
Artificial Intelligence in Emergency Radiology: Where Are We Going?
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. AI basic Terminology
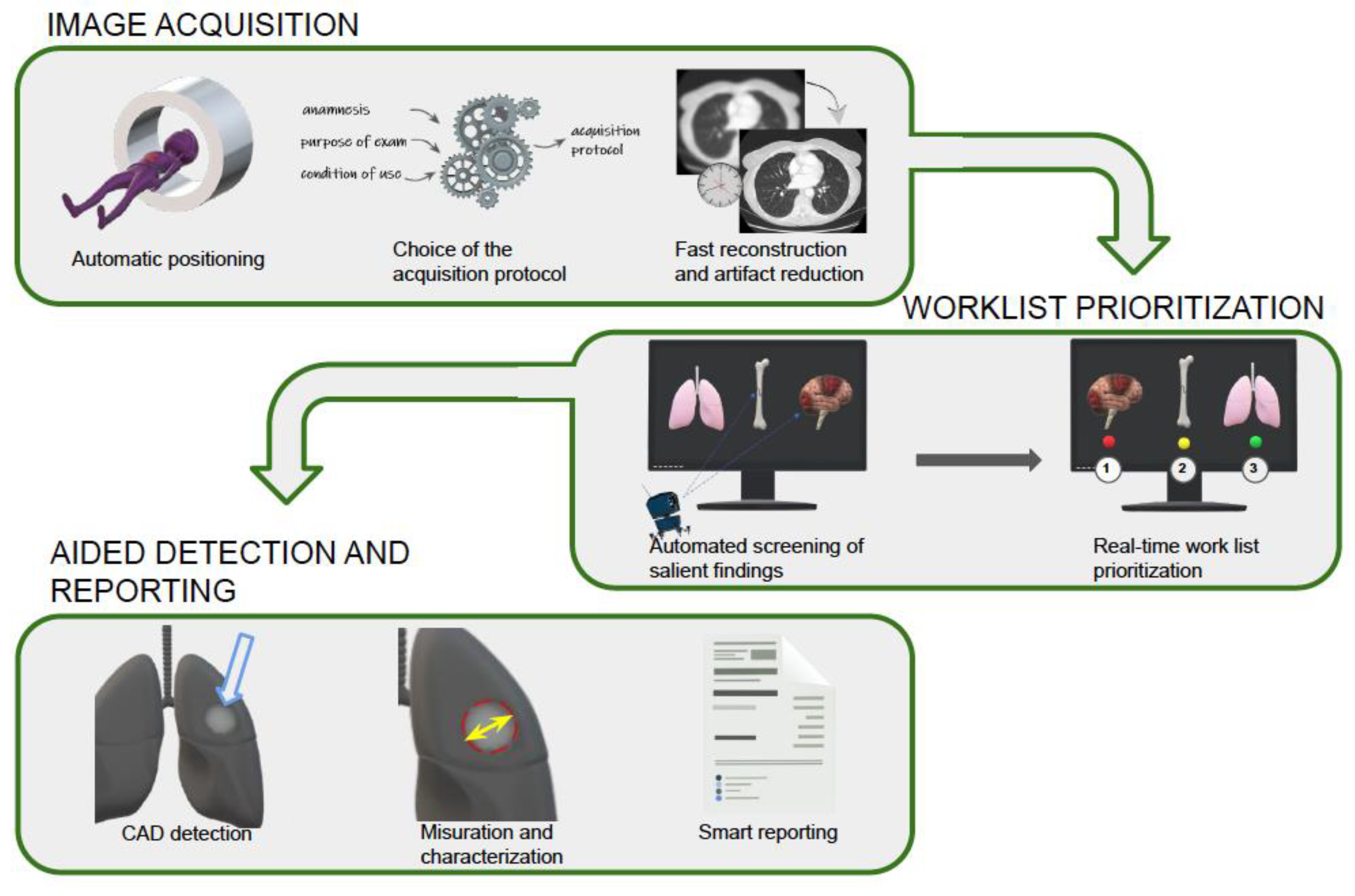
3. AI in Image Acquisition
4. Worklist Prioritization
5. Automatic Detection
5.1. Stroke
5.2. Trauma and Bone Fractures
5.3. Abdominal Emergencies
5.3.1. Abdominal Trauma
5.3.2. Small Bowel Occlusion
5.3.3. Intussusception
5.4. Chest Emergencies
5.4.1. Pulmonary Embolism
5.4.2. Pneumonia
6. Smart Reporting
7. Challenges and Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Center for Health Statistics. National Hospital Ambulatory Medical Care Survey: 2018 Emergency Department Summary Tables. 2018. Available online: https://ftp.cdc.gov/pub/Health_ (accessed on 26 October 2022).
- Tadavarthi, Y.; Makeeva, V.; Wagstaff, W.; Zhan, H.; Podlasek, A.; Bhatia, N.; Heilbrun, M.; Krupinski, E.; Safdar, N.; Banerjee, I.; et al. Overview of Noninterpretive Artificial Intelligence Models for Safety, Quality, Workflow, and Education Applications in Radiology Practice. Radiol. Artif. Intell. 2022, 4. [Google Scholar] [CrossRef] [PubMed]
- García-Gigorro, R.; Vigo, F.D.L.C.; Andrés-Esteban, E.; Chacón-Alves, S.; Varas, G.M.; Sánchez-Izquierdo, J.; González, J.M. Impact on patient outcome of emergency department length of stay prior to ICU admission. Med. Intensiv. 2017, 41, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Katzman, B.D.; van der Pol, C.B.; Soyer, P.; Patlas, M.N. Artificial intelligence in emergency radiology: A review of applications and possibilities. Diagn. Interv. Imaging 2022, in press. [Google Scholar] [CrossRef]
- Annarumma, M.; Withey, S.J.; Bakewell, R.J.; Pesce, E.; Goh, V.; Montana, G. Automated Triaging of Adult Chest Radiographs with Deep Artificial Neural Networks. Radiology 2019, 291, 272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artificial Intelligence: Can It Replace Human Intelligence?—MIT—Centre for Future Skills Excellence. Available online: https://mitfutureskills.org/blog/artificial-intelligence-can-it-replace-human-intelligence/ (accessed on 26 October 2022).
