
Microvascular Changes after Scleral Buckling for Rhegmatogenous Retinal Detachment: An Optical Coherence Tomography Angiography Study
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
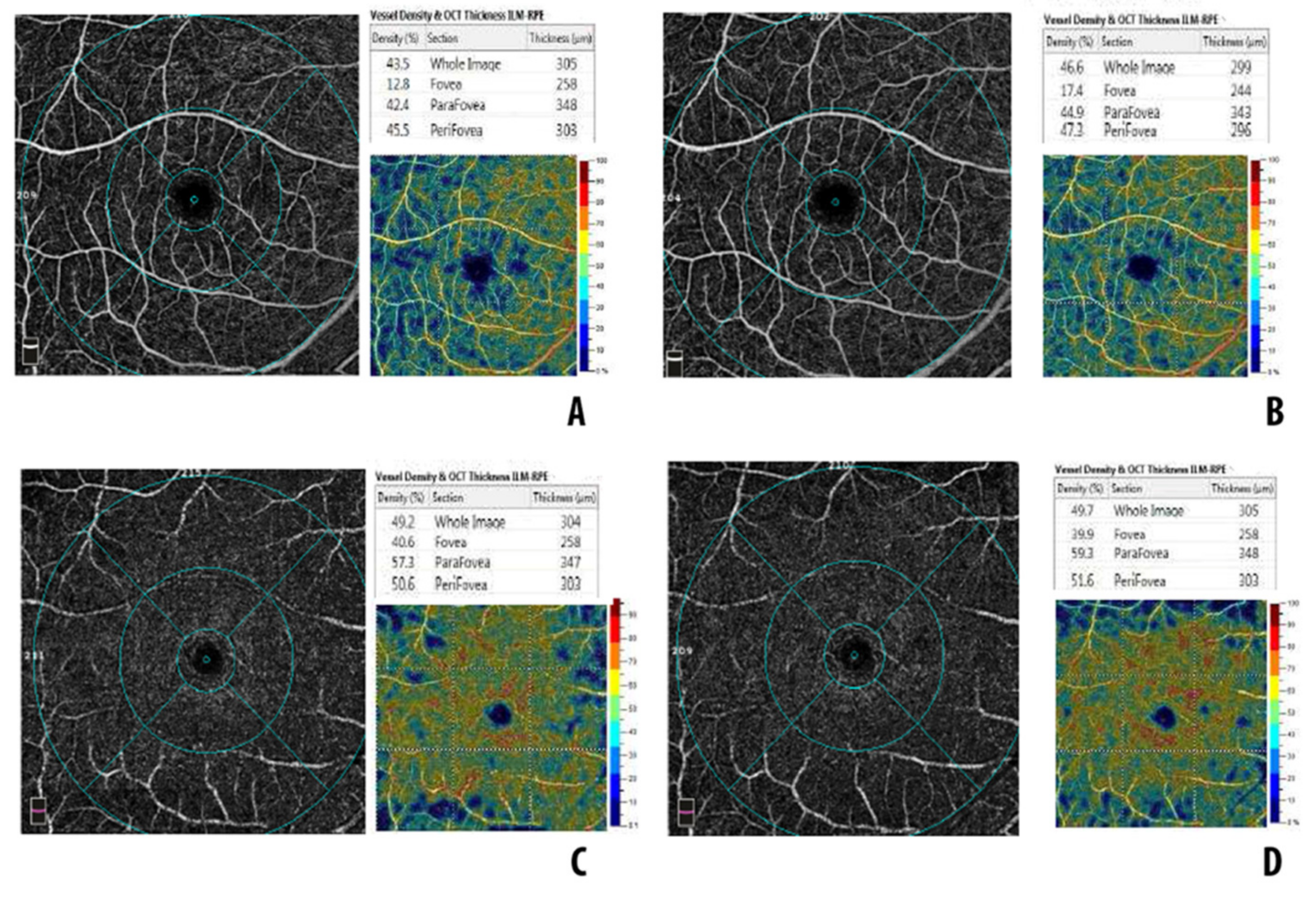
3.1. Macula-On RRD Group
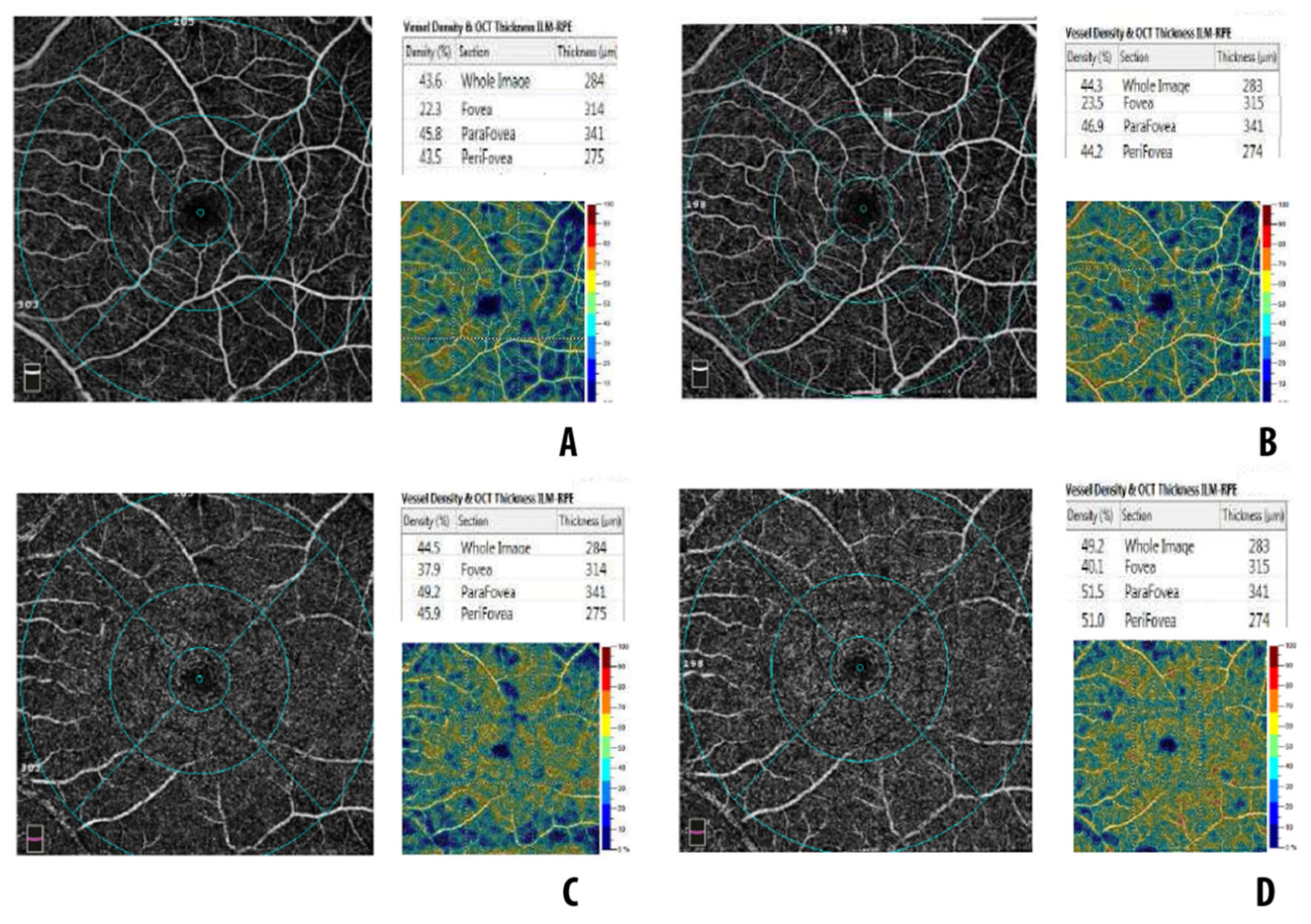
3.2. Macula-Off RRD Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heimann, H.; Bartz-Schmidt, K.U.; Bornfeld, N.; Weiss, C.; Hilgers, R.D.; Foerster, M.H. Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment. A Prospective Randomized Multicenter Clinical Study. Ophthalmology 2007, 114, 2142–2154. [Google Scholar] [CrossRef] [PubMed]
- Adelman, R.A.; Parnes, A.J.; Ducournau, D. Strategy for the management of uncomplicated retinal detachments: The european vitreo-retinal society retinal detachment study report 1. Ophthalmology 2013, 120, 1804–1808. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Snead, M.P. Scleral buckling—A brief historical overview and current indications. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 467–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallico, M.; Alosi, P.; Reibaldi, M.; Longo, A.; Bonfiglio, V.; Avitabile, T.; Russo, A. Scleral Buckling: A Review of Clinical Aspects and Current Concepts. J. Clin. Med. 2022, 11, 314. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Han, J.W.; Kim, S.S.; Byeon, S.H.; Koh, H.J.; Lee, S.C.; Kim, M. Long-term Effect of Scleral Encircling on Axial Elongation. Am. J. Ophthalmol. 2018, 189, 139–145. [Google Scholar] [CrossRef]
- Eshita, T.; Shinoda, K.; Kimura, I.; Kitamura, S.; Ishida, S.; Inoue, M.; Mashima, Y.; Katsura, H.; Oguchi, Y. Retinal blood flow in the macular area before and after scleral buckling procedures for rhegmatogenous retinal detachment without macular involvement. Jpn. J. Ophthalmol. 2004, 48, 358–363. [Google Scholar] [CrossRef]
- D’Aloisio, R.; Viggiano, P.; Borrelli, E.; Parravano, M.; Agbèanda, A.-G.; Evangelista, F.; Ferro, G.; Toto, L.; Mastropasqua, R. Changes in Iris Perfusion Following Scleral Buckle Surgery for Rhegmatogenous Retinal Detachment: An Anterior Segment Optical Coherence Tomography Angiography (AS-OCTA) Study. J. Clin. Med. 2020, 9, 1231. [Google Scholar] [CrossRef]
