Efficient Pneumonia Detection in Chest Xray Images Using Deep Transfer Learning

 ,
,  and
and
Abstract
:1. Introduction
2. Related Work
3. Background of Deep Learning Methods
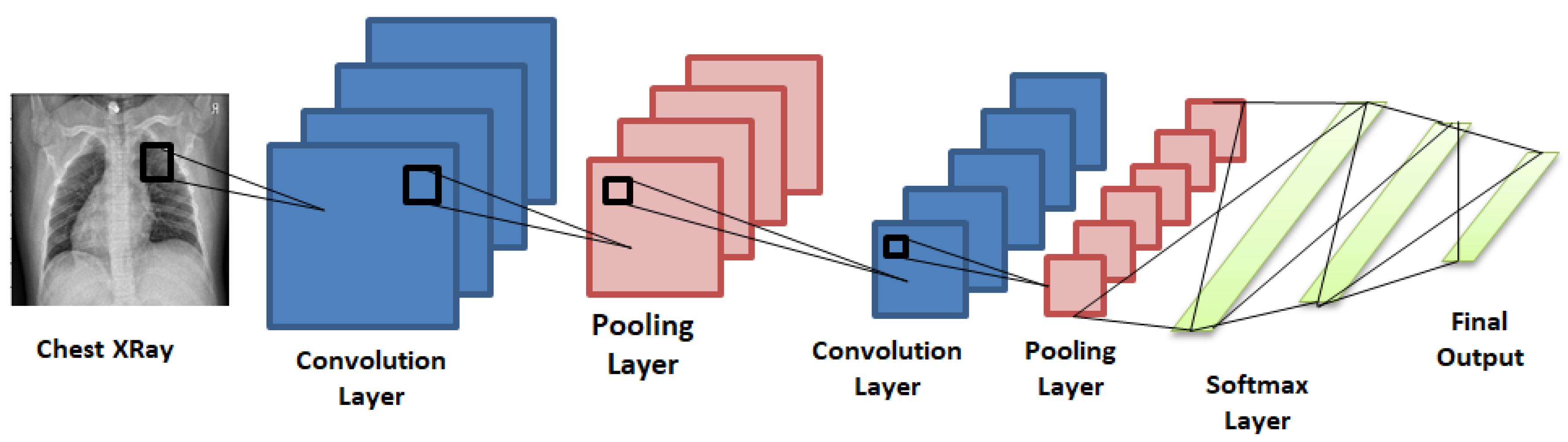
3.1. Convolutional Neural Network
3.2. Transfer Learning
3.3. Pre-Trained Neural Networks
3.4. Performance Metrics for Classification
- Accuracy: It tells us how close the measured value is to a known value.
- Precision: It tells about how accurate the model is in terms of those which were predicted positive.
- Recall: It calculates the number of actual positives the model was able to capture after labeling it as positive (true positive).
- F1: It gives a balance between precision and recall.
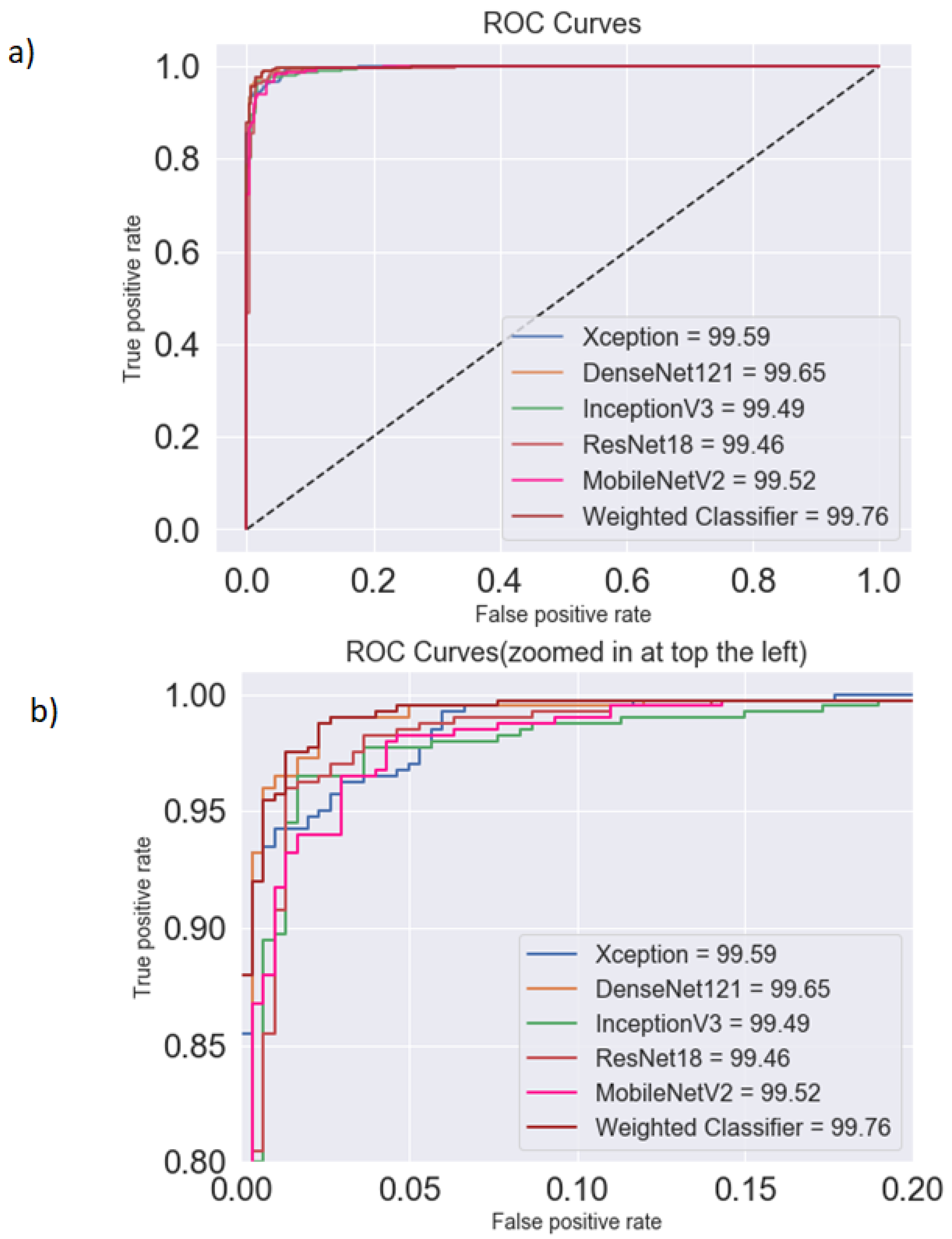
- AUC Score and ROC Curve: ROC (receiver operating characteristics) is a probability curve, and AUC (area under curve) represents the degree of separability. The ROC curve is the plot of sensitivity (true positive rate) against specificity (false positive rate).
