
Immunohistochemical Analysis of Adhesion Molecules E-Selectin, Intercellular Adhesion Molecule-1, and Vascular Cell Adhesion Molecule-1 in Inflammatory Lesions of Atopic Dermatitis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
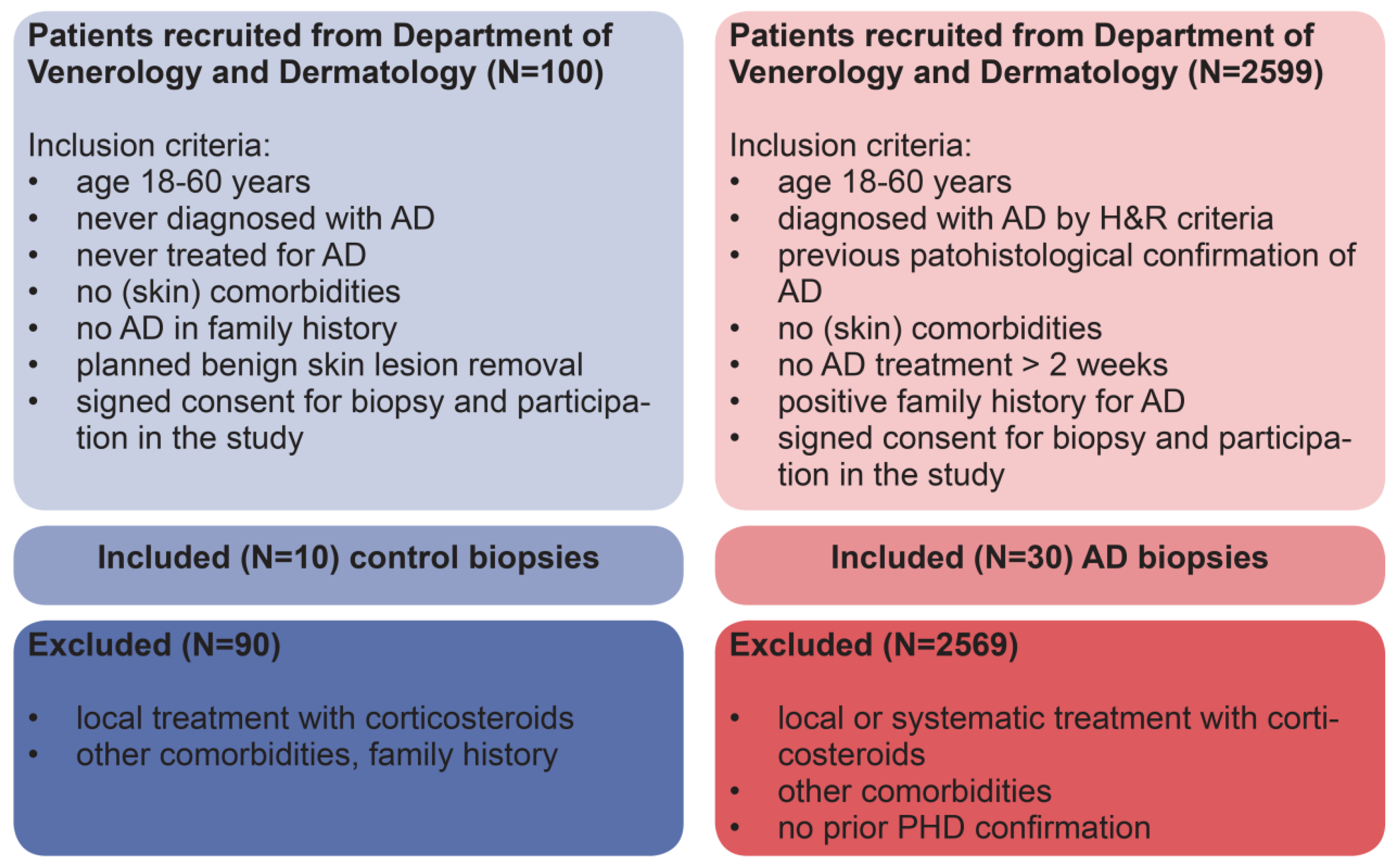
2.1. Biopsy Specimens (Patients)
2.2. Immunohistochemistry
2.3. Quantitative and Qualitative Staining Measurements
2.4. Biopsy Specimens (Patients)
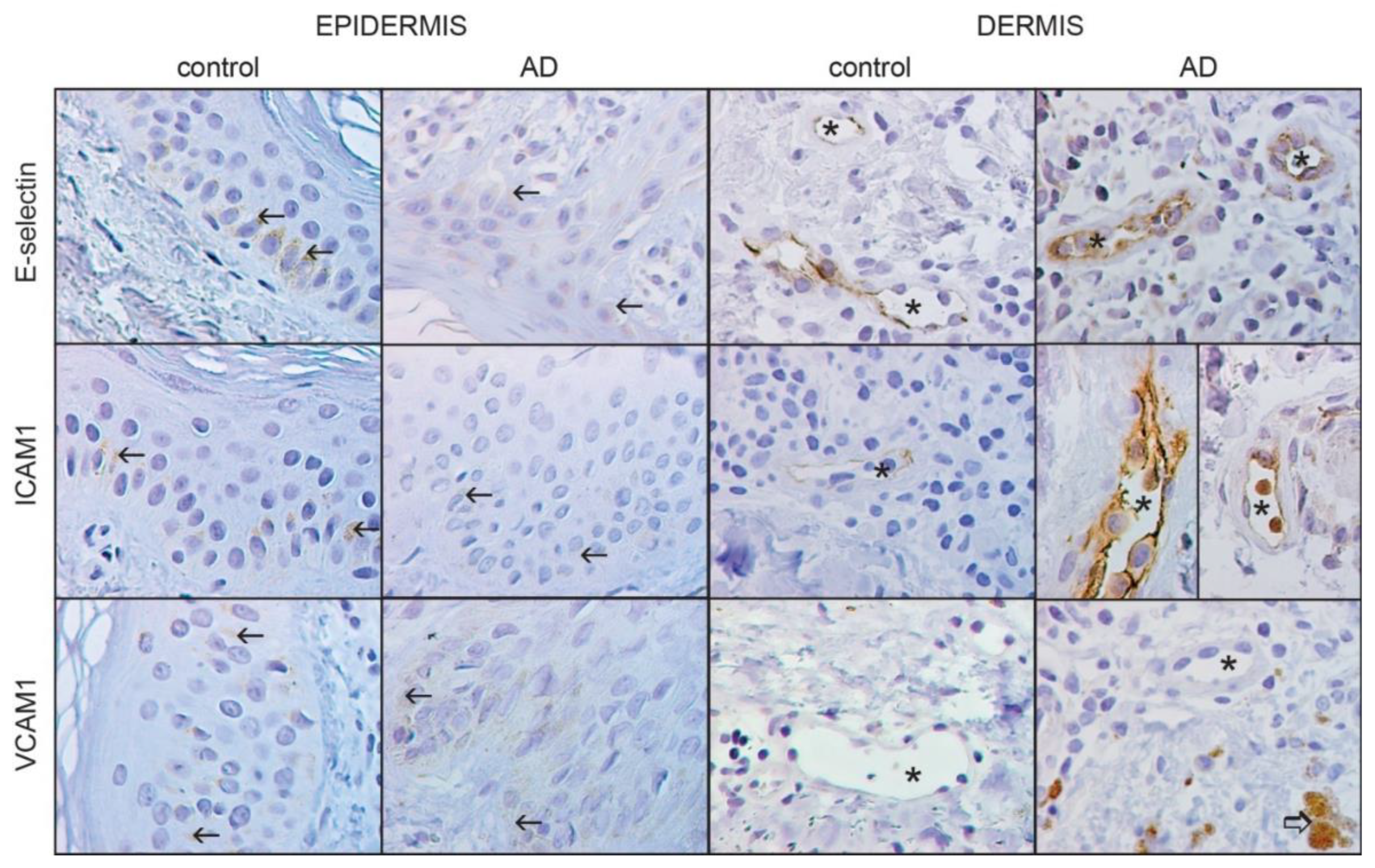
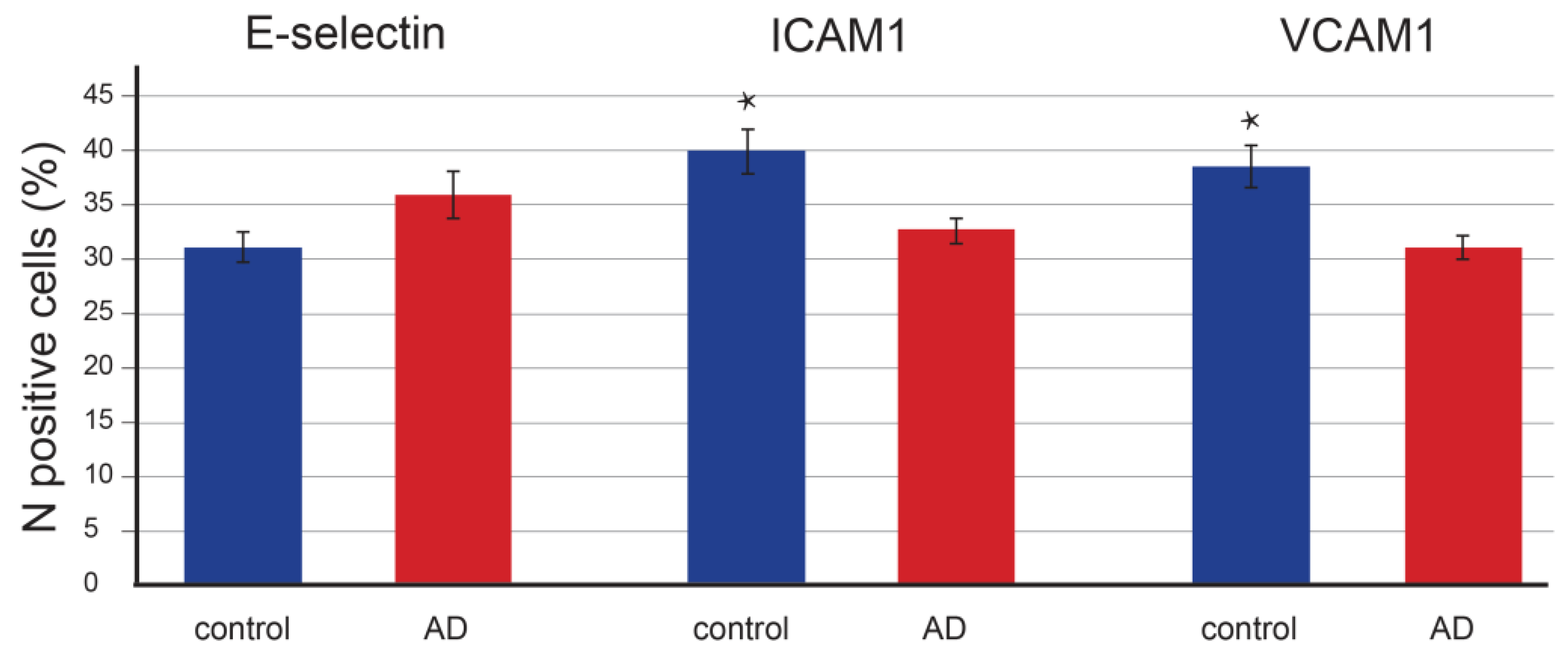
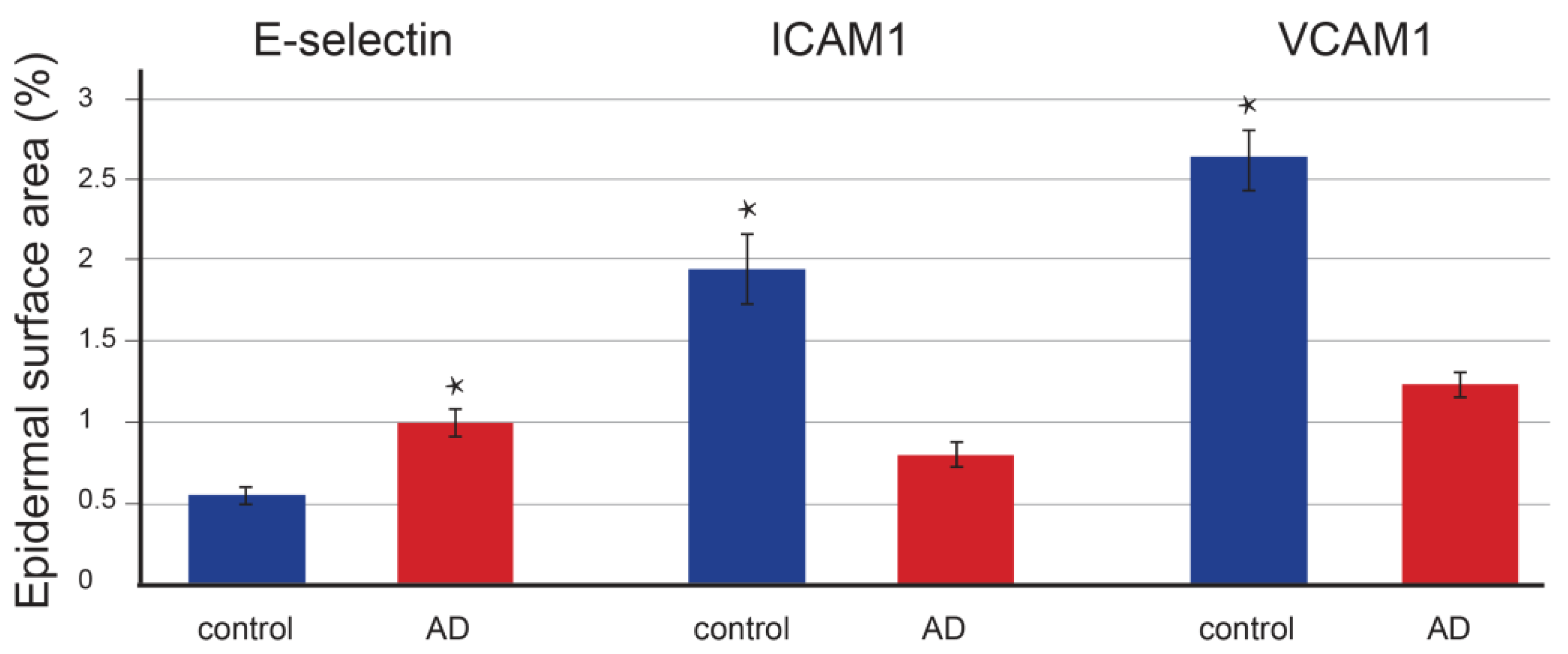
3. Results
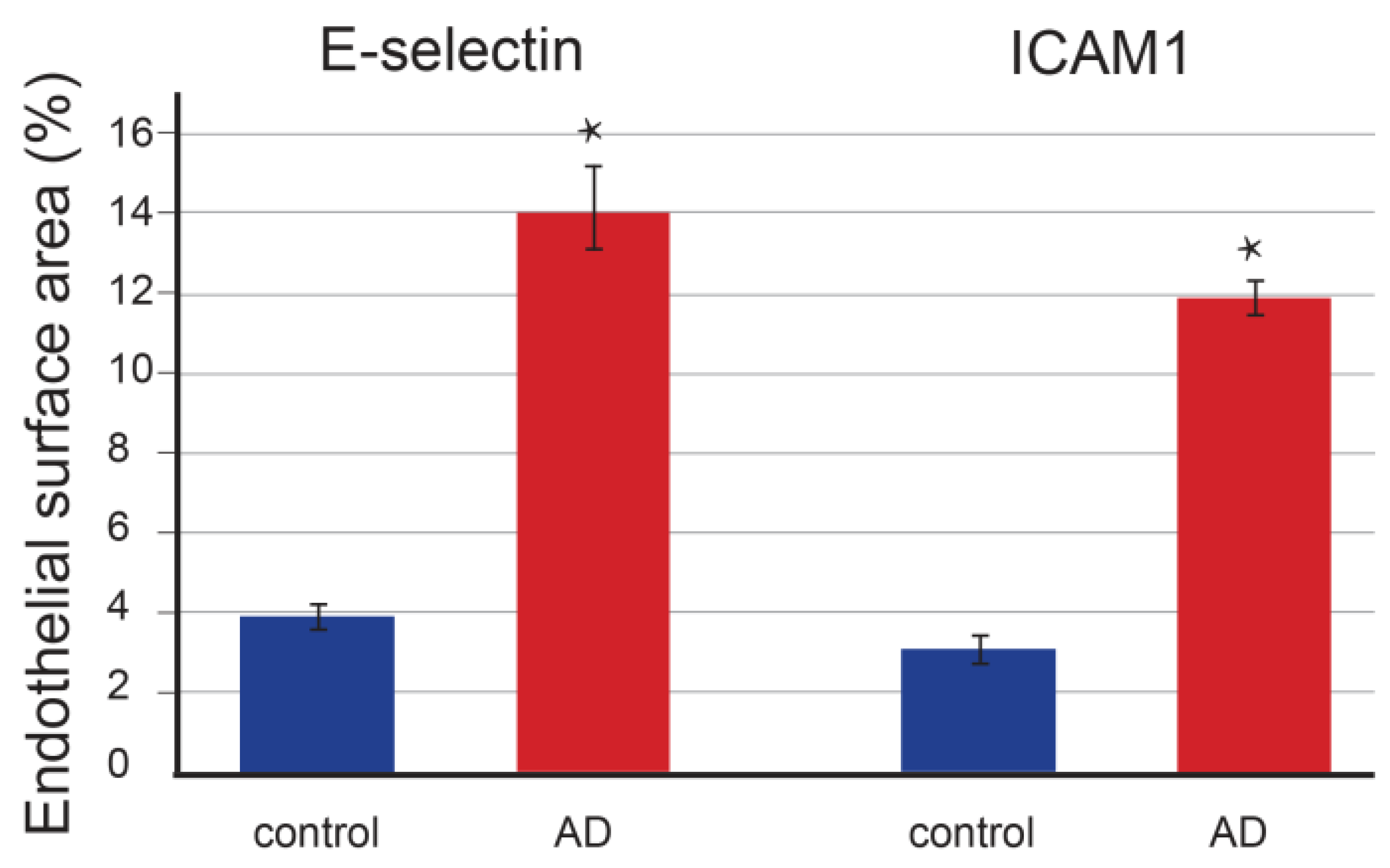
3.1. E-Selectin
3.2. ICAM-1
3.3. VCAM-1
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Patel, N.; Immaneni, S.; Rusniak, B.; Silverberg, N.B.; Debashis, R.; Fewkes, N.; Simpson, E.L. Assessment of atopic dermatitis using self-report and caregiver report: A multicentre validation study. Br. J. Dermatol. 2015, 173, 1400–1404. [Google Scholar] [CrossRef] [Green Version]
- Lugović, L.; Lipozenčić, J.C.A. Are respiratory allergic diseases related to atopic dermatitis? Coll. Antropol. 2000, 24, 11. [Google Scholar]
- Sohn, A.; Frankel, A.; Patel, R.V.; Goldenberg, G. Eczema. Mt. Sinai J. Med. 2011, 78, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Chiesa Fuxench, Z.C.; Block, J.K.; Boguniewicz, M.; Boyle, J.; Fonacier, L.; Gelfand, J.M.; Grayson, M.H.; Margolis, D.J.; Mitchell, L.; Silverberg, J.I.; et al. Atopic dermatitis in America study: A cross-sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J. Investig. Dermatol. 