
Clinical and Imaging Predictors of Disease Progression in Type B Aortic Intramural Hematomas and Penetrating Aortic Ulcers: A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction
2.4. Imaging Evaluation
3. Results
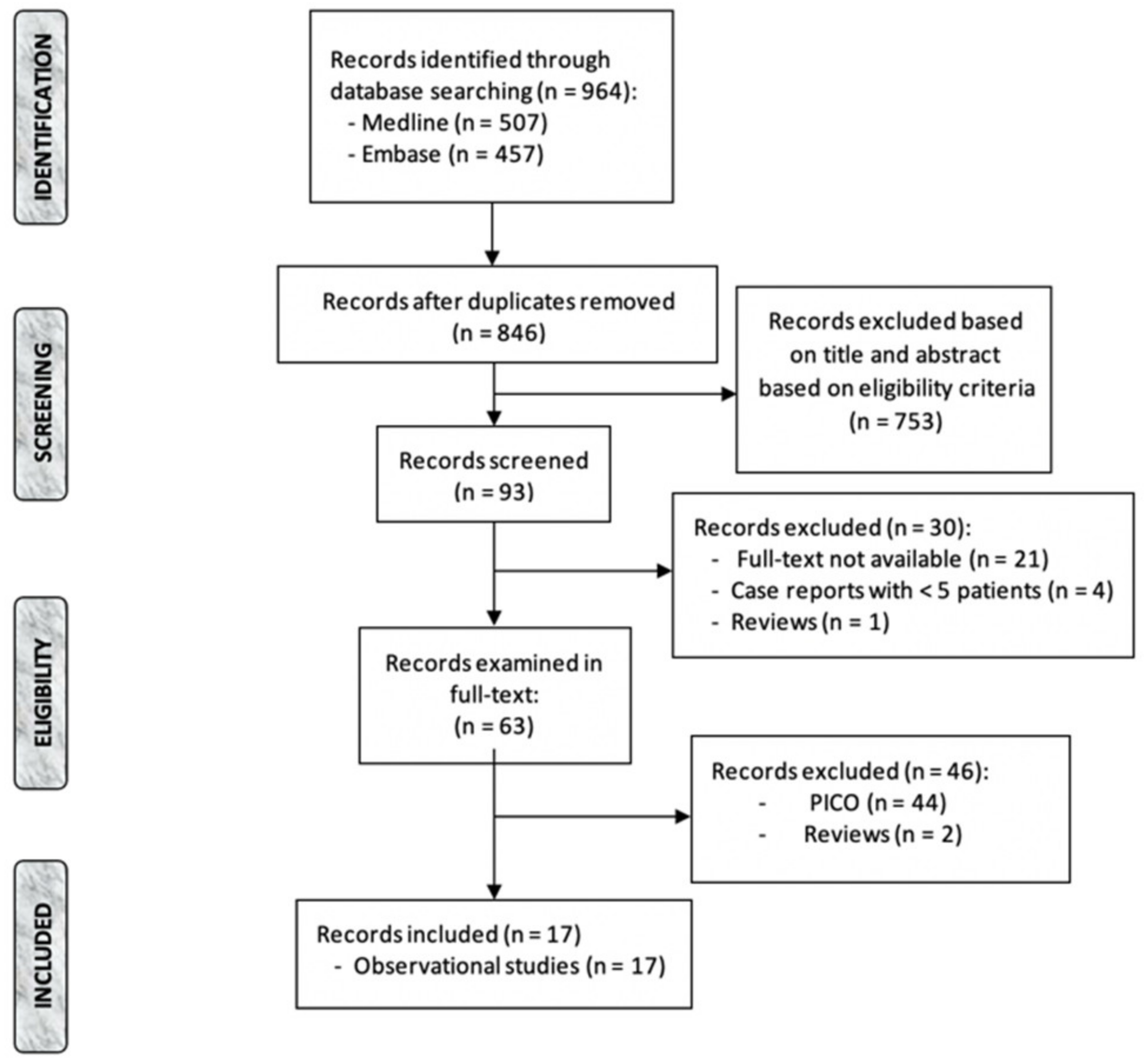
3.1. Study Selection and Overall Characteristics
3.2. Outcomes
3.2.1. PAU

{kind=link}
| Study | Year | N° of PAUs (%) | N° of Type B (%) | Acute (n°) | Follow-Up | Radiologic Features |
|---|---|---|---|---|---|---|
| Jànosi et al. [14] | 2016 | 63 (100) | 52 (82.5) | 63 | 45.6 months | PAU length, depth, neck width, longitudinal extension, MAD. |
| Yang et al. [11] | 2020 | 109 (100) | 76 (70%) | 109 | 23 months | PAU length, depth, neck width, longitudinal extension, MAD, thickness of periaortic hematoma. |
| Squizzato et al. [5] | 2022 | 28 (21) | 28 (100) | 9 | 8.1 years | PAU length, depth, neck width, longitudinal extension, MAD. |
| Piazza et al. [10] | 2022 | 37 (68.5) | 37 (100) | 37 | 34 months | PAU length, depth, neck width, longitudinal extension, MAD, thickness of periaortic hematoma. |
3.2.2. IMH
| Study | Year | N° of IMHs (%) | Type B (%) | Acute (n°) | Follow-Up | Radiologic Features |
|---|---|---|---|---|---|---|
| Sebastià et al. [22] | 2012 | 34 (100) | 34 (100) | 34 | 5.9 years | MAD; MAD indexed with body surface; MHT; IMH length; ulcers; mediastinal hematoma. |
| Sueyoshi et al. [12] | 2017 | 65 (100) | 65 (100) | 65 | 28 months | MAD, MHT, IBP, intimal defect, pleural fluid. |
| Sailer et al. [23] | 2017 | 44 (32) | 44 (100) | 44 | 861 days | MAD. |
| Moral et al. [24] | 2017 | 107 (100) | 107 (100) | 107 | 56 months | FID: presence, location, depth, orifice; MAD; MHT. |
| Liu et al. [21] | 2018 | 123 (100) | 84 (69) | 116 | 20 months | MAD; MHT; atherosclerosis plaque; echo-lucent areas; circular shape. |
| Yang et al. [13] | 2019 | 34 (100) | 34 (100) | 34 | 42 days | Initial ULP and MAD; Changes in ULP and MAD; SUVmax; SUVsvc; TBR. |
| Li et al. [25] | 2019 | 238 (100) | 238 (100) | 238 | 543 days | IMH presence and location; ULP; IBP; MHT; MAD. |
| Bolomey et al. [15] | 2020 | 25 (100) | 25 (100) | 25 | 18 months | IMH location and longitudinal extension, MHT, volume of IMH, MAD, aortic volume, diameter and volume of circulating lumen. |
| Chen et al. [16] | 2020 | 226 (100) | 226 (100) | 226 | 45.9 months | MAD, MHT, aortic tortuosity, FID |
| Chen et al. [18] | 2021 | 149 (100) | 149 (100) | 149 | 38.5 months | MAD, MHT, FID. |
| Ishizu et al. [19] | 2021 | 76 (100) | 76 (100) | 76 | 4 years | MAD, MHT, Presence and location of FID, MHT at FID, calcified plaques adjacent to FID. |
| Yang et al. [20] | 2021 | 61 (100) | 61 (100) | 61 | 167.3 weeks | MAD, MHT, MHT > 10 mm, ULP. |
