
Niosomal Curcumin Suppresses IL17/IL23 Immunopathogenic Axis in Skin Lesions of Psoriatic Patients: A Pilot Randomized Controlled Trial
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparing the CUR-NIO Formulation
2.2. Characterizing the CUR-NIO Composition
2.2.1. Size, Distribution and Zeta Potential
2.2.2. Encapsulation Efficiency (EE%) and Loading Capacity of Vesicles
2.2.3. Preparing the of CUR-NIO Loaded Topical Cream
2.3. Patients and Sample Selection
2.3.1. Criteria
2.3.2. Ex-Vivo Study
2.3.3. Intervention
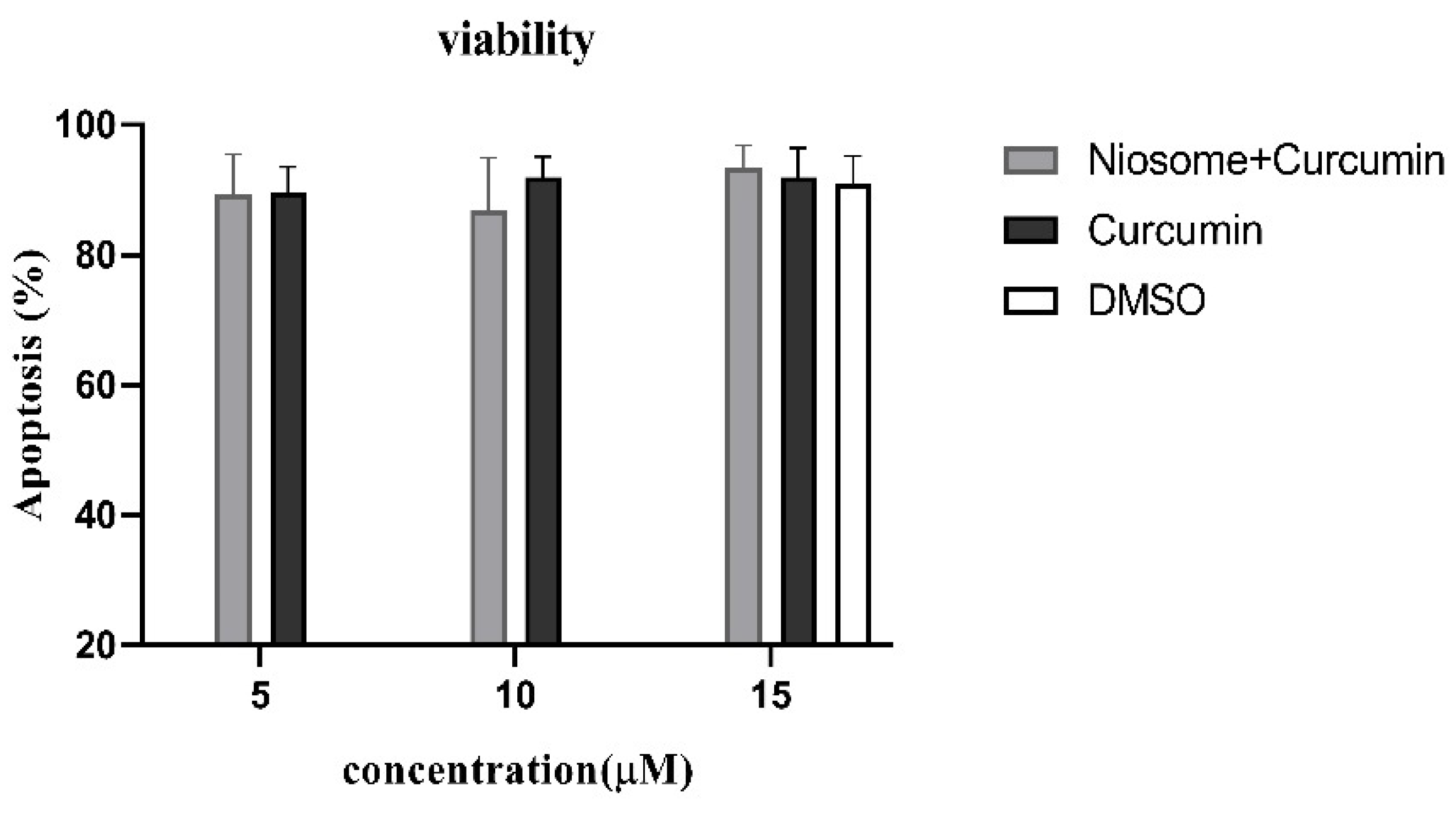
2.4. Apoptosis Assessment of CUR-NIO
2.5. Quantitative Real-Time PCR
2.6. Statistical Analyses
3. Results
3.1. Characterizing NIO Nanoparticles
3.2. The CUR-NIO Suspension Exerted Low Toxic Effects on PBMCs
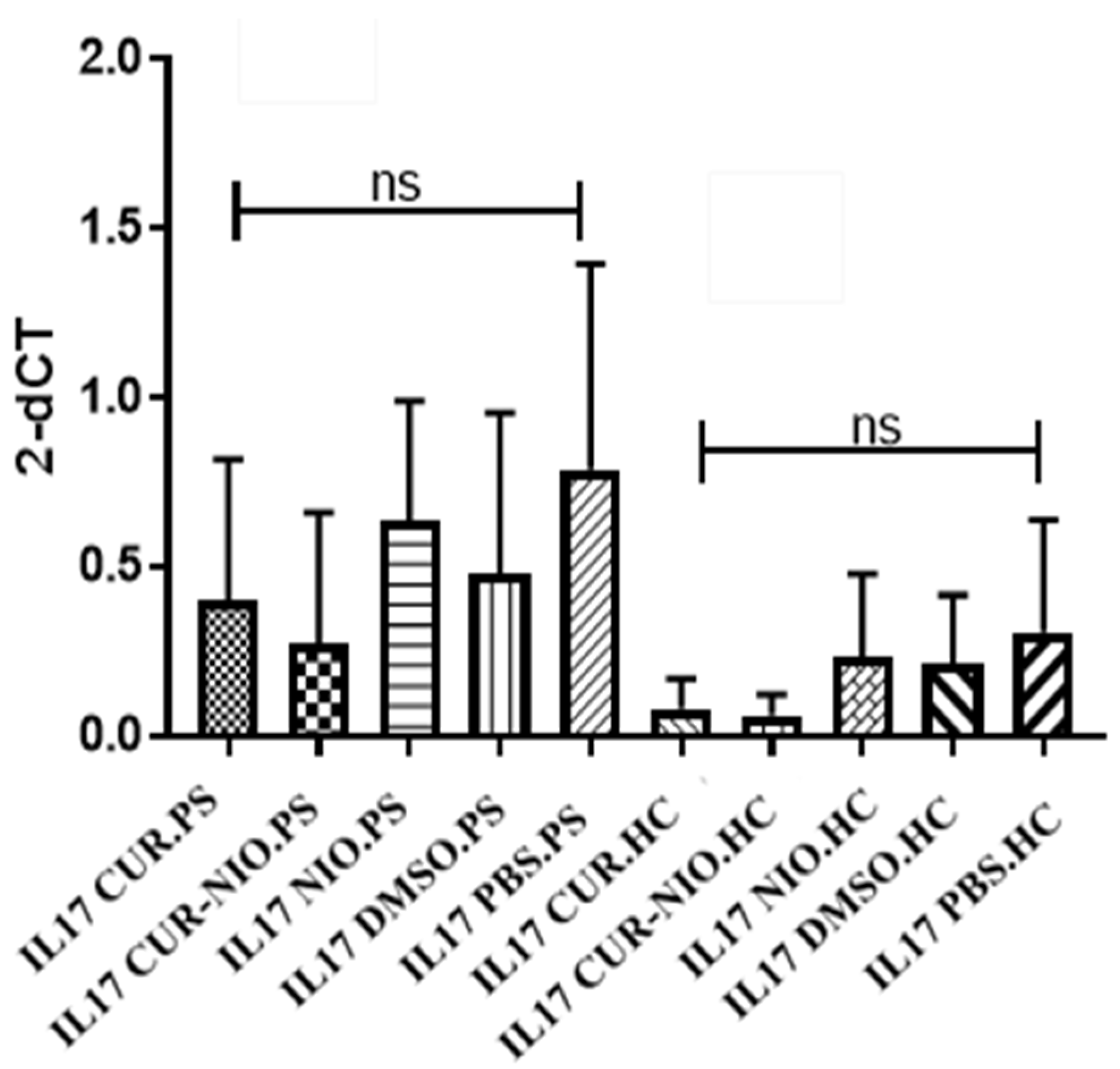
3.3. Effect of CUR on IL17 Gene Expression in PBMCs from Healthy Donors and PS Patients
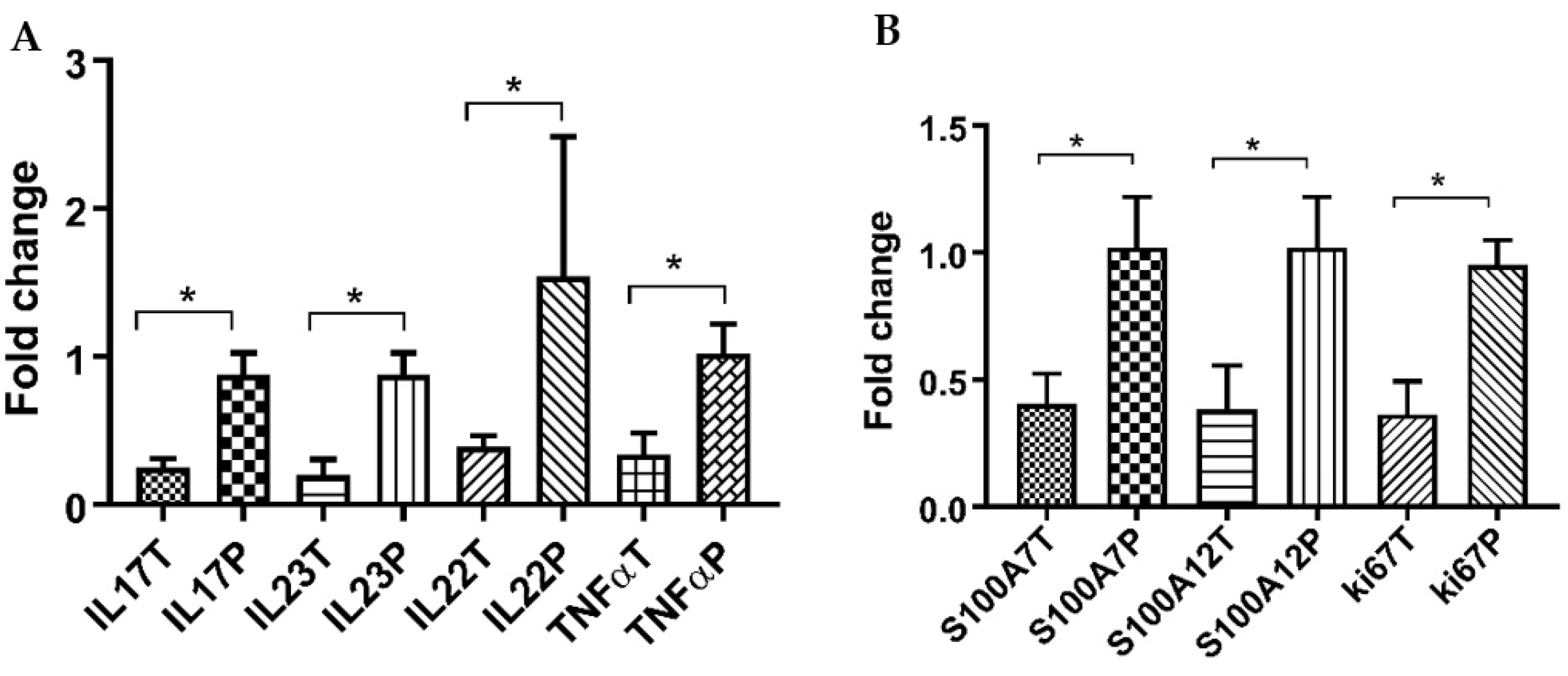
3.4. CUR-NIO Gel Reduces Inflammatory Cytokines in Psoriatic Lesions
3.5. Effects of CUR-NIO Gel on S100A7, S100A12 and ki67
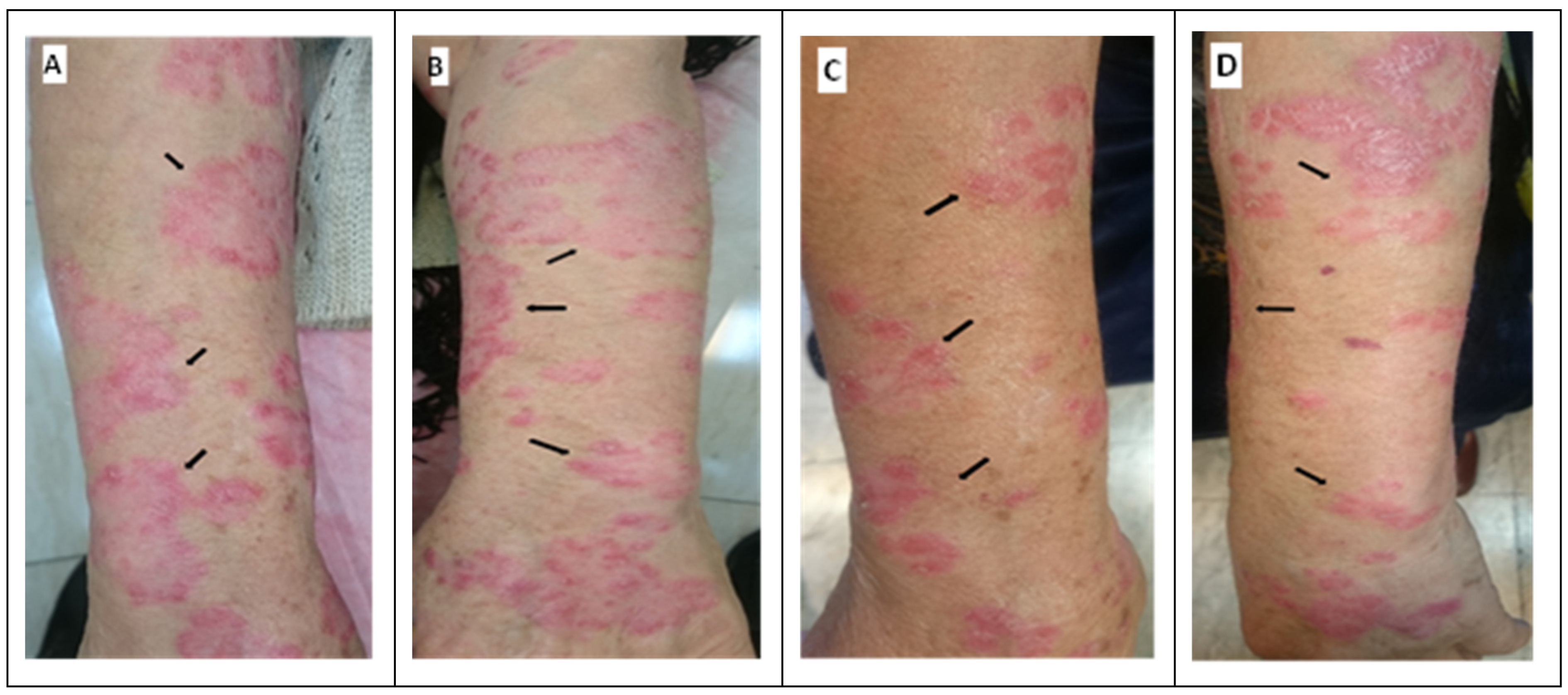
3.6. Clinical Observation of the Skin of PS Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raychaudhuri, S.K.; Maverakis, E.; Raychaudhuri, S.P. Diagnosis and classification of psoriasis. Autoimmun. Rev. 2014, 13, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.; Schäkel, K. Psoriasis pathogenesis and treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [PubMed]
- Bu, J.; Ding, R.; Zhou, L.; Chen, X.; Shen, E. Epidemiology of psoriasis and comorbid diseases: A narrative review. Front. Immunol. 2022, 13, 2484. [Google Scholar] [CrossRef] [PubMed]
- Gialouri, C.G.; Evangelatos, G.; Iliopoulos, A.; Tektonidou, M.G.; Sfikakis, P.P.; Fragoulis, G.E.; Nikiphorou, E. Late-Onset Psoriatic Arthritis: Are There Any Distinct Characteristics? A Retrospective Cohort Data Analysis. Life 2023, 13, 792. [Google Scholar] [CrossRef]
- Springate, D.; Parisi, R.; Kontopantelis, E.; Reeves, D.; Griffiths, C.; Ashcroft, D. Incidence, prevalence and mortality of patients with psoriasis: A UK population-based cohort study. Br. J. Dermatol. 2017, 176, 650–658. [Google Scholar] [CrossRef]
- Parisi, R.; Iskandar, I.Y.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.; Ashcroft, D.M. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Fontánez, N.; Soler, D.C.; McCormick, T.S. Current knowledge on psoriasis and autoimmune diseases. Psoriasis 2016, 6, 7. [Google Scholar]
- Kim, S.; Ryu, Y.W.; Kwon, J.I.; Choe, M.S.; Jung, J.W.; Cho, J.W. Differential expression of cyclin D1, Ki-67, pRb, and p53 in psoriatic skin lesions and normal skin. Mol. Med. Rep. 2018, 17, 735–742. [Google Scholar] [CrossRef]
- Nicolescu, A.C.; Ionescu, M.-A.; Constantin, M.M.; Ancuta, I.; Ionescu, S.; Niculet, E.; Tatu, A.L.; Zirpel, H.; Thaçi, D. Psoriasis Management Challenges Regarding Difficult-to-Treat Areas: Therapeutic Decision and Effectiveness. Life 2022, 12, 2050. [Google Scholar] [CrossRef] [PubMed]
