
[18F]-Fludeoxyglucose Positron Emission Tomography/Computed Tomography with Radiomics Analysis in Patients Undergoing Aortic In-Situ Reconstruction with Cryopreserved Allografts
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cryopreserved Allograft
2.2. Imaging: [18F]FDG PET/CT and Radiomics Analysis
2.3. Statistical Analysis
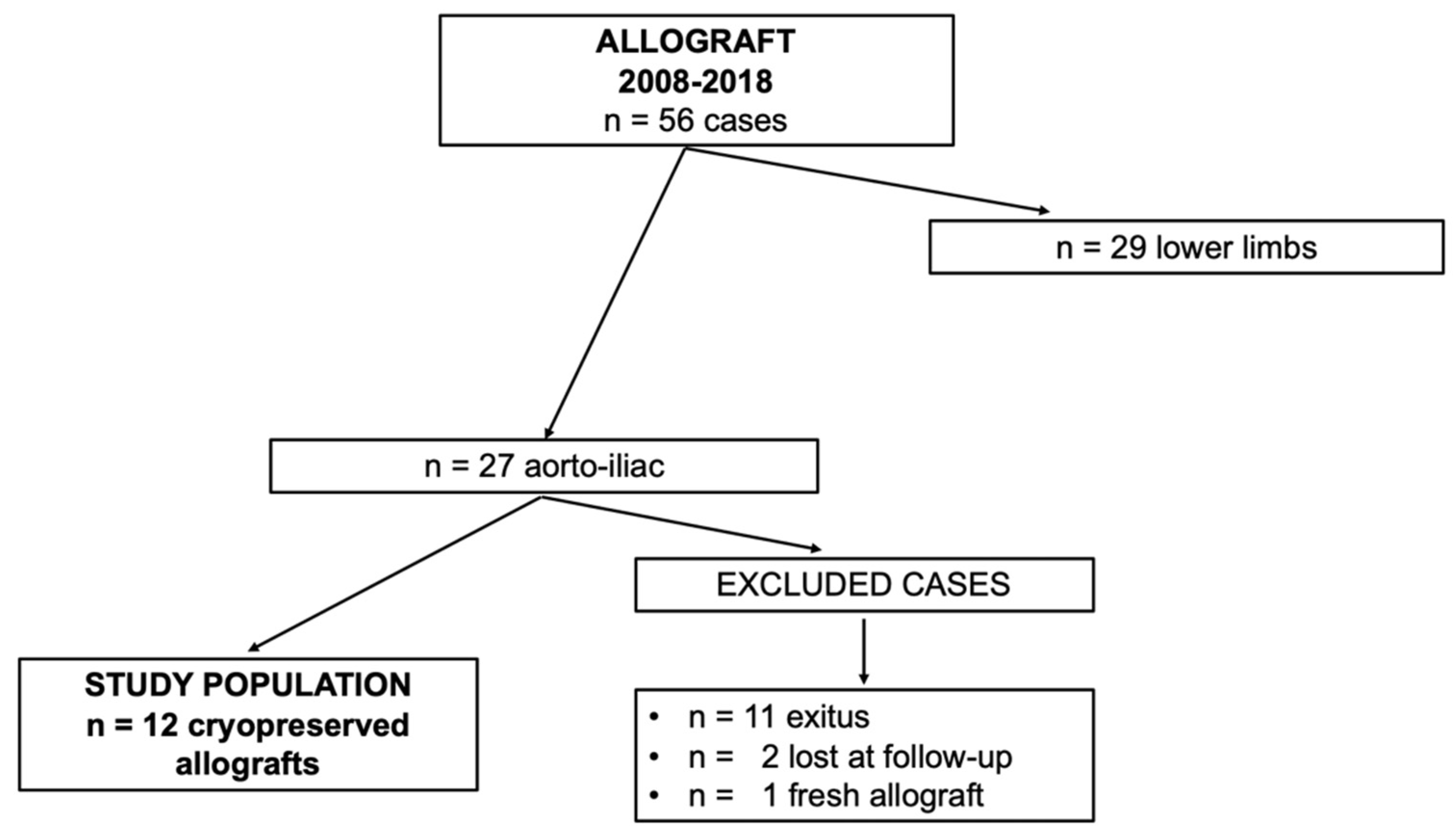
3. Results
[18F]FDG PET/CT and Radiomics Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bunt, T.J. Vascular graft infections: An update. Cardiovasc. Surg. 2001, 9, 225–233. [Google Scholar] [CrossRef]
- Saleem, B.R.; Meerwaldt, R.; Tielliu, I.F.; Verhoeven, E.L.; van den Dungen, J.J.; Zeebregts, C.J. Conservative treatment of vascular prosthetic graft infection is associated with high mortality. Am. J. Surg. 2010, 200, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, P.F. Conservative treatment of aortic graft infection. Semin. Vasc. Surg. 2011, 24, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Kahlberg, A.; Melissano, G.; Tshomba, Y.; Leopardi, M.; Chiesa, R. Strategies to treat thoracic aortitis and infected aortic grafts. J. Cardiovasc. Surg. 2015, 56, 269–280. [Google Scholar]
- Post, I.C.J.H.; Vos, C.G. Systematic review and meta-analysis on the management of open abdominal aortic graft infections. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 258–281. [Google Scholar] [CrossRef]
- Argyriou, C.; Georgiadis, G.S.; Lazarides, M.K.; Georgakarakos, E.; Antoniou, G.A. Endograft infection after endovascular abdominal aortic aneurysm repair: A systematic review and meta-analysis. J. Endovasc. Ther. 2017, 24, 688–697. [Google Scholar] [CrossRef]
- O’Connor, S.; Andrew, P.; Batt, M.; Becquemin, J.P. A systematic review and meta-analysis of treatments for aortic graft infection. J. Vasc. Surg. 2006, 44, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Cardozo, M.A.; Frankini, A.D.; Bonamigo, T.P. Use of the superficial femoral vein in the treatment of infected aortoiliofemoral prosthetic grafts. Cardiovasc. Surg. 2002, 10, 304–310. [Google Scholar] [CrossRef]
- Batt, M.; Jean-Baptiste, E.; O’Connor, S.; Bouillanne, P.J.; Haudebourg, P.; Hassen-Khodja, R.; Declemy, S.; Farhad, R. In-situ revascularization for patients with aortic graft infection: A single centre experience with silver coated polyester grafts. Eur. J. Vasc. Endovasc. Surg. 2008, 36, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Kieffer, E.; Gomes, D.; Chiche, L.; Fleron, M.H.; Koskas, F.; Bahnini, A. Allograft replacement for infrarenal aortic graft infection: Early and late results in 179 patients. J. Vasc. Surg. 2004, 39, 1009–1017. [Google Scholar] [CrossRef] [Green Version]
