
Bone Fracture Detection Using Deep Supervised Learning from Radiological Images: A Paradigm Shift

Abstract
:1. Introduction
- What different kinds of bone fractures are there?
- What deep learning techniques are used in bone fracture detection and classification?
- How are deep learning methods beneficial over traditional methods?
- How does deep learning in radiology immensely help medical practitioners?
- What are the current challenges and opportunities in computerized disease detection from the bone?
- What are the future research prospects in this field?
1.1. Common Bone Disorder
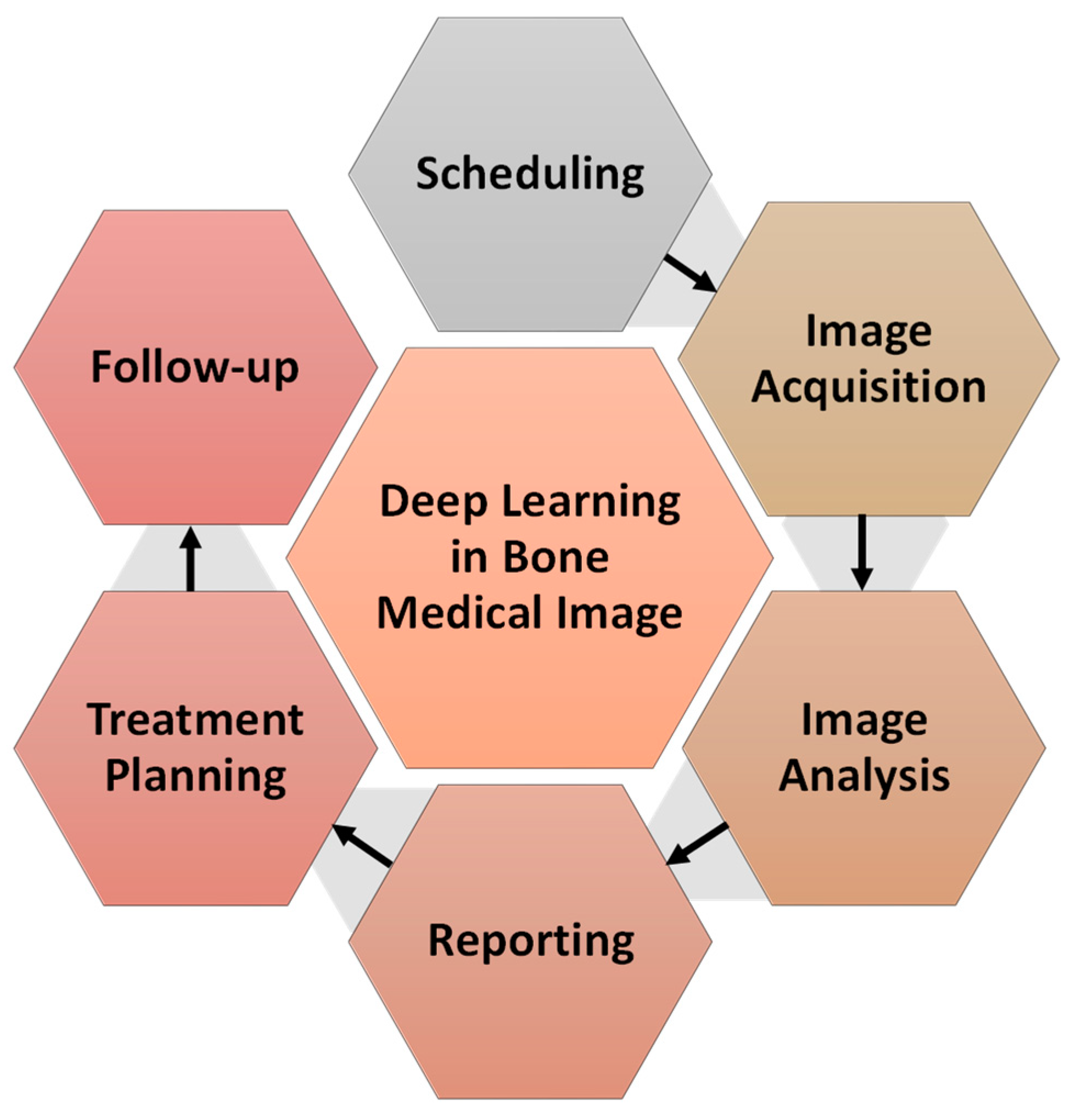
1.2. Importance of Deep Learning in Orthopaedic and Radiology
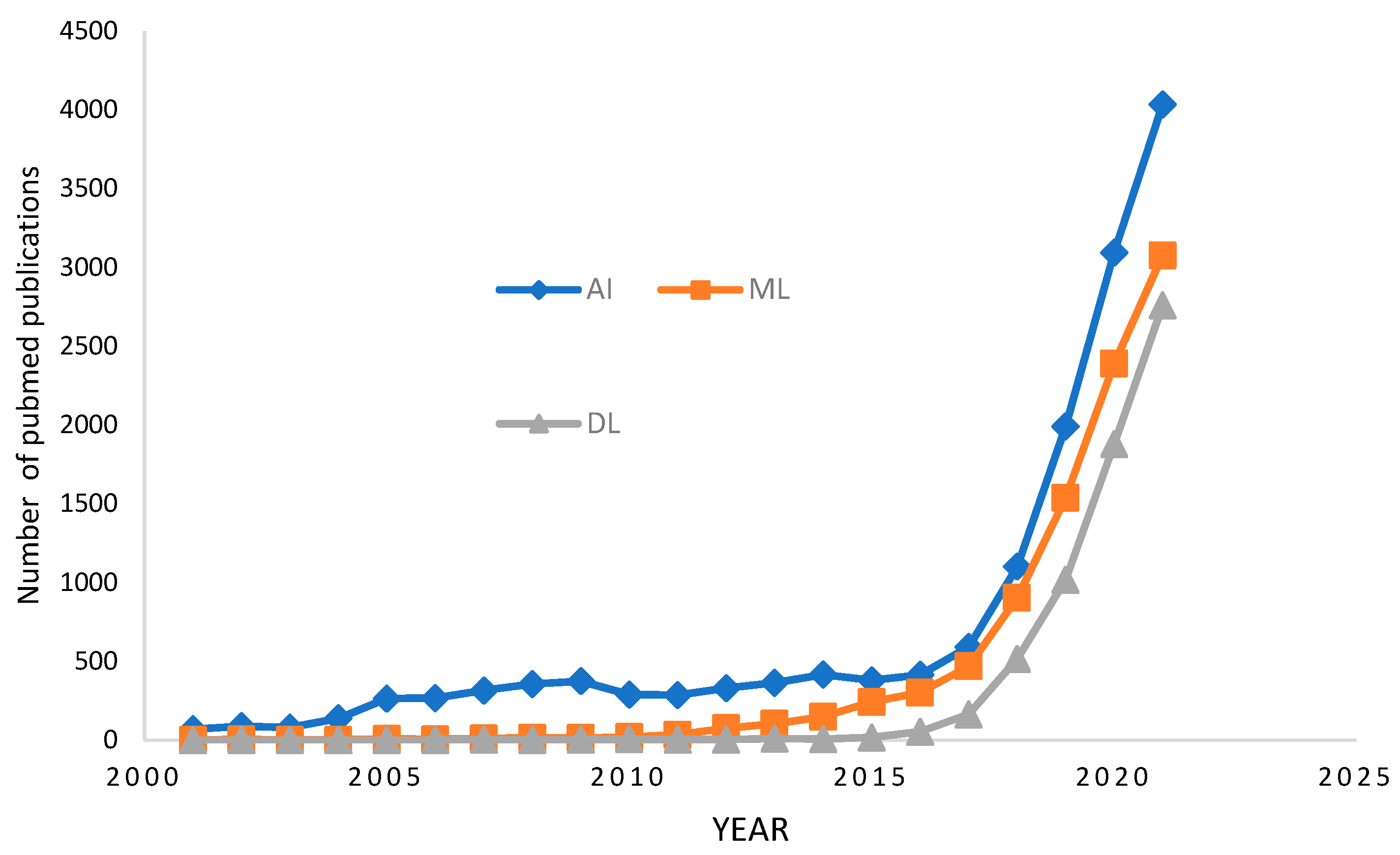
1.3. Historical Perspective