- Balato, A.; Zink, A.; Babino, G.; Buononato, D.; Kiani, C.; Eyerich, K.; Ziehfreund, S.; Scala, E. The Impact of Psoriasis and Atopic Dermatitis on Quality of Life: A Literature Research on Biomarkers. Life 2022, 12, 2026. [Google Scholar] [CrossRef]
- Lin, A.M.; Rubin, C.J.; Khandpur, R.; Wang, J.Y.; Riblett, M.; Yalavarthi, S.; Villanueva, E.C.; Shah, P.; Kaplan, M.J.; Bruce, A.T. Mast cells and neutrophils release IL-17 through extracellular trap formation in psoriasis. J. Immunol. 2011, 187, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Stritesky, G.L.; Yeh, N.; Kaplan, M.H. IL-23 promotes maintenance but not commitment to the Th17 lineage. J. Immunol. 2008, 181, 5948–5955. [Google Scholar] [CrossRef] [PubMed]
- Bugaut, H.; Aractingi, S. Major role of the IL17/23 axis in psoriasis supports the development of new targeted therapies. Front. Immunol. 2021, 12, 621956. [Google Scholar] [CrossRef]
- Li, H.; Yao, Q.; Mariscal, A.G.; Wu, X.; Hülse, J.; Pedersen, E.; Helin, K.; Waisman, A.; Vinkel, C.; Thomsen, S.F. Epigenetic control of IL-23 expression in keratinocytes is important for chronic skin inflammation. Nat. Commun. 2018, 9, 1420. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Chen, Y.; Cui, L.; Shi, Y.; Guo, C. Advances in the pathogenesis of psoriasis: From keratinocyte perspective. Cell Death Dis. 2022, 13, 81. [Google Scholar] [CrossRef]
- Dyring-Andersen, B.; Honoré, T.V.; Madelung, A.; Bzorek, M.; Simonsen, S.; Clemmensen, S.N.; Clark, R.A.; Borregaard, N.; Skov, L. IL-17A and IL-22 producing neutrophils in psoriatic skin. Br. J. Dermatol. 2017, 177, e321. [Google Scholar] [CrossRef]
- Volpe, E.; Servant, N.; Zollinger, R.; Bogiatzi, S.I.; Hupé, P.; Barillot, E.; Soumelis, V. A critical function for transforming growth factor-β, interleukin 23 and proinflammatory cytokines in driving and modulating human TH-17 responses. Nat. Immunol. 2008, 9, 650–657. [Google Scholar] [CrossRef]
- Boniface, K.; Guignouard, E.; Pedretti, N.; Garcia, M.; Delwail, A.; Bernard, F.X.; Nau, F.; Guillet, G.; Dagregorio, G.; Yssel, H. A role for T cell-derived interleukin 22 in psoriatic skin inflammation. Clin. Exp. Immunol. 2007, 150, 407–415. [Google Scholar] [CrossRef]
- Moots, R.J.; Curiale, C.; Petersel, D.; Rolland, C.; Jones, H.; Mysler, E. Efficacy and safety outcomes for originator TNF inhibitors and biosimilars in rheumatoid arthritis and psoriasis trials: A systematic literature review. BioDrugs 2018, 32, 193–199. [Google Scholar] [CrossRef]
- Furue, M.; Furue, M. Interleukin-22 and keratinocytes; pathogenic implications in skin inflammation. Explor. Immunol. 2021, 1, 37–47. [Google Scholar] [CrossRef]
