; et al. Molecular MRI differentiation between primary central nervous system lymphomas and high-grade gliomas using endogenous protein-based amide proton transfer MR imaging at 3 Tesla. Eur. Radiol. 2016, 26, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Wen, X.; Wu, P.; Chen, Y.; Zou, T.; Wang, X.; Jiang, S.; Zhou, J.; Wen, Z. Can amide proton transfer-weighted imaging differentiate tumor grade and predict Ki-67 proliferation status of meningioma? Eur. Radiol. 2019, 29, 5298–5306. [Google Scholar] [CrossRef]
- Joo, B.; Han, K.; Choi, Y.S.; Lee, S.-K.; Ahn, S.S.; Chang, J.H.; Kang, S.-G.; Kim, S.H.; Zhou, J. Amide proton transfer imaging for differentiation of benign and atypical meningiomas. Eur. Radiol. 2018, 28, 331–339. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, H.S.; Park, S.Y.; Jung, S.C.; Kim, J.H.; Heo, H.-Y. Identification of Early Response to Anti-Angiogenic Therapy in Recurrent Glioblastoma: Amide Proton Transfer-weighted and Perfusion-weighted MRI compared with Diffusion-weighted MRI. Radiology 2020, 295, 397–406. [Google Scholar] [CrossRef]
- Mehrabian, H.; Myrehaug, S.; Soliman, H.; Sahgal, A.; Stanisz, G.J. Evaluation of Glioblastoma Response to Therapy With Chemical Exchange Saturation Transfer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 713–723. [Google Scholar] [CrossRef]
- Regnery, S.; Adeberg, S.; Dreher, C.; Oberhollenzer, J.; Meissner, J.-E.; Goerke, S.; Windschuh, J.; Deike-Hofmann, K.; Bickelhaupt, S.; Zaiss, M.; et al. Chemical exchange saturation transfer MRI serves as predictor of early progression in glioblastoma patients. Oncotarget 2018, 9, 28772–28783. [Google Scholar] [CrossRef]
- Jiang, S.; Eberhart, C.G.; Lim, M.; Heo, H.Y.; Zhang, Y.; Blair, L.; Wen, Z.; Holdhoff, M.; Lin, D.; Huang, P.; et al. Identifying recurrent malignant glioma after treatment using amide proton transfer-weighted MR imaging: A validation study with image-guided stereotactic biopsy. Clin. Cancer Res. 2019, 25, 552–561. [Google Scholar] [CrossRef] [Green Version]
- Paech, D.; Dreher, C.; Regnery, S.; Meissner, J.-E.E.; Goerke, S.; Windschuh, J.; Oberhollenzer, J.; Schultheiss, M.; Deike-Hofmann, K.; Bickelhaupt, S.; et al. Relaxation-compensated amide proton transfer (APT) MRI signal intensity is associated with survival and progression in high-grade glioma patients. Eur. Radiol. 2019, 29, 4957–4967. [Google Scholar] [CrossRef]
- Jiang, S.; Zou, T.; Eberhart, C.G.; Villalobos, M.A.V.; Heo, H.-Y.; Zhang, Y.; Wang, Y.; Wang, X.; Yu, H.; Du, Y.; et al. Predicting IDH mutation status in grade II gliomas using amide proton transfer-weighted (APTw) MRI. Magn. Reson. Med. 2017, 78, 1100–1109. [Google Scholar] [CrossRef]
- Jiang, S.; Rui, Q.; Wang, Y.; Heo, H.-Y.; Zou, T.; Yu, H.; Zhang, Y.; Wang, X.; Du, Y.; Wen, X.; et al. Discriminating MGMT promoter methylation status in patients with glioblastoma employing amide proton transfer-weighted MRI metrics. Eur. Radiol. 2018, 28, 2115–2123. [Google Scholar] [CrossRef]