2. Deep Learning and Key Techniques in Bone Imaging
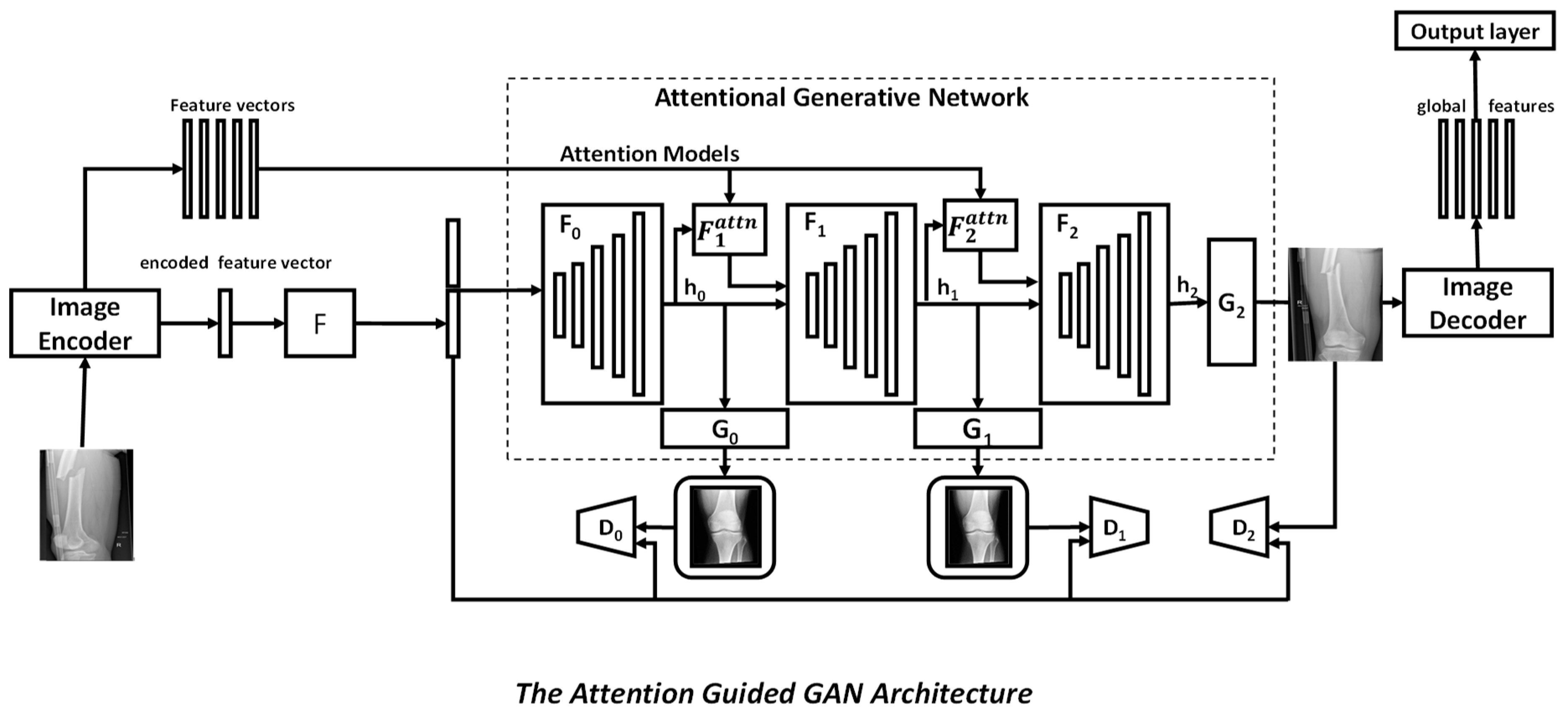
2.1. Network Structure
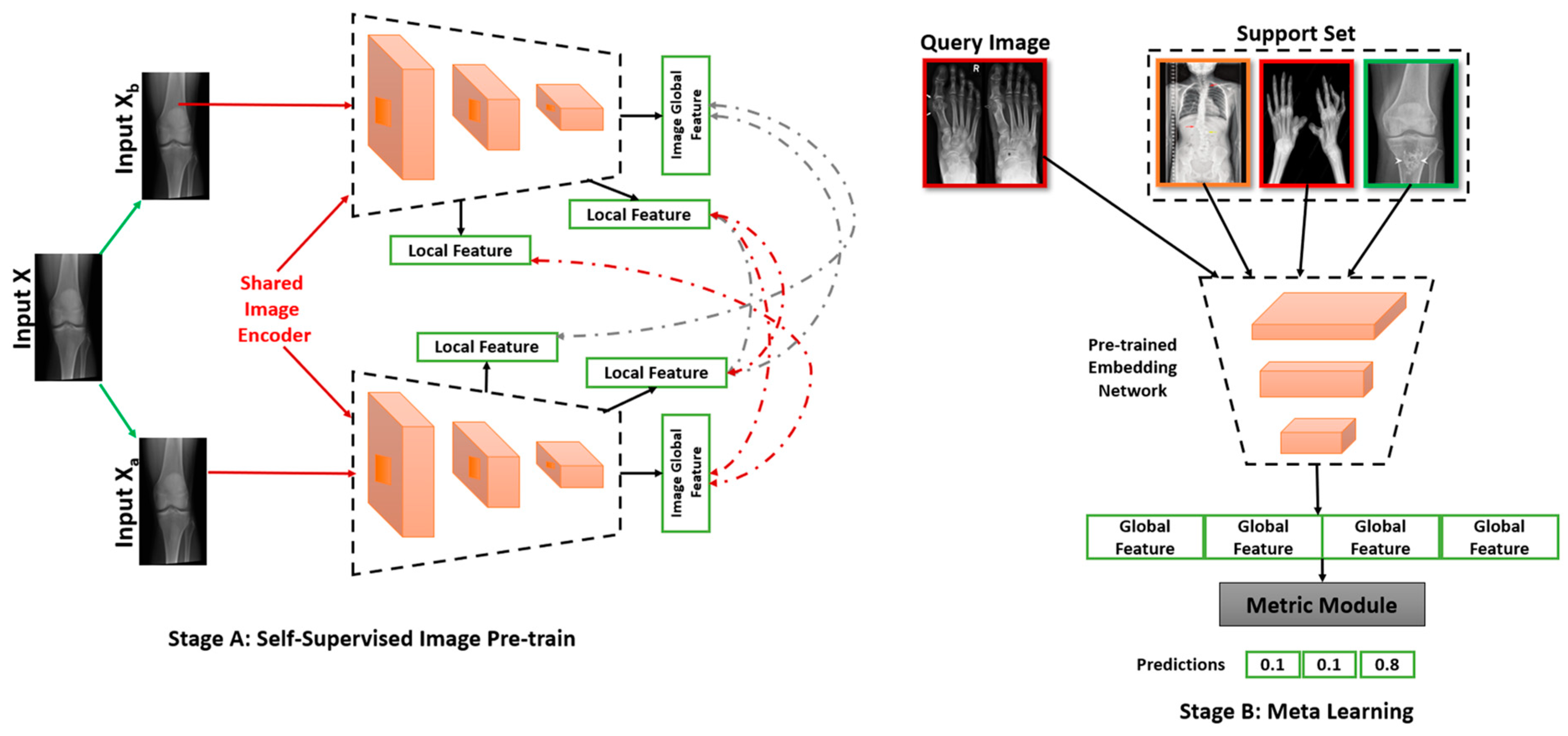
2.2. Annotation Efficient Approaches
2.3. Fractures in Upper Limbs
2.4. Fractures in Lower Limb
2.5. Vertebrae Fractures
3. Deep Learning in Fracture Detection
4. Barriers to DL in Radiology & Challenges
4.1. Challenges in Data Acquisition
4.2. Legal and Ethical Challenges
- A robot may not injure a human being or, through inaction, allow a human being to come to harm.
- A robot must obey the orders given it by human beings except where such orders would conflict with the First Law.
- A robot must protect its own existence as long as such protection does not conflict with the First or Second Laws.