- Broome, A.-M.; Ryan, D.; Eckert, R.L. S100 protein subcellular localization during epidermal differentiation and psoriasis. J. Histochem. Cytochem. 2003, 51, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Hegyi, Z.; Zwicker, S.; Bureik, D.; Peric, M.; Koglin, S.; Batycka-Baran, A.; Prinz, J.C.; Ruzicka, T.; Schauber, J.; Wolf, R. Vitamin D analog calcipotriol suppresses the Th17 cytokine–induced proinflammatory S100 “alarmins” psoriasin (S100A7) and koebnerisin (S100A15) in psoriasis. J. Investig. Dermatol. 2012, 132, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Nograles, K.E.; Johnson-Huang, L.M.; Fuentes-Duculan, J.; Cardinale, I.; Bonifacio, K.M.; Gulati, N.; Mitsui, H.; Guttman-Yassky, E.; Suárez-Fariñas, M. IL-17 induces an expanded range of downstream genes in reconstituted human epidermis model. PLoS ONE 2014, 9, e90284. [Google Scholar] [CrossRef]
- Yang, D.; Han, Z.; Oppenheim, J.J. Alarmins and immunity. Immunol. Rev. 2017, 280, 41–56. [Google Scholar] [CrossRef]
- Furue, M.; Furue, K.; Tsuji, G.; Nakahara, T. Interleukin-17A and keratinocytes in psoriasis. Int. J. Mol. Sci. 2020, 21, 1275. [Google Scholar] [CrossRef] [PubMed]
- Wilsmann-Theis, D.; Wagenpfeil, J.; Holzinger, D.; Roth, J.; Koch, S.; Schnautz, S.; Bieber, T.; Wenzel, J. Among the S100 proteins, S100A12 is the most significant marker for psoriasis disease activity. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.B.; Jerome, D.; Yeung, J. Diagnosis and management of psoriasis. Can. Fam. Physician 2017, 63, 278–285. [Google Scholar]
- Carrascosa, J.M.; Theng, C.; Thaçi, D. Spotlight on Topical Long-Term Management of Plaque Psoriasis. Clin. Cosmet. Investig. Dermatol. 2020, 13, 495. [Google Scholar] [CrossRef]
- Barnes, L.; Kaya, G.; Rollason, V. Topical corticosteroid-induced skin atrophy: A comprehensive review. Drug Saf. 2015, 38, 493–509. [Google Scholar] [CrossRef]
- Brunner, K.; Oláh, P.; Moezzi, M.; Pár, G.; Vincze, Á.; Breitenbach, Z.; Gyulai, R. Association of nonalcoholic hepatic fibrosis with body composition in female and male psoriasis patients. Life 2021, 11, 763. [Google Scholar] [CrossRef]
- Dodero-Anillo, J.M.; Lozano-Cuadra, I.C.; Rios-Sanchez, E.; Pedrosa-Martinez, M.J.; Ruiz-Carrascosa, J.C.; Galan-Gutierrez, M.; Armario-Hita, J.C. Optimising the Therapeutic Interval for Biologics in Patients with Psoriasis. Life 2022, 12, 2075. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Gendrisch, F.; Schempp, C.M.; Wölfle, U. New herbal biomedicines for the topical treatment of dermatological disorders. Biomedicines 2020, 8, 27. [Google Scholar] [CrossRef]
- Olveira, A.; Augustin, S.; Benlloch, S.; Ampuero, J.; Suárez-Pérez, J.A.; Armesto, S.; Vilarrasa, E.; Belinchón-Romero, I.; Herranz, P.; Crespo, J. The Essential Role of IL-17 as the Pathogenetic Link between Psoriasis and Metabolic-Associated Fatty Liver Disease. Life 2023, 13, 419. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Su, X.; Liu, A.; Zhang, L.; Yu, A.; Xi, Y.; Zhai, G. Advances in clinical study of curcumin. Curr. Pharm. Des. 2013, 19, 1966–1973. [Google Scholar] [PubMed]