2019, 139, 583–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverberg, J.I. Public health burden and epidemiology of atopic dermatitis. Dermatol. Clin. 2017, 35, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Langan, S.; Deckert, S.; Svensson, A.; von Kobyletzki, L.; Thomas, K.; Spuls, P. Assessment of clinical signs of atopic dermatitis: A systematic review and recommendation. J. Allergy Clin. Immunol. 2013, 132, 1337–1347. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm. Venereol. 1980, 92, 4. [Google Scholar] [CrossRef]
- Kim, K.H. Overview of atopic dermatitis. Asia Pac. Allergy 2013, 3, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Gu, H.; Chen, X.S.; Chen, K.; Yan, Y.; Jing, H.; Chen, X.Q.; Shao, C.G.; Ye, G.Y. Evaluation of diagnostic criteria for atopic dermatitis: Validity of the criteria of Williams et al. in a hospital-based setting. Br. J. Dermatol. 2001, 145, 428–433. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Tom, W.L.; Chamlin, S.L.; Feldman, S.R.; Hanifin, J.M.; Simpson, E.L.; Berger, T.G.; Bergman, J.N.; Cohen, D.E.; Cooper, K.D.; et al. Guidelines of care for the management of atopic dermatitis: Section 1. Diagnosis and assessment of atopic dermatitis. J. Am. Acad. Dermatol. 2014, 70, 338–351. [Google Scholar] [CrossRef] [Green Version]