- Antonopoulos, C.N.; Papakonstantinou, N.A.; Hardy, D.; Lyden, S.P. Cryopreserved allografts for arterial reconstruction after aorto-iliac infection: A systematic review and meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Sah, B.R.; Husmann, L.; Mayer, D.; Scherrer, A.; Rancic, Z.; Puippe, G.; Weber, R.; Hasse, B.; VASGRA Cohort. Diagnostic performance of 18F-FDG-PET/CT in vascular graft infections. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 455–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogt, P.R.; Brunner-LaRocca, H.P.; Lachat, M.; Ruef, C.; Turina, M.I. Technical details with the use of cryopreserved arterial allografts for aortic infection: Influence on early and midterm mortality. J. Vasc. Surg. 2002, 35, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Erba, P.A.; Lancellotti, P.; Vilacosta, I.; Gaemperli, O.; Rouzet, F.; Hacker, M.; Signore, A.; Slart, R.H.J.A.; Habib, G. Recommendations on nuclear and multimodality imaging in IE and CIED infections. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1795–1815. [Google Scholar] [CrossRef]
- Jamar, F.; Buscombe, J.; Chiti, A.; Christian, P.E.; Delbeke, D.; Donohoe, K.J.; Israel, O.; Martin-Comin, J.; Signore, A. EANM/SNMMI guideline for 18F-FDG use in inflammation and infection. J. Nucl. Med. 2013, 54, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Slart, R.H.J.A.; Glaudemans, A.W.J.M.; Gheysens, O.; Lubberink, M.; Kero, T.; Dweck, M.R.; Habib, G.; Gaemperli, O.; Saraste, A.; Gimelli, A.; et al. 4Is Cardiovascular Imaging: A joint initiative of the European Association of Cardiovascular Imaging (EACVI); European Association of Nuclear Medicine (EANM). Procedural recommendations of cardiac PET/CT imaging: Standardization in inflammatory-, infective-, infiltrative-, and innervation (4Is)-related cardiovascular diseases: A joint collaboration of the EACVI and the EANM. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1016–1039. [Google Scholar]
- European Society of Radiology (ESR). White paper on imaging biomarkers. Insights Imaging 2010, 1, 42–45. [Google Scholar] [CrossRef] [Green Version]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuzé, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A freeware for radiomic feature calculation in multimodality imaging to accelerate advances in the characterization of tumor heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [Green Version]