- Mahammedi, H.; Planchat, E.; Pouget, M.; Durando, X.; Curé, H.; Guy, L.; Van-Praagh, I.; Savareux, L.; Atger, M.; Bayet-Robert, M. The new combination docetaxel, prednisone and curcumin in patients with castration-resistant prostate cancer: A pilot phase II study. Oncology 2016, 90, 69–78. [Google Scholar] [CrossRef]
- Basu, P.; Dutta, S.; Begum, R.; Mittal, S.; Dutta, P.D.; Bharti, A.C.; Panda, C.K.; Biswas, J.; Dey, B.; Talwar, G.P. Clearance of cervical human papillomavirus infection by topical application of curcumin and curcumin containing polyherbal cream: A phase II randomized controlled study. Asian Pac. J. Cancer Prev. 2013, 14, 5753–5759. [Google Scholar] [CrossRef]
- Wongcharoen, W.; Jai-Aue, S.; Phrommintikul, A.; Nawarawong, W.; Woragidpoonpol, S.; Tepsuwan, T.; Sukonthasarn, A.; Apaijai, N.; Chattipakorn, N. Effects of curcuminoids on frequency of acute myocardial infarction after coronary artery bypass grafting. Am. J. Cardiol. 2012, 110, 40–44. [Google Scholar] [CrossRef]
- Cruz–Correa, M.; Shoskes, D.A.; Sanchez, P.; Zhao, R.; Hylind, L.M.; Wexner, S.D.; Giardiello, F.M. Combination treatment with curcumin and quercetin of adenomas in familial adenomatous polyposis. Clin. Gastroenterol. Hepatol. 2006, 4, 1035–1038. [Google Scholar] [CrossRef]
- Antiga, E.; Bonciolini, V.; Volpi, W.; Del Bianco, E.; Caproni, M. Oral curcumin (Meriva) is effective as an adjuvant treatment and is able to reduce IL-22 serum levels in patients with psoriasis vulgaris. BioMed Res. Int. 2015, 2015, 283634. [Google Scholar] [CrossRef]
- Kumar, A.; Harsha, C.; Parama, D.; Girisa, S.; Daimary, U.D.; Mao, X.; Kunnumakkara, A.B. Current clinical developments in curcumin-based therapeutics for cancer and chronic diseases. Phytother. Res. 2021, 35, 6768–6801. [Google Scholar] [CrossRef]
- Bahraini, P.; Rajabi, M.; Mansouri, P.; Sarafian, G.; Chalangari, R.; Azizian, Z. Turmeric tonic as a treatment in scalp psoriasis: A randomized placebo-control clinical trial. J. Cosmet. Dermatol. 2018, 17, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Bilia, A.R.; Bergonzi, M.C.; Isacchi, B.; Antiga, E.; Caproni, M. Curcumin nanoparticles potentiate therapeutic effectiveness of acitrein in moderate-to-severe psoriasis patients and control serum cholesterol levels. J. Pharm. Pharmacol. 2018, 70, 919–928. [Google Scholar] [CrossRef]
- Lee, G.; Chung, H.-S.; Lee, K.; Lee, H.; Kim, M.; Bae, H. Curcumin attenuates the scurfy-induced immune disorder, a model of IPEX syndrome, with inhibiting Th1/Th2/Th17 responses in mice. Phytomedicine 2017, 33, 1–6. [Google Scholar] [CrossRef]
- Umerska, A.; Gaucher, C.; Oyarzun-Ampuero, F.; Fries-Raeth, I.; Colin, F.; Villamizar-Sarmiento, M.G.; Maincent, P.; Sapin-Minet, A. Polymeric nanoparticles for increasing oral bioavailability of curcumin. Antioxidants 2018, 7, 46. [Google Scholar] [CrossRef]