- Jurakić Tončić, R.; Marinović, B. The role of impaired epidermal barrier function in atopic dermatitis. Acta Dermatovenerol. Croat. 2016, 24, 95–109. [Google Scholar]
- Bin, L.; Leung, D.Y.M. Genetic and epigenetic studies of atopic dermatitis. Allergy Asthma Clin. Immunol. 2016, 12, 52. [Google Scholar] [CrossRef] [Green Version]
- Brunner, P.M.; Emerson, R.O.; Tipton, C.; Garcet, S.; Khattri, S.; Coats, I.; Krueger, J.G.; Guttman-Yassky, E. Nonlesional atopic dermatitis skin shares similar T-cell clones with lesional tissues. Allergy 2017, 72, 2017–2025. [Google Scholar] [CrossRef] [PubMed]
- Tokura, Y. Extrinsic and intrinsic types of atopic dermatitis. J. Dermatol. Sci. 2010, 58, 6. [Google Scholar] [CrossRef]
- Fölster-Holst, R.; Pape, M.; Buss, Y.L.; Christophers, E.; Weichenthal, M. Low prevalence of the intrinsic form of atopic dermatitis among adult patients. Allergy 2006, 61, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Drislane, C.; Irvine, A.D. The role of filaggrin in atopic dermatitis and allergic disease. Ann. Allergy Asthma Immunol. 2020, 124, 36–43. [Google Scholar] [CrossRef] [Green Version]
- Palmer, C.N.; Irvine, A.D.; Terron-Kwiatkowski, A.; Zhao, Y.; Liao, H.; Lee, S.P.; Goudie, D.R.; Sandilands, A.; Campbell, L.E.; Smith, F.J.; et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat. Genet. 2006, 38, 441–446. [Google Scholar] [CrossRef]