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, A. Machine Learning: The Basics; Springer Nature: Berlin/Heidelberg, Germany, 2022; Available online: https://books.google.com/books/about/Machine_Learning.html?hl=it&id=1IBaEAAAQBAJ (accessed on 26 October 2022).
- Tan, P.N.; Steinbach, M.; Karpatne, A.; Kumar, V. Introduction To Data Mining; Pearson: London, UK, 2018. [Google Scholar]
- Cellina, M.; Cè, M.; Irmici, G.; Ascenti, V.; Khenkina, N.; Toto-Brocchi, M.; Martinenghi, C.; Papa, S.; Carrafiello, G. Artificial Intelligence in Lung Cancer Imaging: Unfolding the Future. Diagnostics 2022, 12, 2644. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.; Guido, S. Introduction to Machine Learning with Python: A Guide for Data Scientists; O’Reilly Media: Sebastopol, CA, USA, 2016. [Google Scholar]
- Chollet, F. Deep Learning with Python; Manning Publications: Shelter Island, NY, USA, 2017; Available online: https://www.manning.com/books/deep-learning-with-python (accessed on 26 October 2022).
- Parekh, V.S.; Jacobs, M.A. Deep learning and radiomics in precision medicine. Expert Rev. Precis. Med. Drug Dev. 2019, 4, 59–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicini, S.; Bortolotto, C.; Rengo, M.; Ballerini, D.; Bellini, D.; Carbone, I.; Preda, L.; Laghi, A.; Coppola, F.; Faggioni, L. A narrative review on current imaging applications of artificial intelligence and radiomics in oncology: Focus on the three most common cancers. La Radiol. Med. 2022, 127, 819–836. [Google Scholar] [CrossRef]
- Hassan, A.I.; Skalej, M.; Schlattl, H.; Hoeschen, C. Determination and verification of the x-ray spectrum of a CT scanner. J. Med. Imaging 2018, 5, 1. [Google Scholar] [CrossRef]
- Saltybaeva, N.; Schmidt, B.; Wimmer, A.; Flohr, T.; Alkadhi, H. Precise and Automatic Patient Positioning in Computed Tomography: Avatar Modeling of the Patient Surface Using a 3-Dimensional Camera. Investig. Radiol. 2018, 53, 641–646. [Google Scholar] [CrossRef]
- Booij, R.; Budde, R.P.; Dijkshoorn, M.L.; van Straten, M. Accuracy of automated patient positioning in CT using a 3D camera for body contour detection. Eur. Radiol. 2019, 29, 2079–2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gang, Y.; Chen, X.; Li, H.; Wang, H.; Li, J.; Guo, Y.; Zeng, J.; Hu, Q.; Hu, J.; Xu, H. A comparison between manual and artificial intelligence-based automatic positioning in CT imaging for COVID-19 patients. Eur. Radiol. 2021, 31, 6049–6058. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Suehling, M.; Flohr, T.; Comaniciu, D. Artificial Intelligence in Diagnostic Imaging: Status Quo, Challenges, and Future Opportunities. J. Thorac. Imaging 2020, 35 (Suppl. 1), S11–S16. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Leng, S. Use of artificial intelligence in computed tomography dose optimisation. Ann. ICRP 2020, 49 (Suppl. 1), 113–125. [Google Scholar] [CrossRef] [PubMed]
- Suyudi, I.; Anam, C.; Sutanto, H.; Triadyaksa, P.; Fujibuchi, T. Comparisons of hounsfield unit linearity between images reconstructed using an adaptive iterative dose reduction (AIDR) and a filter back-projection (FBP) techniques. J. Biomed. Phys. Eng. 2020, 10, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Agostini, A.; Borgheresi, A.; Carotti, M.; Ottaviani, L.; Badaloni, M.; Floridi, C.; Giovagnoni, A. Third-generation iterative reconstruction on a dual-source, high-pitch, low-dose chest CT protocol with tin filter for spectral shaping at 100 kV: A study on a small series of COVID-19 patients. Radiol. Med. 2021, 126, 388–398. [Google Scholar] [CrossRef]
- Stiller, W. Basics of iterative reconstruction methods in computed tomography: A vendor-independent overview. Eur. J. Radiol. 2018, 109, 147–154. [Google Scholar] [CrossRef]
- Mohammadinejad, P.; Mileto, A.; Yu, L.; Leng, S.; Guimaraes, L.S.; Missert, A.D.; Jensen, C.T.; Gong, H.; McCollough, C.H.; Fletcher, J.G. CT Noise-Reduction Methods for Lower-Dose Scanning: Strengths and Weaknesses of Iterative Reconstruction Algorithms and New Techniques. Radiographics 2021, 41, 1493–1508. [Google Scholar] [CrossRef]
- Padole, A.; Khawaja, R.D.A.; Kalra, M.K.; Singh, S. CT Radiation Dose and Iterative Reconstruction Techniques. Am. J. Roentgenol. 2015, 204, W384–W392. [Google Scholar] [CrossRef]
- Sun, J.; Li, H.; Gao, J.; Li, J.; Li, M.; Zhou, Z.; Peng, Y. Performance evaluation of a deep learning image reconstruction (DLIR) algorithm in “double low” chest CTA in children: A feasibility study. La Radiol. Med. 2021, 126, 1181–1188. [Google Scholar] [CrossRef]