- Shome, S.; Talukdar, A.D.; Choudhury, M.D.; Bhattacharya, M.K.; Upadhyaya, H. Curcumin as potential therapeutic natural product: A nanobiotechnological perspective. J. Pharm. Pharmacol. 2016, 68, 1481–1500. [Google Scholar] [CrossRef] [PubMed]
- Abd, E.; Namjoshi, S.; Mohammed, Y.H.; Roberts, M.S.; Grice, J.E. Synergistic skin penetration enhancer and nanoemulsion formulations promote the human epidermal permeation of caffeine and naproxen. J. Pharm. Sci. 2016, 105, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Hua, S. Lipid-based nano-delivery systems for skin delivery of drugs and bioactives. Front. Pharmacol. 2015, 6, 219. [Google Scholar] [CrossRef]
- Sohrabi, S.; Haeri, A.; Mahboubi, A.; Mortazavi, A.; Dadashzadeh, S. Chitosan gel-embedded moxifloxacin niosomes: An efficient antimicrobial hybrid system for burn infection. Int. J. Biol. Macromol. 2016, 85, 625–633. [Google Scholar] [CrossRef]
- Kumar, N.; Goindi, S. Statistically designed nonionic surfactant vesicles for dermal delivery of itraconazole: Characterization and in vivo evaluation using a standardized Tinea pedis infection model. Int. J. Pharm. 2014, 472, 224–240. [Google Scholar] [CrossRef]
- Handjani-Vila, R.; Ribier, A.; Rondot, B.; Vanlerberghie, G. Dispersions of lamellar phases of non-ionic lipids in cosmetic products. Int. J. Cosmet. Sci. 1979, 1, 303–314. [Google Scholar] [CrossRef]
- Brown, M.B.; Jones, S.A. Hyaluronic acid: A unique topical vehicle for the localized delivery of drugs to the skin. J. Eur. Acad. Dermatol. Venereol. 2005, 19, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Xu, C.; Zhao, X.; Lin, C.; Yang, X.; Xin, X.; Zhang, L.; Qin, C.; Han, X.; Yang, L. Nanoplatform assembled from a CD44-targeted prodrug and smart liposomes for dual targeting of tumor microenvironment and cancer cells. ACS Nano 2018, 12, 1519–1536. [Google Scholar] [CrossRef]
- Yeo, L.K.; Chaw, C.S.; Elkordy, A.A. The effects of hydration parameters and co-surfactants on methylene blue-loaded niosomes prepared by the thin film hydration method. Pharmaceuticals 2019, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Hasani, M.; Sani, N.A.; Khodabakhshi, B.; Arabi, M.S.; Mohammadi, S.; Yazdani, Y. Encapsulation of Leflunomide (LFD) in a novel niosomal formulation facilitated its delivery to THP-1 monocytic cells and enhanced Aryl hydrocarbon receptor (AhR) nuclear translocation and activation. DARU J. Pharm. Sci. 2019, 27, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Langley, R.G.; Ellis, C.N. Evaluating psoriasis with psoriasis area and severity index, psoriasis global assessment, and lattice system physician’s global assessment. J. Am. Acad. Dermatol. 2004, 51, 563–569. [Google Scholar] [CrossRef]
- Mohammadi, S.; Sedighi, S.; Memarian, A. IL-17 is aberrantly overexpressed among under-treatment systemic lupus erythematosus patients. Iran. J. Pathol. 2019, 14, 236. [Google Scholar] [CrossRef]