- Paech, D.; Windschuh, J.; Oberhollenzer, J.; Dreher, C.; Sahm, F.; Meissner, J.E.; Goerke, S.; Schuenke, P.; Zaiss, M.; Regnery, S.; et al. Assessing the predictability of IDH mutation and MGMT methylation status in glioma patients using relaxation-compensated multipool CEST MRI at 7.0 T. Neuro. Oncol. 2018, 20, 1661–1671. [Google Scholar] [CrossRef] [Green Version]
- Nolden, M.; Zelzer, S.; Seitel, A.; Wald, D.; Müller, M.; Franz, A.M.; Maleike, D.; Fangerau, M.; Baumhauer, M.; Maier-Hein, L.; et al. The Medical Imaging Interaction Toolkit: Challenges and advances: 10 years of open-source development. Int. J. Comput. Assist. Radiol. Surg. 2013, 8, 607–620. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.; Blakeley, J.O.; Hong, X.; Zhang, H.; Jiang, S.; Blair, L.; Zhang, Y.; Heo, H.Y.; Zhang, M.; van Zijl, P.C.M.; et al. Applying amide proton transfer-weighted MRI to distinguish pseudoprogression from true progression in malignant gliomas. J. Magn. Reson. Imaging 2016, 44, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Desmond, K.L.; Mehrabian, H.; Chavez, S.; Sahgal, A.; Soliman, H.; Rola, R.; Stanisz, G.J. Chemical exchange saturation transfer for predicting response to stereotactic radiosurgery in human brain metastasis. Magn. Reson. Med. 2017, 78, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Mehrabian, H.; Lam, W.W.; Myrehaug, S.; Sahgal, A.; Stanisz, G.J. Glioblastoma (GBM) effects on quantitative MRI of contralateral normal appearing white matter. J. Neurooncol. 2018, 139, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Barajas, R.F.; Cha, S.; Cha, S. Benefits of dynamic susceptibility-weighted contrast-enhanced perfusion MRI for glioma diagnosis and therapy. CNS Oncol. 2014, 3, 407–419. [Google Scholar] [CrossRef]
- Slone, H.W.; Blake, J.J.; Shah, R.; Guttikonda, S.; Bourekas, E.C. CT and MRI Findings of Intracranial Lymphoma. Am. J. Roentgenol. 2005, 184, 1679–1685. [Google Scholar] [CrossRef]
- Huang, W.-Y.; Wen, J.-B.; Wu, G.; Yin, B.; Li, J.-J.; Geng, D.-Y. Diffusion-Weighted Imaging for Predicting and Monitoring Primary Central Nervous System Lymphoma Treatment Response. AJNR Am. J. Neuroradiol. 2016, 37, 2010–2018. [Google Scholar] [CrossRef] [Green Version]
- Kamimura, K.; Nakajo, M.; Yoneyama, T.; Fukukura, Y.; Hirano, H.; Goto, Y.; Sasaki, M.; Akamine, Y.; Keupp, J.; Yoshiura, T. Histogram analysis of amide proton transfer-weighted imaging: Comparison of glioblastoma and solitary brain metastasis in enhancing tumors and peritumoral regions. Eur. Radiol. 2019, 29, 4133–4140. [Google Scholar] [CrossRef]
- Stupp, R.; Brada, M.; van den Bent, M.J.; Tonn, J.-C.; Pentheroudakis, G. High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii93–iii101. [Google Scholar] [CrossRef]
- Calli, C.; Kitis, O.; Yunten, N.; Yurtseven, T.; Islekel, S.; Akalin, T. Perfusion and diffusion MR imaging in enhancing malignant cerebral tumors. Eur. J. Radiol. 2006, 58, 394–403. [Google Scholar] [CrossRef]