- Park, C.; Choo, K.S.; Jung, Y.; Jeong, H.S.; Hwang, J.-Y.; Yun, M.S. CT iterative vs. deep learning reconstruction: Comparison of noise and sharpness. Eur. Radiol. 2021, 31, 3156–3164. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.K.C. Artificial Intelligence for Radiation Dose Optimization in Pediatric Radiology: A Systematic Review. Children 2022, 9, 1044. [Google Scholar] [CrossRef] [PubMed]
- McLeavy, C.; Chunara, M.; Gravell, R.; Rauf, A.; Cushnie, A.; Talbot, C.S.; Hawkins, R. The future of CT: Deep learning reconstruction. Clin. Radiol. 2021, 76, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Greffier, J.; Si-Mohamed, S.; Frandon, J.; Loisy, M.; de Oliveira, F.; Beregi, J.P.; Dabli, D. Impact of an artificial intelligence deep-learning reconstruction algorithm for CT on image quality and potential dose reduction: A phantom study. Med. Phys. 2022, 49, 5052–5063. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, D.; Ozawa, S.; Yokomachi, K.; Higaki, T.; Shiinoki, T.; Saito, A.; Kimura, T.; Nishibuchi, I.; Takahashi, I.; Takeuchi, Y.; et al. Metal artifact reduction techniques for single energy CT and dual-energy CT with various metal materials. BJR|Open 2019, 1, bjro.20180045. [Google Scholar] [CrossRef]
- Baltruschat, I.; Steinmeister, L.; Nickisch, H.; Saalbach, A.; Grass, M.; Adam, G.; Knopp, T.; Ittrich, H. Smart chest X-ray worklist prioritization using artificial intelligence: A clinical workflow simulation. Eur. Radiol. 2021, 31, 3837–3845. [Google Scholar] [CrossRef]
- Davis, M.A.; Rao, B.; Cedeno, P.A.; Saha, A.; Zohrabian, V.M. Machine Learning and Improved Quality Metrics in Acute Intracranial Hemorrhage by Noncontrast Computed Tomography. Curr. Probl. Diagn. Radiol. 2022, 51, 556–561. [Google Scholar] [CrossRef]
- Kao, E.F.; Liu, G.C.; Lee, L.Y.; Tsai, H.Y.; Jaw, T.S. Computer-aided detection system for chest radiography: Reducing report turnaround times of examinations with abnormalities. Acta Radiol. 2015, 56, 696–701. [Google Scholar] [CrossRef]
- Winkel, D.J.; Heye, T.; Weikert, T.J.; Boll, D.T.; Stieltjes, B. Evaluation of an AI-Based Detection Software for Acute Findings in Abdominal Computed Tomography Scans: Toward an Automated Work List Prioritization of Routine CT Examinations. Investig. Radiol. 2019, 54, 55–59. [Google Scholar] [CrossRef]
- Do, H.M.; Spear, L.G.; Nikpanah, M.; Mirmomen, S.M.; Machado, L.B.; Toscano, A.P.; Turkbey, B.; Bagheri, M.H.; Gulley, J.L.; Folio, L.R. Augmented Radiologist Workflow Improves Report Value and Saves Time: A Potential Model for Implementation of Artificial Intelligence. Acad. Radiol. 2020, 27, 96–105. [Google Scholar] [CrossRef]
- Prevedello, L.M.; Erdal, B.S.; Ryu, J.L.; Little, K.J.; Demirer, M.; Qian, S.; White, R.D. Automated Critical Test Findings Identification and Online Notification System Using Artificial Intelligence in Imaging. Radiology 2017, 285, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Arbabshirani, M.R.; Fornwalt, B.K.; Mongelluzzo, G.J.; Suever, J.D.; Geise, B.D.; Patel, A.A.; Moore, G.J. Advanced machine learning in action: Identification of intracranial hemorrhage on computed tomography scans of the head with clinical workflow integration. NPJ Digit. Med. 2018, 1, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, N.W.; Sheehan, T.O.; Guo, Y.; Kelly, D.L.; Horgas, A.L.; Yoon, S.L. Factors Associated With Emergency Department Length of Stay and In-hospital Mortality in Intracerebral Hemorrhage Patients. J. Neurosci. Nurs. 2021, 53, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Ro, Y.S.; Park, J.H.; Jeong, J.; Shin, S.D.; Moon, S. Association between time to emergency neurosurgery and clinical outcomes for spontaneous hemorrhagic stroke: A nationwide observational study. PLoS ONE 2022, 17, e0267856. [Google Scholar] [CrossRef] [PubMed]
- Marra, P.; Muscogiuri, G.; Sironi, S. Advanced neuroimaging in stroke patients management: It is not just a matter of time. J. Clin. Ultrasound 2022, 50, 182–184. [Google Scholar] [CrossRef]
- Soun, J.; Chow, D.; Nagamine, M.; Takhtawala, R.; Filippi, C.; Yu, W.; Chang, P. Artificial Intelligence and Acute Stroke Imaging. AJNR Am. J. Neuroradiol. 2021, 42, 2–11. [Google Scholar] [CrossRef]
- Matsoukas, S.; Scaggiante, J.; Schuldt, B.R.; Smith, C.J.; Chennareddy, S.; Kalagara, R.; Majidi, S.; Bederson, J.B.; Fifi, J.T.; Mocco, J.; et al. Accuracy of artificial intelligence for the detection of intracranial hemorrhage and chronic cerebral microbleeds: A systematic review and pooled analysis. Radiol. Med. 2022, 127, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Rava, R.A.; Seymour, S.E.; LaQue, M.E.; Peterson, B.A.; Snyder, K.V.; Mokin, M.; Waqas, M.; Hoi, Y.; Davies, J.M.; Levy, E.I.; et al. Assessment of an Artificial Intelligence Algorithm for Detection of Intracranial Hemorrhage. World Neurosurg. 2021, 150, e209–e217. [Google Scholar] [CrossRef]
