
Echocardiographic Assessment of Patients with Pulmonary Tumor Thrombotic Microangiopathy First Diagnosed in the Emergency Department

 , , , , ,
, , , , ,
Abstract
:1. Introduction
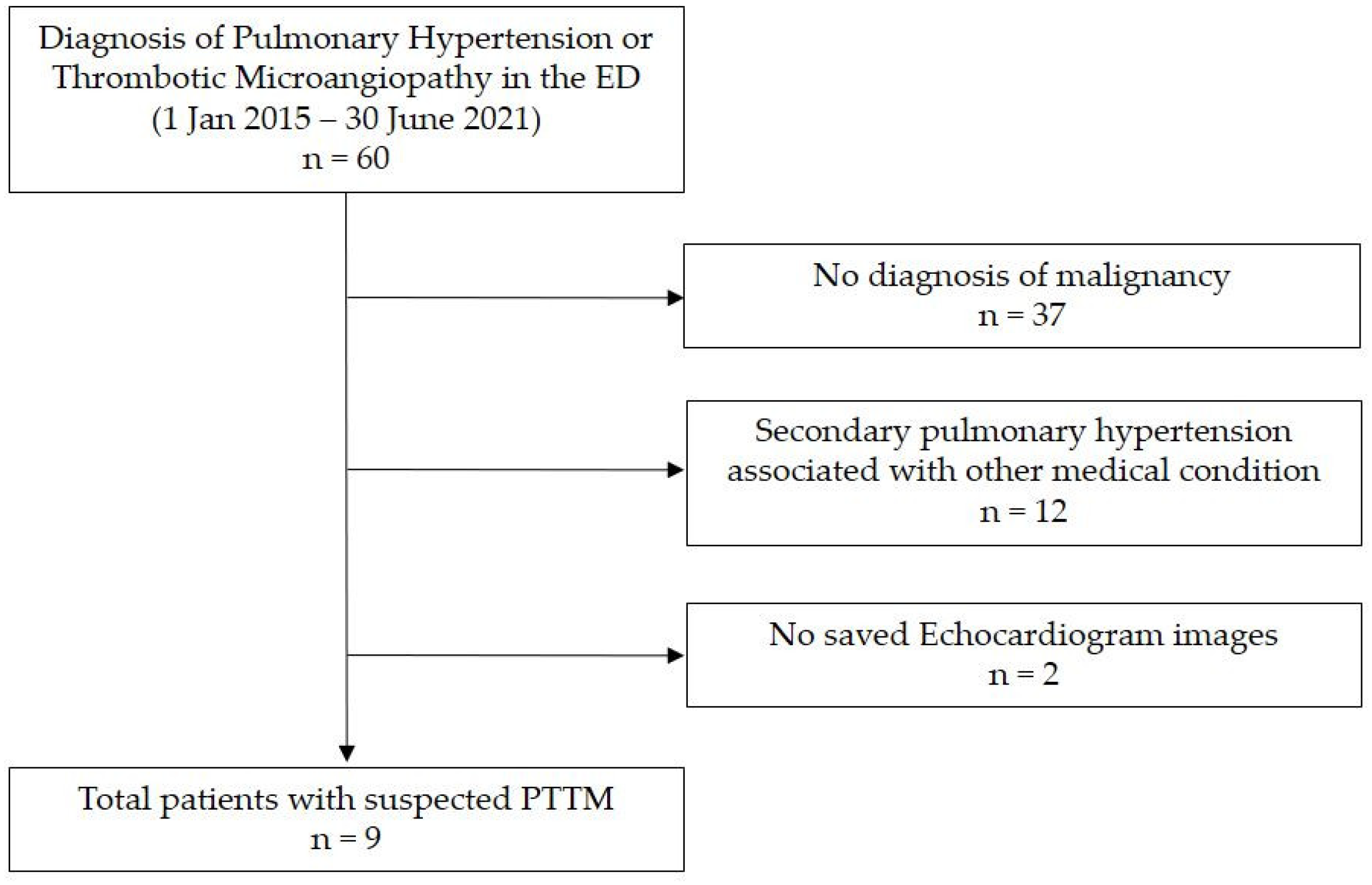
2. Materials and Methods
Data Collection
3. Results
3.1. Baseline Characteristics and Clinical Manifestations
3.2. Laboratory Tests, Plain Chest Radiography, and CT Findings
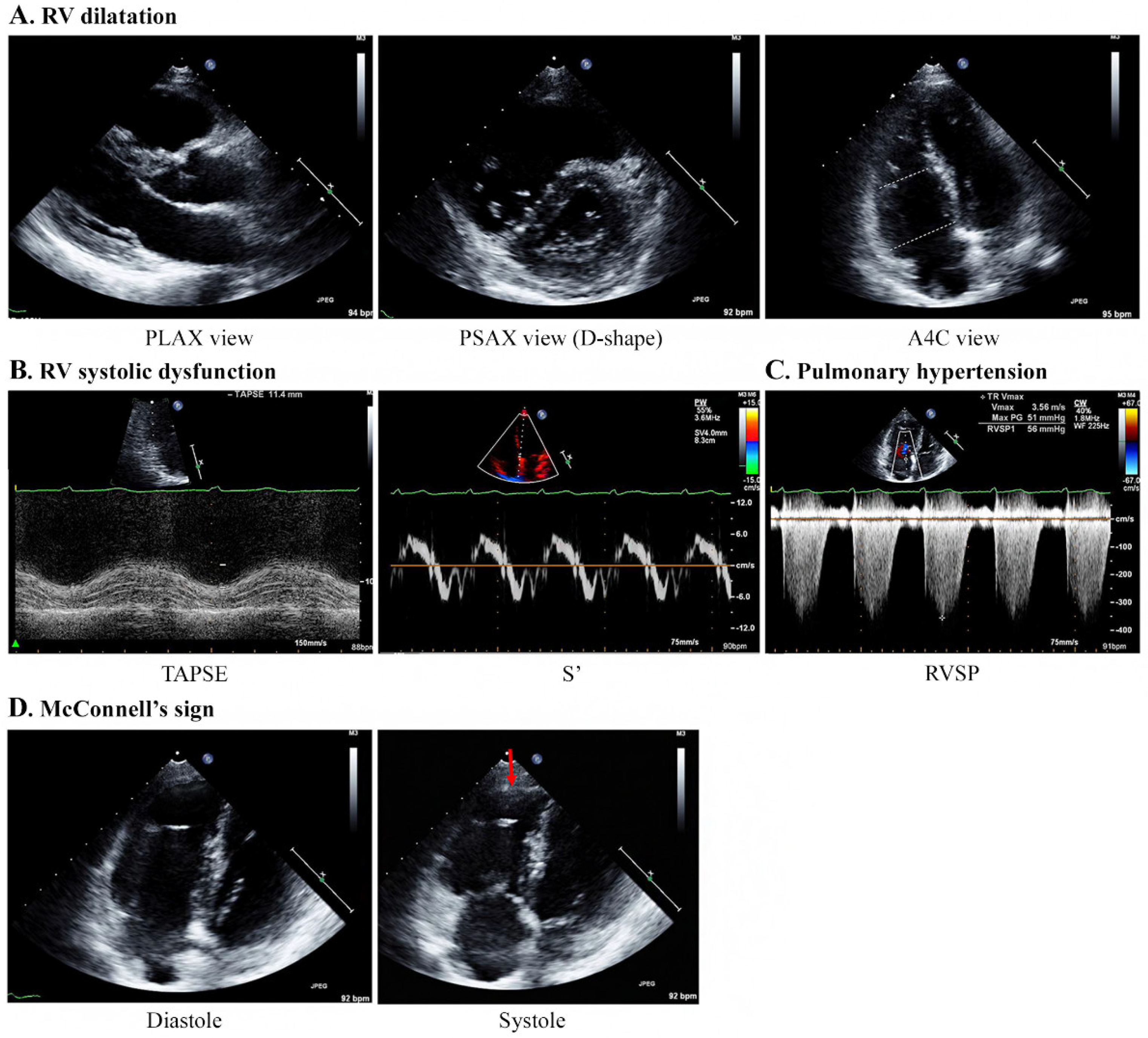
3.3. Echocardiography Findings
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Case | Hb (g/dL) | pH | pCO2 (mmHg) | pO2 (mmHg) | HCO3− (mmol/L) | BE (mmol/L) | SO2 (%) | Oxygen Applied during ABGA Sampling (/min) |
|---|---|---|---|---|---|---|---|---|
| 1 | 10.5 | 7.539 | 26.1 | 83.7 | 21.8 | 0.1 | 95.7 | FM 5 L |
| 2 | 13.8 | 7.464 | 16.6 | 58.7 | 11.6 | −9.2 | 89.5 | RA |
| 3 | 10.7 | 7.482 | 27.4 | 85.4 | 20.0 | −2.4 | 95.3 | NC 5L |
| 4 | 10.0 | 7.48 | 24 | 97 | 17.9 | −3.8 | 98.6 | NC 4 L |
| 5 | 13.2 | 7.42 | 30 | 102 | 19.5 | −3.9 | 98.3 | NC 3 L |
| 6 | 10.5 | 7.47 | 28 | 35 | 20.4 | −2.4 | 62.5 | RA |
| 7 | 8.3 | 7.535 | 24.0 | 117.3 | 19.8 | −2.1 | 97.9 | NC 5 L |
| 8 | 11.6 | 7.49 | 22 | 86 | 16.8 | −4.5 | 97.9 | FM 8 L |
| 9 | 13.2 | 7.482 | 27.9 | 116.8 | 20.4 | −1.8 | 97.8 | FM 5 L |
Appendix B. Patients with PTTM
Appendix B.1. Case 1
Appendix B.2. Case 2
Appendix B.3. Case 3
Appendix B.4. Case 4
Appendix B.5. Case 5
Appendix B.6. Case 6
Appendix B.7. Case 7
Appendix B.8. Case 8
Appendix B.9. Case 9
References
- Godbole, R.H.; Saggar, R.; Kamangar, N. Pulmonary tumor thrombotic microangiopathy: A systematic review. Pulm. Circ. 2019, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Price, L.C.; Wells, A.U.; Wort, S.J. Pulmonary tumour thrombotic microangiopathy. Curr. Opin. Pulm. Med. 2016, 22, 421–428. [Google Scholar] [CrossRef]
- Mitsui, Y.; Yagi, M.; Muraki, S.; Matsuura, T.; Bando, Y.; Fujimoto, S.; Kitamura, S.; Okamoto, K.; Muguruma, N.; Sata, M.; et al. Pulmonary Tumor Thrombotic Microangiopathy Due to Gastric Cancer Diagnosed Antemortem by a Cytological Examination of Aspirated Pulmonary Artery Blood. Intern. Med. 2021, 8313–8321. [Google Scholar] [CrossRef]
