
Anatomical and Functional Outcomes after Endoresection and Adjuvant Ruthenium Brachytherapy for Uveal Melanoma: A Single-Center Experience
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
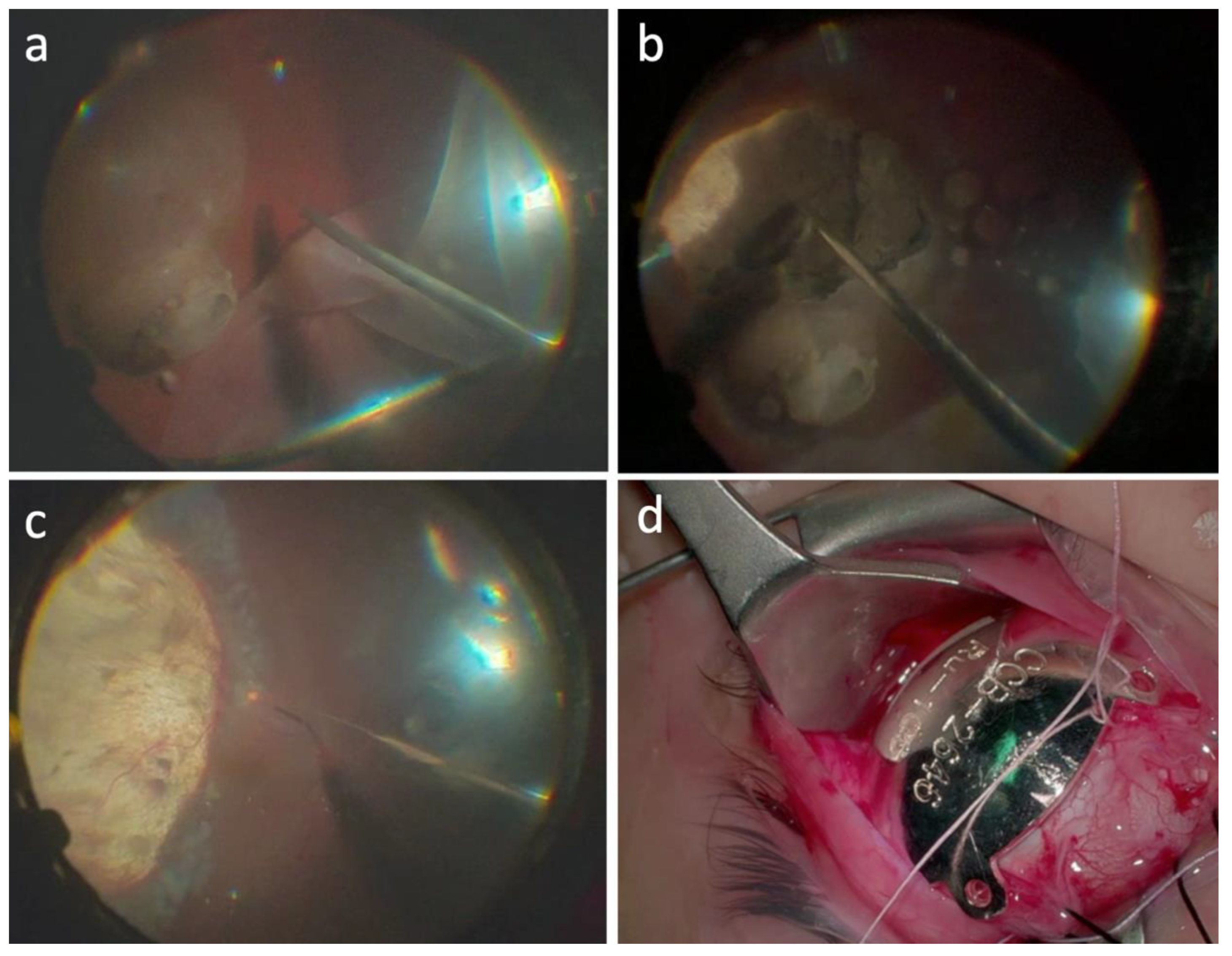
Surgical Procedure
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Treatment Outcomes
3.3. Histophatological and Cytogenetic Analysis
3.4. Treatment Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virgili, G.; Gatta, G.; Ciccolallo, L.; Capocaccia, R.; Biggeri, A.; Crocetti, E.; Lutz, J.-M.; Paci, E. Incidence of uveal melanoma in Europe. Ophthalmology 2007, 114, 2309–2315. [Google Scholar] [CrossRef] [PubMed]
- Krantz, B.A.; Dave, N.; Komatsubara, K.M.; Marr, B.P.; Carvajal, R.D. Uveal melanoma: Epidemiology, etiology, and treatment of primary disease. Clin. Ophthalmol. 2017, 11, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Manson, D.K.; Marr, B.P.; Carvajal, R.D. Treatment of uveal melanoma: Where are we now? Ther. Adv. Med. Oncol. 2018, 10, 1758834018757175. [Google Scholar] [CrossRef]
- Collaborative Ocular Melanoma Study Group. Assessment of metastatic disease status at death in 435 patients with large choroidal melanoma in the Collaborative Ocular Melanoma Study (COMS): COMS report no. 15. Arch. Ophthalmol. 2001, 119, 670–676. [Google Scholar] [CrossRef]
- Collaborative ocular Melanoma Study Group. The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma: V. Twelve-year mortality rates and prognostic factors:COMS report No. 28. Arch. Ophthalmol. 2006, 124, 1684–1693. [Google Scholar] [CrossRef] [PubMed]
- Messineo, D.; Barile, G.; Morrone, S.; La Torre, G.; Turchetti, P.; Accetta, L.; Battagliola, E.T.; Agostinelli, E.; Pacella, F. Meta-analysis on the utility of radiotherapy for the treatment of Ocular Melanoma. Clin. Ter. 2020, 170, e89–e98. [Google Scholar]
- Damato, B.; Groenewald, C.; McGalliard, J.; Wong, D. Endoresection of choroidal melanoma. Br. J. Ophthalmol. 1998, 82, 213–218. [Google Scholar] [CrossRef]
- Bechrakis, N.E.; Foerster, M.H. Neoadjuvant proton beam radiotherapy combined with subsequent endoresection of choroidal melanomas. Int. Ophthalmol. Clin. 2006, 46, 95–107. [Google Scholar] [CrossRef]
- Karkhaneh, R.; Chams, H.; Amoli, F.A.; Riazi-Esfahani, M.; Ahmadabadi, M.N.; Mansouri, M.R.; Nouri, K.; Karkhaneh, A. Long-term surgical outcome of posterior choroidal melanoma treated by endoresection. Retina 2007, 27, 908–914. [Google Scholar] [CrossRef]
- Caminal, J.M.; Mejia, K.; Masuet-Aumatell, C.; Arias, L.; Piulats, J.M.; Gutierrez, C.; Pera, J.; Catala, J.; Rubio, M.; Arruga, J. Endoresection versus iodine-125 plaque brachytherapy for the treatment of choroidal melanoma. Am. J. Ophthalmol. 2013, 156, 334–342.e1. [Google Scholar] [CrossRef]