- Lugović, L.; Cupić, H.; Lipozencić, J.; Jakić-Razumović, J. The role of adhesion molecules in atopic dermatitis. Acta Dermatovenerol. Croat. 2006, 14, 2–7. [Google Scholar] [PubMed]
- Sigurdsson, V.; de Vries, I.J.; Toonstra, J.; Bihari, I.C.; Thepen, T.; Bruijnzeel-Koomen, C.A.; van Vloten, W.A. Expression of VCAM-1, ICAM-1, E-selectin, and P-selectin on endothelium in situ in patients with erythroderma, mycosis fungoides and atopic dermatitis. J. Cutan. Pathol. 2000, 27, 436–440. [Google Scholar] [CrossRef]
- Tatu, A.L.; Nadasdy, S.T.; Arbune, S.A.; Chioncel, S.V.; Bobeica, S.C.; Niculet, E.; Iancu, S.A.V.; Dumitru, C.; Popa, V.T.; Kluger, S.N.; et al. Interrelationship and sequencing of interleukins 4, 13, 31, and 33: An integrated systematic review: Dermatological and multidisciplinary perspectives. J. Inflamm. Res. 2022, 15, 5163–5184. [Google Scholar] [CrossRef] [PubMed]
- Foti, C.; Romita, P.; Ambrogio, F.; Manno, C.; Filotico, R.; Cassano, N.; Vena, G.A.; De Marco, A.; Cazzato, G.; Mennuni, B.G. Treatment of severe atopic dermatitis with dupilumab in three patients with renal diseases. Life 2022, 12, 2002. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Newman, W.; Gopal, T.V.; Horgan, K.J.; Graber, N.; Beall, L.D.; van Seventer, G.A.; Shaw, S. Four molecular pathways of T-cell adhesion to endothelial cells: Roles of