4.3. Requirement for Accessing to Large Volumes of Medical Data
5. Limitations and Constraints of DL Application in Clinical Settings
6. Future Aspect
6.1. DL in Radiology Training
6.2. Will DL Be Free to Hold the Position of a Radiologist?
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and Validation of a Deep Learning Algorithm for Detection of Diabetic Retinopathy in Retinal Fundus Photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Bandyopadhyay, S.K. A new method of brain tissues segmentation from MRI with accuracy estimation. Procedia Comput. Sci. 2016, 85, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Roy, S.; Whitehead, T.D.; Quirk, J.D.; Salter, A.; Ademuyiwa, F.O.; Li, S.; An, H.; Shoghi, K.I. Optimal co-clinical radiomics: Sensitivity of radiomic features to tumour volume, image noise and resolution in co-clinical T1-weighted and T2-weighted magnetic resonance imaging. eBioMedicine 2020, 59, 102963. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Whitehead, T.D.; Li, S.; Ademuyiwa, F.O.; Wahl, R.L.; Dehdashti, F.; Shoghi, K.I. Co-clinical FDG-PET radiomic signature in predicting response to neoadjuvant chemotherapy in triple-negative breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 550–562. [Google Scholar] [CrossRef] [PubMed]
- International Osteoporosis Foundation. Broken Bones, Broken Lives: A Roadmap to Solve the Fragility Fracture Crisis in Europe; International Osteoporosis Foundation: Nyon, Switzerland, 2019; Available online: https://ncdalliance.org/news-events/news/ (accessed on 20 January 2022).