| Squizzato et al. [5] | 2022 | 12 (9) | 11 (91.7) | 8 | 8.1 years | IMH location and longitudinal extension, MHT, MAD. |
| Chen et al. [17] | 2022 | 127 (100) | 127 (100) | 127 | 43 months | MAD, MHT, FID. |
| Piazza et al. [10] | 2022 | 17 (31.5) | 17 (100) | 17 | 34 months | IMH location and longitudinal extension; MHT, ULP; IBP; MAD. |
3.3. Markers of Disease Progression
3.3.1. PAU
| Study | Year | Disease Progression | Aortic-Related Mortality | Radiologic Evolution | Predictors of AAE |
|---|---|---|---|---|---|
| Jànosi et al. [14] | 2016 | TEVAR < 14 d = 33/63 (52.3%); TEVAR 40 d = 30/63 (47.7%) | 30 d = 5/63 (7.9%); 1 y, 5 y and 10 y survival = 88.4%, 84.2%, 65.7% | - | PAU depth > 15 mm |
| Yang et al. [11] | 2020 | 30 d PAU AAE = 31/109 (28%); 30 d AD = 7/109 (6.4%); 30 d clinically-related adverse events = 7/109 (6.4%); Late aortic-related events = 34/109 (31%); Late AD 8/109 (7.3%); Late clinically related adverse events = 13/109 (12%) | 30 d = 3/109 (2.7%); Late = 5/109 (4.6%) | Increase in PAU diameter and depth = 23/109 (21%) | PAU diameter > 12.5 PAU depth > 9.5 mm |
| Squizzato et al. [5] | 2022 | Freedom from clinical progression at 1, 5 and 10 y = 90.5%, 70.6% and 45.8%; 10 y PAU rupture rate = 7.2%; Disease resolution at 1, 5 and 10 y = 0%, 10.6%, 10.6% | 10 y PAU mortality rate= 8.4%; | MAD increase = 0.4 mm/y (IQR 0–1.8); PAU depth increase = 0.5 mm/y (IQR 0.1–1.4); PAU width increase = 1.1 mm/y (IQR 0.7–1.7); Neck width increase = 1.1 mm/y (IQR 0.6–4.6) | PAU depth > 10 mm |
| Piazza et al. [10] | 2022 | Evolution to AD = 1/37 (2.7); TEVAR = 10/37 (27); Open 1/37 (2.7) | 30 d = 1/37 (2.7) | MAD increase = 5 mm/2 weeks = 2/37 (5.4) | PAU width > 20 mm PAU depth > 15 mm PAU depth/total aortic diameter > 0.3 Paravisceral aortic PAU MAD > 35 mm |
3.3.2. IMH
| Study | Year | Clinical Progression | Aortic-Related Mortality | Radiologic Evolution | Predictors of AAE |
|---|---|---|---|---|---|
| Sebastià et al. [22] | 2012 | TEVAR = 2/34 (5.8) | 0 | Regression = 19/34 (56); Progression 15/34 (44); Regression of mediastinal hematoma = 4/4 (100); 7/10 ulcers progressed to aneurysm | Ulcers |
| Sueyoshi et al. [12] | 2017 | AAE = 23/65 (35%); Surgical repair = 7/65 (10.7) | 3/65 (4.6) | Enlargement of ULP = 15/65 (24%) | EFL at initial CTA |
| Sailer et al. [23] | 2017 | Adverse events = 9/44 (21); AD = 7/44 (16); Resolution = 26/44 (59); TEVAR = 5/44 (11); 1 y, 2 y and 5 y probability of event-free survival = 76.5%, 76.5%, 68.9% | - | Non-resorbing IMH = Aortic grow-rate 1.49 mm/month | Non-reabsorption of IMH |
| Moral et al. [24] | 2017 | Early TEVAR = 10/107 (10); Late TEVAR = 7/94 | 30 d = 4/107 (4); Late = 1/94 (1) | FID development = 43/107 (40%) → 11 in the acute phase | FID development in the acute phase; |