- Harlander-Locke, M.P.; Harmon, L.K.; Lawrence, P.F.; Oderich, G.S.; McCready, R.A.; Morasch, M.D.; Feezor, R.J.; Vascular Low-Frequency Disease Consortium; Zhou, W.; Bismuth, J.; et al. The use of cryopreserved aortoiliac allograft for aortic reconstruction in the United States. J.Vasc. Surg. 2014, 59, 669–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couture, T.; Gaudric, J.; Du Montcel, S.T.; Jayet, J.; Verscheure, D.; Davaine, J.M.; Jarraya, M.; Chiche, L.; Koskas, F. Short and Mid Term Outcomes of Cryopreserved Abdominal Aortic Allografts Used as a Substitute for Infected Prosthetic Grafts in 200 Patients. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Vogt, P.R. Arterial allografts in treating aortic graft infections: Something old, something new. Semin. Vasc. Surg. 2011, 24, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Antunovic, L.; Chiti, A.; Kirienko, M. Towards clinical application of image mining: A systematic review on artificial intelligence and radiomics. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2656–2672. [Google Scholar] [CrossRef] [Green Version]
- Charalambous, S.; Klontzas, M.E.; Kontopodis, N.; Ioannou, C.V.; Perisinakis, K.; Maris, T.G.; Damilakis, J.; Karantanas, A.; Tsetis, D. Radiomics and machine learning to predict aggressive type 2 endoleaks after endovascular aneurysm repair: A proof of concept. Acta Radiol. 2022, 63, 1293–1299. [Google Scholar] [CrossRef]
- Häyry, P.; Isoniemi, H.; Yilmaz, S.; Mennander, A.; Lemström, K.; Räisänen-Sokolowski, A.; Koskinen, P.; Ustinov, J.; Lautenschlager, I.; Taskinen, E.; et al. Chronic allograft rejection. Immunol. Rev. 1993, 134, 33–81. [Google Scholar] [CrossRef]
- Plissonnier, D.; Nochy, D.; Poncet, P.; Mandet, C.; Hinglais, N.; Bariety, J.; Michel, J.B. Sequential immunological targeting of chronic experimental arterial allograft. Transplantation 1995, 60, 414–424. [Google Scholar] [CrossRef]
- Pasquinelli, G.; Pistillo, M.P.; Ricci, F.; Buzzi, M.; Tazzari, P.L.; Foroni, L.; Manferdini, C.; Ceccarelli, C.; Stella, A.; Conte, R. The “in situ” expression of human leukocyte antigen class I antigens is not altered by cryopreservation in human arterial allografts. Cell Tissue Bank 2007, 8, 195–203. [Google Scholar] [CrossRef]
- Mirelli, M.; Buzzi, M.; Pasquinelli, G.; Tazzari, P.L.; Testi, G.; Ricchi, E.; Conte, R.; Stella, A. Fresh and cryopreserved arterial homografts: Immunological and clinical results. Transpl. Proc. 2005, 37, 2688–2691. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n = 12 Patients | |
|---|---|
| Male sex | 10 (83.3%) |
| Smoking | 4 (33.3%) |
| Former smoking | 4 (33.3%) |
| Hypertension | 10 (83.3%) |