- Krupinski, E.A.; Berbaum, K.S.; Caldwell, R.T.; Schartz, K.M.; Kim, J. Long Radiology Workdays Reduce Detection and Accommodation Accuracy. J. Am. Coll. Radiol. 2010, 7, 698–704. [Google Scholar] [CrossRef] [Green Version]
- Hallas, P.; Ellingsen, T. Errors in fracture diagnoses in the emergency department—Characteristics of patients and diurnal variation. BMC Emerg. Med. 2006, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Lindsey, R.; Daluiski, A.; Chopra, S.; Lachapelle, A.; Mozer, M.; Sicular, S.; Hanel, D.; Gardner, M.; Gupta, A.; Hotchkiss, R.; et al. Deep neural network improves fracture detection by clinicians. Proc. Natl. Acad. Sci. USA 2018, 115, 11591–11596. [Google Scholar] [CrossRef] [Green Version]
- Rayan, J.C.; Reddy, N.; Kan, J.H.; Zhang, W.; Annapragada, A. Binomial classification of pediatric elbow fractures using a deep learning multiview approach emulating radiologist decision making. Radiol. Artif. Intell. 2019, 1, e180015. [Google Scholar] [CrossRef]
- Urakawa, T.; Tanaka, Y.; Goto, S.; Matsuzawa, H.; Watanabe, K.; Endo, N. Detecting intertrochanteric hip fractures with orthopedist-level accuracy using a deep convolutional neural network. Skelet. Radiol. 2019, 48, 239–244. [Google Scholar] [CrossRef]
- Wang, X.; Xu, Z.; Tong, Y.; Xia, L.; Jie, B.; Ding, P.; Bai, H.; Zhang, Y.; He, Y. Detection and classification of mandibular fracture on CT scan using deep convolutional neural network. Clin. Oral Investig. 2022, 26, 4593–4601. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. In Proceedings of the NIPS’12: Proceedings of the 25th International Conference on Neural Information Processing Systems, Red Hook, NY, USA, 3–6 December 2012; pp. 1097–1105. [Google Scholar]
- Kim, H.E.; Cosa-Linan, A.; Santhanam, N.; Jannesari, M.; Maros, M.E.; Ganslandt, T. Transfer learning for medical image classification: A literature review. BMC Med. Imaging 2022, 22, 69. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, Z.; Zhi, W.; Liang, B.; Moses, D.; Dawes, L. Using Convolutional Neural Networks and Transfer Learning for Bone Age Classification. In Proceedings of the 2017 International Conference on Digital Image Computing: Techniques and Applications (DICTA), Sydney, Australia, 29 November–1 December 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Anand, I.; Negi, H.; Kumar, D.; Mittal, M.; Kim, T.; Roy, S. ResU-Net Deep Learning Model for Breast Tumor Segmentation. In Magnetic Resonance Images; Computers, Materials & Continua, Tech Science Press: Henderson, NV, USA, 2021; Volume 67, pp. 3107–3127. [Google Scholar] [CrossRef]
- Shah, P.M.; Ullah, H.; Ullah, R.; Shah, D.; Wang, Y.; Islam, S.U.; Gani, A.; Joel, J.P.; Rodrigues, C. DC-GAN-based synthetic X-ray images augmentation for increasing the performance of EfficientNet for COVID-19 detection. Expert Syst. 2022, 39, e12823. [Google Scholar] [CrossRef] [PubMed]
- Sanaat, A.; Shiri, I.; Ferdowsi, S.; Arabi, H.; Zaidi, H. Robust-Deep: A Method for Increasing Brain Imaging Datasets to Improve Deep Learning Models’ Performance and Robustness. J. Digit. Imaging 2022, 35, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Shoghi, K.I. Computer-Aided Tumor Segmentation from T2-Weighted MR Images of Patient-Derived Tumor Xenografts. In Image Analysis and Recognition; ICIAR 2019. Lecture Notes in Computer Science; Karray, F., Campilho, A., Yu, A., Eds.; Springer: Cham, Switzerland, 2019; Volume 11663. [Google Scholar] [CrossRef]
- Roy, S.; Mitra, A.; Roy, S.; Setua, S.K. Blood vessel segmentation of retinal image using Clifford matched filter and Clifford convolution. Multimed. Tools Appl. 2019, 78, 34839–34865. [Google Scholar] [CrossRef]
- Roy, S.; Bhattacharyya, D.; Bandyopadhyay, S.K.; Kim, T.-H. An improved brain MR image binarization method as a preprocessing for abnormality detection and features extraction. Front. Comput. Sci. 2017, 11, 717–727. [Google Scholar] [CrossRef]
- Al Ghaithi, A.; Al Maskari, S. Artificial intelligence application in bone fracture detection. J. Musculoskelet. Surg. Res. 2021, 5, 4. [Google Scholar] [CrossRef]
- Lin, Q.; Li, T.; Cao, C.; Cao, Y.; Man, Z.; Wang, H. Deep learning based automated diagnosis of bone metastases with SPECT thoracic bone images. Sci. Rep. 2021, 11, 4223. [Google Scholar] [CrossRef]
- Marwa, F.; Zahzah, E.-H.; Bouallegue, K.; Machhout, M. Deep learning based neural network application for automatic ultrasonic computed tomographic bone image segmentation. Multimed. Tools Appl. 2022, 81, 13537–13562. [Google Scholar] [CrossRef]