- Ginat, D.T. Analysis of head CT scans flagged by deep learning software for acute intracranial hemorrhage. Neuroradiology 2020, 62, 335–340. [Google Scholar] [CrossRef]
- McLouth, J.; Elstrott, S.; Chaibi, Y.; Quenet, S.; Chang, P.D.; Chow, D.S.; Soun, J.E. Validation of a Deep Learning Tool in the Detection of Intracranial Hemorrhage and Large Vessel Occlusion. Front. Neurol. 2021, 12, 655. [Google Scholar] [CrossRef]
- Verdolotti, T.; Pilato, F.; Cottonaro, S.; Monelli, E.; Giordano, C.; Guadalupi, P.; Benenati, M.; Ramaglia, A.; Costantini, A.M.; Alexandre, A.; et al. ColorViz, a New and Rapid Tool for Assessing Collateral Circulation during Stroke. Brain Sci. 2020, 10, 882. [Google Scholar] [CrossRef] [PubMed]
- Stinner, D.J.; Edwards, D. Surgical Management of Musculoskeletal Trauma. Surg Clin. N. Am. 2017, 97, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Laur, O.; Wang, B. Musculoskeletal trauma and artificial intelligence: Current trends and projections. Skelet. Radiol. 2022, 51, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Klontzas, M.E.; Papadakis, G.Z.; Marias, K.; Karantanas, A.H. Musculoskeletal trauma imaging in the era of novel molecular methods and artificial intelligence. Injury 2020, 51, 2748–2756. [Google Scholar] [CrossRef] [PubMed]
- Hirschmann, A.; Cyriac, J.; Stieltjes, B.; Kober, T.; Richiardi, J.; Omoumi, P. Artificial Intelligence in Musculoskeletal Imaging: Review of Current Literature, Challenges, and Trends. Semin. Musculoskelet. Radiol. 2019, 23, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Chea, P.; Mandell, J.C. Current applications and future directions of deep learning in musculoskeletal radiology. Skelet. Radiol. 2020, 49, 183–197. [Google Scholar] [CrossRef]
- Krogue, J.D.; Cheng, K.V.; Hwang, K.M.; Toogood, P.; Meinberg, E.G.; Geiger, E.J.; Zaid, M.; McGill, K.C.; Patel, R.; Sohn, J.H.; et al. Automatic hip fracture identification and functional subclassification with deep learning. Radiol. Artif. Intell. 2020, 2, e190023. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.T.; Ho, T.Y.; Lee, T.Y.; Chang, C.C.; Chou, C.C.; Chen, C.C.; Chung, I.F.; Liao, C.H. Application of a deep learning algorithm for detection and visualization of hip fractures on plain pelvic radiographs. Eur. Radiol. 2019, 29, 5469–5477. [Google Scholar] [CrossRef] [Green Version]
- Jones, R.M.; Sharma, A.; Hotchkiss, R.; Sperling, J.W.; Hamburger, J.; Ledig, C.; O’Toole, R.; Gardner, M.; Venkatesh, S.; Roberts, M.M.; et al. Assessment of a deep-learning system for fracture detection in musculoskeletal radiographs. NPJ Digit. Med. 2020, 3, 144. [Google Scholar] [CrossRef]
- Minamoto, Y.; Akagi, R.; Maki, S.; Shiko, Y.; Tozawa, R.; Kimura, S.; Yamaguchi, S.; Kawasaki, Y.; Ohtori, S.; Sasho, T. Automated detection of anterior cruciate ligament tears using a deep convolutional neural network. BMC Musculoskelet. Disord. 2022, 23, 577. [Google Scholar] [CrossRef]
- Awan, M.J.; Rahim, M.S.M.; Salim, N.; Mohammed, M.A.; Garcia-Zapirain, B.; Abdulkareem, K.H. Efficient Detection of Knee Anterior Cruciate Ligament from Magnetic Resonance Imaging Using Deep Learning Approach. Diagnostics 2021, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Bien, N.; Rajpurkar, P.; Ball, R.L.; Irvin, J.; Park, A.; Jones, E.; Bereket, M.; Patel, B.N.; Yeom, K.W.; Shpanskaya, K.; et al. Deep-learning-assisted diagnosis for knee magnetic resonance imaging: Development and retrospective validation of MRNet. PLoS Med. 2018, 15, e1002699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couteaux, V.; Si-Mohamed, S.; Nempont, O.; Lefevre, T.; Popoff, A.; Pizaine, G.; Villain, N.; Bloch, I.; Cotten, A.; Boussel, L. Automatic knee meniscus tear detection and orientation classification with Mask-RCNN. Diagn. Interv. Imaging 2019, 100, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Zhou, Z.; Samsonov, A.; Blankenbaker, D.; Larison, W.; Kanarek, A.; Lian, K.; Kambhampati, S.; Kijowski, R. Deep Learning Approach for Evaluating Knee MR Images: Achieving High Diagnostic Performance for Cartilage Lesion Detection. Radiology 2018, 289, 160–169. [Google Scholar] [CrossRef] [Green Version]
- Roblot, V.; Giret, Y.; Antoun, M.B.; Morillot, C.; Chassin, X.; Cotten, A.; Zerbib, J.; Fournier, L. Artificial intelligence to diagnose meniscus tears on MRI. Diagn. Interv. Imaging 2019, 100, 243–249. [Google Scholar] [CrossRef]
- Chang, P.D.; Wong, T.T.; Rasiej, M.J. Deep Learning for Detection of Complete Anterior Cruciate Ligament Tear. J. Digit. Imaging 2019, 32, 980–986. [Google Scholar] [CrossRef]