- Takada, N.; Nishida, H.; Kondo, Y.; Oyama, Y.; Kusaba, T.; Kadowaki, H.; Hirakawa, K.; Iwao, S.; Kiyooka, S.; Daa, T. Pulmonary wedge aspiration cytology for the rapid diagnosis of pulmonary tumor thrombotic microangiopathy: A case report. Diagn. Cytopathol. 2021, 49, E277–E280. [Google Scholar] [CrossRef]
- Lee, L.; DeCara, J.M. Point-of-Care Ultrasound. Curr. Cardiol. Rep. 2020, 22, 1–10. [Google Scholar] [CrossRef]
- Ha, Y.-R.; Toh, H.-C. Clinically integrated multi-organ point-of-care ultrasound for undifferentiated respiratory difficulty, chest pain, or shock: A critical analytic review. J. Intensiv. Care 2016, 4, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Marbach, J.A.; Almufleh, A.; Di Santo, P.; Simard, T.; Jung, R.; Diemer, G.; West, F.M.; Millington, S.J.; Mathew, R.; Le May, M.R.; et al. A Shifting Paradigm: The Role of Focused Cardiac Ultrasound in Bedside Patient Assessment. Chest 2020, 158, 2107–2118. [Google Scholar] [CrossRef] [PubMed]
- Pirozzi, C.; Numis, F.G.; Pagano, A.; Melillo, P.; Copetti, R.; Schiraldi, F. Immediate versus delayed integrated point-of-care-ultrasonography to manage acute dyspnea in the emergency department. Crit. Ultrasound J. 2014, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Herbay, A.; Illes, A.; Waldherr, R.; Otto, H.F. Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension. Cancer 1990, 66, 587–592. [Google Scholar] [CrossRef]
- Oh, J. Echocardiography in heart failure: Beyond diagnosis. Eur. J. Echocardiogr. 2007, 8, 4–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godbole, R.; Ghatol, A.; Betancourt, J.; Sacoolidge, J.; Kamangar, N. Pulmonary Tumor Thrombotic Microangiopathy: Clinical, Radiologic, and Histologic Correlation. J. Clin. Imaging Sci. 2015, 5, 44. [Google Scholar] [CrossRef]
- Kridel, R.; Myit, S.; Pache, J.-C.; Gaspoz, J.-M. Pulmonary Tumor Embolism: A Rare Cause of Acute Right Heart Failure with Elevated d-Dimers. J. Thorac. Oncol. 2008, 3, 1482–1483. [Google Scholar] [CrossRef] [PubMed]