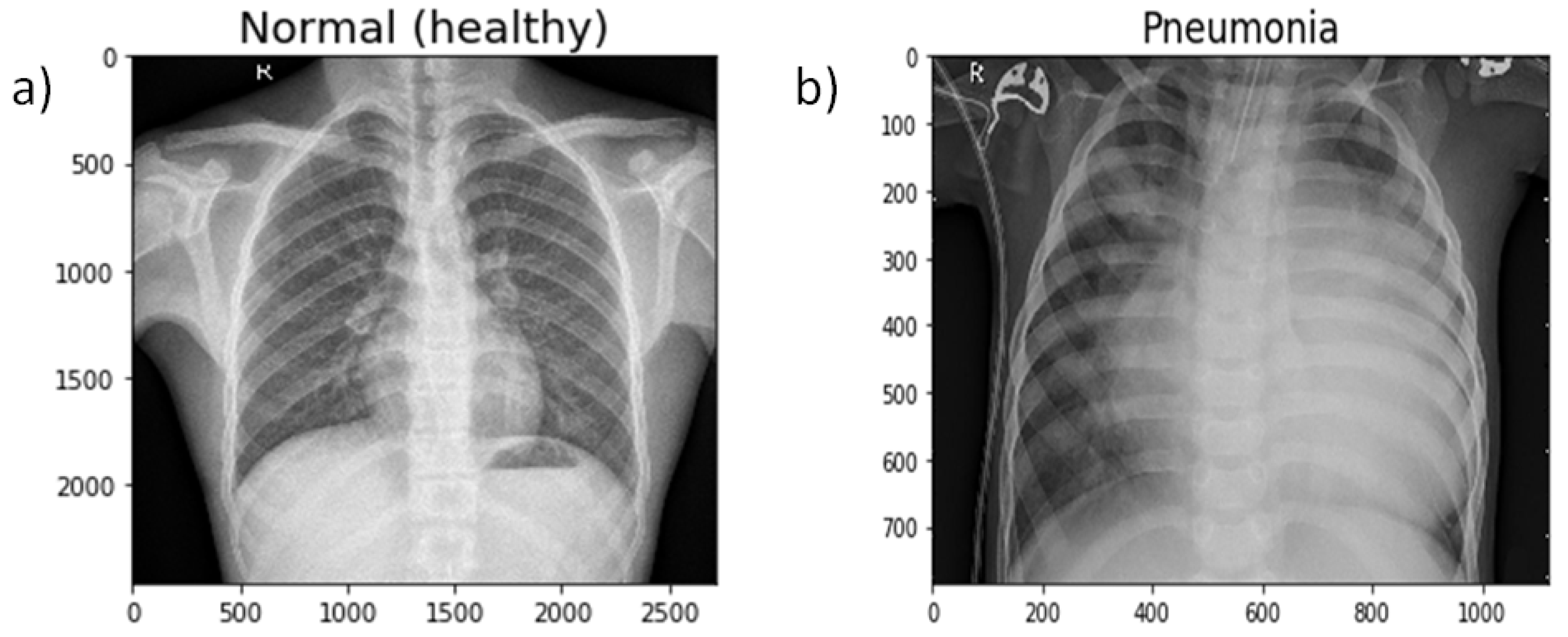
4. Materials
Experimental Dataset
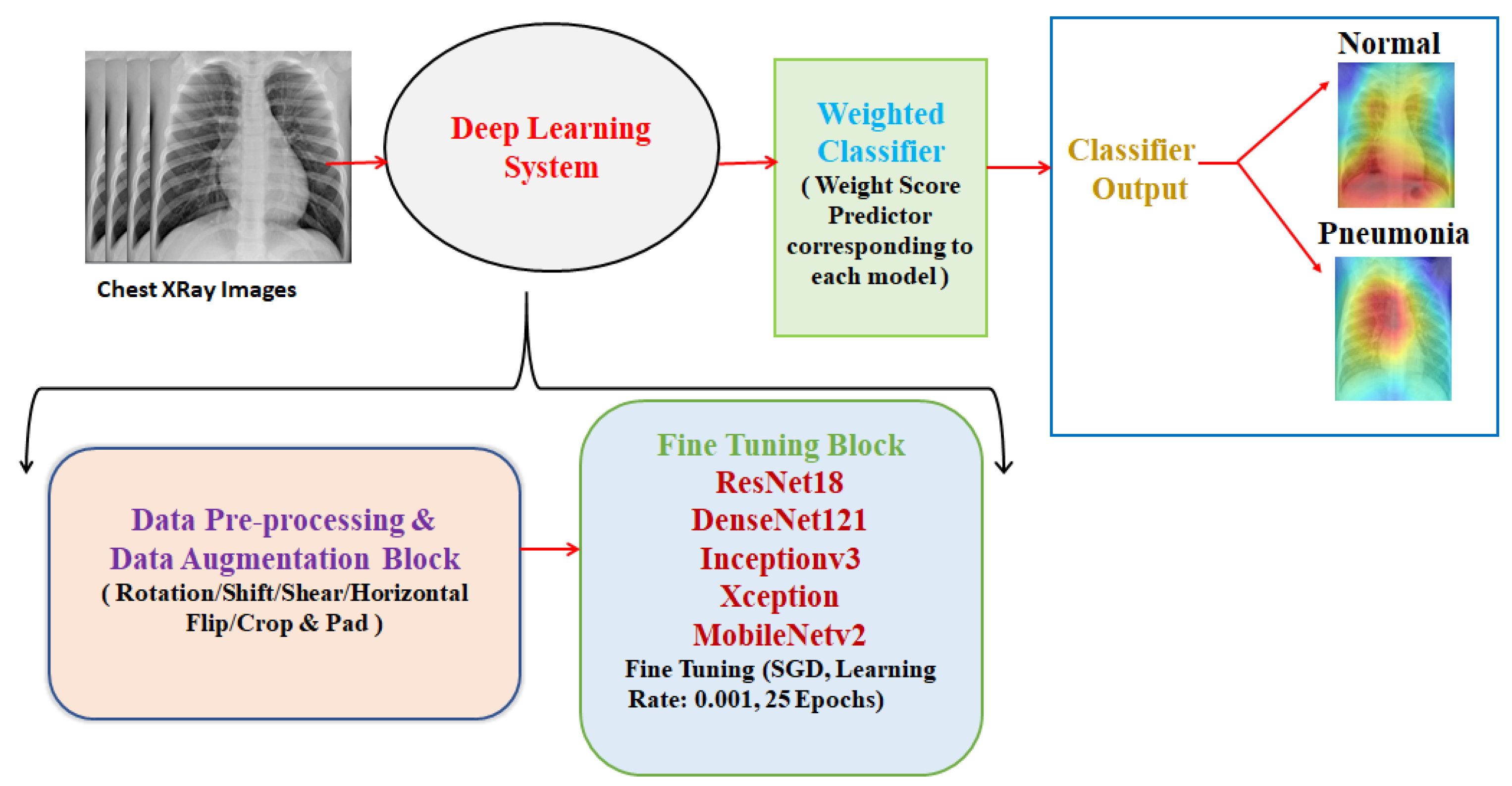
5. Proposed Methodology
5.1. Data Preprocessing and Augmentation
5.2. Fine-Tuning the Architectures
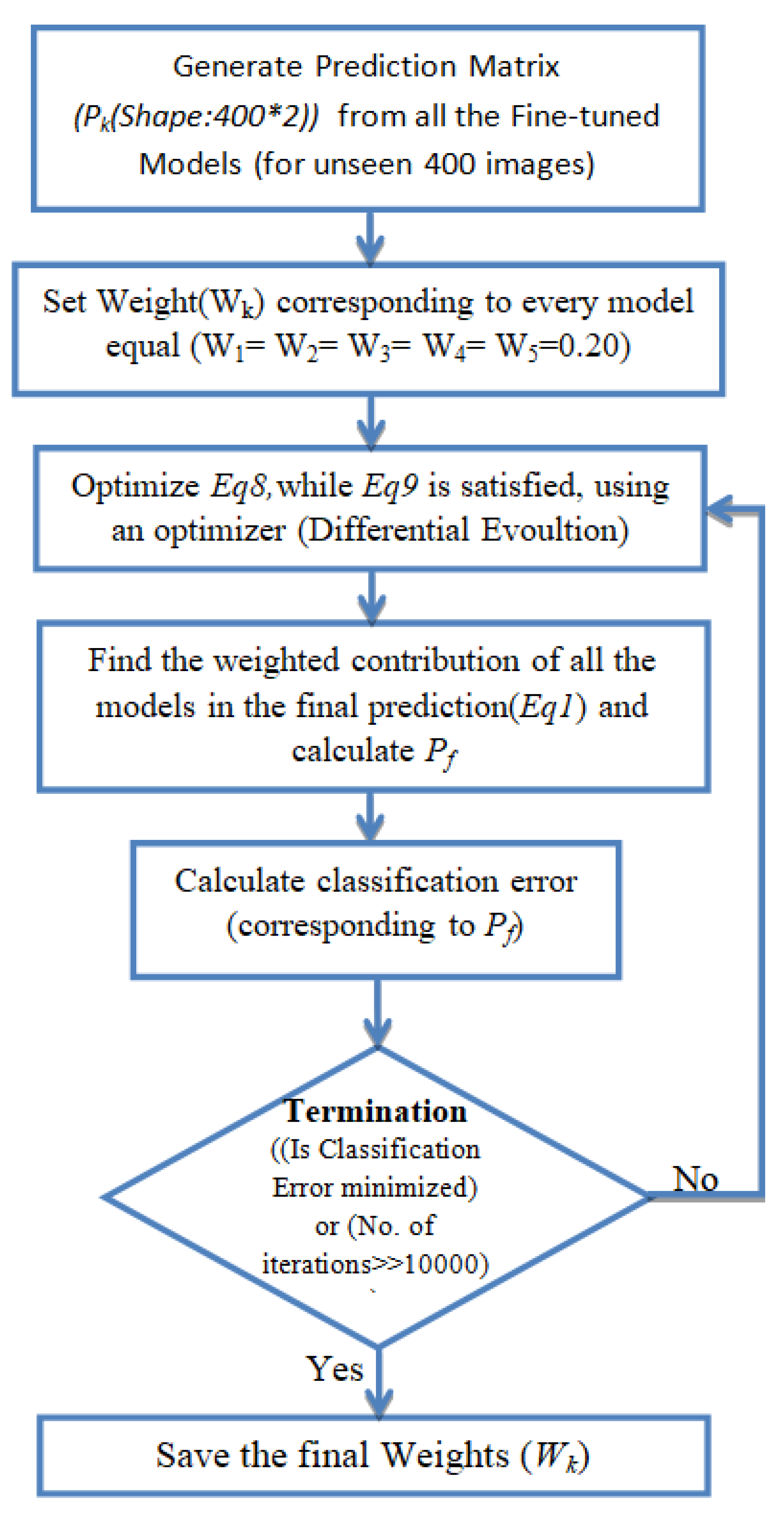
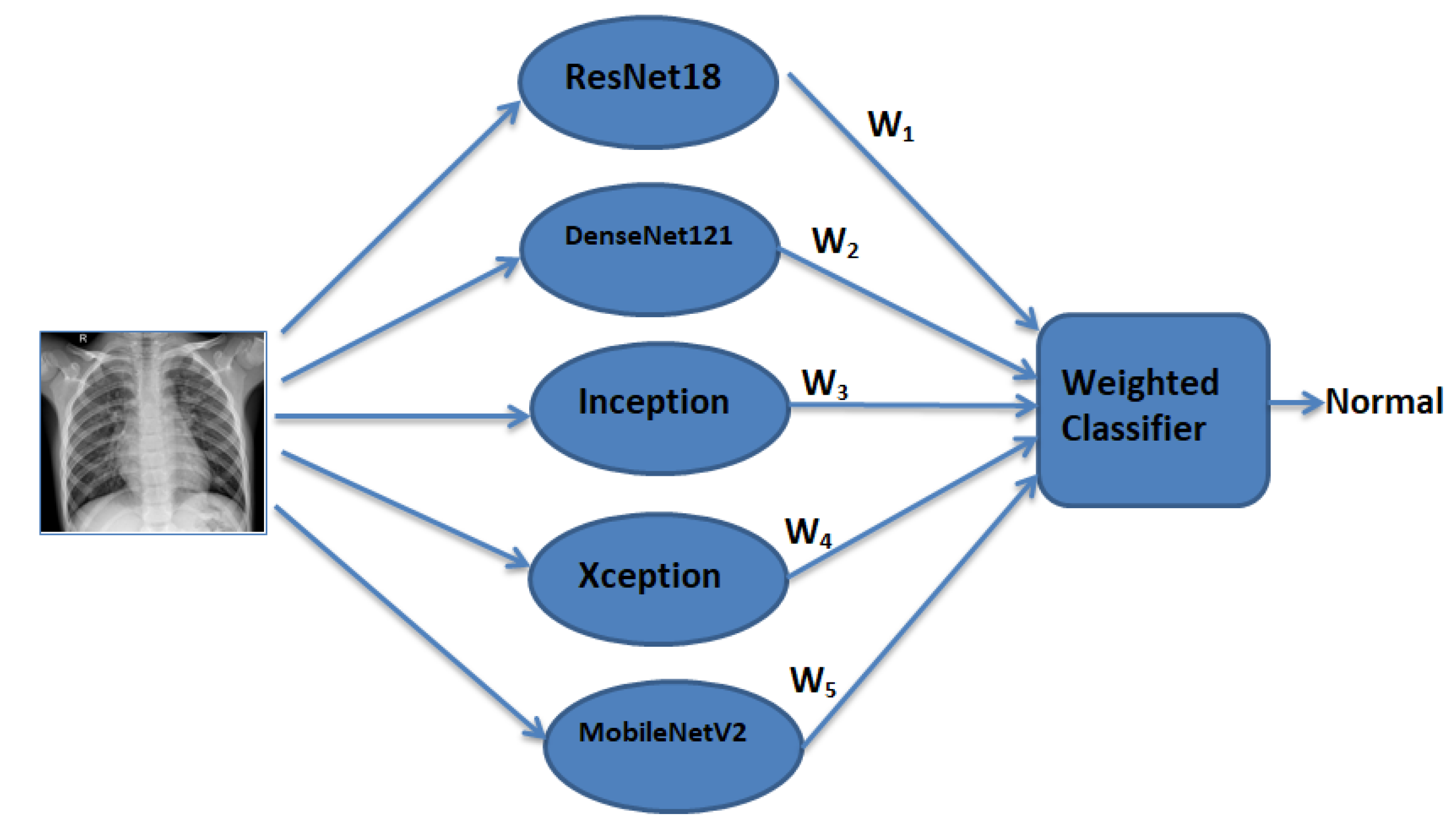
5.3. Weighted Classifier
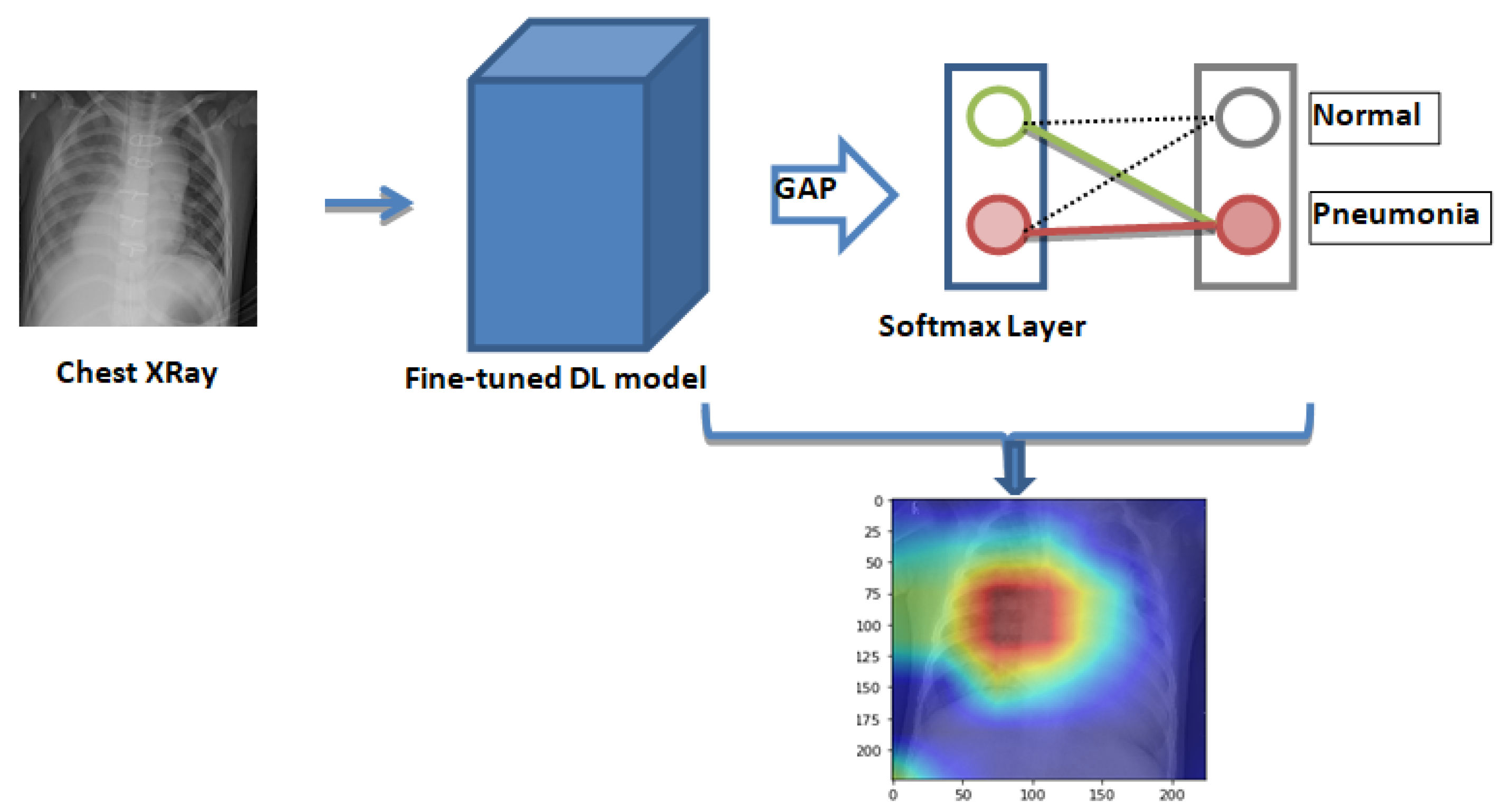
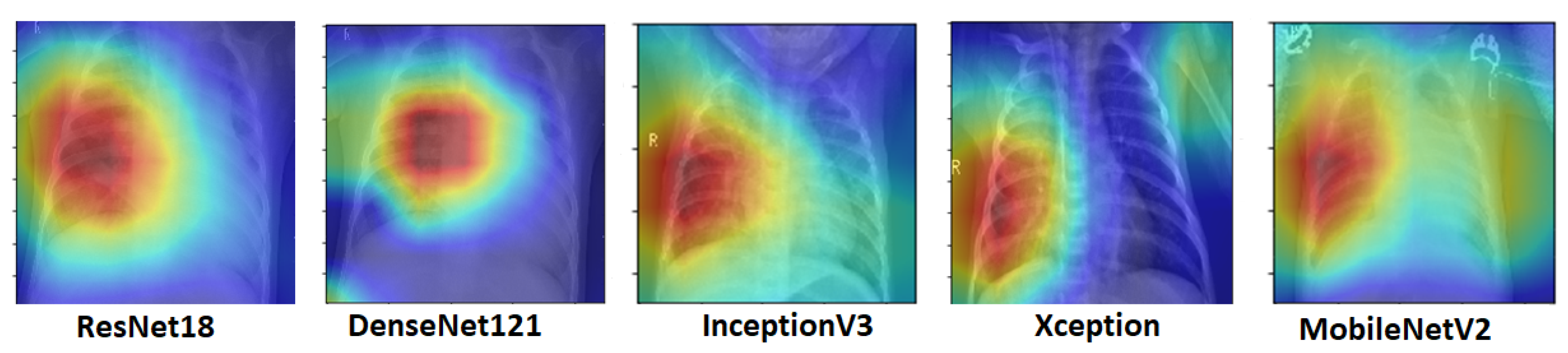
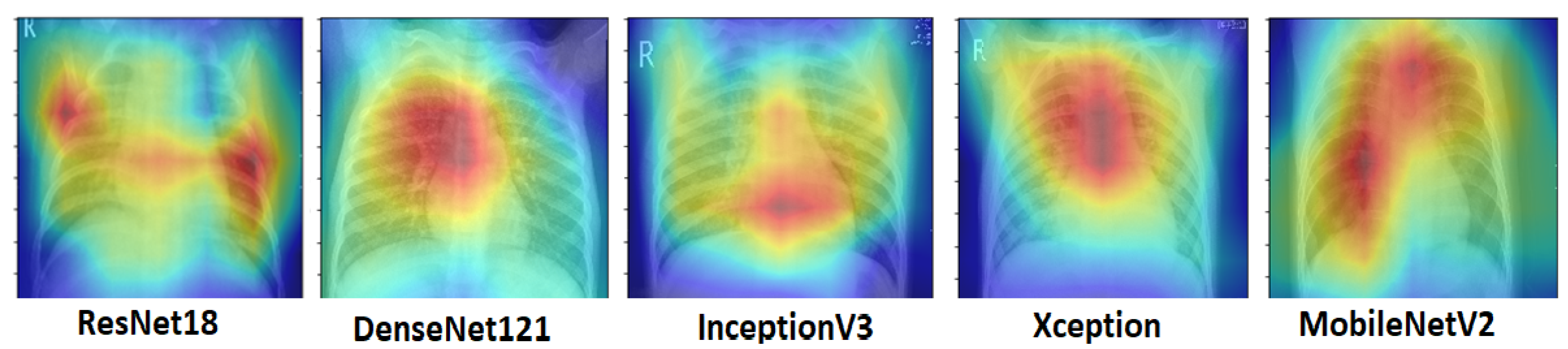
5.4. Class Activation Maps
6. Experimental Results
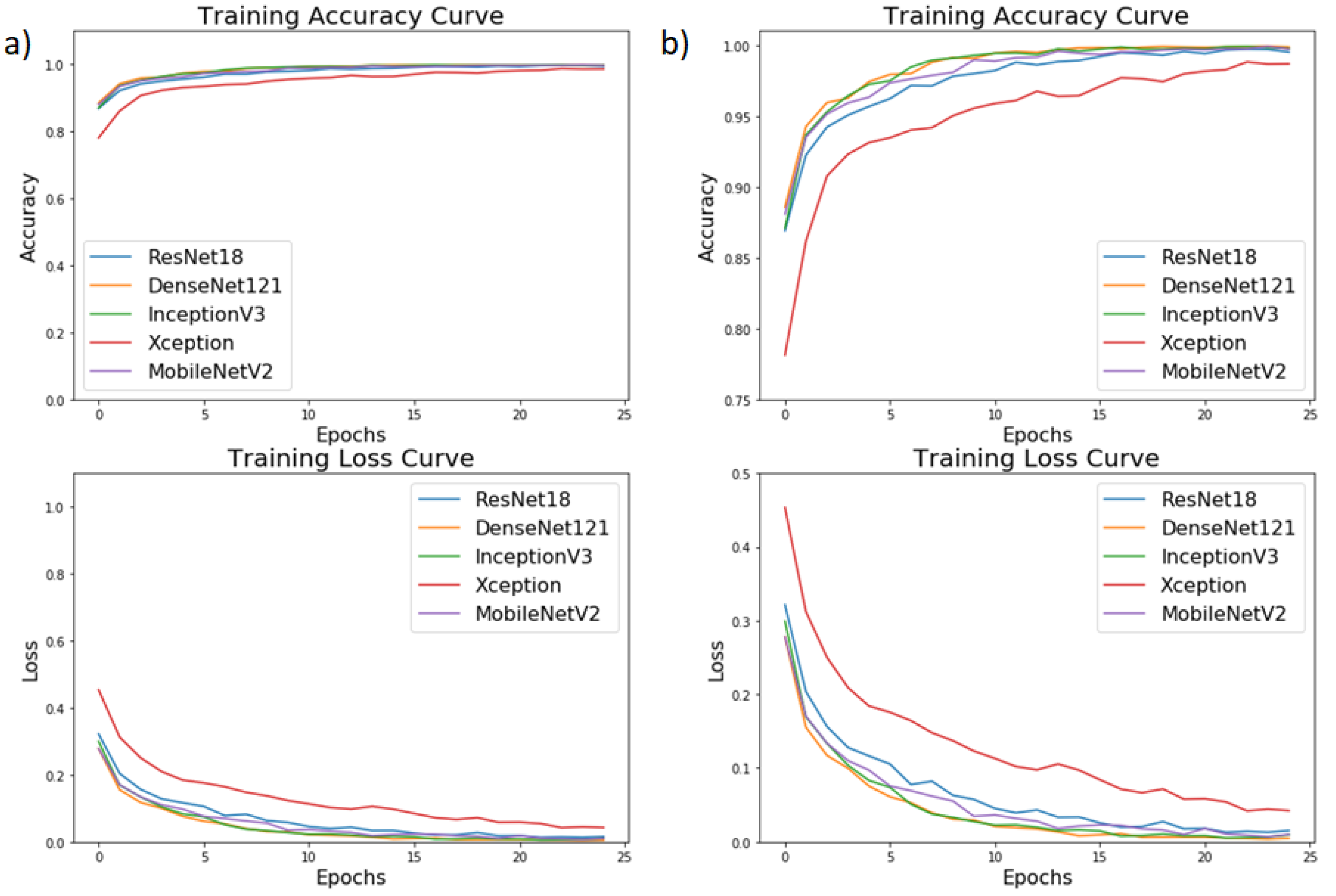