- Ferizi, U.; Besser, H.; Hysi, P.; Jacobs, J.; Rajapakse, C.S.; Chen, C.; Saha, P.; Honig, S.; Chang, G. Artificial Intelligence Applied to Osteoporosis: A Performance Comparison of Machine Learning Algorithms in Predicting Fragility Fractures From MRI Data. J. Magn. Reson. Imaging 2018, 49, 1029–1038. [Google Scholar] [CrossRef]
- Arpitha, A.; Rangarajan, L. Computational techniques to segment and classify lumbar compression fractures. Radiol. Med. 2020, 125, 551–560. [Google Scholar] [CrossRef]
- Kuo, R.Y.L.; Harrison, C.; Curran, T.-A.; Jones, B.; Freethy, A.; Cussons, D.; Stewart, M.; Collins, G.S.; Furniss, D. Artificial Intelligence in Fracture Detection: A Systematic Review and Meta-Analysis. Radiology 2022, 304, 50–62. [Google Scholar] [CrossRef]
- Liu, J.; Varghese, B.; Taravat, F.; Eibschutz, L.S.; Gholamrezanezhad, A. An Extra Set of Intelligent Eyes: Application of Artificial Intelligence in Imaging of Abdominopelvic Pathologies in Emergency Radiology. Diagnostics 2022, 12, 1351. [Google Scholar] [CrossRef]
- Volpicelli, G.; Lamorte, A.; Tullio, M.; Cardinale, L.; Giraudo, M.; Stefanone, V.; Boero, E.; Nazerian, P.; Pozzi, R.; Frascisco, M.F. Point-of-care multiorgan ultrasonography for the evaluation of undifferentiated hypotension in the emergency department. Intensiv. Care Med. 2013, 39, 1290–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjogren, A.R.; Leo, M.M.; Feldman, J.; Gwin, J.T. Image Segmentation and Machine Learning for Detection of Abdominal Free Fluid in Focused Assessment With Sonography for Trauma Examinations. J. Ultrasound Med. 2016, 35, 2501–2509. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.; Todd, W.M.; O’Brien, E.; Lin, H. Free fluid in Morison’s pouch on bedside ultrasound predicts need for operative intervention in suspected ectopic pregnancy. Acad. Emerg. Med. 2007, 14, 755–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, J.S.; Richards, J.R.; Battistella, F.; Bair, A.E.; McGahan, J.P.; Kuppermann, N. The fast is positive, now what? Derivation of a clinical decision rule to determine the need for therapeutic laparotomy in adults with blunt torso trauma and a positive trauma ultrasound. J. Emerg. Med. 2005, 29, 15–21. [Google Scholar] [CrossRef]
- Cheng, C.Y.; Chiu, I.M.; Hsu, M.Y.; Pan, H.Y.; Tsai, C.M.; Lin, C.H.R. Deep Learning Assisted Detection of Abdominal Free Fluid in Morison’s Pouch During Focused Assessment With Sonography in Trauma. Front. Med. 2021, 8, 707437. [Google Scholar] [CrossRef]
- Dreizin, D.; Chen, T.; Liang, Y.; Zhou, Y.; Paes, F.; Wang, Y.; Yuille, A.L.; Roth, P.; Champ, K.; Li, G.; et al. Added value of deep learning-based liver parenchymal CT volumetry for predicting major arterial injury after blunt hepatic trauma: A decision tree analysis. Abdom. Radiol. 2021, 46, 2556–2566. [Google Scholar] [CrossRef]
- Letoublon, C.; Morra, I.; Chen, Y.; Monnin, V.; Voirin, D.; Arvieux, C. Hepatic arterial embolization in the management of blunt hepatic trauma: Indications and complications. J. Trauma 2011, 70, 1032–1036. [Google Scholar] [CrossRef]
- Moschetta, M.; Telegrafo, M.; Rella, L.; Ianora, A.A.S.; Angelelli, G. Multi-detector CT features of acute intestinal ischemia and their prognostic correlations. World J. Radiol. 2014, 6, 130. [Google Scholar] [CrossRef]
- Lappas, J.C.; Reyes, B.L.; Maglinte, D.D.T. Abdominal radiography findings in small-bowel obstruction: Relevance to triage for additional diagnostic imaging. AJR Am. J. Roentgenol. 2001, 176, 167–174. [Google Scholar] [CrossRef]
- Thompson, W.M.; Kilani, R.K.; Smith, B.B.; Thomas, J.; Jaffe, T.A.; Delong, D.M.; Paulson, E.K. Accuracy of abdominal radiography in acute small-bowel obstruction: Does reviewer experience matter? AJR Am. J. Roentgenol. 2007, 188, W233–W238. [Google Scholar] [CrossRef]
- Kim, D.; Wit, H.; Thurston, M.; Long, M.; Maskell, G.; Strugnell, M.; Shetty, D.; Smith, I.; Hollings, N. An artificial intelligence deep learning model for identification of small bowel obstruction on plain abdominal radiographs. Br. J. Radiol. 2021, 94, 20201407. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R.; Mui, L.W.; Riyahi, S.; Prince, M.R.; Lee, H.K. Machine Learning Based Prediction Model for Closed-Loop Small Bowel Obstruction Using Computed Tomography and Clinical Findings. J. Comput. Assist. Tomogr. 2022, 46, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Song, G.; Lian, D.; Zhang, Q.; Dong, L. Process Management of Intussusception in Children: A Retrospective Analysis in China. Pediatr. Emerg. Care 2022, 38, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Hom, J.; Kaplan, C.; Fowler, S.; Messina, C.; Chandran, L.; Kunkov, S. Evidence-Based Diagnostic Test Accuracy of History, Physical Examination, and Imaging for Intussusception. Pediatr. Emerg. Care 2020, 38, e225–e230. [Google Scholar] [CrossRef] [PubMed]