| Liu et al. [21] | 2018 | TEVAR = 10/81 (12.3); 30 d AAE = 42/123; 30 d-6 m AAE = 7/81 | 30 d = 3/84 (3.5) | IMH regression = 68/123 | Baseline MAD ≥ 44.75; Acute PAU development; |
| Yang et al. [13] | 2019 | AAE = 18/34 (53); TEVAR = 3/34 (8.8) | 0 | - | TBR > 1.5 in patients with ULP |
| Li et al. [25] | 2019 | AAE = 83/238 (40); Treatment = 76/238 (32); | Overall = 7/238 (3) | Median MHT and MAD change during follow-up = −1.5 mm and −1.1 mm; Newly developed ULP and IBP = 16 and 75 | Baseline MHT ≥ 18.8; baseline MAD ≥ 38.2; ULP development; Changes in MHT; Pleural effusion development |
| Bolomey et al. [15] | 2020 | FEG = 13/25 pts (52%); UEG = 12/25 pts (48); 11 interventions; | 2/25 pts (8%) | UEG: increase in aortic diameter | Male gender; Typical pain; IMH occurrence < 2015; Aortic diameter > 38 mm at D0 and 40 mm at M1; Circulating lumen diameter > 32 mm at D0 and 34 mm at M1; PAU at M1 |
| Chen et al. [16] | 2020 | TEVAR= 27/187 pts (14.4%) | 1 y: 28/187 (15%); postoperative: 13/27 (48%) | FID development = 61/187 (32.6); MHT increase = 6/187 (3.2) | FID development; Higher CRP level |
| Chen et al. [18] | 2021 | Acute phase TEVAR = DM 1/60 (2%); non-DM 11/89 (12%); Disease progression after onset = DM 12 d; non-DM 6.4 d | 30 d = DM 0/60 (0%), non-DM 8/89 (9%); Late = DM 1/60(2%), non-DM 9/81 (11%) | Acute ULP = DM 0/60 (0%); non-DM 7/89 (7%); Acute signs of aortic rupture = DM 0/60 (0%); non-DM 8/89 (9%); Late worsening of hematoma = DM 3/60 (5%); non-DM 18/81 (22%) | ULP development during acute phase; Higher CRP level; Higher MMP-9 level |
| Ishizu et al. [19] | 2021 | AAE = no-FID 4 (15%); small-FID 2 (9%); large-FID 15 (54%); | 30 d = 0; Late= no-FID 2/26 (8%), small-FID 1/22 (5%), large-FID 5/28 (18%); | Significant enlargement of large-FID | Large FID; MAD ≥ 40 mm |
| Yang et al. [20] | 2021 | AAE = 36/61 (59%); intervention = 24/61 (39%) | 1/61 (1.6) | IMH progression 14/61 (23%); ULP progression 11/61 (18%) | ULP; eGFR < 90 |
| Squizzato et al. [5] | 2022 | Freedom from clinical progression at 1, 5 and 10 y = 44.4%; The 10 y aortic rupture rate = 20%; Disease resolution at 1 and 5 y: 0%, 22.2% | 10 y = 28.9 % | Aortic grow-rate = 0.2 mm/y (IQR −0.1–0.6) | Initial MAD; IMH location in the aortic arch |
| Chen et al. [17] | 2022 | Acute AAE = 17/76 (22%); Late TEVAR/surgery/reintervention = OSA 28/76 (37%); 2/51 (4%) | OSA = 9/76 (11.8%); non-OSA = 1/51 (1.9%) | Acute ULP = OSA 13/76 (17%); non-OSA 0/51 (0%); Late ULP = OSA 28/76 (37%); non-OSA 1/51 (2%); Late IMH resolution = OSA 41/76 (54%); non-OSA 49/51 (96%) | TEVAR; Higher mean morning systolic pressure; OSA; |
