
Diagnosis and Treatment of Idiopathic Premature Ventricular Contractions: A Stepwise Approach Based on the Site of Origin

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Prevalence and Mechanism
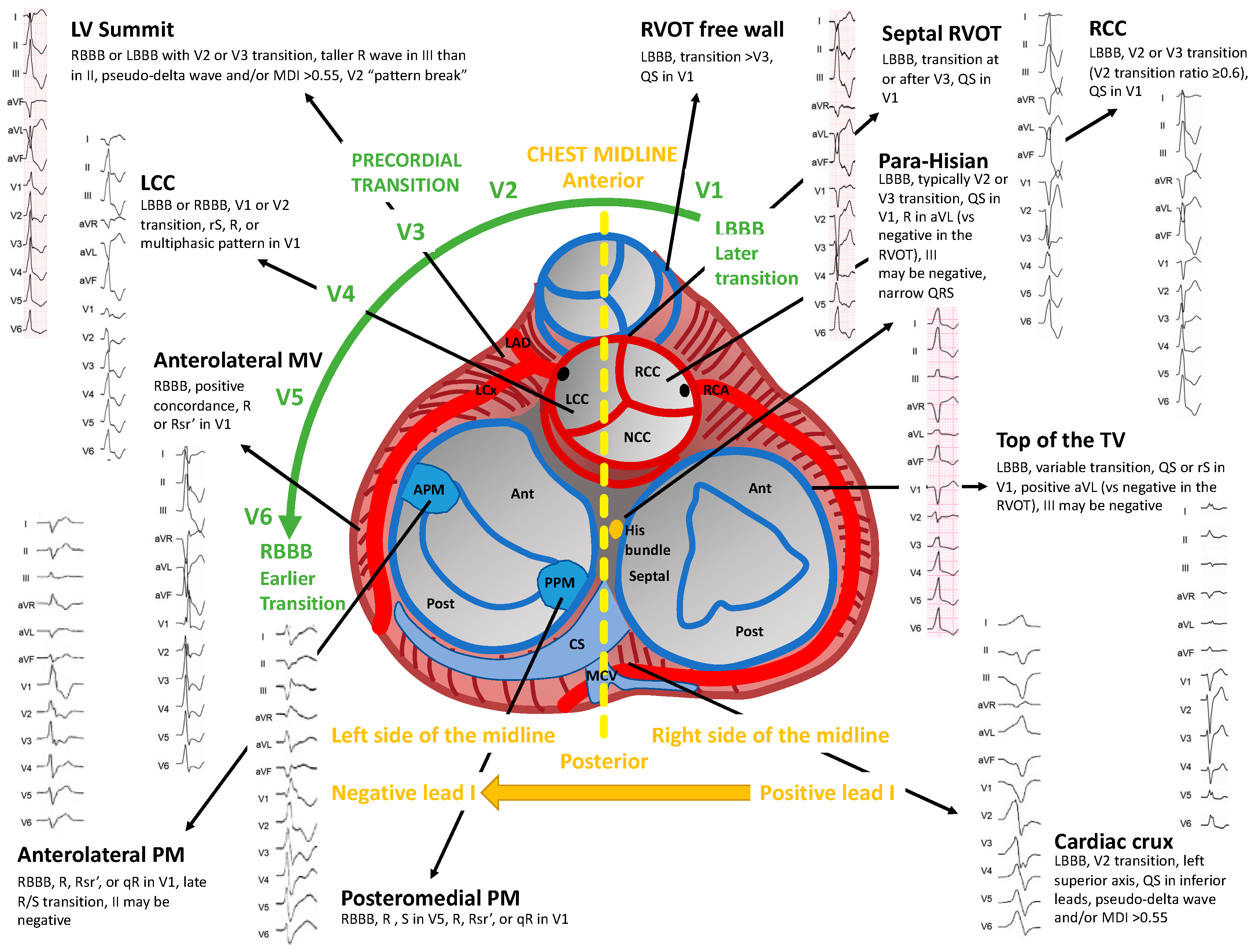
3. Twelve Leads Electrocardiographic Localization of Premature Ventricular Contractions
3.1. Outflow Tract Structures
3.2. Left Ventricular Summit and Intramural Left Ventricular Outflow Tract
3.3. Cardiac Crux
3.4. Mitral and Tricuspid Valve Annuli
3.5. Para-Hisian
3.6. Left and Right Ventricular Papillary Muscles, Moderator Band and Left Bundle Branch Fasciculi
4. Diagnostic Work-Up
5. Prognosis
6. Medical Therapy and Catheter Ablation
7. Future Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Maury, P.; Rollin, A.; Mondoly, P.; Duparc, A. Management of outflow tract ventricular arrhythmias. Curr. Opin. Cardiol. 2015, 30, 50–57. [Google Scholar] [CrossRef]
- LaValle, C.; Mariani, M.V.; Piro, A.; Straito, M.; Severino, P.; Della Rocca, D.; Forleo, G.B.; Romero, J.; Di Biase, L.; Fedele, F. Electrocardiographic features, mapping and ablation of idiopathic outflow tract ventricular arrhythmias. J. Interv. Card. Electrophysiol. 2019, 57, 207–218. [Google Scholar] [CrossRef]
- Latchamsetty, R.; Yokokawa, M.; Morady, F.; Kim, H.M.; Mathew, S.; Tilz, R.; Kuck, K.-H.; Nagashima, K.; Tedrow, U.; Stevenson, W.G.; et al. Multicenter Outcomes for Catheter Ablation of Idiopathic Premature Ventricular Complexes. JACC Clin. Electrophysiol. 2015, 1, 116–123. [Google Scholar] [CrossRef]
- Hayashi, T.; Liang, J.J.; Shirai, Y.; Kuo, L.; Muser, D.; Kubala, M.; Kumareswaran, R.; Arkles, J.S.; Garcia, F.C.; Supple, G.E.; et al. Trends in Successful Ablation Sites and Outcomes of Ablation for Idiopathic Outflow Tract Ventricular Arrhythmias. JACC Clin. Electrophysiol. 2019, 6, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Sadek, M.M.; Benhayon, D.; Sureddi, R.; Chik, W.; Santangeli, P.; Supple, G.E.; Hutchinson, M.D.; Bala, R.; Carballeira, L.; Zado, E.S.; et al. Idiopathic ventricular arrhythmias originating from the moderator band: Electrocardiographic characteristics and treatment by catheter ablation. Heart Rhythm 2015, 12, 67–75. [Google Scholar] [CrossRef]
- Sirichand, S.; Killu, A.M.; Padmanabhan, D.; Hodge, D.O.; Chamberlain, A.M.; Brady, P.A.; Kapa, S.; Noseworthy, P.A.; Packer, D.L.; Munger, T.M.; et al. Incidence of Idiopathic Ventricular Arrhythmias. Circ. Arrhythmia Electrophysiol. 2017, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, Y.; Tada, H.; Ito, S.; Naito, S.; Higuchi, K.; Kumagai, K.; Hachiya, H.; Hirao, K.; Oshima, S.; Taniguchi, K.; et al. Gender and Age Differences in Candidates for Radiofrequency Catheter Ablation of Idiopathic Ventricular Arrhythmias. Circ. J. 2011, 75, 1585–1591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopinathannair, R.; Etheridge, S.P.; Marchlinski, F.E.; Spinale, F.G.; Lakkireddy, D.; Olshansky, B. Arrhythmia-Induced Cardiomyopathies. J. Am. Coll. Cardiol. 2015, 66, 1714–1728. [Google Scholar] [CrossRef] [Green Version]
- Pol, L.C.; Deyell, M.W.; Frankel, D.S.; Benhayon, D.; Squara, F.; Chik, W.; Kohari, M.; Deo, R.; Marchlinski, F.E. Ventricular premature depolarization QRS duration as a new marker of risk for the development of ventricular premature depolarization–induced cardiomyopathy. Heart Rhythm 2014, 11, 299–306. [Google Scholar] [CrossRef]
- Baman, T.S.; Lange, D.C.; Ilg, K.J.; Gupta, S.K.; Liu, T.-Y.; Alguire, C.; Armstrong, W.; Good, E.; Chugh, A.; Jongnarangsin, K.; et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm 2010, 7, 865–869. [Google Scholar] [CrossRef]
- Lerman, B.B. Mechanism, diagnosis, and treatment of outflow tract tachycardia. Nat. Rev. Cardiol. 2015, 12, 597–608. [Google Scholar] [CrossRef]
- Lerman, B.B.; Belardinelli, L.; West, G.A.; Berne, R.M.; DiMarco, J.P. Adenosine-sensitive ventricular tachycardia: Evidence suggesting cyclic AMP-mediated triggered activity. Circulation 1986, 74, 270–280. [Google Scholar] [CrossRef] [Green Version]