6.1. Result in Terms of Testing Accuracy and Testing Loss
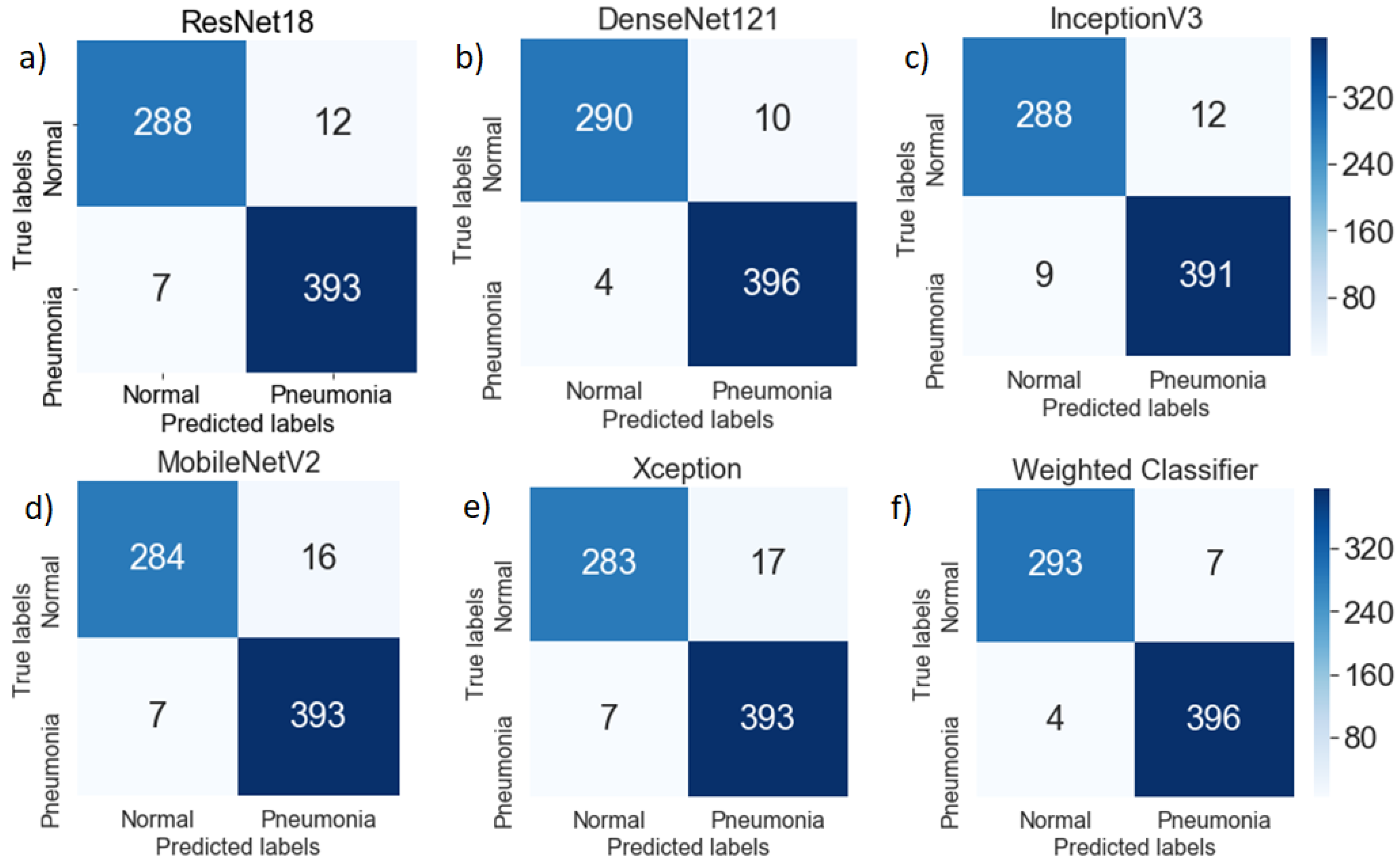
6.2. Performance Analysis
6.3. Explanation of the Results Using Heat Maps
6.4. Comparative Analysis of Various Existing Methods
7. Discussion
8. Conclusions and Future Scope
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| 2D | 2-dimensional |
| 3D | 3-dimensional |
| AI | Artificial intelligence |
| AUC | Area under the curve |
| BPNN | Back propagation neural network |
| CNN | Convolutional neural network |
| CpNN | Competitive neural network |
| CT | Computed tomography |