LFA-1, VCAM-1, and ELAM-1 and changes in pathway hierarchy under different activation conditions. J. Cell Biol. 1991, 113, 1203–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wüthrich, B.; Joller-Jemelka, H.; Kägi, M.K. Levels of soluble ICAM-1 in atopic dermatitis. A new marker for monitoring the clinical activity? Allergy 1995, 50, 88–89. [Google Scholar] [CrossRef]
- Jung, K.; Linse, F.; Heller, R.; Moths, C.; Goebel, R.; Neumann, C. Adhesion molecules in atopic dermatitis: VCAM-1 and ICAM-1 expression is increased in healthy-appearing skin. Allergy 1996, 51, 452–460. [Google Scholar] [CrossRef]
- Koide, M.; Furukawa, F.; Tokura, Y.; Shirahama, S.; Takigawa, M. Evaluation of soluble cell adhesion molecules in atopic dermatitis. J. Dermatol. 1997, 24, 88–93. [Google Scholar] [CrossRef]
- Yusuf-Makagiansar, H.; Anderson, M.E.; Yakovleva, T.V.; Murray, J.S.; Siahaan, T.J. Inhibition of LFA-1/ICAM-1 and VLA-4/VCAM-1 as a therapeutic approach to inflammation and autoimmune diseases. Med. Res. Rev. 2002, 22, 146–167. [Google Scholar] [CrossRef]
- Wolkerstorfer, A.; Savelkoul, H.F.; de Waard van der Spek, F.B.; Neijens, H.J.; van Meurs, T.; Oranje, A.P. Soluble E-selectin and soluble ICAM-1 levels as markers of the activity of atopic dermatitis in children. Pediatr. Allergy Immunol. 2003, 14, 302–306. [Google Scholar] [CrossRef]