| Piazza et al. [10] | 2022 | Progression to AD = 2/17 (11.8); TEVAR =8/17 (47); Open = 3/17 (37.6) | Acute = 2/17 (11.8) | MAD > 5 mm/2 w = 4/17 (23.6) | ULP; IMH extension > 3 aortic zones |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Riambau, V.; Böckler, D.; Brunkwall, J.; Cao, P.; Chiesa, R.; Coppi, G.; Czerny, M.; Fraedrich, G.; Haulon, S.; Jacobs, M.J.; et al. Editor’s Choice—Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 4–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathan, D.P.; Boonn, W.; Lai, E.; Wang, G.J.; Desai, N.; Woo, E.Y.; Fairman, R.M.; Jackson, B.M. Presentation, complications, and natural history of penetrating atherosclerotic ulcer disease. J. Vasc. Surg. 2012, 55, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutschow, S.E.; Walker, C.M.; Martínez-Jiménez, S.; Rosado-de-Christenson, M.L.; Stowell, J.; Kunin, J.R. Emerging Concepts in Intramural Hematoma Imaging. RadioGraphics 2016, 36, 660–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, H.; Matsuoka, Y.; Sakamoto, I.; Sueyoshi, E.; Okimoto, T.; Hayashi, K.; Matsunaga, N. Penetrating atherosclerotic ulcer of the aorta: Imaging features and disease concept. RadioGraphics 2000, 20, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Squizzato, F.; Hyun, M.; Sen, I.; D’Oria, M.; Bower, T.; Oderich, G. Predictors of Long-Term Aortic Growth and Disease Progression in Patients With Aortic Dissection, Intramural Hematoma, and Penetrating Aortic Ulcer. J. Vasc. Surg. 2022, 75, 1117. [Google Scholar] [CrossRef]
- Oderich, G.S.; Kärkkäinen, J.M.; Reed, N.R.; Tenorio, E.R.; Sandri, G.A. Penetrating Aortic Ulcer and Intramural Hematoma. Cardiovasc. Interv. Radiol. 2019, 42, 321–334. [Google Scholar] [CrossRef]
- Harris, K.M.; Strauss, C.E.; Eagle, K.A.; Hirsch, A.T.; Isselbacher, E.M.; Tsai, T.T.; Shiran, H.; Fattori, R.; Evangelista, A.; Cooper, J.V.; et al. Correlates of delayed recognition and treatment of acute type A aortic dissection: The International Registry of Acute Aortic Dissection (IRAD). Circulation 2011, 124, 1911–1918. [Google Scholar] [CrossRef] [Green Version]
- DeMartino, R.R.; Sen, I.; Huang, Y.; Bower, T.C.; Oderich, G.S.; Pochettino, A.; Greason, K.; Kalra, M.; Johnstone, J.; Shuja, F.; et al. Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004689. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Piazza, M.; Squizzato, F.; Porcellato, L.; Casali, E.; Grego, F.; Antonello, M. Predictors Of Intervention In Acute Type B Aortic Penetrating Ulcer And Intramural Hematoma. Semin. Thorac. Cardiovasc. Surg. 2022. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, Q.-Y.; Wang, X.-Z.; Zhao, X.; Liu, X.-Z.; Wang, P.; Jing, Q.-M.; Han, Y.-L. Long-term imaging evolution and clinical prognosis among patients with acute penetrating aortic ulcers: A retrospective observational study. J. Am. Heart Assoc. 2020, 9, e014505. [Google Scholar] [CrossRef] [PubMed]