| DDR | Double data rate |
| GPU | General processing unit |
| DNN | Deep neural network |
| PC | Personal computer |
| SGD | Stochastic gradient descent |
| UNICEF | United Nations Children’s Fund |
| WHO | World Health Organization |
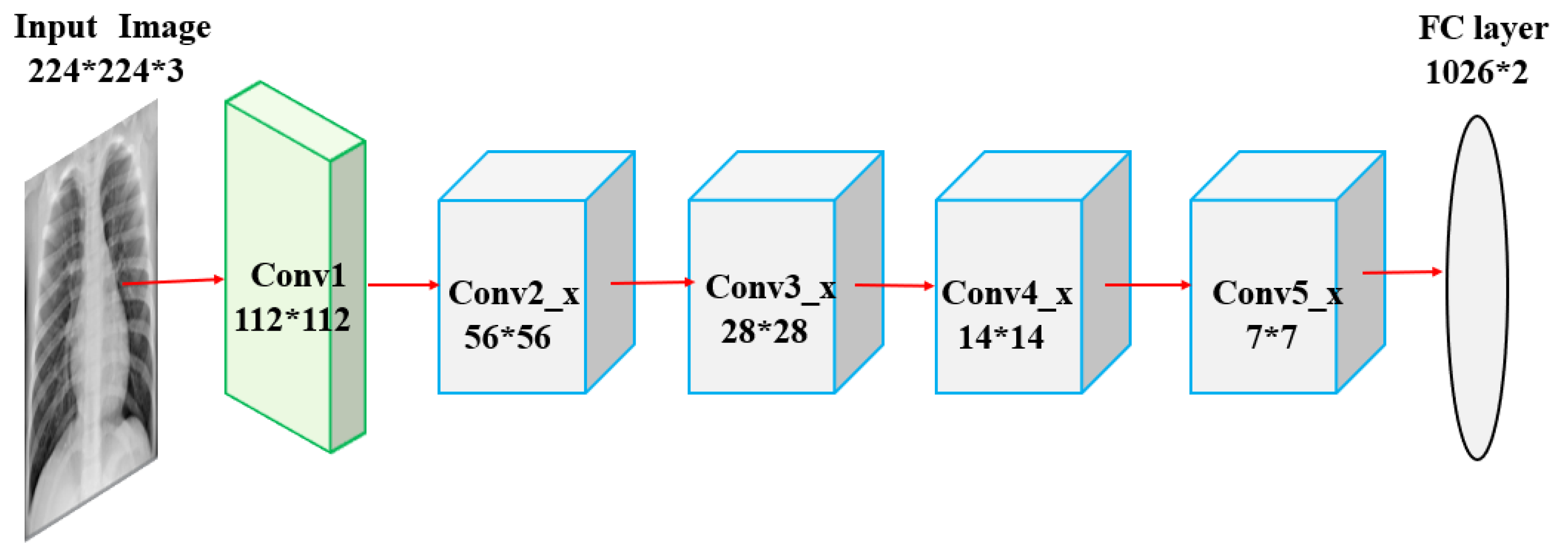
Appendix A. Pre-Trained Neural Networks Used in the Paper
Appendix A.1. ResNet18

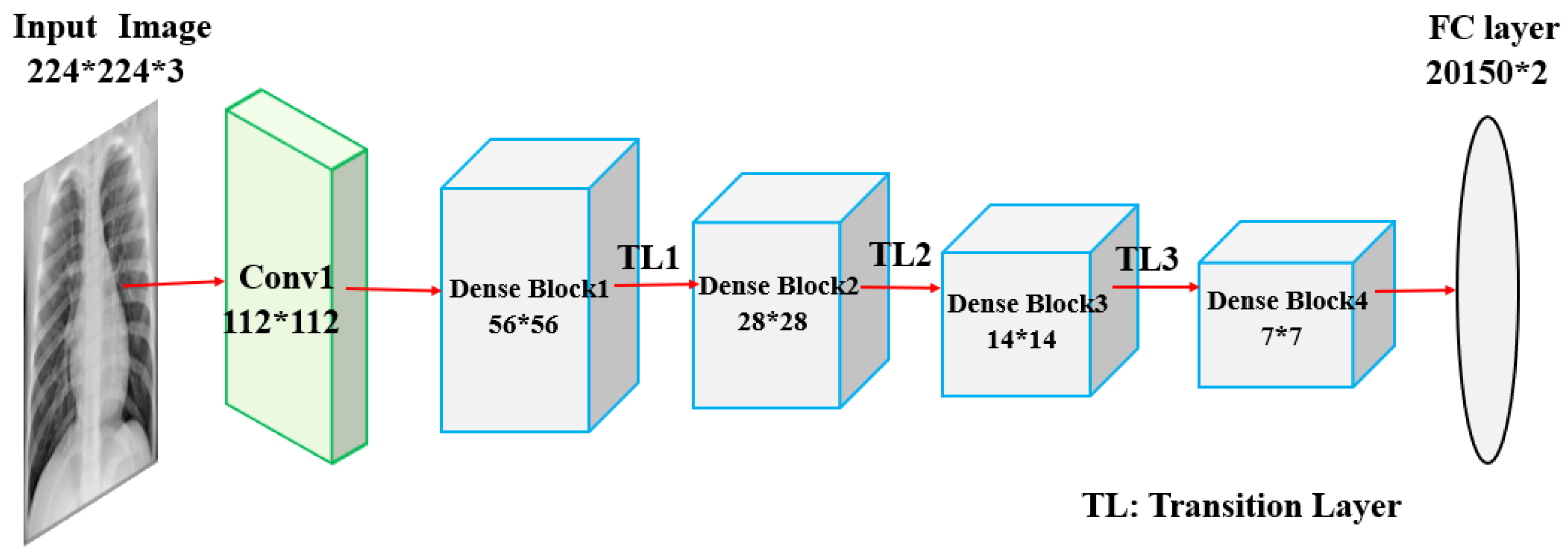
Appendix A.2. DenseNet121

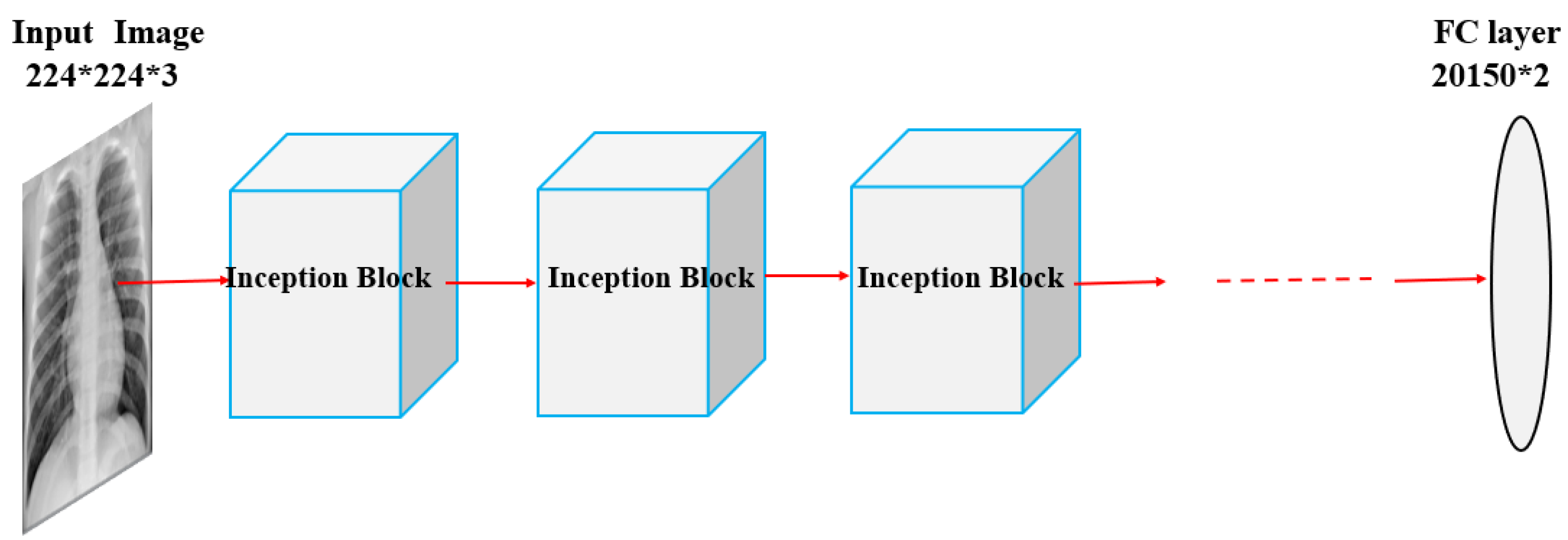
Appendix A.3. InceptionV3

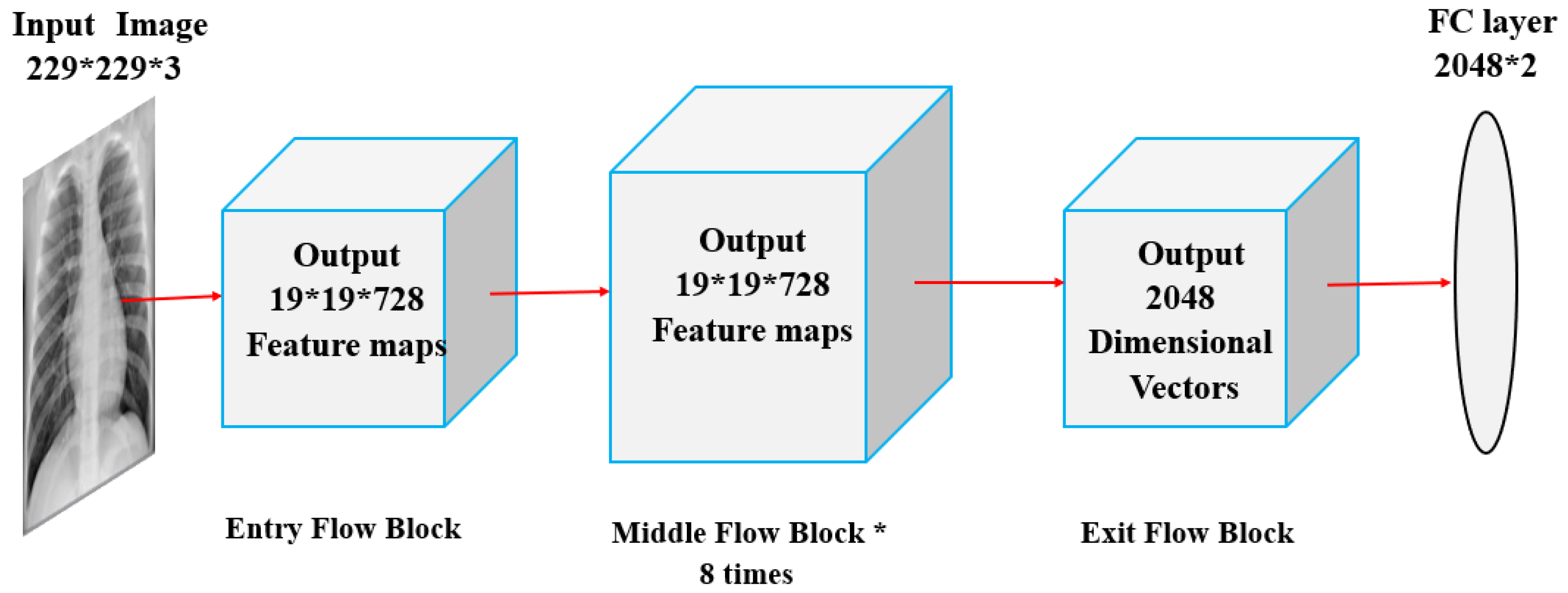
Appendix A.4. Xception