| Chronic obstructive pulmonary disease | 4 (33.3%) |
| Diabetes mellitus | 5 (41.7%) |
| Coronary artery disease | 4 (33.3%) |
| Chronic renal failure * | 2 (16.6%) |
| Allograft | Native Aorta | p | |
|---|---|---|---|
| SUVmin | 0.56 | 0.26 | 0.0134 |
| SUVmax | 3.54 | 2.66 | 0.0228 |
| TLG (mL) | 51.53 | 34.44 | 0.0051 |
| SHAPE_Volume | 29.05 | 16.478 | 0.0007 |
| SHAPE_Sphericity | 0.93 | 0.38 | 0.0014 |
| SHAPE_Compacity | 2.09 | 1.23 | 0.0001 |
| GLCM_Correlation | 0.54 | 0.23 | 0.0033 |
| GLRLM_GLNU | 158.29 | 57.31 | 0.0041 |
| GLRLM_RLNU | 566.08 | 119.97 | 0.0003 |
| NGLDM_Coarseness | 0.09 | <0.001 | 0.0041 |
| NGLDM_Busyness | 1.83 | 1.35 | 0.0192 |
| GLZLM_GLNU | 7.73 | 3.34 | 0.0008 |
| GLZLM_ZLNU | 11.69 | 3.56 | 0.0011 |
| Dilated Allograft | Native Aorta | p | |
|---|---|---|---|
| SUVmin | 0.25 | 0.15 | 0.0156 |
| SUVmax | 4.18 | 2.59 | 0.0312 |
| TLG (mL) | 112.7 | 84.25 | 0.0063 |
| SHAPE_Volume | 71.27 | 56.48 | 0.0043 |
| SHAPE_Sphericity | 0.87 | 0.38 | 0.0064 |
| SHAPE_Compacity | 2.92 | 1.74 | 0.0063 |
| GLCM_Correlation | 0.62 | 0.23 | 0.0026 |
| GLRLM_GLNU | 342 | 259.42 | 0.0044 |
| GLRLM_RLNU | 1386.71 | 1123.42 | 0.0044 |
| NGLDM_Coarseness | 0.005 | <0.001 | 0.0129 |
| NGLDM_Busyness | 3.11 | 2.22 | 0.0091 |
| GLZLM_GLNU | 14.79 | 10.71 | 0.0044 |
| GLZLM_ZLNU | 27.61 | 23.86 | 0.0452 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berchiolli, R.; Torri, L.; Bertagna, G.; Canovaro, F.; Zanca, R.; Bartoli, F.; Mocellin, D.M.; Ferrari, M.; Erba, P.A.; Troisi, N. [18F]-Fludeoxyglucose Positron Emission Tomography/Computed Tomography with Radiomics Analysis in Patients Undergoing Aortic In-Situ Reconstruction with Cryopreserved Allografts. Diagnostics 2022, 12, 2831. https://doi.org/10.3390/diagnostics12112831
Berchiolli R, Torri L, Bertagna G, Canovaro F, Zanca R, Bartoli F, Mocellin DM, Ferrari M, Erba PA, Troisi N. [18F]-Fludeoxyglucose Positron Emission Tomography/Computed Tomography with Radiomics Analysis in Patients Undergoing Aortic In-Situ Reconstruction with Cryopreserved Allografts. Diagnostics. 2022; 12(11):2831. https://doi.org/10.3390/diagnostics12112831
Chicago/Turabian StyleBerchiolli, Raffaella, Lorenzo Torri, Giulia Bertagna, Francesco Canovaro, Roberta Zanca, Francesco Bartoli, Davide Maria Mocellin, Mauro Ferrari, Paola Anna Erba, and Nicola Troisi. 2022. "[18F]-Fludeoxyglucose Positron Emission Tomography/Computed Tomography with Radiomics Analysis in Patients Undergoing Aortic In-Situ Reconstruction with Cryopreserved Allografts" Diagnostics 12, no. 11: 2831. https://doi.org/10.3390/diagnostics12112831