- Kono, K.; Inoue, Y.; Nakayama, K.; Shakudo, M.; Morino, M.; Ohata, K.; Wakasa, K.; Yamada, R. The role of diffusion-weighted imaging in patients with brain tumors. AJNR Am. J. Neuroradiol. 2001, 22, 1081–1088. [Google Scholar]
- Yao, J.; Tan, C.H.P.; Schlossman, J.; Chakhoyan, A.; Raymond, C.; Pope, W.B.; Salamon, N.; Lai, A.; Ji, M.; Nghiemphu, P.L.; et al. pH-weighted amine chemical exchange saturation transfer echoplanar imaging (CEST-EPI) as a potential early biomarker for bevacizumab failure in recurrent glioblastoma. J. Neurooncol. 2019, 142, 587–595. [Google Scholar] [CrossRef]
- Jones, C.K.; Huang, A.; Xu, J.; Edden, R.A.E.; Schär, M.; Hua, J.; Oskolkov, N.; Zacà, D.; Zhou, J.; McMahon, M.T.; et al. Nuclear Overhauser enhancement (NOE) imaging in the human brain at 7 T. Neuroimage 2013, 77, 114–124. [Google Scholar] [CrossRef] [Green Version]
- Meissner, J.; Korzowski, A.; Regnery, S.; Goerke, S.; Breitling, J.; Floca, R.O.; Debus, J.; Schlemmer, H.; Ladd, M.E.; Bachert, P.; et al. Early response assessment of glioma patients to definitive chemoradiotherapy using chemical exchange saturation transfer imaging at 7 T. J. Magn. Reson. Imaging 2019, 50, 1268–1277. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, H.S.; Park, K.J.; Kim, S.J.; Kim, J.H.; Smith, S.A. Pre-and posttreatment glioma: Comparison of amide proton transfer imaging with MR spectroscopy for biomarkers of tumor proliferation. Radiology 2016, 278, 514–523. [Google Scholar] [CrossRef]
- Zaiss, M.; Windschuh, J.; Goerke, S.; Paech, D.; Meissner, J.-E.; Burth, S.; Kickingereder, P.; Wick, W.; Bendszus, M.; Schlemmer, H.-P.; et al. Downfield-NOE-suppressed amide-CEST-MRI at 7 Tesla provides a unique contrast in human glioblastoma. Magn. Reson. Med. 2017, 77, 196–208. [Google Scholar] [CrossRef]
- Goerke, S.; Breitling, J.; Korzowski, A.; Paech, D.; Zaiss, M.; Schlemmer, H.P.; Ladd, M.E.; Bachert, P. Clinical routine acquisition protocol for 3D relaxation-compensated APT and rNOE CEST-MRI of the human brain at 3T. Magn. Reson. Med. 2021, 86, 393–404. [Google Scholar] [CrossRef]
- Herz, K.; Mueller, S.; Perlman, O.; Zaitsev, M.; Knutsson, L.; Sun, P.Z.; Zhou, J.; Zijl, P.; Heinecke, K.; Schuenke, P.; et al. Pulseq-CEST: Towards multi-site multi-vendor compatibility and reproducibility of CEST experiments using an open-source sequence standard. Magn. Reson. Med. 2021, 86, 1845–1858. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Number | Age (Mean + SD) | Sex (m/f) | Under Treatment vs. No Therapy | |
|---|---|---|---|---|
| Glioblastoma | 6 | 60.50 ± 4.23 | 5/1 | 4 vs. 2 |
| Lymphoma | 4 | 74.50 ± 5.69 | 1/3 | 3 vs. 1 |
| Meningioma | 6 | 59.00 ± 18.47 | 2/4 | 2 vs. 4 |
| Metastases | 11 | 61.82 ± 6.69 | 3/8 | 8 vs. 3 |
| All | 27 | 62.48 ± 10.77 | 11/16 | 17 vs. 10 |
| Comparison of Means | Sensitivity/Specificity | AUC/Cut-Off | p-Value | |
|---|---|---|---|---|
| A Tumor Tissue vs. Normal-Appearing White Matter (NAWM) | ||||
| Whole tumor sample vs. NAWM | ||||
| MTRasym mean | 0.32 vs. −0.64 | 0.89/0.78 | 0.82/−0.22 | <0.01 |
| MTRasym 90th pc | 2.27 vs. 0.77 | 0.89/0.67 | 0.80/0.96 | <0.01 |