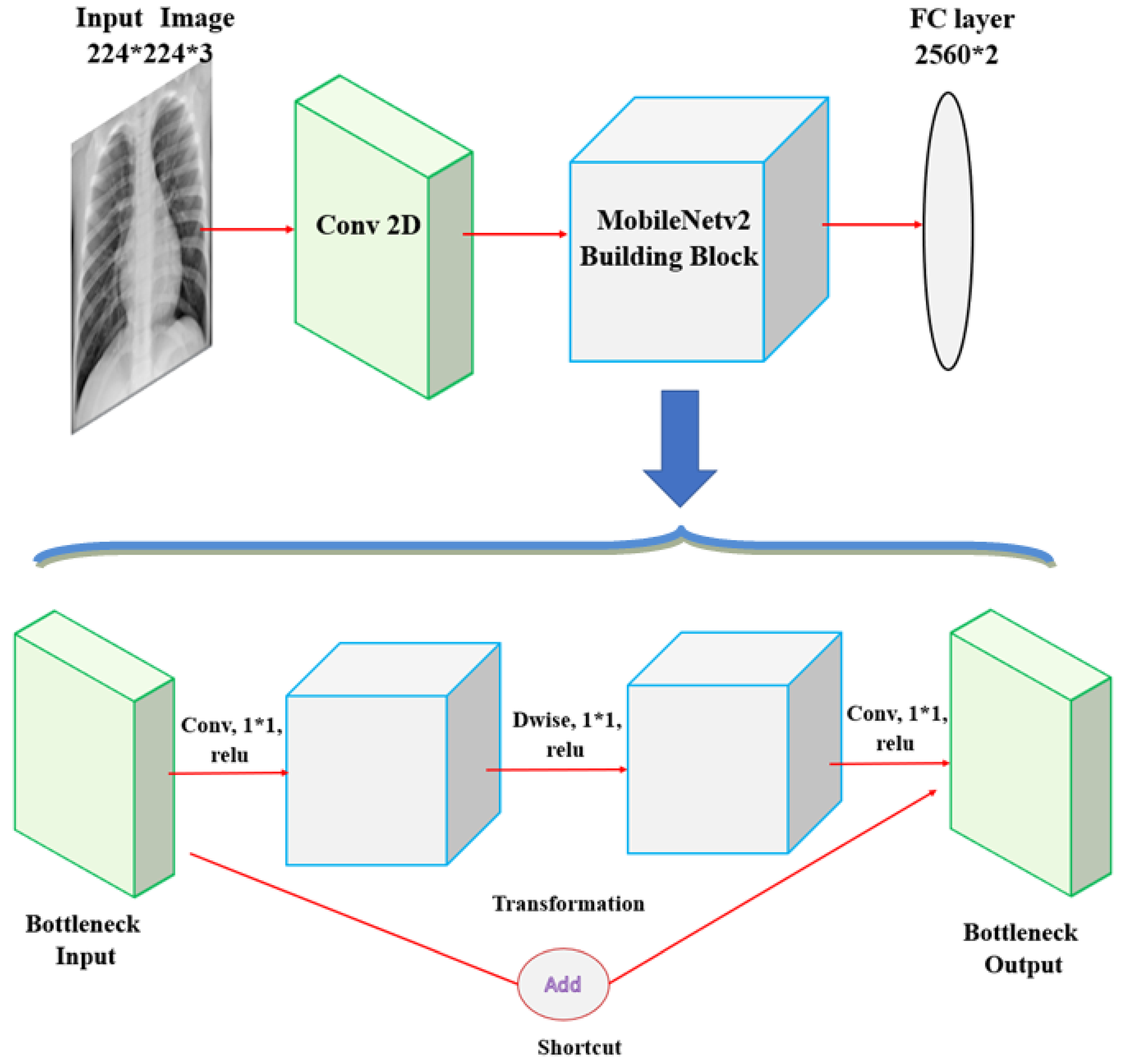
Appendix A.5. MobileNetV2

References
- Johns Hopkins Medicine. Pneumonia. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/pneumonia (accessed on 31 December 2019).
- Johnson, S.; Wells, D.; Healthline. Viral Pneumonia: Symptoms, Risk Factors, and More. Available online: https://www.healthline.com/health/viral-pneumonia (accessed on 31 December 2019).
- Healthcare, University of Utah. Pneumonia Makes List for Top 10 Causes of Death. 2016. Available online: https://healthcare.utah.edu/the-scope/shows.php?shows=0_riw4wti7 (accessed on 31 December 2019).
- WHO. Pneumonia is the Leading Cause of Death in Children. 2011. Available online: https://www.who.int/maternal_child_adolescent/news_events/news/2011/pneumonia/en (accessed on 31 December 2019).
- Rudan, I.; Tomaskovic, L.; Boschi-Pinto, C.; Campbell, H. Global estimate of the incidence of clinical pneumonia among children under five years of age. Bull. World Health Organ. 2004, 82, 895–903. [Google Scholar] [PubMed]
- Pneumonia. Available online: https://www.radiologyinfo.org/en/info.cfm?pg=pneumonia (accessed on 31 December 2019).