- Weihmiller, S.N.; Buonomo, C.; Bachur, R. Risk stratification of children being evaluated for intussusception. Pediatrics 2011, 127, e296–e303. [Google Scholar] [CrossRef] [PubMed]
- Kwon, G.; Ryu, J.; Oh, J.; Lim, J.; Kang, B.-K.; Ahn, C.; Bae, J.; Lee, D.K. Deep learning algorithms for detecting and visualising intussusception on plain abdominal radiography in children: A retrospective multicenter study. Sci. Rep. 2020, 10, 17582. [Google Scholar] [CrossRef]
- Schoepf, U.J.; Costello, P. Spiral computed tomography is the first-line chest imaging test for acute pulmonary embolism: Yes. J. Thromb. Haemost. 2005, 3, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Schoepf, U.J. Diagnosing pulmonary embolism: Time to rewrite the textbooks. Int. J. Cardiovasc. Imaging 2005, 21, 155–163. [Google Scholar] [CrossRef]
- Becattini, C.; Vedovati, M.C.; Agnelli, G. Diagnosis and prognosis of acute pulmonary embolism: Focus on serum troponins. Expert Rev. Mol. Diagn. 2008, 8, 339–349. [Google Scholar] [CrossRef]
- Ben Cheikh, A.; Gorincour, G.; Nivet, H.; May, J.; Seux, M.; Calame, P.; Thomson, V.; Delabrousse, E.; Crombé, A. How artificial intelligence improves radiological interpretation in suspected pulmonary embolism. Eur. Radiol. 2022, 32, 5831. [Google Scholar] [CrossRef]
- Batra, K.; Xi, Y.; Al-Hreish, K.M.; Kay, F.U.; Browning, T.; Baker, C.; Peshock, R.M. Detection of Incidental Pulmonary Embolism on Conventional Contrast-Enhanced Chest CT: Comparison of an Artificial Intelligence Algorithm and Clinical Reports. AJR Am. J. Roentgenol 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Soffer, S.; Klang, E.; Shimon, O.; Barash, Y.; Cahan, N.; Greenspana, H.; Konen, E. Deep learning for pulmonary embolism detection on computed tomography pulmonary angiogram: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 15814. [Google Scholar] [CrossRef] [PubMed]
- Müller-Peltzer, K.; Kretzschmar, L.; de Figueiredo, G.N.; Crispin, A.; Stahl, R.; Bamberg, F.; Trumm, C.G. Present Limitations of Artificial Intelligence in the Emergency Setting—Performance Study of a Commercial, Computer-Aided Detection Algorithm for Pulmonary Embolism. RoFo Fortschr. Auf. Dem. Geb. Der Rontgenstrahlen Und. Der Bildgeb. Verfahr. 2021, 193, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Cellina, M.; Orsi, M.; Pittino, C.V.; Toluian, T.; Oliva, G. Chest computed tomography findings of COVID-19 pneumonia: Pictorial essay with literature review. Jpn. J. Radiol. 2020, 38, 1012–1019. [Google Scholar] [CrossRef]
- Soda, P.; D’Amico, N.C.; Tessadori, J.; Valbusa, G.; Guarrasi, V.; Bortolotto, C.; Akbar, M.U.; Sicilia, R.; Cordelli, E.; Fazzini, D.; et al. AIforCOVID: Predicting the clinical outcomes in patients with COVID-19 applying AI to chest-X-rays. An Italian multicentre study. Med. Image Anal. 2021, 74, 102216. [Google Scholar] [CrossRef]
- Bai, H.X.; Wang, R.; Xiong, Z.; Hsieh, B.; Chang, K.; Halsey, K.; Tran, T.M.L.; Choi, J.W.; Wang, D.-C.; Shi, L.-B.; et al. Artificial Intelligence Augmentation of Radiologist Performance in Distinguishing COVID-19 from Pneumonia of Other Origin at Chest CT. Radiology 2020, 296, E156–E165. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. CheXNet: Radiologist-Level Pneumonia Detection on Chest X-Rays with Deep Learning. arxiv 2017, arXiv:1711.05225. [Google Scholar]
- Institute of Medicine (US) Committee on Data Standards for Patient Safety. Key Capabilities of an Electronic Health Record System; Letter Report; National Academies Press (US): Washington, DC, USA, 2003. [Google Scholar] [CrossRef]
- Cai, T.; Giannopoulos, A.A.; Yu, S.; Kelil, T.; Ripley, B.; Kumamaru, K.K.; Rybicki, F.J.; Mitsouras, D. Natural Language Processing Technologies in Radiology Research and Clinical Applications. Radiographics 2016, 36, 176–191. [Google Scholar] [CrossRef] [Green Version]
- Fanni, S.C.; Gabelloni, M.; Alberich-Bayarri, A.; Neri, E. Structured Reporting and Artificial Intelligence. In Structured Reporting in Radiology; Springer: Berlin/Heidelberg, Germany, 2022; pp. 169–183. [Google Scholar] [CrossRef]
- Pons, E.; Braun, L.M.M.; Hunink, M.G.M.; Kors, J.A. Natural Language Processing in Radiology: A Systematic Review. Radiology 2016, 279, 329–343. [Google Scholar] [CrossRef]