- Cennamo, G.; Reibaldi, M.; Montorio, D.; D’Andrea, L.; Fallico, M.; Triassi, M. Optical coherence tomography angiography features in post COVID-19 pneumonia patients: A pilot study. Am. J. Ophthalmol. 2021, 227, 182–190. [Google Scholar] [CrossRef]
- Christou, E.E.; Stavrakas, P.; Batsos, G.; Christodoulou, E.; Stefaniotou, M. Association of OCT-A characteristics with postoperative visual acuity after rhegmatogenous retinal detachment surgery: A review of the literature. Int. Ophthalmol. 2021, 41, 2283–2292. [Google Scholar] [CrossRef]
- Barca, F.; Bacherini, D.; Dragotto, F.; Tartaro, R.; Lenzetti, C.; Finocchio, L.; Virgili, G.; Caporossi, T.; Giansanti, F.; Savastano, A.; et al. OCT Angiography Findings in Macula-ON and Macula-OFF Rhegmatogenous Retinal Detachment: A Prospective Study. J. Clin. Med. 2020, 9, 3982. [Google Scholar] [CrossRef]
- Tsen, C.L.; Sheu, S.J.; Chen, S.C.; Wu, T.T. Imaging analysis with optical coherence tomography angiography after primary repair of macula-off rhegmatogenous retinal detachment. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1847–1855. [Google Scholar] [CrossRef]
- Woo, J.M.; Yoon, Y.S.; Woo, J.E.; Min, J.K. Foveal Avascular Zone Area Changes Analyzed Using OCT Angiography after Successful Rhegmatogenous Retinal Detachment Repair. Curr. Eye Res. 2018, 43, 674–678. [Google Scholar] [CrossRef]
- Nam, S.H.; Kim, K.; Kim, E.S.; Kim, D.G.; Yu, S.Y. Longitudinal Microvascular Changes on Optical Coherence Tomographic Angiography after Macula-Off Rhegmatogenous Retinal Detachment Repair Surgery. Ophthalmologica 2021, 244, 34–41. [Google Scholar] [CrossRef]
- Bonfiglio, V.; Ortisi, E.; Scollo, D.; Reibaldi, M.; Russo, A.; Pizzo, A.; Faro, G.; Macchi, I.; Fallico, M.; Toro, M.D.; et al. Vascular changes after vitrectomy for rhegmatogenous retinal detachment: Optical coherence tomography angiography study. Acta Ophthalmol. 2020, 98, e563–e569. [Google Scholar] [CrossRef]