- Betensky, B.P.; Park, R.E.; Marchlinski, F.E.; Hutchinson, M.D.; Garcia, F.C.; Dixit, S.; Callans, D.J.; Cooper, J.M.; Bala, R.; Lin, D.; et al. The V2 Transition Ratio: A New Electrocardiographic Criterion for Distinguishing Left From Right Ventricular Outflow Tract Tachycardia Origin. J. Am. Coll. Cardiol. 2011, 57, 2255–2262. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, N.; Yamada, T.; McElderry, H.T.; Inden, Y.; Shimano, M.; Murohara, T.; Kumar, V.; Doppalapudi, H.; Plumb, V.J.; Kay, G.N. A Novel Electrocardiographic Criterion for Differentiating a Left from Right Ventricular Outflow Tract Tachycardia Origin: The V2S/V3R Index. J. Cardiovasc. Electrophysiol. 2014, 25, 747–753. [Google Scholar] [CrossRef]
- Ouyang, F.; Fotuhi, P.; Ho, S.Y.; Hebe, J.; Volkmer, M.; Goya, M.; Burns, M.; Antz, M.; Ernst, S.; Cappato, R.; et al. Repetitive monomorphic ventricular tachycardia originating from the aortic sinus cusp: Electrocardiographic characterization for guiding catheter ablation. J. Am. Coll. Cardiol. 2002, 39, 500–508. [Google Scholar] [CrossRef] [Green Version]
- Cheng, D.; Ju, W.; Zhu, L.; Chen, K.; Zhang, F.; Chen, H.; Yang, G.; Li, X.; Li, M.; Gu, K.; et al. V 3 R/V 7 Index: A Novel Electrocardiographic. Ciriterion for Differentiating Left from Right Ventricular Outflow Tract. Arrhythmias Origins. Circ. Arrhythmia Electrophysiol. 2018, 11, e006243. [Google Scholar] [CrossRef]
- Zhang, F.; Hamon, D.; Fang, Z.; Xu, Y.; Yang, B.; Ju, W.; Bradfield, J.; Shivkumar, K.; Chen, M.; Tung, R. Value of a Posterior Electrocardiographic Lead for Localization of Ventricular Outflow Tract Arrhythmias. JACC Clin. Electrophysiol. 2017, 3, 678–686. [Google Scholar] [CrossRef]
- Lin, D.; Ilkhanoff, L.; Gerstenfeld, E.; Dixit, S.; Beldner, S.; Bala, R.; Garcia, F.; Callans, D.; Marchlinski, F. Twelve-lead electrocardiographic characteristics of the aortic cusp region guided by intracardiac echocardiography and electroanatomic mapping. Heart Rhythm 2008, 5, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Bala, R.; Garcia, F.C.; Hutchinson, M.; Gerstenfeld, E.P.; Dhruvakumar, S.; Dixit, S.; Cooper, J.M.; Lin, D.; Harding, J.; Riley, M.P.; et al. Electrocardiographic and electrophysiologic features of ventricular arrhythmias originating from the right/left coronary cusp commissure. Heart Rhythm 2010, 7, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Dixit, S.; Gerstenfeld, E.P.; Lin, D.; Callans, D.J.; Hsia, H.H.; Nayak, H.M.; Zado, E.; Marchlinski, F.E. Identification of distinct electrocardiographic patterns from the basal left ventricle: Distinguishing medial and lateral sites of origin in patients with idiopathic ventricular tachycardia. Heart Rhythm 2005, 2, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Enriquez, A.; Malavassi, F.; Saenz, L.C.; Supple, G.; Santangeli, P.; Marchlinski, F.E.; Garcia, F.C. How to map and ablate left ventricular summit arrhythmias. Heart Rhythm 2016, 14, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santangeli, P.; Marchlinski, F.E.; Zado, E.S.; Benhayon, D.; Hutchinson, M.D.; Lin, D.; Frankel, D.S.; Riley, M.P.; Supple, G.E.; Garcia, F.C.; et al. Percutaneous Epicardial Ablation of Ventricular Arrhythmias Arising From the Left Ventricular Summit. Circ. Arrhythmia Electrophysiol. 2015, 8, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abularach, M.E.J.; Campos, B.; Park, K.-M.; Tschabrunn, C.; Frankel, D.S.; Park, R.E.; Gerstenfeld, E.P.; Mountantonakis, S.; Garcia, F.C.; Dixit, S.; et al. Ablation of ventricular arrhythmias arising near the anterior epicardial veins from the left sinus of Valsalva region: ECG features, anatomic distance, and outcome. Heart Rhythm 2012, 9, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Santangeli, P.; Pathak, R.K.; Muser, D.; Liang, J.J.; Castro, S.A.; Garcia, F.C.; Hutchinson, M.D.; Supple, G.E.; Frankel, D.S.; et al. Outcomes of Catheter Ablation of Idiopathic Outflow Tract Ventricular Arrhythmias With an R Wave Pattern Break in Lead V2: A Distinct Clinical Entity. J. Cardiovasc. Electrophysiol. 2017, 28, 504–514. [Google Scholar] [CrossRef]