- Aoki, R.; Yanagihara, T.; Mannoji, H.; Sunami, S.; Tsuruta, N.; Yoneda, R.; Usui, M. Pulmonary tumor embolism from breast cancer diagnosed by selective aspiration cytology using a Swan-Ganz catheter. Respir. Med. Case Rep. 2021, 34, 101527. [Google Scholar] [CrossRef] [PubMed]
- Keenan, N.; Nicholson, A.; Oldershaw, P. Fatal acute pulmonary hypertension caused by pulmonary tumour thrombotic microangiopathy. Int. J. Cardiol. 2008, 124, e11–e13. [Google Scholar] [CrossRef]
- Patrignani, A.; Purcaro, A.; Calcagnoli, F.; Mandolesi, A.; Bearzi, I.; Ciampani, N. Pulmonary tumor thrombotic microangiopathy. J. Cardiovasc. Med. 2014, 15, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, S.; Ikeda, T.; Ito, G.; Inoue, M.; Nara, K.; Nishinaga, Y.; Hasegawa, Y. Pulmonary tumor thrombotic microangiopathy successfully treated with corticosteroids: A case report. J. Med. Case Rep. 2017, 11, 356. [Google Scholar] [CrossRef]
- Yoo, S.-H.; Park, K.; Hong, J.Y.; Kim, J.Y.; Park, J.W.; Park, Y.W.; Lee, K.-H.; Jeon, K.-S. Pulmonary Tumor Thrombotic Microangiopathy Associated with Advanced Gastric Cancer Successfully Treated with Chemotherapy. EMJ 2014, 37, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Morin-Thibault, L.V.; Wiseman, D.; Joubert, P.; Paulin, R.; Bonnet, S.; Provencher, S. Pulmonary tumor thrombotic microangiopathy: A systematic review of the literature. Can. J. Respir. Crit. Care Sleep Med. 2021, 5, 20–27. [Google Scholar] [CrossRef]
- Lu, L.; Wang, Z.; Li, H.; Li, X.; Ma, S.; Wang, L.; Yang, B. Bevacizumab combined with pemetrexed successfully treated lung adenocarcinoma complicated with pulmonary tumor thrombotic microangiopathy: A case report and literature review. Ann. Palliat. Med. 2021, 10, 767–777. [Google Scholar] [CrossRef]
- Chae, E.J.; Seo, J.B.; Jang, Y.M.; Krauss, B.; Lee, C.W.; Lee, H.J.; Song, K.-S. Dual-Energy CT for Assessment of the Severity of Acute Pulmonary Embolism: Pulmonary Perfusion Defect Score Compared with CT Angiographic Obstruction Score and Right Ventricular/Left Ventricular Diameter Ratio. Am. J. Roentgenol. 2010, 194, 604–610. [Google Scholar] [CrossRef]