- Sueyoshi, E.; Onizuka, H.; Nagayama, H.; Sakamoto, I.; Uetani, M. Clinical importance of minimal enhancement of type B intramural hematoma of the aorta on computed tomography imaging. J. Vasc. Surg. 2017, 65, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, F.; Luo, J.; Hou, Q.; Xie, N.; Nie, Z.; Huang, W.; Liu, Y.; Zhou, Y.; Chen, J.; Geng, Q. Predictive value of 18F-FDG PET/CT in patients with acute type B aortic intramural hematoma. J. Nucl. Cardiol. 2019, 26, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Jánosi, R.A.; Gorla, R.; Tsagakis, K.; Kahlert, P.; Horacek, M.; Bruckschen, F.; Dohle, D.-S.; Jakob, H.; Schlosser, T.; Eggebrecht, H.; et al. Thoracic Endovascular Repair of Complicated Penetrating Aortic Ulcer: An 11-Year Single-Center Experience. J. Endovasc. Ther. Off. J. Int. Soc. Endovasc. Spec. 2016, 23, 150–159. [Google Scholar] [CrossRef]
- Bolomey, S.; Blanchard, A.; Barral, P.-A.; Mancini, J.; Lagier, D.; Bal, L.; De Masi, M.; Jacquier, A.; Piquet, P.; Gaudry, M. Is the Natural Anatomical Evolution of Type B Intramural Hematomas Reliable to Identify the Patients at Risk of Aneurysmal Progression? Ann. Vasc. Surg. 2020, 64, 62–70. [Google Scholar] [CrossRef]
- Chen, Q.; Jiang, D.; Kuang, F.; Shan, Z. The evolution of treatments for uncomplicated type B intramural hematoma patients. J. Card. Surg. 2020, 35, 580–590. [Google Scholar] [CrossRef]
- Chen, Q.; Jiang, D.; Shan, Z. Progression of type B intramural hematoma in patients with obstructive sleep apnea. J. Vasc. Surg. 2022, 76, 378–388.e3. [Google Scholar] [CrossRef]
- Chen, Q.; Jiang, D.; Kuang, F.; Yang, F.; Shan, Z. Outcomes of uncomplicated Type B intramural hematoma patients with Type 2 diabetes mellitus. J. Card. Surg. 2021, 36, 1209–1218. [Google Scholar] [CrossRef]
- Ishizu, K.; Kaji, S.; Nakashima, M.; Kitai, T.; Kim, K.; Ehara, N.; Kinoshita, M.; Furukawa, Y. Focal Intimal Disruption Size at Multidetector CT and Disease Progression in Type B Aortic Intramural Hematoma. Radiology 2021, 301, 311–319. [Google Scholar] [CrossRef]
- Yang, Y.; Li, W.; Liu, M.; Zhang, X.; Li, Q. Prognostic value of estimated glomerular filtration rate and presence of proteinuria in type B aortic intramural hematoma. J. Thorac. Dis. 2021, 13, 946–954. [Google Scholar] [CrossRef]