| ADC mean | 932.71 vs. 896.71 | 0.56/0.52 | 0.54/860.18 | 0.60 |
| ADC 10th pc | 709.21 vs. 729.55 | 0.59/0.27 | 0.43/678.50 | 0.36 |
| Glioblastoma vs. NAWM | ||||
| MTRasym mean | 0.79 vs. −1.09 | 1.00/0.80 | 0.96/−0.52 | <0.01 |
| MTRasym 90th pc | 2.22 vs. 0.1 | 1.00/0.80 | 0.96/0.56 | <0.01 |
| ADC mean | 846.59 vs. 974.92 | 1.00/0.80 | 0.84/828.46 | 0.02 |
| ADC 10th pc | 777.12 vs. 869.75 | 1.00/0.80 | 0.80/726.35 | 0.09 |
| rCBVmean | 771.77 vs. 294.86 | 1.00/1.00 | 1.00/465.24 | <0.01 |
| rCBV90 | 1174.12 vs. 476.88 | 1.00/1.00 | 1.00/897.75 | <0.01 |
| Lymphoma vs. NAWM | ||||
| MTRasym mean | 0.70 vs. −0.22 | 1.00/0.50 | 0.75/−0.41 | 0.18 |
| MTRasym 90th pc | 3.07 vs. 1.52 | 1.00/0.50 | 0.75/0.96 | 0.18 |
| ADC mean | 896.57 vs. 884.56 | 1.00/0.50 | 0.63/798.87 | 0.58 |
| ADC 10th pc | 540.25 vs. 710.63 | 1.00/1.00 | 1.00/640.75 | <0.01 |
| Meningioma vs. NAWM | ||||
| MTRasym mean | 0.54 vs. −0.66 | 1.00/1.00 | 1.00/−0.01 | <0.01 |
| MTRasym 90th pc | 3.38 vs. 0.68 | 1.00/1.00 | 1.00/1.63 | <0.01 |
| ADC mean | 963.41 vs. 902.76 | 0.67/0.66 | 0.61/864.41 | 0.53 |
| ADC 10th pc | 685.7 vs. 697.67 | 0.50/0.50 | 0.56/713.00 | 0.77 |
| Metastasis vs. NAWM | ||||
| MTRasym mean | −0.2 vs. −0.53 | 0.73/0.82 | 0.67/−0.22 | 0.2 |
| MTRasym 90th pc | 1.4 vs. 0.92 | 0.73/0.55 | 0.61/0.95 | 0.38 |
| ADC mean | 976.07 vs. 855.16 | 0.82/0.73 | 0.74/847.31 | 0.04 |
| ADC 10th pc | 746.43 vs. 677.35 | 0.55/0.81 | 0.65/745.60 | 0.25 |
| B Primary Brain Tumors vs. Metastases | ||||
| MTRasym mean | 0.68 vs. −0.2 | 0.81/0.55 | 0.74/0.1 | 0.02 |
| MTRasym 90th pc | 2.86 vs. 1.4 | 0.88/0.63 | 0.72/1.54 | 0.04 |
| ADC mean | 902.19 vs. 976.07 | 0.64/0.69 | 0.63/923.33 | 0.26 |
| ADC 10th pc | 683.62 vs. 746.43 | 0.55/0.75 | 0.60/734.40 | 0.40 |
| C Under Treatment vs. No Therapy | ||||
| MTRasym mean | 0.07 vs. 0.74 | 0.60/0.53 | 0.67/0.26 | 0.12 |
| MTRasym 90th pc | 1.73 vs. 3.17 | 0.80/0.53 | 0.71/1.66 | 0.049 |
| ADC mean | 887.27 vs. 1009.95 | 0.70/0.59 | 0.70/864.98 | 0.11 |
| ADC 10th pc | 671.24 vs. 773.75 | 0.60/0.77 | 0.69/734.40 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lingl, J.P.; Wunderlich, A.; Goerke, S.; Paech, D.; Ladd, M.E.; Liebig, P.; Pala, A.; Kim, S.Y.; Braun, M.; Schmitz, B.L.; et al. The Value of APTw CEST MRI in Routine Clinical Assessment of Human Brain Tumor Patients at 3T. Diagnostics 2022, 12, 490. https://doi.org/10.3390/diagnostics12020490
Lingl JP, Wunderlich A, Goerke S, Paech D, Ladd ME, Liebig P, Pala A, Kim SY, Braun M, Schmitz BL, et al. The Value of APTw CEST MRI in Routine Clinical Assessment of Human Brain Tumor Patients at 3T. Diagnostics. 2022; 12(2):490. https://doi.org/10.3390/diagnostics12020490
Chicago/Turabian StyleLingl, Julia P., Arthur Wunderlich, Steffen Goerke, Daniel Paech, Mark E. Ladd, Patrick Liebig, Andrej Pala, Soung Yung Kim, Michael Braun, Bernd L. Schmitz, and et al. 2022. "The Value of APTw CEST MRI in Routine Clinical Assessment of Human Brain Tumor Patients at 3T" Diagnostics 12, no. 2: 490. https://doi.org/10.3390/diagnostics12020490