- Chapman, W.W.; Bridewell, W.; Hanbury, P.; Cooper, G.F.; Buchanan, B.G. A simple algorithm for identifying negated findings and diseases in discharge summaries. J. Biomed. Inform. 2001, 34, 301–310. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.T.E.; Zheng, J.; Savova, G.K.; Erickson, B.J. Discerning tumor status from unstructured MRI reports-completeness of information in existing reports and utility of automated natural language processing. J. Digit. Imaging 2010, 23, 119–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, H.B.; Liu, C.; Ai, J.; Jaworsky, C.; Guerrier, C.E.; Flores, E.; Pianykh, O. Predicting No-Shows in Radiology Using Regression Modeling of Data Available in the Electronic Medical Record. J. Am. Coll. Radiol. 2017, 14, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, D.A.; Rosman, G.; Rus, D.; Meireles, O.R. Artificial Intelligence in Surgery: Promises and Perils. Ann. Surg. 2018, 268, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Toosi, A.; Bottino, A.G.; Saboury, B.; Siegel, E.; Rahmim, A. A Brief History of AI: How to Prevent Another Winter (A Critical Review). PET Clin. 2021, 16, 449–469. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Ranschaert, E.; Topff, L.; Pianykh, O. Optimization of Radiology Workflow with Artificial Intelligence. Radiol. Clin. N. Am. 2021, 59, 955–966. [Google Scholar] [CrossRef]
- Soliman, M.A.; Kelahan, L.C.; Magnetta, M.; Savas, H.; Agrawal, R.; Avery, R.J.; Aouad, P.; Liu, B.; Xue, Y.; Chae, Y.K.; et al. A Framework for Harmonization of Radiomics Data for Multicenter Studies and Clinical Trials. JCO Clin. Cancer Inform. 2022, 6, e2200023. [Google Scholar] [CrossRef]
- Cabini, R.F.; Brero, F.; Lancia, A.; Stelitano, C.; Oneta, O.; Ballante, E.; Puppo, E.; Mariani, M.; Alì, E.; Bartolomeo, V.; et al. Preliminary report on harmonization of features extraction process using the ComBat tool in the multi-center “Blue Sky Radiomics” study on stage III unresectable NSCLC. Insights Imaging 2022, 13, 38. [Google Scholar] [CrossRef]
- Tafuri, B.; Lombardi, A.; Nigro, S.; Urso, D.; Monaco, A.; Pantaleo, E.; Diacono, D.; De Blasi, R.; Bellotti, R.; Tangaro, S.; et al. The impact of harmonization on radiomic features in Parkinson’s disease and healthy controls: A multicenter study. Front Neurosci. 2022, 16, 1012287. [Google Scholar] [CrossRef]
- Ribeiro, M.T.; Singh, S.; Guestrin, C. “Why Should I Trust You?” Explaining the predictions of any classifier. In Proceedings of the ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 1135–1144. [Google Scholar]
- Rudin, C.; Radin, J. Why Are We Using Black Box Models in AI When We Don’t Need To? A Lesson From an Explainable AI Competition. Harv. Data Sci. Rev. 2019, 1, 2019. [Google Scholar] [CrossRef]
- Chen, C.; Li, O.; Tao, C.; Barnett, A.J.; Su, J.; Rudin, C. This Looks Like That: Deep Learning for Interpretable Image Recognition. Adv. Neural Inf. Process. Syst. 2019, 32, 1–5. [Google Scholar]
- Eche, T.; Schwartz, L.H.; Mokrane, F.-Z.; Dercle, L. Toward Generalizability in the Deployment of Artificial Intelligence in Radiology: Role of Computation Stress Testing to Overcome Underspecification. Radiol. Artif. Intell. 2021, 3, e210097. [Google Scholar] [CrossRef] [PubMed]
- Geman, S.; Bienenstock, E.; Doursat, R. Neural Networks and the Bias/Variance Dilemma. Neural Comput. 1992, 4, 1–58. [Google Scholar] [CrossRef]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coppola, F.; Faggioni, L.; Regge, D.; Giovagnoni, A.; Golfieri, R.; Bibbolino, C.; Miele, V.; Neri, E.; Grassi, R. Artificial intelligence: Radiologists’ expectations and opinions gleaned from a nationwide online survey. Radiol. Med. 2021, 126, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Langlotz, C.P. Will Artificial Intelligence Replace Radiologists? Radiol. Artif. Intell. 2019, 1, e190058. [Google Scholar] [CrossRef] [PubMed]
- Al-Dasuqi, K.; Johnson, M.H.; Cavallo, J.J. Use of artificial intelligence in emergency radiology: An overview of current applications, challenges, and opportunities. Clin. Imaging 2022, 89, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Jalal, S.; Parker, W.; Ferguson, D.; Nicolaou, S. Exploring the Role of Artificial Intelligence in an Emergency and Trauma Radiology Department. Can. Assoc. Radiol. J. 2020, 72, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Neri, E.; Coppola, F.; Miele, V.; Bibbolino, C.; Grassi, R. Artificial intelligence: Who is responsible for the diagnosis? Radiol. Med. 2020, 125, 517–521. [Google Scholar] [CrossRef]
- Cannarsa, M. Ethics Guidelines for Trustworthy AI. In The Cambridge Handbook of Lawyering in the Digital Age; Cambridge University Press: Cambridge, UK, 2021; pp. 283–297. Available online: https://www.academia.edu/38205904/ETHICS_GUIDELINES_FOR_TRUSTWORTHY_AI (accessed on 28 October 2022).