- Liu, Y.-J.; Zhang, Q.-Y.; Du, Z.-K.; Yang, L.; Zhang, L.; He, R.-X.; Wang, Y.; Han, Y.-L.; Wang, X.-Z. Long-term follow-up and clinical implications in Chinese patients with aortic intramural hematomas. Int. J. Cardiol. 2018, 270, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Sebastià, C.; Evangelista, A.; Quiroga, S.; Cuellar, H.; Aguilar, R.; Muntanyà, X. Predictive value of small ulcers in the evolution of acute type B intramural hematoma. Eur. J. Radiol. 2012, 81, 1569–1574. [Google Scholar] [CrossRef] [PubMed]
- Sailer, A.M.; Nelemans, P.J.; Hastie, T.J.; Chin, A.S.; Huininga, M.; Chiu, P.; Fischbein, M.P.; Dake, M.D.; Miller, D.C.; Schurink, G.W.; et al. Prognostic significance of early aortic remodeling in acute uncomplicated type B aortic dissection and intramural hematoma. J. Thorac. Cardiovasc. Surg. 2017, 154, 1192–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moral, S.; Cuéllar, H.; Avegliano, G.; Ballesteros, E.; Salcedo, M.T.; Ferreira-González, I.; García-Dorado, D.; Evangelista, A. Clinical Implications of Focal Intimal Disruption in Patients with Type B Intramural Hematoma. J. Am. Coll. Cardiol. 2017, 69, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Lu, B.; Chen, Y.; Hou, Z.; Chen, B.; Zhang, Y.; An, Y.; Wei, Y. Acute type B aortic intramural hematoma: The added prognostic value of a follow-up CT. Eur. Radiol. 2019, 29, 6571–6580. [Google Scholar] [CrossRef] [PubMed]
- Batt, M.; Haudebourg, P.; Planchard, P.-F.; Ferrari, E.; Hassen-Khodja, R.; Bouillanne, P.-J. Penetrating atherosclerotic ulcers of the infrarenal aorta: Life-threatening lesions. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2005, 29, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coady, M.A.; Rizzo, J.A.; Hammond, G.L.; Pierce, J.G.; Kopf, G.S.; Elefteriades, J.A. Penetrating ulcer of the thoracic aorta: What is it? How do we recognize it? How do we manage it? J. Vasc. Surg. 1998, 27, 1006. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, J.V.; Hughes, G.C.; Appoo, J.J.; Bavaria, J.E.; Beck, A.W.; Cambria, R.P.; Charlton-Ouw, K.; Eslami, M.H.; Kim, K.M.; Leshnower, B.G.; et al. Society for Vascular Surgery (SVS) and Society of Thoracic Surgeons (STS) Reporting Standards for Type B Aortic Dissections. Ann. Thorac. Surg. 2020, 109, 959–981. [Google Scholar] [CrossRef]
- Hussain, S.; Glover, J.L.; Bree, R.; Bendick, P.J. Penetrating atherosclerotic ulcers of the thoracic aorta. J. Vasc. Surg. 1989, 9, 710–717. [Google Scholar] [CrossRef] [Green Version]
- Evangelista, A.; Mukherjee, D.; Mehta, R.H.; O’Gara, P.T.; Fattori, R.; Cooper, J.V.; Smith, D.E.; Oh, J.K.; Hutchison, S.; Sechtem, U.; et al. Acute intramural hematoma of the aorta: A mystery in evolution. Circulation 2005, 111, 1063–1070. [Google Scholar] [CrossRef]