- Yamada, T.; McElderry, H.T.; Doppalapudi, H.; Okada, T.; Murakami, Y.; Yoshida, Y.; Yoshida, N.; Inden, Y.; Murohara, T.; Plumb, V.J.; et al. Idiopathic Ventricular Arrhythmias Originating From the Left Ventricular Summit. Circ. Arrhythmia Electrophysiol. 2010, 3, 616–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazan, V.; Gerstenfeld, E.P.; Garcia, F.C.; Bala, R.; Rivas, N.; Dixit, S.; Zado, E.; Callans, D.J.; Marchlinski, F.E. Site-specific twelve-lead ECG features to identify an epicardial origin for left ventricular tachycardia in the absence of myocardial infarction. Heart Rhythm 2007, 4, 1403–1410. [Google Scholar] [CrossRef]
- Berruezo, A.; Mont, L.; Nava, S.; Chueca, E.; Bartholomay, E.; Brugada, J. Electrocardiographic Recognition of the Epicardial Origin of Ventricular Tachycardias. Circulation 2004, 109, 1842–1847. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, M.; Gerstenfeld, E.P.; Vedantham, V.; Rodrigues, D.M.; Burkhardt, J.D.; Kobayashi, Y.; Hsia, H.H.; Marcus, G.M.; Marchlinski, F.E.; Scheinman, M.M.; et al. Idiopathic Ventricular Arrhythmia Originating From the Cardiac Crux or Inferior Septum. Circ. Arrhythmia Electrophysiol. 2014, 7, 1152–1158. [Google Scholar] [CrossRef] [Green Version]
- Tada, H.; Ito, S.; Naito, S.; Kurosaki, K.; Kubota, S.; Sugiyasu, A.; Tsuchiya, T.; Miyaji, K.; Yamada, M.; Kutsumi, Y.; et al. Idiopathic ventricular arrhythmia arising from the mitral annulus: A distinct subgroup of idiopathic ventricular arrhythmias. J. Am. Coll. Cardiol. 2005, 45, 877–886. [Google Scholar] [CrossRef] [Green Version]
- Tada, H.; Tadokoro, K.; Ito, S.; Naito, S.; Hashimoto, T.; Kaseno, K.; Miyaji, K.; Sugiyasu, A.; Tsuchiya, T.; Kutsumi, Y.; et al. Idiopathic ventricular arrhythmias originating from the tricuspid annulus: Prevalence, electrocardiographic characteristics, and results of radiofrequency catheter ablation. Heart Rhythm 2007, 4, 7–16. [Google Scholar] [CrossRef]
- Yamauchi, Y.; Aonuma, K.; Takahashi, A.; Sekiguchi, Y.; Hachiya, H.; Yokoyama, Y.; Kumagai, K.; Nogami, A.; Iesaka, Y.; Isobe, M. Electrocardiographic Characteristics of Repetitive Monomorphic Right Ventricular Tachycardia Originating Near the His-Bundle. J. Cardiovasc. Electrophysiol. 2005, 16, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Enriquez, A.; Supple, G.E.; Marchlinski, F.E.; Garcia, F.C. How to map and ablate papillary muscle ventricular arrhythmias. Heart Rhythm 2017, 14, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Enriquez, A.; Pathak, R.K.; Santangeli, P.; Liang, J.J.; Al Rawahi, M.; Hayashi, T.; Muser, D.; Frankel, D.S.; Supple, G.; Schaller, R.; et al. Inferior lead discordance in ventricular arrhythmias: A specific marker for certain arrhythmia locations. J. Cardiovasc. Electrophysiol. 2017, 28, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Crawford, T.; Mueller, G.; Good, E.; Jongnarangsin, K.; Chugh, A.; Pelosi, F.; Ebinger, M.; Oral, H.; Morady, F.; Bogun, F. Ventricular arrhythmias originating from papillary muscles in the right ventricle. Heart Rhythm 2010, 7, 725–730. [Google Scholar] [CrossRef]
- Jouven, X.; Zureik, M.; Desnos, M.; Courbon, D.; Ducimetière, P. Long-Term Outcome in Asymptomatic Men with Exercise-Induced Premature Ventricular Depolarizations. N. Engl. J. Med. 2000, 343, 826–833. [Google Scholar] [CrossRef]
- Frolkis, J.P.; Pothier, C.E.; Blackstone, E.H.; Lauer, M.S. Frequent Ventricular Ectopy after Exercise as a Predictor of Death. N. Engl. J. Med. 2003, 348, 781–790. [Google Scholar] [CrossRef] [Green Version]