- Hong, E.H.; Cho, H.; Kim, D.R.; Kang, M.H.; Shin, Y.U.; Seong, M. Changes in retinal vessel and retinal layer thickness after vitrectomy in retinal detachment via swept-source OCT angiography. Investig. Ophthalmol. Vis. Sci. 2020, 61, 35. [Google Scholar] [CrossRef] [Green Version]
- Matthew Mckay, K.; Vingopoulos, F.; Wang, J.C.; Papakostas, T.D.; Silverman, R.F.; Marmalidou, A.; Lains, I.; Eliott, D.; Vavvas, D.G.; Kim, L.A.; et al. Retinal microvasculature changes after repair of macula-off retinal detachment assessed with optical coherence tomography angiography. Clin. Ophthalmol. 2020, 14, 1759–1767. [Google Scholar] [CrossRef]
- Wang, H.; Xu, X.; Sun, X.; Ma, T.; Sun, T. Macular perfusion changes assessed with optical coherence tomography angiography after vitrectomy for rhegmatogenous retinal detachment. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 733–740. [Google Scholar] [CrossRef] [Green Version]
- Sato, E.; Shinoda, K.; Kimura, I.; Ohtake, Y.; Inoue, M. Microcirculation in eyes after rhegmatogenous retinal detachment surgery. Curr. Eye Res. 2007, 32, 773–779. [Google Scholar] [CrossRef]
- Cardillo Piccolino, F. Vascular changes in rhegmatogenous retinal detachment. Ophthalmologica 1983, 186, 17–24. [Google Scholar] [CrossRef]
- Quintyn, J.; Brasseur, G. Subretinal fluid in primary rhegmatogenous retinal detachment: Physiopathology and composition. Surv. Ophthalmol. 2004, 49, 96–108. [Google Scholar] [CrossRef]
- Delolme, M.P.; Dugas, B.; Nicot, F.; Muselier, A.; Bron, A.M.; Creuzot-Garcher, C. Anatomical and functional macular changes after rhegmatogenous retinal detachment with macula off. Am. J. Ophthalmol. 2012, 153, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Bonfiglio, V.; Fallico, M.R.; Russo, A.; De Grande, V.; Longo, A.; Uva, M.G.; Reibaldi, M.; Avitabile, T. Intravitreal dexamethasone implant for cystoid macular edema and inflammation after scleral buckling. Eur. J. Ophthalmol. 2015, 25, e98–e100. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Aggarwal, K.; Akella, M.; Agrawal, R.; Khandelwal, N.; Bansal, R.; Singh, R.; Gupta, V. Fractal dimension and optical coherence tomography angiography features of the central macula after repair of rhegmatogenous retinal detachments. Retina 2019, 39, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, G.; Chihara, E. Implication of Deep-Vascular-Layer Alteration Detected by Optical Coherence Tomography Angiography for the Pathogenesis of Diabetic Retinopathy. Ophthalmologica 2019, 241, 179–182. [Google Scholar] [CrossRef]
- Fernández-Espinosa, G.; Boned-Murillo, A.; Orduna-Hospital, E.; Díaz-Barreda, M.D.; Sánchez-Cano, A.; Bielsa-Alonso, S.; Acha, J.; Pinilla, I. Retinal Vascularization Abnormalities Studied by Optical Coherence Tomography Angiography (OCTA) in Type 2 Diabetic Patients with Moderate Diabetic Retinopathy. Diagnostics 2022, 12, 379. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Macula-On Group | Macula-Off Group | p | |
|---|---|---|---|
| Eyes (n.) | 19 | 18 | |
| Gender (male/female) | 9/10 | 10/8 | 0.862 |
| Age, years | 54 ± 6 (45–63) | 56 ± 7 (43–65) | 0.356 |
| BCVA, logMAR | 0.10 ± 0.03 (0.04–0.16) | 0.94 ± 0.07 (0.88–1.20) | <0.001 |
| Axial length, mm | 25.2 ± 0.5 (24.23–25.92) | 24.8 ± 1.1 (23.76–25.81) | 0.101 |
| Macula-On RRD Eyes, n 19 | Fellow Eyes, n 19 | t Test | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 1 Month | 3 Months | 6 Months | p (ANOVA) | Baseline | 1 Month | 3 Months | 6 Months | Baseline | 1 Month | 3 Months | 6 Months | |
| BCVA (logMar) | 0.10 ± 0.03 (0.04–0.16) | 0.09 ± 0.04 (0.02–0.14) | 0.09 ± 0.05 (0.02–0.14) | 0.09 ± 0.03 (0.04–0.16) | 0.687 | 0.07 ± 0.03 (0.02–0.10) | 0.07 ± 0.04 (0.00–0.14) | 0.08 ± 0.03 (0.02–0.14) | 0.08 ± 0.04 (0.02–0.16) | 0.003 | 0.081 | 0.187 | 0.062 |
| axial length (mm) | 25.2 ± 0.5 (24.23–25.92) | - | - | 26.1 ± 0.8 (24.77–27.32) | <0.001 (t-test) | 26.0 ± 1.5 (24.23–27.83) | - | - | 26.0 ± 1.3 (24.25–27.83) | 0.014 | - | - | 0.475 |
| FAZ | 0.227 ± 0.019 (0.181–0.261) | 0.230 ±0.007 (0.217–0.242) | 0.221 ± 0.015 0.181–0.241) | 0.229 ± 0.016 (0.193–0.261) | 0.310 | 0.226 ± 0.014 (0.194–0.254) | 0.226 ± 0.011 (0.205–0.244) | 0.221 ± 0.013 (0.189–0.233) | 0.224 ± 0.014 (0.181–0.244) | 0.863 | 0.084 | 0.983 | 0.164 |