- Lawson, C.; Wolf, S. ICAM-1 signaling in endothelial cells. Pharmacol. Rep. 2009, 61, 22–32. [Google Scholar] [CrossRef]
- Chen, Q.; Massagué, J. Molecular Pathways: VCAM-1 as a potential therapeutic target in metastasis. Clin. Cancer Res. 2012, 18, 5520–5525. [Google Scholar] [CrossRef] [Green Version]
- Telen, M.J. Cellular adhesion and the endothelium: E-selectin, L-selectin, and pan-selectin inhibitors. Hematol. Oncol. Clin. N. Am. 2014, 28, 341–354. [Google Scholar] [CrossRef]
- Yamashita, N.; Kaneko, S.; Kouro, O.; Furue, M.; Yamamoto, S.; Sakane, T. Soluble E-selectin as a marker of disease activity in atopic dermatitis. J. Allergy Clin. Immunol. 1997, 99, 410–416. [Google Scholar] [CrossRef]
- Käßmeyer, S.; Plendl, J.; Custodis, P.; Bahramsoltani, M. New insights in vascular development: Vasculogenesis and endothelial progenitor cells. Anat. Histol. Embryol. 2009, 38, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wierenga, E.A.; Snoek, M.; Jansen, H.M.; Bos, J.D.; van Lier, R.A.; Kapsenberg, M.L. Human atopen-specific types 1 and 2 T helper cell clones. J. Immunol. 1991, 147, 2942–2949. [Google Scholar] [CrossRef] [PubMed]
- Bos, J.D.; Kapsenberg, M.L.; Smitt, J.H. Pathogenesis of atopic eczema. Lancet 1994, 343, 1338–1341. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lin, S.X.; Amin, S.; Overbergh, L.; Maggiolino, G.; Chan, L.S. VCAM-1 blockade delays disease onset, reduces disease severity and inflammatory cells in an atopic dermatitis model. Immunol. Cell Biol. 2010, 88, 334–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antiga, E.; Volpi, W.; Torchia, D.; Fabbri, P.; Caproni, M. Effects of tacrolimus ointment on Toll-like receptors in atopic dermatitis. Clin. Exp. Derm. 2011, 36, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Philips, B.; Thornton, H. The 2011 Oxford CEBM Evidence Levels of Evidence (Introductory Document); Oxford Centre for Evidence-Based Medicine: Oxford, UK, 2011; Available online: http://www.cebm.net/index.aspx?o=5653 (accessed on 18 January 2022).
- Kamp, S.; Balkert, L.S.; Stenderup, K.; Rosada, C.; Pakkenberg, B.; Kemp, K.; Jemec, G.B.; Dam, T.N. Stereological estimation of epidermal volumes and dermo-epidermal surface area in normal skin. Dermatology 2011, 223, 131–139. [Google Scholar] [CrossRef]
- Fedchenko, N.; Reifenrath, J. Different approaches for interpretation and reporting of immunohistochemistry analysis results in the bone tissue—A review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef] [Green Version]
- Zou, Z.; Liu, S.; An, J.; Huang, Y.; Sun, D.; Shen, H. Stereological study of epidermis in human skin grafts on nude athymic mice. Anal. Quant. Cytol. Histol. 2017, 39, 7. [Google Scholar]