{kind=link}
| Type of ML | Mechanism | Type of Data Provided | Tasks for which the Mechanism can be used | Examples of Models |
|---|---|---|---|---|
| Supervised learning (SL) | The algorithm, provided with tuples (x,y) of input (labeled) and output (unlabeled), infers the relations that map the data. | Labeled data | Classification task; Regression task |
|
| Unsupervised learning (UL) | The algorithm exhibits self-organization, to capture hidden patterns in data. | Unlabeled data | Clustering Association; Anomalies detection |
|
| Semi-supervised learning (SSL) | The algorithm is placed between unsupervised learning (with no labeled training data) and supervised learning (with only labeled training data). | Mostly unlabeled data, with a small amount of labeled data. | Transductive task (infer the correct labels for the given unlabeled data) or inductive tasks (infer the correct mapping from x to y). |
|
| Reinforcement learning (RL) | The algorithm is created with a goal and a set of rules. The algorithm tends to maximize the "reward function" or reinforcement signals, to achieve the goal. | Not needing labeled input/output pairs to be presented; only a numerical performance score is given as guidance. | Good for modeling complex-task decision-making processes, such as economics and game theory under bounded rationality. |
|
| Section | Authors | Main Application | Technique | Findings |
|---|---|---|---|---|
| Neuroradiology | Matsoukas et al. [43] | Intracranial hemorrhages | CT | Sensitivity, specificity, and accuracy of 92.06%, 93.54%, and 93.46%. |
| Cerebral microbleeds | CT | Sensitivity, specificity, and accuracy of 91.6%, 93.9%, and 92.7%. | ||
| Rava et al. [44] | Intracranial hemorrhages | CT | Sensitivity of 93%, specificity of 93%, a positive predicting value of 85%, and a negative predicting value of 98%. | |
| McLouth et al. [46] | Large vessel occlusion | CT | Accuracy of 98.1%, sensitivity of 98.1%, specificity of 98.2%. | |
| MSK | Cheng et al. [54] | Femoral fractures detection | X-ray | AUC of 0.98, accuracy of 91%, sensitivity of 98%, specificity of 84%, and an F1 score of 0.916. |
| Jones et al. [55] | Fractures detection in 16 anatomical regions. | X-ray | AUC of 0.974, sensitivity of 95.2%, specificity of 81.3%, a positive predictive value (PPV) of 47.4%, and a negative predictive value (NPV) of 99.0%. | |
| Minamoto et al. [56] | Anterior Cruciate Ligament lesion | MRI | Ssensitivity of 91%, specificity of 86%, accuracy of 88.5%, a positive predictive value of 87.0%, and a negative predictive value of 91.0%. | |
| Bien et al. [58] | Anterior Cruciate Ligament lesion | MRI | AUC of 0.965, when compared to three musculoskeletal radiologists. | |
| Meniscal tears | MRI | AUC of 0.965, when compared to three musculoskeletal radiologists. | ||
| Liu et al. [60] | Meniscal tears | MRI | Sensitivity and sensibility of 84.1% and 85.2%, respectively, for evaluation 1, and of 80.5% and 87.9%, respectively, for evaluation 2. Areas under the ROC curve were 0.917 and 0.914 for evaluations 1 and 2, respectively. | |
| Roblot et al. [61] | Meniscal tears | MRI | AUC of 0.92 for the detection of the position of the two meniscal horns, of 0.94 for the presence of a meniscal tear, of 0.83 for determining the orientation of the tear, and a final weighted AUC of 0.90. | |
| Abdominal | Cheng et al. [71] | Ascites in the Morison pouch | Ultrasound | 0.961 for accuracy, 0.976 for sensitivity, 0.947 for specificity in the validation set, and 0.967, 0.985, and 0.913 in the test set, respectively. |
| Drezin et al. [72] | Measurement of the liver parenchymal disruption index | CT | Accuracy of 0.84 | |
| Kim et al. [77] | Small bowel occlusion | X-ray | AUC of 0.961, sensitivity of 91%, specificity of 93%. | |
| Goyal et al. [78] | Closed-loop small bowel occlusion | CT | AUC of 0.73, sensitivity of 0.72, specificity of 0.8, accuracy of 0.73. | |
| Chest | Cheik et al. [86] | Pulmonary embolism | CT | The AI had the best sensitivity and negative predictive values (92.6% vs. 90%, and 98.6% vs. 98.1%, respectively), whereas radiologists had the highest specificity and positive predictive values (99.1% vs. 95.8%, and 95% vs. 80.4%, respectively). |
| Batra et al. [87] | Incidental pulmonary embolism | CT | AI had a lower positive predictive value (86.8% versus 97.3%, p = 0.03) and specificity (99.8% vs. 100.0%, p = 0.045) vs. radiologists. | |
| Soffer et al. [88] | Pulmonary embolism | CT | Sensitivity and specificity were 0.88 and 0.86, respectively. | |
| Xiong et al. [92] | COVID-19 pneumonia | CT | Accuracy of 96%, sensitivity of 95%, and specificity of 96%. | |
| Rajpurkar et al. [93] | Pneumonia | X-ray | F1 score of 0.435. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cellina, M.; Cè, M.; Irmici, G.; Ascenti, V.; Caloro, E.; Bianchi, L.; Pellegrino, G.; D’Amico, N.; Papa, S.; Carrafiello, G. Artificial Intelligence in Emergency Radiology: Where Are We Going? Diagnostics 2022, 12, 3223. https://doi.org/10.3390/diagnostics12123223
Cellina M, Cè M, Irmici G, Ascenti V, Caloro E, Bianchi L, Pellegrino G, D’Amico N, Papa S, Carrafiello G. Artificial Intelligence in Emergency Radiology: Where Are We Going? Diagnostics. 2022; 12(12):3223. https://doi.org/10.3390/diagnostics12123223
Chicago/Turabian StyleCellina, Michaela, Maurizio Cè, Giovanni Irmici, Velio Ascenti, Elena Caloro, Lorenzo Bianchi, Giuseppe Pellegrino, Natascha D’Amico, Sergio Papa, and Gianpaolo Carrafiello. 2022. "Artificial Intelligence in Emergency Radiology: Where Are We Going?" Diagnostics 12, no. 12: 3223. https://doi.org/10.3390/diagnostics12123223