- Marcus, G.M. Evaluation and Management of Premature Ventricular Complexes. Circulation 2020, 141, 1404–1418. [Google Scholar] [CrossRef]
- Sassone, B.; Muser, D.; Casella, M.; Luzi, M.; Virzì, S.; Balla, C.; Nucifora, G. For the Task Force on Imaging and Task Force on Ablation of Ventricular Tachycardia of the Italian Association of Arrhythmias and Cardiac Pacing (AIAC) Detection of concealed structural heart disease by imaging in patients with apparently idiopathic premature ventricular complexes: A review of current literature. Clin. Cardiol. 2019, 42, 1162–1169. [Google Scholar] [CrossRef] [Green Version]
- Yokokawa, M.; Kim, H.M.; Good, E.; Chugh, A.; Pelosi, F.; Alguire, C.; Armstrong, W.; Crawford, T.; Jongnarangsin, K.; Oral, H.; et al. Relation of symptoms and symptom duration to premature ventricular complex–induced cardiomyopathy. Heart Rhythm 2012, 9, 92–95. [Google Scholar] [CrossRef]
- Latchamsetty, R.; Bogun, F. Premature Ventricular Complexes and Premature Ventricular Complex Induced Cardiomyopathy. Curr. Probl. Cardiol. 2015, 40, 379–422. [Google Scholar] [CrossRef]
- Bogun, F.; Crawford, T.; Reich, S.; Koelling, T.M.; Armstrong, W.; Good, E.; Jongnarangsin, K.; Marine, J.E.; Chugh, A.; Pelosi, F.; et al. Radiofrequency ablation of frequent, idiopathic premature ventricular complexes: Comparison with a control group without intervention. Heart Rhythm 2007, 4, 863–867. [Google Scholar] [CrossRef]
- Marcus, F.I.; McKenna, W.J.; Sherrill, D.; Basso, C.; Bauce, B.; Bluemke, D.; Calkins, H.; Corrado, D.; Cox, M.G.; Daubert, J.P.; et al. Diagnosis of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia. Circulation 2010, 121, 1533–1541. [Google Scholar] [CrossRef] [PubMed]
- Fogante, M.; Agliata, G.; Basile, M.; Compagnucci, P.; Volpato, G.; Falanga, U.; Stronati, G.; Guerra, F.; Vignale, D.; Esposito, A.; et al. Cardiac Imaging in Athlete’s Heart: The Role of the Radiologist. Medicina 2021, 57, 455. [Google Scholar] [CrossRef]
- Compagnucci, P.; Volpato, G.; Falanga, U.; Cipolletta, L.; Conti, M.; Grifoni, G.; Ciliberti, G.; Stronati, G.; Fogante, M.; Bergonti, M.; et al. Myocardial Inflammation, Sports Practice, and Sudden Cardiac Death: 2021 Update. Medicina 2021, 57, 277. [Google Scholar] [CrossRef]
- Priori, S.; Blomström-Lundqvist, C.; Mazzanti, A.; A Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Ar-rhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [CrossRef] [Green Version]
- Ciliberti, G.; Compagnucci, P.; Urbinati, A.; Bianco, F.; Stronati, G.; Lattanzi, S.; Russo, A.D.; Guerra, F. Myocardial Infarction Without Obstructive Coronary Artery Disease (MINOCA): A Practical Guide for Clinicians. Curr. Probl. Cardiol. 2020, 46, 100761. [Google Scholar] [CrossRef]
- Jeserich, M.; Friedrich, M.G.; Olschewski, M.; Kirchberger, J.; Kimmel, S.; Bode, C.; Geibel, A. Evidence for non-ischemic scarring in patients with ventricular ectopy. Int. J. Cardiol. 2011, 147, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Mavrogeni, S.; Anastasakis, A.; Sfendouraki, E.; Gialafos, E.; Aggeli, C.; Stefanadis, C.; Kolovou, G. Ventricular tachycardia in patients with family history of sudden cardiac death, normal coronaries and normal ventricular function. Can cardiac magnetic resonance add to diagnosis? Int. J. Cardiol. 2013, 168, 1532–1533. [Google Scholar] [CrossRef]
- Nucifora, G.; Muser, D.; Masci, P.G.; Barison, A.; Rebellato, L.; Piccoli, G.; Daleffe, E.; Toniolo, M.; Zanuttini, D.; Facchin, D.; et al. Prevalence and Prognostic Value of Concealed Structural Abnormalities in Patients With Apparently Idiopathic Ventricular Arrhythmias of Left Versus Right Ventricular Origin. Circ. Arrhythmia Electrophysiol. 2014, 7, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muser, D.; Santangeli, P.; Castro, S.A.; Arroyo, R.C.; Maeda, S.; Benhayon, D.A.; Liuba, I.; Liang, J.J.; Sadek, M.M.; Chahal, A.; et al. Risk Stratification of Patients With Apparently Idiopathic Premature Ventricular Contractions. JACC Clin. Electrophysiol. 2019, 6, 722–735. [Google Scholar] [CrossRef]