- Campbell, N.K.; Fitzgerald, H.K.; Malara, A.; Hambly, R.; Sweeney, C.M.; Kirby, B.; Fletcher, J.M.; Dunne, A. Naturally derived Heme-Oxygenase 1 inducers attenuate inflammatory responses in human dendritic cells and T cells: Relevance for psoriasis treatment. Sci. Rep. 2018, 8, 10287. [Google Scholar] [CrossRef]
- Mohammadi, S.; Sedighi, S.; Memarian, A.; Yazdani, Y. Overexpression of interferon-γ and indoleamine 2, 3-dioxygenase in systemic lupus erythematosus: Relationship with the disease activity. LaboratoriumsMedizin 2017, 41, 41–47. [Google Scholar] [CrossRef]
- Jhaj, R.; Asati, D.P.; Chaudhary, D.; Sadasivam, B. Topical steroid containing combinations: Burden of adverse effects and why the recent regulatory action may not be enough. Indian J. Pharmacol. 2021, 53, 371. [Google Scholar]
- Seminara, N.; Abuabara, K.; Shin, D.; Langan, S.; Kimmel, S.; Margolis, D.; Troxel, A.; Gelfand, J. Validity of The Health Improvement Network (THIN) for the study of psoriasis. Br. J. Dermatol. 2011, 164, 602–609. [Google Scholar] [CrossRef]
- Mollazadeh, H.; Cicero, A.F.; Blesso, C.N.; Pirro, M.; Majeed, M.; Sahebkar, A. Immune modulation by curcumin: The role of interleukin-10. Crit. Rev. Food Sci. Nutr. 2019, 59, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Thangapazham, R.L.; Sharma, A.; Maheshwari, R.K. Beneficial role of curcumin in skin diseases. In Molecular Targets and Therapeutic Uses of Curcumin in Health and Disease; Springer: Boston, MA, USA, 2007; pp. 343–357. [Google Scholar]
- Kang, D.; Li, B.; Luo, L.; Jiang, W.; Lu, Q.; Rong, M.; Lai, R. Curcumin shows excellent therapeutic effect on psoriasis in mouse model. Biochimie 2016, 123, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Kurd, S.K.; Smith, N.; VanVoorhees, A.; Troxel, A.B.; Badmaev, V.; Seykora, J.T.; Gelfand, J.M. Oral curcumin in the treatment of moderate to severe psoriasis vulgaris: A prospective clinical trial. J. Am. Acad. Dermatol. 2008, 58, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Sarafian, G.; Afshar, M.; Mansouri, P.; Asgarpanah, J.; Raoufinejad, K.; Rajabi, M. Topical Turmeric Microemulgel in the Management of Plaque Psoriasis; A Clinical Evaluation. Iran. J. Pharm. Res. 2015, 14, 865–876. [Google Scholar] [PubMed]
- Varma, S.R.; Sivaprakasam, T.O.; Mishra, A.; Prabhu, S.; Rafiq, M.; Rangesh, P. Imiquimod-induced psoriasis-like inflammation in differentiated Human keratinocytes: Its evaluation using curcumin. Eur. J. Pharmacol. 2017, 813, 33–41. [Google Scholar] [CrossRef]
- Jain, A.; Doppalapudi, S.; Domb, A.J.; Khan, W. Tacrolimus and curcumin co-loaded liposphere gel: Synergistic combination towards management of psoriasis. J. Control. Release 2016, 243, 132–145. [Google Scholar] [CrossRef]