- Caproni, M.; Volpi, W.; Giomi, B.; Torchia, D.; Del Bianco, E.; Fabbri, P. Cellular adhesion molecules in chronic urticaria: Modulation of serum levels occurs during levocetirizine treatment. Br. J. Dermatol. 2006, 155, 1270–1274. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Atopic Dermatitis | Controls | |
|---|---|---|
| N | 30 | 10 |
| N females | 21 | 5 |
| N males | 9 | 5 |
| age | 28–45 | 24–32 |
| mean age | 32 | 28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marinović Kulišić, S.; Takahashi, M.; Himelreich Perić, M.; Mužić Radović, V.; Jurakić Tončić, R. Immunohistochemical Analysis of Adhesion Molecules E-Selectin, Intercellular Adhesion Molecule-1, and Vascular Cell Adhesion Molecule-1 in Inflammatory Lesions of Atopic Dermatitis. Life 2023, 13, 933. https://doi.org/10.3390/life13040933
Marinović Kulišić S, Takahashi M, Himelreich Perić M, Mužić Radović V, Jurakić Tončić R. Immunohistochemical Analysis of Adhesion Molecules E-Selectin, Intercellular Adhesion Molecule-1, and Vascular Cell Adhesion Molecule-1 in Inflammatory Lesions of Atopic Dermatitis. Life. 2023; 13(4):933. https://doi.org/10.3390/life13040933
Chicago/Turabian StyleMarinović Kulišić, Sandra, Marta Takahashi, Marta Himelreich Perić, Vedrana Mužić Radović, and Ružica Jurakić Tončić. 2023. "Immunohistochemical Analysis of Adhesion Molecules E-Selectin, Intercellular Adhesion Molecule-1, and Vascular Cell Adhesion Molecule-1 in Inflammatory Lesions of Atopic Dermatitis" Life 13, no. 4: 933. https://doi.org/10.3390/life13040933