- Oebel, S.; Dinov, B.; Arya, A.; Hilbert, S.; Sommer, P.; Bollmann, A.; Hindricks, G.; Paetsch, I.; Jahnke, C. ECG morphology of premature ventricular contractions predicts the presence of myocardial fibrotic substrate on cardiac magnetic resonance imaging in patients undergoing ablation. J. Cardiovasc. Electrophysiol. 2017, 28, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Ghannam, M.; Siontis, K.C.; Kim, H.M.; Cochet, H.; Jais, P.; Eng, M.J.; Attili, A.; Sharaf-Dabbagh, G.; Latchamsetty, R.; Jongnarangsin, K.; et al. Factors predictive for delayed enhancement in cardiac resonance imaging in patients undergoing catheter ablation of premature ventricular complexes. Heart Rhythm O2 2020, 2, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; Pingitore, A.; Strata, E.; Di Bella, G.; Molinaro, S.; Lombardi, M. Cardiac Magnetic Resonance Predicts Outcome in Patients With Premature Ventricular Complexes of Left Bundle Branch Block Morphology. J. Am. Coll. Cardiol. 2010, 56, 1235–1243. [Google Scholar] [CrossRef] [Green Version]
- Muser, D.; Nucifora, G.; Pieroni, M.; Castro, S.A.; Arroyo, R.C.; Maeda, S.; Benhayon, D.A.; Liuba, I.; Sadek, M.; Magnani, S.; et al. Prognostic Value of Non-Ischemic Ring-Like Left Ventricular Scar in Patients with Apparently Idiopathic Non-Sustained Ventricular Arrhythmias. Circulation 2021. [Google Scholar] [CrossRef] [PubMed]
- Ghannam, M.; Siontis, K.C.; Kim, M.H.; Cochet, H.; Jais, P.; Eng, M.J.; Attili, A.; Sharaf-Dabbagh, G.; Latchamsetty, R.; Jongnarangsin, K.; et al. Risk stratification in patients with frequent premature ventricular complexes in the absence of known heart disease. Heart Rhythm 2019, 17, 423–430. [Google Scholar] [CrossRef]
- Nikolaidou, C.; Kouskouras, K.; Fragakis, N.; Vassilikos, V.; Karvounis, H.; Karamitsos, T. Bolus Intravenous Procainamide in Patients with Frequent Ventricular Ectopics during Cardiac Magnetic Resonance Scanning: A Way to Ensure High Quality Imaging. Diagnostics 2021, 11, 178. [Google Scholar] [CrossRef] [PubMed]
- Muser, D.; Santangeli, P.; Nucifora, G. Procainamide for the Rapid Suppression of Premature Ventricular Contractions: An (Almost) Forgotten Tool in the Cardiologist’s Armamentarium. Diagnostics 2021, 11, 357. [Google Scholar] [CrossRef]
- Compagnucci, P.; Volpato, G.; Falanga, U.; Cipolletta, L.; Conti, M.; Grifoni, G.; Verticelli, L.; Schicchi, N.; Giovagnoni, A.; Casella, M.; et al. Recent advances in three-dimensional electroanatomical mapping guidance for the ablation of complex atrial and ventricular arrhythmias. J. Interv. Card. Electrophysiol. 2020, 61, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Bergonti, M.; Russo, A.D.; Sicuso, R.; Ribatti, V.; Compagnucci, P.; Catto, V.; Gasperetti, A.; Zucchetti, M.; Cellucci, S.; Vettor, G.; et al. Long-Term Outcomes of Near-Zero Radiation Ablation of Paroxysmal Supraventricular Tachycardia. JACC Clin. Electrophysiol. 2021, 7, 1108–1117. [Google Scholar] [CrossRef]
- Santangeli, P.; Hamilton-Craig, C.; Russo, A.D.; Pieroni, M.; Casella, M.; Pelargonio, G.; Biase, L.D.; Smaldone, C.; Bartoletti, S.; Narducci, M.L.; et al. Imaging of Scar in Patients with Ventricular Arrhythmias of Right Ventricular Origin: Cardiac Magnetic Resonance Versus Electroanatomic Mapping. J. Cardiovasc. Electrophysiol. 2011, 22, 1359–1366. [Google Scholar] [CrossRef]
- Castro, S.A.; Pathak, R.K.; Muser, D.; Santangeli, P.; Owens, A.; Marchlinski, F.; Garcia, F.C. Incremental value of electroanatomical mapping for the diagnosis of arrhythmogenic right ventricular cardiomyopathy in a patient with sustained ventricular tachycardia. HeartRhythm Case Rep. 2016, 2, 469–472. [Google Scholar] [CrossRef] [Green Version]
- Bergonti, M.; Casella, M.; Compagnucci, P.; Russo, A.D.; Tondo, C. Electroanatomic Mapping System and Intracardiac-Echo to Guide Endomyocardial Biopsy. Card. Electrophysiol. Clin. 2021, 13, 381–392. [Google Scholar] [CrossRef]