- Tashima, Y.; Abe, K.; Matsuo, Y.; Baba, S.; Kaneko, K.; Isoda, T.; Yabuuchi, H.; Sasaki, M.; Honda, H. Pulmonary Tumor Thrombotic Microangiopathy: FDG-PET/CT Findings. Clin. Nucl. Med. 2009, 34, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Kamada, H.; Ota, H.; Terui, Y.; Sugimura, K.; Fukui, S.; Shimokawa, H.; Takase, K. Three cases of pulmonary tumor thrombotic microangiopathy (PTTM): Challenge in antemortem diagnosis using lung perfusion blood volume images by dual-energy computed tomography. Eur. J. Radiol. Open 2020, 7, 100212. [Google Scholar] [CrossRef]
- Mediratta, A.; Addetia, K.; Medvedofsky, D.; Gomberg-Maitland, M.; Mor-Avi, V.; Lang, R.M. Echocardiographic Diagnosis of Acute Pulmonary Embolism in Patients with McConnell’s Sign. Echocardiography 2016, 33, 696–702. [Google Scholar] [CrossRef]
- Zuin, R.; Zonzin, P.; Zuliani, G.; Roncon, L. Bedside diagnosis of acute pulmonary embolism: The McConnell’s sign. Qjm: Int. J. Med. 2021, 114, 525–526. [Google Scholar] [CrossRef]
- Oh, S.B.; Bang, S.J.; Kim, M.J. McConnell’s sign; a distinctive echocardiographic finding for diagnosing acute pulmonary embolism in emergency department. Crit. Ultrasound J. 2015, 7, A20. [Google Scholar] [CrossRef] [Green Version]
- Ashraf, H.; Rosenthal, J.L. Right Heart Failure. Cardiol. Clin. 2020, 38, 175–183. [Google Scholar] [CrossRef]
- Arrigo, M.; Huber, L.C.; Winnik, S.; Mikulicic, F.; Guidetti, F.; Frank, M.; Flammer, A.J.; Ruschitzka, F. Right Ventricular Failure: Pathophysiology, Diagnosis and Treatment. Card. Fail. Rev. 2019, 5, 140–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieillard-Baron, A.; Naeije, R.; Haddad, F.; Bogaard, H.J.; Bull, T.M.; Fletcher, N.; Lahm, T.; Magder, S.; Orde, S.; Schmidt, G.; et al. Diagnostic workup, etiologies and management of acute right ventricle failure. Intensiv. Care Med. 2018, 44, 774–790. [Google Scholar] [CrossRef]