| CMT (µm) | 244 ± 13 (229–270) | 250 ± 10 (236–272) | 252 ± 9 (231–271) | 249 ± 11 (229–273) | 0.197 | 246 ± 12 (229–266) | 249 ± 13 (231–273) | 248 ± 12 (238–274) | 247 ± 12 (231–273) | 0.612 | 0.203 | 0.091 | 0.183 |
| Vessel density | |||||||||||||
| SCP whole | 40.9 ± 1.8 c (37.8–43.3) | 42.1 ± 2.2 (38.6–45.3) | 42.6 ± 1.6 c (38.6–45.3) | 43.1 ± 2.2 d (39.4–46.7) | 0.004 | 44.3 ± 1.6 (40.2–46.1) | 44.4 ± 1.8 (40.3–48.1) | 44.2 ± 1.5 (40.7–46.3) | 44.2 ± 1.9 (39.9–46.4) | <0.001 | <0.001 | <0.001 | 0.003 |
| SCP fovea | 21.4 ± 2.8 (12.8–27.8) | 20.1 ± 2.9 (9–22.6) | 19.8 ± 1.4 (17.2–22.2) | 21.3 ± 1.7 (17.4–23.8) | 0.073 | 21.5 ± 1.7 (17.2–23.8) | 21.3 ± 1.2 (19.3–23.7) | 21.4 ± 1.3 (18.9–23.2) | 21.6 ± 1.6 (17.6–23.7) | 0.826 | 0.027 | 0.012 | 0.121 |
| SCP parafovea | 41.0 ± 2.6 (37.5–46.5) | 43.1 ± 1.9 (39.7–46.5) | 43.5 ± 1.7 e (39.2–46.3) | 43.6 ± 2.8 f (36.8–49.4) | 0.005 | 45.6 ± 1.5 (43.1–49.1) | 45.8 ± 1.7 (43.7–50.8) | 45.5 ± 1.4 (43.5–48.5) | 45.2 ± 1.4 (42.1–48.7) | <0.001 | <0.001 | <0.001 | 0.006 |
| SCP perifovea | 40.7 ± 2.4 (35.9–45.5) | 39.9 ± 1.4 (37.2–43.6) | 40.6 ± 1.4 (37.6–42.8) | 42.7 ± 2.8 g (37.9–48.8) | 0.001 | 44.4 ± 1.8 (41.7–47.2) | 44.2 ± 2.1 (40.1–48.1) | 44.3 ± 1.7 (41.2–47.1) | 44.1 ± 1.6 (41.1–46.9) | <0.001 | <0.001 | <0.001 | 0.021 |
| DCP whole | 48.8 ± 1.8 (42.9–51.1) | 49.7 ± 1.3 (46.9–51.9) | 49.4 ± 1.7 (46.1–52.9) | 49.4 ± 2.1 (43.9–53.3) | 0.481 | 50.1 ± 2.1 (44.8–53.4) | 50.1 ± 1.9 (47.5–54.2) | 49.7 ± 2.1 (44.9–52.6) | 49.9 ± 1.9 (45.1–52.2) | 0.065 | 0.105 | 0.184 | 0.109 |
| DCP fovea | 40.7 ± 1.4 (38.2–44.2) | 40.2 ± 1.7 (37.5–44.3) | 40.9 ± 2.0 (38.4–44.3) | 41.1 ± 1.2 (38.1–43.3) | 0.320 | 41.6 ± 1.5 (38.0–44.1) | 41.5 ± 1.2 (39.1–43.7) | 41.5 ± 1.3 (38.5–43.7) | 41.6 ± 1.8 (37.8–46.5) | 0.078 | 0.055 | 0.091 | 0.207 |
| DCP parafovea | 52.1 ± 2.3 (47.3–57.3) | 51.1 ± 1.6 (47.3–53.6) | 50.8 ± 2.2 (46.0–55.8) | 51.4 ± 2.7 (46.4–59.3) | 0.320 | 52.6 ± 2.1 (47.9–57.7) | 52.4 ± 1.9 (48.2–56.7) | 52.1 ± 23.3 (48.1–55.9) | 52.3 ± 2.1 (43.3–54.4) | 0.530 | 0.093 | 0.059 | 0.087 |
| DCP perifovea | 48.2 ± 2.9 (42.2–53.4) | 49.2 ± 1.8 (46.6–53.4) | 47.8 ± 2.8 (41.9–53.4) | 48.4 ± 3.1 (42.0–53.4) | 0.432 | 49.4 ± 2.9 (43.3–54.7) | 49.6 ± 2.6 (45.3–54.9) | 49.1 ± 2.7 (42.9–53.2) | 49.4 ± 2.7 (43.5–53.7) | 0.200 | 0.481 | 0.183 | 0.367 |