- Sun, L.; Liu, Z.; Wang, L.; Cun, D.; Tong, H.H.; Yan, R.; Chen, X.; Wang, R.; Zheng, Y. Enhanced topical penetration, system exposure and anti-psoriasis activity of two particle-sized, curcumin-loaded PLGA nanoparticles in hydrogel. J. Control. Release 2017, 254, 44–54. [Google Scholar] [CrossRef]
- Reena, K.; Singh, L.; Sharma, S. Curcumin: A Review of its’ Efficacy in the Management of Psoriasis. Drug Deliv. Lett. 2022, 12, 163–183. [Google Scholar] [CrossRef]
- Raja, M.A.; Zeenat, S.; Arif, M.; Liu, C. Self-assembled nanoparticles based on amphiphilic chitosan derivative and arginine for oral curcumin delivery. Int. J. Nanomed. 2016, 11, 4397. [Google Scholar] [CrossRef]
- Algahtani, M.S.; Ahmad, M.Z.; Ahmad, J. Nanoemulsion loaded polymeric hydrogel for topical delivery of curcumin in psoriasis. J. Drug Deliv. Sci. Technol. 2020, 59, 101847. [Google Scholar] [CrossRef]
- Patel, N.A.; Patel, N.J.; Patel, R.P. Formulation and evaluation of curcumin gel for topical application. Pharm. Dev. Technol. 2009, 14, 83–92. [Google Scholar] [CrossRef]
- Sharma, R.; Dua, J.; Parsad, D. An overview on Niosomes: Novel Pharmaceutical drug delivery system. J. Drug Deliv. Ther. 2022, 12, 171–177. [Google Scholar] [CrossRef]
- Shah, A.; Boldhane, S.; Pawar, A.; Bothiraja, C. Advanced development of a non-ionic surfactant and cholesterol material based niosomal gel formulation for the topical delivery of anti-acne drugs. Mater. Adv. 2020, 1, 1763–1774. [Google Scholar] [CrossRef]
- Abdelbary, A.A.; AbouGhaly, M.H. Design and optimization of topical methotrexate loaded niosomes for enhanced management of psoriasis: Application of Box–Behnken design, in-vitro evaluation and in-vivo skin deposition study. Int. J. Pharm. 2015, 485, 235–243. [Google Scholar] [CrossRef]
- Fernández, T.D.; Pearson, J.R.; Leal, M.P.; Torres, M.J.; Blanca, M.; Mayorga, C.; Le Guével, X. Intracellular accumulation and immunological properties of fluorescent gold nanoclusters in human dendritic cells. Biomaterials 2015, 43, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Park, H.; Feng, C.; Hou, L.; Cheng, X.; Chen, X. Construction of hyaluronic acid noisome as functional transdermal nanocarrier for tumor therapy. Carbohydr. Polym. 2013, 94, 634–641. [Google Scholar] [CrossRef]
- Brück, J.; Holstein, J.; Glocova, I.; Seidel, U.; Geisel, J.; Kanno, T.; Kumagai, J.; Mato, N.; Sudowe, S.; Widmaier, K. Nutritional control of IL-23/Th17-mediated autoimmune disease through HO-1/STAT3 activation. Sci. Rep. 2017, 7, 44482. [Google Scholar] [CrossRef]
- Skyvalidas, D.Ν.; Mavropoulos, A.; Tsiogkas, S.; Dardiotis, E.; Liaskos, C.; Mamuris, Z.; Roussaki-Schulze, A.; Sakkas, L.I.; Zafiriou, E.; Bogdanos, D.P. Curcumin mediates attenuation of pro-inflammatory interferon γ and interleukin 17 cytokine responses in psoriatic disease, strengthening its role as a dietary immunosuppressant. Nutr. Res. 2020, 75, 95–108. [Google Scholar] [CrossRef]