- Ibrahim, B.S. Right ventricular failure. E-J. Cardiol. Pract. 2016, 14, 32. [Google Scholar]



| Case | Age (year) | Sex | PH History | Malignancy Diagnosis before ED | Dyspnea Exacerbation (days) | Oxygen Needs (/min) | D-Dimer (μg/mL) | NT-Pro BNP (pg/mL) | Primary Malignancy | ChemoTx. Initiation Time from ED | Death | Time to Death (days) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 40 | F | − | + | 3 | FM 5 L | 3.41 | 3664 | Breast Ca. | − | + | 2 |
| 2 | 47 | F | − | − | 10 | FM 15 L | 4.28 | 8153 | Ovarian Ca. | − | + | 1 |
| 3 | 59 | F | − | + | 7 | HFNC | 25.09 | 4253 | Breast Ca. | − | + | 3 |
| 4 | 41 | F | − | − | 3 | NC 4 L | 60.00 | 4273 | MUO | − | + | 3 |
| 5 | 59 | F | − | + | 1 | NC 3 L | 6.64 | 9130 | Breast Ca. | 24 h | − | − |
| 6 | 43 | F | − | + | 2 | FM 15 L | 16.52 | 5311 | Gastric Ca. | 48 h | − | − |
| 7 | 54 | F | − | + | 1 | NC 5 L | 6.18 | 1728 | Breast Ca. | − | + | N/A |
| 8 | 73 | F | − | + | 2 | FM 8 L | 28.11 | 21,925 | Gastric Ca. | − | + | 1 |
| 9 | 53 | M | − | + | 14 | FM 5 L | 17.98 | 1520 | Bladder Ca. | − | + | 3 |
| Case | Plain Radiography | Computed Tomography | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cardiomegaly | Pulmonary Trunk Enlargement | Abnormal Findings | RV Inner Cavity (cm) | LV Inner Cavity (cm) | RV: LV Ratio | PTE | Vascular Tree-in-Bud Sign | Centri- Lobular GGNs <3 mm | Peripheral Wedge GGOs | Interstitial Thickening | Consolidation | |
| 1 | − | + | − | 4.1 | 3.4 | 1.2 | − | − | Diffuse | − | − | − |
| 2 | + | + | − | 4.3 | 2.8 | 1.5 | − | − | - | − | − | − |
| 3 | − | − | − | 3.5 | 1.9 | 1.8 | − | − | Several random | + | − | − |
| 4 | + | − | − | 3.2 | 2.0 | 1.6 | + | + | Diffuse | − | + | − |
| 5 | + | − | − | 3.3 | 2.7 | 1.2 | − | + | Diffuse | + | − | − |
| 6 | + | + | GGOs, pleural effusion | 4.4 | 3.0 | 1.5 | − | + | Several segmental | + | − | + |
| 7 | − | + | − | 3.6 | 3.1 | 1.2 | − | − | Diffuse | + | − | − |
| 8 | − | + | Interstitial thickening | 4.1 | 1.8 | 2.3 | − | + | Diffuse | + | + | − |