- Muser, D.; Santangeli, P.; Liang, J.J.; Castro, S.A.; Magnani, S.; Hayashi, T.; Garcia, F.C.; Frankel, D.S.; Dixit, S.; Zado, E.S.; et al. Characterization of the Electroanatomic Substrate in Cardiac Sarcoidosis. JACC Clin. Electrophysiol. 2017, 4, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, H.L.; Whitlock, J.A.; Sprague, M.K.; Kennedy, L.J.; Buckingham, T.A.; Goldberg, R.J. Long-Term Follow-up of Asymptomatic Healthy Subjects with Frequent and Complex Ventricular Ectopy. N. Engl. J. Med. 1985, 312, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Davis, H.T.; DeCamilla, J.; Bayer, L.W. Ventricular ectopic beats and their relation to sudden and nonsudden cardiac death after myocardial infarction. Circulation 1979, 60, 998–1003. [Google Scholar] [CrossRef] [Green Version]
- Dukes, J.W.; Dewland, T.A.; Vittinghoff, E.; Mandyam, M.C.; Heckbert, S.R.; Siscovick, D.S.; Stein, P.K.; Psaty, B.M.; Sotoodehnia, N.; Gottdiener, J.S.; et al. Ventricular Ectopy as a Predictor of Heart Failure and Death. J. Am. Coll. Cardiol. 2015, 66, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, V.; Hemingway, H.; Harb, R.; Crake, T.; Lambiase, P. The prognostic significance of premature ventricular complexes in adults without clinically apparent heart disease: A meta-analysis and systematic review. Heart 2012, 98, 1290–1298. [Google Scholar] [CrossRef] [PubMed]
- Ataklte, F.; Erqou, S.; Laukkanen, J.; Kaptoge, S. Meta-Analysis of Ventricular Premature Complexes and Their Relation to Cardiac Mortality in General Populations. Am. J. Cardiol. 2013, 112, 1263–1270. [Google Scholar] [CrossRef]
- Yokokawa, M.; Siontis, K.C.; Kim, H.M.; Stojanovska, J.; Latchamsetty, R.; Crawford, T.; Jongnarangsin, K.; Ghanbari, H.; Cunnane, R.; Chugh, A.; et al. Value of cardiac magnetic resonance imaging and programmed ventricular stimulation in patients with frequent premature ventricular complexes undergoing radiofrequency ablation. Heart Rhythm 2017, 14, 1695–1701. [Google Scholar] [CrossRef]
- Niwano, S.; Wakisaka, Y.; Niwano, H.; Fukaya, H.; Kurokawa, S.; Kiryu, M.; Hatakeyama, Y.; Izumi, T. Prognostic significance of frequent premature ventricular contractions originating from the ventricular outflow tract in patients with normal left ventricular function. Heart 2009, 95, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- The Cardiac Arrhythmia Suppression Trial (CAST) Investigators Preliminary Report: Effect of Encainide and Flecainide on Mortality in a Randomized Trial of Arrhythmia Suppression after Myocardial Infarction. N. Engl. J. Med. 1989, 321, 406–412. [CrossRef]
- Singh, S.N.; Fletcher, R.D.; Fisher, S.G.; Singh, B.N.; Lewis, H.D.; Deedwania, P.C.; Massie, B.M.; Colling, C.; Lazzeri, D. Amiodarone in Patients with Congestive Heart Failure and Asymptomatic Ventricular Arrhythmia. N. Engl. J. Med. 1995, 333, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Noda, T.; Shimizu, W.; Taguchi, A.; Aiba, T.; Satomi, K.; Suyama, K.; Kurita, T.; Aihara, N.; Kamakura, S. Malignant Entity of Idiopathic Ventricular Fibrillation and Polymorphic Ventricular Tachycardia Initiated by Premature Extrasystoles Originating From the Right Ventricular Outflow Tract. J. Am. Coll. Cardiol. 2005, 46, 1288–1294. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, C.T.; Kay, G.N.; Kalman, J.; Borggrefe, M.; Della-Bella, P.; Dickfeld, T.; Dorian, P.; Huikuri, H.; Kim, Y.-H.; Knight, B.; et al. EHRA/HRS/APHRS Expert Consensus on Ventricular Arrhythmias. Heart Rhythm 2014, 11, e166–e196. [Google Scholar] [CrossRef] [PubMed]
- Krittayaphong, R.; Bhuripanyo, K.; Punlee, K.; Kangkagate, C.; Chaithiraphan, S. Effect of atenolol on symptomatic ventricular arrhythmia without structural heart disease: A randomized placebo-controlled study. Am. Heart J. 2002, 144, 1–5. [Google Scholar] [CrossRef]