| Macula-Off RRD Eyes, n 19 | Fellow Eyes, n 19 | t Test | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 1 Month | 3 Months | 6 Months | p (ANOVA) | Baseline | 1 Month | 3 Months | 6 Months | Baseline | 1 Month | 3 Months | 6 Months | |
| BCVA (logMar) | 1.04 ± 0.09 (0.88–1.20) | 0.30 ± 0.10 (0.12–0.46) | 0.26 ± 0.08 (0.12–0.38) | 0.25 ± 0.08 (0.12–0.38) | <0.001 | 0.09 ± 0.04 (0.2–0.12) | 0.09 ± 0.05 (0.2–0.20) | 0.08 ± 0.04 (0.2–0.18) | 0.08 ± 0.04 (0.4–0.20) | <0.001 | <0.001 | <0.001 | <0.001 |
| axial length (mm) | 24.9 ± 0.5 (24.31–25.8) | 26.2 ± 0.7 (24.77–27.32) | 0.001 (t-test) | 25.6 ± 0.8 (24.23–27.83) | 25.6 ± 0.8 (24.25–27.81) | 0.019 | 0.037 | ||||||
| FAZ (mm2) | NA | 0.231 ± 0.031 (0.166–0.288) | 0.218 ± 0.017 (0.171–0.242) | 0.226 ± 0.013 (0.173–0.263) | 0.224 | 0.231 ± 0.010 (0.216–0.254) | 0.230 ± 0.016 (0.193–0.267) | 0.228 ± 0.012 (0.195–0.249) | 0.232 ± 0.015 (0.219–0.281) | - | 0.744 | 0.061 | 0.186 |
| CMT (µm) | NA | 273 ± 14 (259–314) | 276 ± 13 (249–296) | 275 ± 15 (249–315) | 0.316 | 269 ± 11 (249–294) | 267 ± 8 (252–285) | 271 ± 9 (259–289) | 268 ± 11 (248–288) | - | 0.289 | 0.227 | 0.194 |
| Vessel density | |||||||||||||
| SCP whole | NA | 40.5 ± 1.4 (38.6–43.6) | 40.6 ± 1.3 (38.6–42.6) | 41.3 ± 1.7 (36.9–44.3) | 0.054 | 44.6 ± 1.1 (42.6–47.3) | 44.7 ± 1.3 (42.5–46.8) | 44.7 ± 1.5 (42.6–48.3) | 44.7 ± 1.5 (42.4–48.3) | - | <0.001 | <0.001 | <0.001 |
| SCP fovea | NA | 20.1 ± 1.4 (17.2–22.3) | 20.5 ± 1.0 (18.3–22.3) | 20.9 ± 1.6 (17.2–23.7) | 0.108 | 20.5 ± 1.6 (17.2–23.8) | 20.6 ± 1.6 (17.5–24.1) | 20.4 ± 1.5 (17.2–23.8) | 20.7 ± 1.5 (18.1–24.2) | - | 0.532 | 0.871 | 0.718 |
| SCP parafovea | NA | 41.5 ± 1.6 (39.2–45.8) | 41.6 ± 1.3 (39.2–44.8) | 41.6 ± 1.9 (38.1–46.9) | 0.689 | 45.1 ± 1.5 (42.7–47.6) | 45.3 ± 1.5 (42.9–47.9) | 45.2 ± 1.4 (42.5–47.8) | 45.2 ± 1.6 (42.3–48.1) | - | <0.001 | <0.001 | <0.001 |
| SCP perifovea | NA | 40.3 ± 1.7 (37.2–43.6) | 40.6 ± 1.4 (37.6–42.8) | 41.0 ± 1.5 (37.6–46.9) | 0.108 | 43.5 ± 1.3 (41.4–46.2) | 43.6 ± 1.4 (41.7–46.5) | 43.4 ± 1.3 (41.1–47.3) | 43.6 ± 1.5 (40.9–46.4) | - | <0.001 | <0.001 | <0.001 |