- Ganaha, F.; Miller, D.C.; Sugimoto, K.; Do, Y.S.; Minamiguchi, H.; Saito, H.; Mitchell, R.S.; Dake, M.D. Prognosis of aortic intramural hematoma with and without penetrating atherosclerotic ulcer: A clinical and radiological analysis. Circulation 2002, 106, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Pandey, G.; Sharma, P. The Management of Patients With Penetrating Aortic Ulcers: A Systematic Review. Vasc. Endovasc. Surg. 2021, 55, 730–740. [Google Scholar] [CrossRef] [PubMed]
- Czerny, M.; Funovics, M.; Sodeck, G.; Dumfarth, J.; Schoder, M.; Juraszek, A.; Dziodzio, T.; Loewe, C.; Reineke, D.; Krähenbühl, E.; et al. Results after thoracic endovascular aortic repair in penetrating atherosclerotic ulcers. Ann. Thorac. Surg. 2011, 92, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Georgiadis, G.S.; Trellopoulos, G.; Antoniou, G.A.; Georgakarakos, E.I.; Nikolopoulos, E.S.; Pelekas, D.; Pitta, X.; Lazarides, M.K. Endovascular therapy for penetrating ulcers of the infrarenal aorta. ANZ J. Surg. 2013, 83, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Mestres, G.; Rodríguez, R.; García-Madrid, C.; Montañà, X.; Burrel, M.; Cruz, L.F.; Flores, C.; Riambau, V. Endovascular treatment of penetrating aortic ulcers: Mid-term follow-up. Rev. Esp. Cardiol. 2012, 65, 54–59. [Google Scholar] [CrossRef]
- Evangelista, A.; Czerny, M.; Nienaber, C.; Schepens, M.; Rousseau, H.; Cao, P.; Moral, S.; Fattori, R. Interdisciplinary expert consensus on management of type B intramural haematoma and penetrating aortic ulcer. Eur. J. Cardio-Thoracic Surg. 2015, 47, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Gifford, S.M.; Duncan, A.A.; Greiten, L.E.; Gloviczki, P.; Oderich, G.S.; Kalra, M.; Fleming, M.D.; Bower, T.C. The natural history and outcomes for thoracic and abdominal penetrating aortic ulcers. J. Vasc. Surg. 2016, 63, 1182–1188. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colacchio, E.C.; Squizzato, F.; Piazza, M.; Menegolo, M.; Grego, F.; Antonello, M. Clinical and Imaging Predictors of Disease Progression in Type B Aortic Intramural Hematomas and Penetrating Aortic Ulcers: A Systematic Review. Diagnostics 2022, 12, 2727. https://doi.org/10.3390/diagnostics12112727
Colacchio EC, Squizzato F, Piazza M, Menegolo M, Grego F, Antonello M. Clinical and Imaging Predictors of Disease Progression in Type B Aortic Intramural Hematomas and Penetrating Aortic Ulcers: A Systematic Review. Diagnostics. 2022; 12(11):2727. https://doi.org/10.3390/diagnostics12112727
Chicago/Turabian StyleColacchio, Elda Chiara, Francesco Squizzato, Michele Piazza, Mirko Menegolo, Franco Grego, and Michele Antonello. 2022. "Clinical and Imaging Predictors of Disease Progression in Type B Aortic Intramural Hematomas and Penetrating Aortic Ulcers: A Systematic Review" Diagnostics 12, no. 11: 2727. https://doi.org/10.3390/diagnostics12112727