- Belhassen, B.; Horowitz, L.N. Use of intravenous verapamil for ventricular tachycardia. Am. J. Cardiol. 1984, 54, 1131–1133. [Google Scholar] [CrossRef]
- Zhong, L.; Lee, Y.-H.; Huang, X.-M.; Asirvatham, S.J.; Shen, W.-K.; Friedman, P.A.; Hodge, D.O.; Slusser, J.P.; Song, Z.-Y.; Packer, D.L.; et al. Relative efficacy of catheter ablation vs antiarrhythmic drugs in treating premature ventricular contractions: A single-center retrospective study. Heart Rhythm 2014, 11, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Stec, S.; Sikorska, A.; Zaborska, B.; Kryński, T.; Szymot, J.; Kułakowski, P. Benign symptomatic premature ventricular com-plexes: Short- and long-term efficacy of antiarrhythmic drugs and radiofrequency ablation. Kardiol Pol. 2012, 70, 351–358. [Google Scholar]
- Capucci, A.; Di Pasquale, G.; Boriani, G.; Carini, G.; Balducelli, M.; Frabetti, L.; Carozzi, A.; Finzi, A.; Pinelli, G.; Magnani, B. A double-blind crossover comparison of flecainide and slow-release mexiletine in the treatment of stable premature ventricular complexes. Int. J. Clin. Pharmacol. Res. 1991, 11, 23–33. [Google Scholar]
- Anderson, J.L.; Askins, J.C.; Gilbert, E.M.; Miller, R.H.; Keefe, D.L.; Somberg, J.C.; Freedman, R.A.; Haft, L.R.; Mason, J.W.; Lessem, J.N. Multicenter trial of sotalol for suppression of frequent, complex ventricular arrhythmias: A double-blind, randomized, placebo-controlled evaluation of two doses. J. Am. Coll. Cardiol. 1986, 8, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Hyman, M.C.; Mustin, D.; Supple, G.; Schaller, R.D.; Santangeli, P.; Arkles, J.; Lin, D.; Muser, D.; Dixit, S.; Nazarian, S.; et al. Class IC antiarrhythmic drugs for suspected premature ventricular contraction–induced cardiomyopathy. Heart Rhythm 2018, 15, 159–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cronin, E.; Bogun, F.M.; Maury, P.; Peichl, P.; Chen, M.; Namboodiri, N.; Aguinaga, L.; Leite, L.R.; Al-Khatib, S.M.; Anter, E.; et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias: Executive summary. Heart Rhythm 2019, 17, e155–e205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakkireddy, D.; Di Biase, L.; Ryschon, K.; Biria, M.; Swarup, V.; Reddy, Y.M.; Verma, A.; Bommana, S.; Burkhardt, D.; Dendi, R.; et al. Radiofrequency Ablation of Premature Ventricular Ectopy Improves the Efficacy of Cardiac Resynchronization Therapy in Nonresponders. J. Am. Coll. Cardiol. 2012, 60, 1531–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, Z.; Liu, Z.; Su, L.; Zipunnikov, V.; Wu, J.; Du, H.; Woo, K.; Chen, S.; Zhong, B.; Lan, X.; et al. Radiofrequency Ablation Versus Antiarrhythmic Medication for Treatment of Ventricular Premature Beats From the Right Ventricular Outflow Tract. Circ. Arrhythmia Electrophysiol. 2014, 7, 237–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Yang, B.; Chen, H.; Ju, W.; Kojodjojo, P.; Cao, K.; Chen, M. Magnetic versus manual catheter navigation for mapping and ablation of right ventricular outflow tract ventricular arrhythmias: A randomized controlled study. Heart Rhythm 2013, 10, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Haïssaguerre, M.; Shoda, M.; Jaïs, P.; Nogami, A.; Shah, D.C.; Kautzner, J.; Arentz, T.; Kalushe, D.; Lamaison, D.; Griffith, M.; et al. Mapping and Ablation of Idiopathic Ventricular Fibrillation. Circulation 2002, 106, 962–967. [Google Scholar] [CrossRef]
- Yamada, T.; Yoshida, N.; Itoh, T.; Litovsky, S.H.; Doppalapudi, H.; McElderry, H.T.; Kay, G.N. Idiopathic Ventricular Arrhythmias Originating From the Parietal Band. Circ. Arrhythmia Electrophysiol. 2017, 10. [Google Scholar] [CrossRef]
- Yue-Chun, L.; Wen-Wu, Z.; Na-Dan, Z.; Teng, Z.; Pin-Xiao, W.; Bei, G.; Jia, L.; Kang-Ting, J.; Jia-Feng, L. Idiopathic premature ventricular contractions and ventricular tachycardias originating from the vicinity of tricuspid annulus: Results of radiofrequency catheter ablation in thirty-five patients. BMC Cardiovasc. Disord. 2012, 12, 32. [Google Scholar] [CrossRef] [Green Version]