| DCP whole | NA | 41.0 ± 1.6 (38.6–44.5) | 43.6 ± 1.2 (40.8–45.3) | 43.9 ± 1.7 (41.8–49.2) | <0.001 | 46.5 ± 1.2 (44.2–48.2) | 46.6 ± 1.1 (45.1–48.6) | 46.4 ± 1.2 (44.6–48.7) | 46.5 ± 1.2 (43.9–48.4) | - | <0.001 | <0.001 | <0.001 |
| DCP fovea | NA | 35.4 ± 2.4 (32.6–44.5) | 36.3 ± 1.9 (33.2–41.3) | 36.2 ± 1.8 (33.8–40.1) | 0.068 | 37.7 ± 1.0 (36.1–39.4) | 37.8 ± 1.0 (36.5–39.7) | 37.5 ± 1.1 (36.4–39.1) | 37.6 ± 1.0 (35.3–39.2) | - | <0.001 | 0.016 | 0.009 |
| DCP parafovea | NA | 45.0 ± 1.4 (42.9–49.2) | 46.1 ± 1.7 (41.8–48.3) | 48.6 ± 2.6 (42.1–52.9) | <0.001 | 51.8 ± 2.1 (47.9–57.7) | 51.9 ± 2.0 (49.2–57.9) | 51.6 ± 2.1 (48.5–58.2) | 51.5 ± 2.4 (45.8–56.9) | - | <0.001 | <0.001 | <0.001 |
| DCP perifovea | NA | 40.4 ± 2.1 (36.5–45.9) | 40.9 ± 1.5 (37.6–43.1) | 40.5 ± 2.9 (37.6–51.1) | 0.317 | 47.2 ± 1.6 (44.5–51.6) | 47.2 ± 1.7 (44.3–51.7) | 47.4 ± 1.8 (44.4–52.9) | 47.3 ± 1.5 (44.8–51.4) | - | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fallico, M.; Longo, A.; Avitabile, T.; Alosi, P.; Grillo, M.; Castellino, N.; Bonfiglio, V.; Reibaldi, M.; Pignatelli, F.; Russo, A. Microvascular Changes after Scleral Buckling for Rhegmatogenous Retinal Detachment: An Optical Coherence Tomography Angiography Study. Diagnostics 2022, 12, 3015. https://doi.org/10.3390/diagnostics12123015
Fallico M, Longo A, Avitabile T, Alosi P, Grillo M, Castellino N, Bonfiglio V, Reibaldi M, Pignatelli F, Russo A. Microvascular Changes after Scleral Buckling for Rhegmatogenous Retinal Detachment: An Optical Coherence Tomography Angiography Study. Diagnostics. 2022; 12(12):3015. https://doi.org/10.3390/diagnostics12123015
Chicago/Turabian StyleFallico, Matteo, Antonio Longo, Teresio Avitabile, Pietro Alosi, Marco Grillo, Niccolò Castellino, Vincenza Bonfiglio, Michele Reibaldi, Francesco Pignatelli, and Andrea Russo. 2022. "Microvascular Changes after Scleral Buckling for Rhegmatogenous Retinal Detachment: An Optical Coherence Tomography Angiography Study" Diagnostics 12, no. 12: 3015. https://doi.org/10.3390/diagnostics12123015