- Gottapu, R.D.; Dagli, C.H. DenseNet for Anatomical Brain Segmentation. Procedia Comput. Sci. 2018, 140, 179–185. [Google Scholar] [CrossRef]
- Papandrianos, N.I.; Papageorgiou, E.I.; Anagnostis, A.; Papageorgiou, K.; Feleki, A.; Bochtis, D. Development of Convolutional Neural Networkbased Models for Bone Metastasis Classification in Nuclear Medicine. In Proceedings of the 2020 11th International Conference on Information, Intelligence, Systems and Applications (IISA), Piraeus, Greece, 15–17 July 2020; pp. 1–8. [Google Scholar] [CrossRef]
- Rahmaniar, W.; Wang, W.J. Real-time automated segmentation and classification of calcaneal fractures in CT images. Appl. Sci. 2019, 9, 3011. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Goodfellow, I.; Metaxas, D.; Odena, A. Self-Attention Generative Adversarial Networks. In Proceedings of the 36th International Conference on Machine Learning (ICML 2019), Long Beach, CA, USA, 9–15 June 2019; pp. 7354–7363. [Google Scholar]
- Sarvamangala, D.R.; Kulkarni, R.V. Convolutional neural networks in medical image understanding: A survey. Evol. Intell. 2022, 15, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Tyson, S.; Hatem, S.F. Easily Missed Fractures of the Upper Extremity. Radiol. Clin. N. Am. 2015, 53, 717–736. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; MacKinnon, T. Artificial intelligence in fracture detection: Transfer learning from deep convolutional neural networks. Clin. Radiol. 2018, 73, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Olczak, J.; Fahlberg, N.; Maki, A.; Razavian, A.S.; Jilert, A.; Stark, A.; Sköldenberg, O.; Gordon, M. Artificial intelligence for analyzing orthopedic trauma radiographs. Acta Orthop. 2017, 88, 581–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, S.W.; Han, S.S.; Lee, J.W.; Oh, K.S.; Kim, N.R.; Yoon, J.P.; Kim, J.Y.; Moon, S.H.; Kwon, J.; Lee, H.-J.; et al. Automated detection and classification of the proximal humerus fracture by using deep learning algorithm. Acta Orthop. 2018, 89, 468–473. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.T.; Ho, T.Y.; Lee, T.Y.; Chang, C.C.; Chou, C.C.; Chen, C.C.; Chung, I.; Liao, C.H. Application of a deep learning algorithm for detection and visualization of hip fractures on plain pelvic radiographs. Eur. Radiol. 2019, 29, 5469–5477. [Google Scholar] [CrossRef]
- Adams, M.; Chen, W.; Holcdorf, D.; McCusker, M.W.; Howe, P.D.; Gaillard, F. Computer vs. human: Deep learning versus perceptual training for the detection of neck of femur fractures. J. Med. Imaging Radiat. Oncol. 2019, 63, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Balaji, G.N.; Subashini, T.S.; Madhavi, P.; Bhavani, C.H.; Manikandarajan, A. Computer-Aided Detection and Diagnosis of Diaphyseal Femur Fracture. In Smart Intelligent Computing and Applications; Satapathy, S.C., Bhateja, V., Mohanty, J.R., Udgata, S.K., Eds.; Springer: Singapore, 2020; pp. 549–559. [Google Scholar]
- Kitamura, G.; Chung, C.Y.; Moore, B.E., 2nd. Ankle fracture detection utilizing a convolutional neural network ensemble implemented with a small sample, de novo training, and multiview incorporation. J. Digit. Imaging 2019, 32, 672–677. [Google Scholar] [CrossRef] [Green Version]
- Pranata, Y.D.; Wang, K.C.; Wang, J.C.; Idram, I.; Lai, J.Y.; Liu, J.W.; Hsieh, I.-H. Deep learning and SURF for automated classification and detection of calcaneus fractures in CT images. Comput. Methods Programs Biomed. 2019, 171, 27–37. [Google Scholar] [CrossRef]
- Muehlematter, U.J.; Mannil, M.; Becker, A.S.; Vokinger, K.N.; Finkenstaedt, T.; Osterhoff, G.; Fischer, M.A.; Guggenberger, R. Vertebral body insufficiency fractures: Detection of vertebrae at risk on standard CT images using texture analysis and machine learning. Eur. Radiol. 2019, 29, 2207–2217. [Google Scholar] [CrossRef]
- Tomita, N.; Cheung, Y.Y.; Hassanpour, S. Deep neural networks for automatic detection of osteoporotic vertebral fractures on CT scans. Comput. Biol. Med. 2018, 98, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.S.; Yu, S.M.; Erdal, B.S.; Demirer, M.; Gupta, V.; Bigelow, M.; Salvador, A.; Rink, T.; Lenobel, S.; Prevedello, L.; et al. Detection and localisation of hip fractures on anteroposterior radiographs with artificial intelligence: Proof of concept. Clin. Radiol. 2020, 75, 237.e1–237.e9. [Google Scholar] [CrossRef]