| 9 | − | − | − | 3.7 | 1.6 | 2.3 | − | + | Diffuse | − | − | − |
| Case | LV | RV | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Size | EF * (%) | Diastolic Function (e/e′) | RV Dilatation † | Size (Base/Mid) (mm) | D-Shape | TAPSE (mm) | S′ (cm/s) | TR Vmax (m/s) | RVSP (mmHg) | McConnell’s Sign | |
| 1 | Normal | 62 | 7.1 | Moderate | 40/29 | + | 11.4 | 7.7 | 3.56 | 56 | + |
| 2 | Normal | Normal | N/A | Severe | N/A | + | 8 | N/A | 3.6 | 60 | − |
| 3 | Normal | 67 | N/A | Severe | 42/33 | + | 21.1 | 11.9 | 4.5 | 87 | + |
| 4 | Normal | 63 | N/A | Severe | 42/39 | + | 16.4 | N/A | 3.7 | 72 | + |
| 5 | Normal | 57 | N/A | Severe | 50/34 | + | 17 | 11.3 | 3.82 | 64 | + |
| 6 | Normal | 58 | 5.7 | Moderate | 44/37 | + | 15.3 | N/A | 3.43 | 62 | + |
| 7 | Normal | 56 | 8.9 | Moderate | 45/37 | + | N/A | N/A | 3.49 | 54 | − |
| 8 | Normal | Normal | N/A | Severe | N/A | + | N/A | N/A | N/A | N/A | − |
| 9 | Normal | 56 | 5.8 | Moderate | 42/31 | + | 13.5 | 10.6 | 4.91 | 93 | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Yoon, H.; Kim, M.Y.; Jo, I.J.; Kang, S.Y.; Lee, G.; Park, J.E.; Kim, T.; Lee, S.U.; Hwang, S.Y.; et al. Echocardiographic Assessment of Patients with Pulmonary Tumor Thrombotic Microangiopathy First Diagnosed in the Emergency Department. Diagnostics 2022, 12, 259. https://doi.org/10.3390/diagnostics12020259
Kim M, Yoon H, Kim MY, Jo IJ, Kang SY, Lee G, Park JE, Kim T, Lee SU, Hwang SY, et al. Echocardiographic Assessment of Patients with Pulmonary Tumor Thrombotic Microangiopathy First Diagnosed in the Emergency Department. Diagnostics. 2022; 12(2):259. https://doi.org/10.3390/diagnostics12020259
Chicago/Turabian StyleKim, Minjoo, Hee Yoon, Min Yeong Kim, Ik Joon Jo, Soo Yeon Kang, Guntak Lee, Jong Eun Park, Taerim Kim, Se Uk Lee, Sung Yeon Hwang, and et al. 2022. "Echocardiographic Assessment of Patients with Pulmonary Tumor Thrombotic Microangiopathy First Diagnosed in the Emergency Department" Diagnostics 12, no. 2: 259. https://doi.org/10.3390/diagnostics12020259