- Sun, J.; Zhao, Y.; Hu, J. Curcumin inhibits imiquimod-induced psoriasis-like inflammation by inhibiting IL-1beta and IL-6 production in mice. PLoS ONE 2013, 8, e67078. [Google Scholar] [CrossRef]
- Pol, A.; Bergers, M.; Schalkwijk, J. Comparison of antiproliferative effects of experimental and established antipsoriatic drugs on human kerationocytes, using a simple 96-well-plate assay. Vitr. Cell. Dev. Biol.-Anim. 2003, 39, 36–42. [Google Scholar] [CrossRef]
- Guilloteau, K.; Paris, I.; Pedretti, N.; Boniface, K.; Juchaux, F.; Huguier, V.; Guillet, G.; Bernard, F.-X.; Lecron, J.-C.; Morel, F. Skin inflammation induced by the synergistic action of IL-17A, IL-22, oncostatin M, IL-1α, and TNF-α recapitulates some features of psoriasis. J. Immunol. 2010, 184, 5263–5270. [Google Scholar] [CrossRef] [PubMed]
- Granata, M.; Skarmoutsou, E.; Mazzarino, M.C.; D’Amico, F. S100A7 in psoriasis: Immunodetection and activation by CRISPR technology. In Calcium-Binding Proteins of the EF-Hand Superfamily; Springer: Berlin/Heidelberg, Germany, 2019; pp. 729–738. [Google Scholar]
- Lin, J.; Tang, Y.; Kang, Q.; Feng, Y.; Chen, A. Curcumin inhibits gene expression of receptor for advanced glycation end-products (RAGE) in hepatic stellate cells in vitro by elevating PPARγ activity and attenuating oxidative stress. Br. J. Pharmacol. 2012, 166, 2212–2227. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Plus (5′ > 3′) | Minus (5′ > 3′) | Product (bp) | Tm | |
|---|---|---|---|---|---|
| 1 | IL23A | TCAGGCTCAAAGCAAGTGGA | AGCAGCAACAGCAGCATTAC | 128 | 60 |
| 2 | IL17A | CGCAATGAGGACCCTGAGAG | TAGTCCACGTTCCCATCAGC | 92 | 60 |
| 3 | IL22 | AGCCCTATATCACCAACCGC | TCTCCCCAATGAGACGAACG | 87 | 60 |
| 4 | TNFα | CATCCAACCTTCCCAAACGC | CTGTAGGCCCCAGTGAGTTC | 246 | 60 |
| 5 | S100A7 | CACTCAAGCTGAGAGGTCCAT | AAAGACATCGGCGAGGTAATTTG | 169 | 60 |
| 6 | S100A12 | ACCACTGCTGGCTTTTTGCT | GGGTGTCAAAATGCCCCTTC | 150 | 60 |
| 7 | Ki67 | TCTGTTATTGATGAGCCTGTA | GTTGACTTCCTTCCATTCTG | 107 | 58 |
| 8 | 18srRNA | ACCCGTTGAACCCCATTCGTGA | GCCTCACTAAACCATCCAATCGG | 159 | 60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolahdooz, H.; Khori, V.; Erfani-Moghadam, V.; Livani, F.; Mohammadi, S.; Memarian, A. Niosomal Curcumin Suppresses IL17/IL23 Immunopathogenic Axis in Skin Lesions of Psoriatic Patients: A Pilot Randomized Controlled Trial. Life 2023, 13, 1076. https://doi.org/10.3390/life13051076
Kolahdooz H, Khori V, Erfani-Moghadam V, Livani F, Mohammadi S, Memarian A. Niosomal Curcumin Suppresses IL17/IL23 Immunopathogenic Axis in Skin Lesions of Psoriatic Patients: A Pilot Randomized Controlled Trial. Life. 2023; 13(5):1076. https://doi.org/10.3390/life13051076
Chicago/Turabian StyleKolahdooz, Hanieh, Vahid Khori, Vahid Erfani-Moghadam, Fatemeh Livani, Saeed Mohammadi, and Ali Memarian. 2023. "Niosomal Curcumin Suppresses IL17/IL23 Immunopathogenic Axis in Skin Lesions of Psoriatic Patients: A Pilot Randomized Controlled Trial" Life 13, no. 5: 1076. https://doi.org/10.3390/life13051076