- Gan, K.; Xu, D.; Lin, Y.; Shen, Y.; Zhang, T.; Hu, K.; Zhou, K.; Bi, M.; Pan, L.; Wu, W.; et al. Artificial intelligence detection of distal radius fractures: A comparison between the convolutional neural network and professional assessments. Acta Orthop. 2019, 90, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.W.; Cho, Y.J.; Lee, S.; Lee, J.; Lee, S.; Choi, Y.H.; Cheon, J.E.; Ha, J.Y. Using a dual-input convolutional neural network for automated detection of pediatric supracondylar fracture on conventional radiography. Investig. Radiol. 2020, 55, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Majkowska, A.; Mittal, S.; Steiner, D.F.; Reicher, J.J.; McKinney, S.M.; Duggan, G.E.; Eswaran, K.; Chen, P.-H.C.; Liu, Y.; Kalidindi, S.R.; et al. Chest radiograph interpretation with deep learning models: Assessment with radiologist-adjudicated reference standards and population-adjusted evaluation. Radiology 2020, 294, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Johari, M.; Esmaeili, F.; Andalib, A.; Garjani, S.; Saberkari, H. Detection of vertical root fractures in intact and endodontically treated premolar teeth by designing a probabilistic neural network: An ex vivo study. Dentomaxillofac. Radiol. 2017, 46, 20160107. [Google Scholar] [CrossRef] [Green Version]
- Heimer, J.; Thali, M.J.; Ebert, L. Classification based on the presence of skull fractures on curved maximum intensity skull projections by means of deep learning. J. Forensic Radiol. Imaging 2018, 14, 16–20. [Google Scholar] [CrossRef]
- Burns, J.E.; Yao, J.; Summers, R.M. Vertebral body compression fractures and bone density: Automated detection and classification on CT images. Radiology 2017, 284, 788–797. [Google Scholar] [CrossRef] [Green Version]
- Gyftopoulos, S.; Lin, D.; Knoll, F.; Doshi, A.M.; Rodrigues, T.C.; Recht, M.P. Artificial Intelligence in Musculoskeletal Imaging: Current Status and Future Directions. AJR Am. J. Roentgenol. 2019, 213, 506–513. [Google Scholar] [CrossRef]
- Recht, M.; Bryan, R.N. Artificial intelligence: Threat or boon to radiologists? J. Am. Coll. Radiol. 2017, 14, 1476–1480. [Google Scholar] [CrossRef] [PubMed]
- Kabiraj, A.; Meena, T.; Reddy, B.; Roy, S. Detection and Classification of Lung Disease Using Deep Learning Architecture from X-ray Images. In Proceedings of the 17th International Symposium on Visual Computing, San Diego, CA, USA, 3–5 October 2022; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Jha, S.; Topol, E.J. Adapting to artificial intelligence: Radiologists and pathologists as information specialists. JAMA 2016, 316, 2353–2354. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.; Pareek, A.; Ro, D.H.; Lu, Y.; Camp, C.L.; Martin, R.K.; Krych, A.J. Artificial intelligence in orthopedics: Three strategies for deep learning with orthopedic specific imaging. Knee Surg. Sport. Traumatol. Arthrosc. 2022, 30, 758–761. [Google Scholar] [CrossRef] [PubMed]
- Debojyoti, P.; Reddy, P.B.; Roy, S. Attention UW-Net: A fully connected model for automatic segmentation and annotation of chest X-ray. Comput. Biol. Med. 2022, 150, 106083. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Author | Year | Modality | Model/Method | Skeletal Joints | Description | Performance |
|---|---|---|---|---|---|---|---|
| 1 | Kim et al. [30] | 2018 | Xray/MRI | Inception V3 | Wrist | The author proved that the concept of transfer learning from CNNs in fracture detection on radiographs can provide the state of the performance. | AUC = 0.954 Sensitivity = 0.90 Specificity = 0.88 |
| 2 | Olczak et al. [31] | 2017 | Xray/MRI | BVLC Reference CaffeNet network/VGG CNN/Network-in- network/VGG CNN S | Various Parts | Here, the research supports the use of deep learning to outperform the human performance. | Accuracy = 0.83 |
| 3 | Cheng et al. [33] | 2019 | Radiographic images | DenseNet 121 | Hips | The aim of this study was to localise and classify hip fractures using deep learning. | 84 |
| 4 | Chung et al. [32] | 2018 | Radiographic images | ResNet 152 | Humeral | The authors proposed a model for the detection and classification of the fractures from AP shoulder radiographic images. | 0.996 |
| 5 | Urakawa et al. [10] | 2018 | Radiographic images | VGG_16 | Hips | This study shows a comparison of diagnostic performance between CNNs and orthopaedic doctors. | 0.984 |
| 6 | Kitamura et al. [36] | 2019 | Radiographic images | 7 modelsInception V3 ResNet (with/without drop&aux) Xception (with/without drop&aux) Ensemble A Ensemble B | Ankle | The study was done in order to determine the efficiency of CNNs on small datasets. | Best performance by Ensemble_A 81 |