- World Health Organization. Standardization of Interpretation of Chest Radiographs for the Diagnosis of Pneumonia in Children; Technical Report; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Cherian, T.; Mulholland, E.K.; Carlin, J.B.; Ostensen, H.; Amin, R.; Campo, M.D.; Greenberg, D.; Lagos, R.; Lucero, M.; Madhi, S.A.; et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull. World Health Organ. 2005, 83, 353–359. [Google Scholar]
- Franquet, T. Imaging of pneumonia: Trends and algorithms. Eur. Respir. J. 2001, 18, 196–208. [Google Scholar] [CrossRef] [Green Version]
- Tahir, A.M.; Chowdhury, M.E.; Khandakar, A.; Al-Hamouz, S.; Abdalla, M.; Awadallah, S.; Reaz, M.B.I.; Al-Emadi, N. A systematic approach to the design and characterization of a smart insole for detecting vertical ground reaction force (vGRF) in gait analysis. Sensors 2020, 20, 957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, M.E.; Alzoubi, K.; Khandakar, A.; Khallifa, R.; Abouhasera, R.; Koubaa, S.; Ahmed, R.; Hasan, A. Wearable real-time heart attack detection and warning system to reduce road accidents. Sensors 2019, 19, 2780. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, M.E.H.; Khandakar, A.; Alzoubi, K.; Mansoor, S.; Tahir, A.M.; Reaz, M.B.I.; Al-Emadi, N. Real-time smart-digital stethoscope system for heart diseases monitoring. Sensors 2019, 19, 2781. [Google Scholar] [CrossRef] [Green Version]
- Kallianos, K.; Mongan, J.; Antani, S.; Henry, T.; Taylor, A.; Abuya, J.; Kohli, M. How far have we come? Artificial intelligence for chest radiograph interpretation. Clin. Radiol. 2019, 74, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Wan, L.; Zhang, Y.; Zhou, T.; Huo, H.; Fang, T. Exploiting convolutional neural networks with deeply local description for remote sensing image classification. IEEE Access 2018, 6, 11215–11228. [Google Scholar] [CrossRef]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Naicker, S.; Plange-Rhule, J.; Tutt, R.C.; Eastwood, J.B. Shortage of healthcare workers in developing countries–Africa. Ethn. Dis. 2009, 19, 60. [Google Scholar]
- Douarre, C.; Schielein, R.; Frindel, C.; Gerth, S.; Rousseau, D. Transfer learning from synthetic data applied to soil–root segmentation in x-ray tomography images. J. Imaging 2018, 4, 65. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wang, G.; Li, M.; Han, S. Automated classification analysis of geological structures based on images data and deep learning model. Appl. Sci. 2018, 8, 2493. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, C.; Zhang, H. Ship classification in high-resolution SAR images using deep learning of small datasets. Sensors 2018, 18, 2929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, C.; Yang, Y.; Wen, C.; Xie, K.; Wen, F. Voiceprint identification for limited dataset using the deep migration hybrid model based on transfer learning. Sensors 2018, 18, 2399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Zhang, Y.; Ouyang, C.; Zhang, F.; Ma, J. Automated landslides detection for mountain cities using multi-temporal remote sensing imagery. Sensors 2018, 18, 821. [Google Scholar] [CrossRef] [Green Version]
- Razzak, M.I.; Naz, S.; Zaib, A. Deep learning for medical image processing: Overview, challenges and the future. In Classification in BioApps; Springer: Cham, Switzerland, 2018; pp. 323–350. [Google Scholar]
- Shen, D.; Wu, G.; Suk, H.I. Deep learning in medical image analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [Green Version]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Milletari, F.; Navab, N.; Ahmadi, S.A. V-net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the International Conference on 3D Vision, Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar]
- Grewal, M.; Srivastava, M.M.; Kumar, P.; Varadarajan, S. Radnet: Radiologist level accuracy using deep learning for hemorrhage detection in ct scans. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging, Washington, DC, USA, 4–7 April 2018; pp. 281–284. [Google Scholar]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Bar, Y.; Diamant, I.; Wolf, L.; Lieberman, S.; Konen, E.; Greenspan, H. Chest pathology detection using deep learning with non-medical training. In Proceedings of the 2015 IEEE 12th International Symposium on Biomedical Imaging (ISBI), New York, NY, USA, 16–19 April 2015; pp. 294–297. [Google Scholar]
- Avni, U.; Greenspan, H.; Konen, E.; Sharon, M.; Goldberger, J. X-ray categorization and retrieval on the organ and pathology level, using patch based visual words. IEEE Trans. Med. Imaging 2010, 30, 733–746. [Google Scholar] [CrossRef]
- Melendez, J.; van Ginneken, B.; Maduskar, P.; Philipsen, R.H.; Reither, K.; Breuninger, M.; Adetifa, I.M.; Maane, R.; Ayles, H.; Sánchez, C.I. A novel multiple-instance learning based approach to computer-aided detection of tuberculosis on chest x-rays. IEEE Trans. Med. Imaging 2014, 34, 179–192. [Google Scholar] [CrossRef]
- Jaeger, S.; Karargyris, A.; Candemir, S.; Folio, L.; Siegelman, J.; Callaghan, F.; Xue, Z.; Palaniappan, K.; Singh, R.K.; Antani, S.; et al. Automatic tuberculosis screening using chest radiographs. IEEE Trans. Med. Imaging 2013, 33, 233–245. [Google Scholar] [CrossRef]
- Hermann, S. Evaluation of scan-line optimization for 3D medical image registration. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 3073–3080. [Google Scholar]
- Nasrullah, N.; Sang, J.; Alam, M.S.; Mateen, M.; Cai, B.; Hu, H. Automated Lung Nodule Detection and Classification Using Deep Learning Combined with Multiple Strategies. Sensors 2019, 19, 3722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, L.; Poblenz, E.; Dagunts, D.; Covington, B.; Bernard, D.; Lyman, K. Learning to diagnose from scratch by exploiting dependencies among labels. arXiv 2017, arXiv:1710.10501. [Google Scholar]
- Khatri, A.A.R.J.; Vashista, H.; Mittal, N.; Ranjan, P.; Janardhanan, R. Pneumonia Identification in Chest X-Ray Images Using EMD. In Trends in Communication, Cloud, and Big Data; Springer: Singapore, 2020; pp. 87–98. [Google Scholar]
- Abiyev, R.H.; Ma’aitah, M.K.S. Deep convolutional neural networks for chest diseases detection. J. Healthc. Eng. 2018, 2018, 4168538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephen, O.; Sain, M.; Maduh, U.J.; Jeong, D.U. An efficient deep learning approach to pneumonia classification in healthcare. J. Healthc. Eng. 2019, 2019, 4180949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J.P.; Bertin, P.; Frappier, V. Chester: A Web Delivered Locally Computed Chest X-Ray Disease Prediction System. arXiv 2019, arXiv:1901.11210. [Google Scholar]
- Rajaraman, S.; Candemir, S.; Kim, I.; Thoma, G.; Antani, S. Visualization and interpretation of convolutional neural network predictions in detecting pneumonia in pediatric chest radiographs. Appl. Sci. 2018, 8, 1715. [Google Scholar] [CrossRef] [Green Version]
- Sirazitdinov, I.; Kholiavchenko, M.; Mustafaev, T.; Yixuan, Y.; Kuleev, R.; Ibragimov, B. Deep neural network ensemble for pneumonia localization from a large-scale chest x-ray database. Comput. Electr. Eng. 2019, 78, 388–399. [Google Scholar] [CrossRef]
- Lakhani, P.; Sundaram, B. Deep learning at chest radiography: Automated classification of pulmonary tuberculosis by using convolutional neural networks. Radiology 2017, 284, 574–582. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Irvin, J.; Ball, R.L.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T. Deep learning for chest radiograph diagnosis: A retrospective comparison of the CheXNeXt algorithm to practicing radiologists. PLoS Med. 2018, 15, e1002686. [Google Scholar] [CrossRef]
- Ho, T.K.K.; Gwak, J. Multiple feature integration for classification of thoracic disease in chest radiography. Appl. Sci. 2019, 9, 4130. [Google Scholar] [CrossRef] [Green Version]
- Saraiva, A.; Santos, D.; Costa, N.J.C.; Sousa, J.V.M.; Ferreira, N.F.; Valente, A.; Soares, S. Models of Learning to Classify X-ray Images for the Detection of Pneumonia using Neural Networks. 2019. Available online: https://www.semanticscholar.org/paper/Models-of-Learning-to-Classify-X-ray-Images-for-the-Saraiva-Santos/0b8f202505b3d49c42fd45d86eca5dbd0b76fded?p2df (accessed on 18 June 2020). [CrossRef]
- Ayan, E.; Ünver, H.M. Diagnosis of Pneumonia from Chest X-Ray Images Using Deep Learning. In Proceedings of the 2019 Scientific Meeting on Electrical-Electronics & Biomedical Engineering and Computer Science (EBBT), Istanbul, Turkey, 2–26 April 2019; pp. 1–5. [Google Scholar]
- Rahman, T.; Chowdhury, M.E.; Khandakar, A.; Islam, K.R.; Islam, K.F.; Mahbub, Z.B.; Kadir, M.A.; Kashem, S. Transfer Learning with Deep Convolutional Neural Network (CNN) for Pneumonia Detection using Chest X-ray. Appl. Sci. 2020, 10, 3233. [Google Scholar] [CrossRef]
- Xiao, Z.; Du, N.; Geng, L.; Zhang, F.; Wu, J.; Liu, Y. Multi-scale heterogeneous 3D CNN for false-positive reduction in pulmonary nodule detection, based on chest CT images. Appl. Sci. 2019, 9, 3261. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.; Wu, H.; Bie, R. CXNet-m1: Anomaly detection on chest X-rays with image based deep learning. IEEE Access 2018, 7, 4466–4477. [Google Scholar] [CrossRef]
- Jaiswal, A.K.; Tiwari, P.; Kumar, S.; Gupta, D.; Khanna, A.; Rodrigues, J.J. Identifying pneumonia in chest X-rays: A deep learning approach. Measurement 2019, 145, 511–518. [Google Scholar] [CrossRef]
- Jung, H.; Kim, B.; Lee, I. Classification of lung nodules in CT scans using three-dimensional deep convolutional neural networks with a checkpoint ensemble method. BMC Med. Imaging 2018, 18, 48. [Google Scholar] [CrossRef]
- Chouhan, V.; Singh, S.K.; Khamparia, A.; Gupta, D.; Tiwari, P.; Moreira, C.; Damaševičius, R.; de Albuquerque, V.H.C. A Novel Transfer Learning Based Approach for Pneumonia Detection in Chest X-ray Images. Appl. Sci. 2020, 10, 559. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Boser, B.; Denker, J.S.; Henderson, D.; Howard, R.E.; Hubbard, W.; Jackel, L.D. Backpropagation applied to handwritten zip code recognition. Neural Comput. 1989, 1, 541–551. [Google Scholar] [CrossRef]
- Pan, S.J.; Yang, Q. A survey on transfer learning. IEEE Trans. Knowl. Data Eng. 2009, 22, 1345–1359. [Google Scholar] [CrossRef]
- Fei-Fei, L. ImageNet: Crowdsourcing, benchmarking & other cool things. In CMU VASC Seminar, Carnegie Mellon University; Pittsburgh, PA, USA, 2010; Volume 16, pp. 18–25. Available online: http://www.image-net.org/papers/ImageNet_2010.pdf (accessed on 18 June 2020).