- Kumagai, K.; Fukuda, K.; Wakayama, Y.; Sugai, Y.; Hirose, M.; Yamaguchi, N.; Takase, K.; Yamauchi, Y.; Takahashi, A.; Aonuma, K.; et al. Electrocardiographic Characteristics of the Variants of Idiopathic Left Ventricular Outflow Tract Ventricular Tachyarrhythmias. J. Cardiovasc. Electrophysiol. 2008, 19, 495–501. [Google Scholar] [CrossRef]
- Yamada, T.; McElderry, H.T.; Okada, T.; Murakami, Y.; Inden, Y.; Doppalapudi, H.; Yoshida, N.; Tabereaux, P.B.; Allred, J.D.; Murohara, T.; et al. Idiopathic Focal Ventricular Arrhythmias Originating from the Anterior Papillary Muscle in the Left Ventricle. J. Cardiovasc. Electrophysiol. 2009, 20, 866–872. [Google Scholar] [CrossRef]
- Yamada, T.; Doppalapudi, H.; McElderry, H.T.; Okada, T.; Murakami, Y.; Inden, Y.; Yoshida, Y.; Yoshida, N.; Murohara, T.; Epstein, A.E.; et al. Electrocardiographic and Electrophysiological Characteristics in Idiopathic Ventricular Arrhythmias Originating From the Papillary Muscles in the Left Ventricle. Circ. Arrhythmia Electrophysiol. 2010, 3, 324–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, K.; Kapa, S.; Mulpuru, S.K.; Deshmukh, A.J.; Asirvatham, S.J.; Munger, T.M.; Friedman, P.A.; Packer, D.L. Safety and Efficacy of Cryoablation in Patients With Ventricular Arrhythmias Originating From the Para-Hisian Region. JACC Clin. Electrophysiol. 2018, 4, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Muser, D.; Santangeli, P. Epicardial Ablation of Idiopathic Ventricular Tachycardia. Card. Electrophysiol. Clin. 2020, 12, 295–312. [Google Scholar] [CrossRef] [PubMed]
- Enriquez, A.; Baranchuk, A.; Briceno, D.; Saenz, L.; Garcia, F. How to use the 12-lead ECG to predict the site of origin of idiopathic ventricular arrhythmias. Heart Rhythm 2019, 16, 1538–1544. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Site of Origin | Acute Procedural Success Rate, % | Complications, % Pericardial Effusion (40%) Thromboembolism (3%) Vascular Access Complications (8%) Coronary Arteries Injury (5%) |
|---|---|---|
| RVOT (60%) | 97% | <1% |
| LVOT (10%) | 94% | 5% |
| LV summit (3%) | 70% | 5% |
| Right Ventricle intracavitary structures (14%) | 93% | 1% |
| Left Ventricle intracavitary structures (10%) | 91% | 9% |
| Mitral and Tricuspid Annular Region (5–10%) | 90% | 3% |
| Left bundle fascicles (10%) | 90% | 3% |
| Epicardial Foci (3–5%) | 80% | 8% |
| Imaging Test | Indications | Advantages | Limitations |
|---|---|---|---|
| Echocardiogram | Potentially indicated in each patient presenting PVCs; may be omitted in asymptomatic healthy subjects with low PVC burden and no family history of SCD |
|
|
| Cardiac magnetic resonance imaging |
|
|
|
| Computed tomographic coronary angiography |
|
|
|
| Invasive coronary angiography |
|
|
|
| Electroanatomical mapping |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muser, D.; Tritto, M.; Mariani, M.V.; Di Monaco, A.; Compagnucci, P.; Accogli, M.; De Ponti, R.; Guarracini, F. Diagnosis and Treatment of Idiopathic Premature Ventricular Contractions: A Stepwise Approach Based on the Site of Origin. Diagnostics 2021, 11, 1840. https://doi.org/10.3390/diagnostics11101840
Muser D, Tritto M, Mariani MV, Di Monaco A, Compagnucci P, Accogli M, De Ponti R, Guarracini F. Diagnosis and Treatment of Idiopathic Premature Ventricular Contractions: A Stepwise Approach Based on the Site of Origin. Diagnostics. 2021; 11(10):1840. https://doi.org/10.3390/diagnostics11101840
Chicago/Turabian StyleMuser, Daniele, Massimo Tritto, Marco Valerio Mariani, Antonio Di Monaco, Paolo Compagnucci, Michele Accogli, Roberto De Ponti, and Fabrizio Guarracini. 2021. "Diagnosis and Treatment of Idiopathic Premature Ventricular Contractions: A Stepwise Approach Based on the Site of Origin" Diagnostics 11, no. 10: 1840. https://doi.org/10.3390/diagnostics11101840