| 7 | Yu [41] | 2020 | Radiographic images | Inception V3 | hip | The proposed algorithm performed well in terms of APFF detection, but not so well in terms of fracture localization. | Accuracy = 96.9 AUC = 0.994 Sensitivity = 97.1 Specificity = 96.7 |
| 8 | Gan [42] | 2019 | Radiographic images | Inception V4 | Wrist | The authors implemented the algorithm for the detection of distal radius fractures. | Accuracy = 93 AUC = 0.961 Sensitivity = 90 Specificity = 96 |
| 9 | Choi [43] | 2019 | Radiographic images | ResNet 50 | Elbow | The authors aimed the development of dual input CNN-based deep learning model for automated detection of supracondylar fracture. | AUC = 0.985 Sensitivity = 93.9 Specificity = 92.2 |
| 10 | Majkowska et al. [44] | 2020 | Radiographic images | Xception | Chest | The authors developed a model to detect opacity, pneumothorax, mass or nodule, and fracture. | 0.86 Sensitivity = 59.9 Specificity = 99.4 |
| 11 | Lindsey et al. [8] | 2018 | Radiographic images | Unet | wrist | This study involves the implementation of deep learning to help doctors to distinguish between fractured and normal wrist. | AUC = 97.5% Sensitivity = 93.9% Specificity = 94.5 |
| 12 | Johari et al. [45] | 2016 | Radiographic images | probabilistic neural network (PNN) CBCT-G1/2/3, PA-G1/2/3 | Vertical Roots | This study supports the initial detection of vertical roots fractures. | Best performance by PNN Model 100 |
| 13 | Heimer et al. [46] | 2018 | CT | deep neural networks. | Skull | The study aims at classification and detection of skull fractures curved maximum intensity projections (CMIP) using deep neural networks. | CMPIs THRESHOLD = 0.79 Specificity= 87.5 Sensitivity =91.4 CMPIs THRESHOLD = 0.75 Specificity= 72.5 Sensitivity =100 |
| 14 | Wang et al. [11] | 2022 | CT | CNN | Mandibule | The author implemented a novel method for the classification and detection of mandibular fracture. | Accuracy = 90% AUC = 0.956 |
| 15 | Rayan et al. [9] | 2021 | Radiographic images | XceptionNet | elbow | This study aims for a binomial classification of acute paediatric elbow radiographic abnormalities. | AUC = 0.95 Accuracy = 88% Sensitivity = 91% Specificity = 84% |
| 16 | Adam et al. [34] | 2019 | Radiographic images | AlexNet and GoogLeNet | femur | Here, the author aimed to evaluate the accuracy of DCNN for the detection of femur fractures. | Accuracy AlexNet = 89.4% GoogLeNet = 94.4% |
| 17 | Balaji et al. [35] | 2019 | x-ray | CNN based model | Diaphyseal Femur | In this study, the author implemented an automated detection and diagnosis of femur fracture. | Accuracy = 90.7% Specificity = 92.3% Sensitivity = 86.6% |
| 18 | Pranata et al. [37] | 2020 | Radiographic images | convolutional neural network (CNN) | Femoral neck | In this study, the author aimed at the detection of femoral neck fracture using genetic and deep learning methods. | Accuracy = 0.793 Specificity = 0.729 Sensitivity = 0.829 |
| 19 | Rahmaniar et al. [26] | 2019 | CT | Computerised system | Calcaneal fractures | Here, the author aims at automated segmentation and detection of calcaneal fractures. | Accuracy = 0.86 |
| 20 | Burns et al. [47] | 2017 | CT | Computerised system | spine | The author implemented a computerized system to detect classify and localize compression fractures. | |
| 21 | Tomita et al. [39] | 2018 | CT | Deep convolutional neural network | vertebra | This study aims at the early detection of osteoporotic vertebral fractures. | Accuracy = 89.2% F1 score = 90.8% |
| 22 | Muehlematter et al. [38] | 2018 | CT | Machine-learning algorithms | vertebra | Here, the author aims at evaluation of the performance of bone texture analysis with a machine learning algorithm. | AUC = 0.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meena, T.; Roy, S. Bone Fracture Detection Using Deep Supervised Learning from Radiological Images: A Paradigm Shift. Diagnostics 2022, 12, 2420. https://doi.org/10.3390/diagnostics12102420
Meena T, Roy S. Bone Fracture Detection Using Deep Supervised Learning from Radiological Images: A Paradigm Shift. Diagnostics. 2022; 12(10):2420. https://doi.org/10.3390/diagnostics12102420
Chicago/Turabian StyleMeena, Tanushree, and Sudipta Roy. 2022. "Bone Fracture Detection Using Deep Supervised Learning from Radiological Images: A Paradigm Shift" Diagnostics 12, no. 10: 2420. https://doi.org/10.3390/diagnostics12102420