- Kermany, D.; Goldbaum, M.; Cai, W. Large dataset of labeled optical coherence tomography (OCT) and chest X-Ray images 2018, 172, 1122–1131. Cell 2018, 172, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.C.; Roelofs, R.; Stern, M.; Srebro, N.; Recht, B. The marginal value of adaptive gradient methods in machine learning. In Advances in Neural Information Processing Systems; Neural Information Processing Systems: City of Berkeley, CA, USA, 2017; pp. 4148–4158. [Google Scholar]
- Storn, R.; Price, K. Differential evolution–a simple and efficient heuristic for global optimization over continuous spaces. J. Glob. Optim. 1997, 11, 341–359. [Google Scholar] [CrossRef]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning deep features for discriminative localization. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 2921–2929. [Google Scholar]
- Koo, H.J.; Lim, S.; Choe, J.; Choi, S.H.; Sung, H.; Do, K.H. Radiographic and CT features of viral pneumonia. Radiographics 2018, 38, 719–739. [Google Scholar] [CrossRef] [Green Version]
- Toğaçar, M.; Ergen, B.; Cömert, Z. A deep feature learning model for pneumonia detection applying a combination of mRMR feature selection and machine learning models. IRBM 2019. [Google Scholar] [CrossRef]
- Gonçalves-Pereira, J.; Conceição, C.; Póvoa, P. Community-acquired pneumonia: Identification and evaluation of nonresponders. Ther. Adv. Infect. Dis. 2013, 1, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Mollura, D.J.; Azene, E.M.; Starikovsky, A.; Thelwell, A.; Iosifescu, S.; Kimble, C.; Polin, A.; Garra, B.S.; DeStigter, K.K.; Short, B.; et al. White paper report of the RAD-AID Conference on International Radiology for Developing Countries: Identifying challenges, opportunities, and strategies for imaging services in the developing world. J. Am. Coll. Radiol. 2010, 7, 495–500. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In The IEEE Conference on Computer Vision and Pattern Recognition (CVPR); July 2017; pp. 4700–4708. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 2818–2826. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Training Set | Test Set |
|---|---|---|
| Normal (Healthy) | 1283 | 300 |
| Pneumonia (Viral + Bacteria) | 3873 | 400 |
| Total | 5156 | 700 |
| Percentage | 88.05% | 11.95% |
| Technique | Setting |
|---|---|
| Rotation | 45 |
| Vertical Shift | 0.2 |
| Horizontal Shift | 0.15 |
| Shear | 16 |
| Crop and Pad | 0.25 |
| Architecture | Image Size | Epochs | Optimizer | Learning Rate | Momentum | Weight Decay |
|---|---|---|---|---|---|---|
| ResNet18 | 224 × 224 | |||||
| DenseNet121 | 224 × 224 | |||||
| InceptionV3 | 229 × 229 | 25 | Stochastic Gradient Descent | 0.001 | 0.9 | 0.0001 |
| Xception | 229 × 229 | |||||
| MobileNetV2 | 224 × 224 |
| Architecture | Testing Accuracy | Testing Loss |
|---|---|---|
| ResNet18 | 97.29 | 0.096 |
| DenseNet121 | 98.00 | 0.064 |
| Inception | 97.00 | 0.098 |
| Xception | 96.57 | 0.101 |
| MobileNetV2 | 96.71 | 0.096 |
| Weighted Classifier (With Equal Weights) | 97.45 | 0.087 |
| Weighted Classifier (With Optimized Weights) | 98.43 | 0.062 |
| Architecture | Weight |
|---|---|
| ResNet18 (W1) | 0.25 |
| DenseNet121 (W2) | 0.30 |
| Inception (W3) | 0.18 |
| Xception (W4) | 0.08 |
| MobileNetV2 (W5) | 0.19 |
| Architecture | Accuracy | Precision | Recall | F1 Score | AUC Score |
|---|---|---|---|---|---|
| ResNet18 | 97.29 | 97.03 | 98.25 | 97.63 | 99.46 |
| DenseNet121 | 98.00 | 97.53 | 99.00 | 98.26 | 99.65 |
| InceptionV3 | 97.00 | 97.02 | 97.75 | 97.39 | 99.49 |
| Xception | 96.57 | 95.85 | 98.25 | 97.03 | 99.59 |
| MobileNetV2 | 96.71 | 96.08 | 98.25 | 97.15 | 99.52 |
| Weighted Classifier | 98.43 | 98.26 | 99.00 | 98.63 | 99.76 |
| Model | No. of Images | Precision | Recall | Accuracy | AUC |
|---|---|---|---|---|---|
| Rahib H.Abiyey et al. [36] | 1000 | - | - | 92.4 | - |
| Okeke Stephen et al. [37] | 5856 | - | - | 93.73 | - |
| Cohen et al. [38] | 5232 | 90.1 | 93.2 | 92.8 | 99.0 |
| Rajaraman et al. [39] | 5856 | 97.0 | 99.5 | 96.2 | 99.0 |
| M.Togacar et al. [60] | 5849 | 96.88 | 96.83 | 96.84 | 96.80 |
| Saraiva et al. [44] | 5840 | 94.3 | 94.5 | 94.4 | 94.5 |
| Ayan et al. [45] | 5856 | 91.3 | 89.1 | 84.5 | 87.0 |
| Rahman et al. [46] | 5247 | 97.0 | 99.0 | 98.0 | 98.0 |
| Vikash et al. [51] | 5232 | 93.28 | 99.6 | 96.39 | 99.34 |
| Proposed Methodology | 5856 | 98.26 | 99.00 | 98.43 | 99.76 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashmi, M.F.; Katiyar, S.; Keskar, A.G.; Bokde, N.D.; Geem, Z.W. Efficient Pneumonia Detection in Chest Xray Images Using Deep Transfer Learning. Diagnostics 2020, 10, 417. https://doi.org/10.3390/diagnostics10060417
Hashmi MF, Katiyar S, Keskar AG, Bokde ND, Geem ZW. Efficient Pneumonia Detection in Chest Xray Images Using Deep Transfer Learning. Diagnostics. 2020; 10(6):417. https://doi.org/10.3390/diagnostics10060417
Chicago/Turabian StyleHashmi, Mohammad Farukh, Satyarth Katiyar, Avinash G Keskar, Neeraj Dhanraj Bokde, and Zong Woo Geem. 2020. "Efficient Pneumonia Detection in Chest Xray Images Using Deep Transfer Learning" Diagnostics 10, no. 6: 417. https://doi.org/10.3390/diagnostics10060417