- Konstantinidis, L.; Groenewald, C.; Coupland, S.E.; Damato, B. Long-term outcome of primary endoresection of choroidal melanoma. Br. J. Ophthalmol. 2013, 98, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Arumi, J.; Leila, M.; Zapata, M.A.; Velázquez, D.; Dinares-Fernandez, M.C.; Tresserra, F.; Corcostegui, B. Endoresection technique with/without brachytherapy for management of high posterior choroidal melanoma: Extended follow-up results. Retina 2015, 35, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Biewald, E.; Lautner, H.; Gök, M.; Horstmann, G.A.; Sauerwein, W.; Flühs, D.; Bornfeld, N. Endoresection of large uveal melanomas: Clinical results in a consecutive series of 200 cases. Br. J. Ophthalmol. 2016, 101, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Vidoris, A.A.C.; Maia, A.; Lowen, M.; Morales, M.; Isenberg, J.; Fernandes, B.F.; Belfort, R.N. Outcomes of primary endoresection for choroidal melanoma. Int. J. Retin. Vitr. 2017, 3, 42. [Google Scholar] [CrossRef] [PubMed]
- Hamza, H.S.; Elhusseiny, A.M. Choroidal Melanoma Resection. Middle East Afr. J. Ophthalmol. 2018, 25, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Reichstein, D.; Karan, K. Endoresection utilizing pars plana vitrectomy for benign and malignant intraocular tumors. Curr. Opin. Ophthalmol. 2019, 30, 151–158. [Google Scholar] [CrossRef]
- Caminal, J.M.; Lorenzo, D.; Gutierrez, C.; Slocker, A.; Piulats, J.M.; Cobos, E.; Garcia-Bru, P.; Morwani, R.; Santamaria, J.F.; Arias, L. Local Resection in Choroidal Melanoma: A Review. J. Clin. Med. 2022, 11, 7156. [Google Scholar] [CrossRef]
- Dogrusöz, M.; Jager, M.J.; Damato, B. Uveal melanoma treatment and prognostication. Asia-Pacific J. Ophthalmol. 2017, 6, 305. [Google Scholar]
- Karimi, S.; Arabi, A.; Siavashpour, Z.; Shahraki, T.; Ansari, I. Efficacy and complications of ruthenium-106 brachytherapy for uveal melanoma: A systematic review and meta-analysis. J. Contemp. Brachytherapy 2021, 13, 358–364. [Google Scholar] [CrossRef]
- Langmann, G.; Pendl, G.; Klaus, M.; Papaefthymiou, G.; Guss, H. Gamma knife radiosurgery for uveal melanomas: An 8-year experience. J. Neurosurg. 2000, 93, 184–188. [Google Scholar] [CrossRef]
- Mueller, A.J.; Talies, S.; Schaller, U.C.; Horstmann, G.; Wowra, B.; Kampik, A. Stereotactic radiosurgery of large uveal melanomas with the gamma-knife. Ophthalmology 2000, 107, 1381–1387. [Google Scholar] [CrossRef] [PubMed]
- Dunavoelgyi, R.; Dieckmann, K.; Gleiss, A.; Sacu, S.; Kircher, K.; Georgopoulos, M.; Georg, D.; Zehetmayer, M.; Poetter, R. Local tumor control, visual acuity, and survival after hypofractionated stereotactic photon radiotherapy of choroidal melanoma in 212 patients treated between 1997 and 2007. Int. J. Radiat. Oncol. 2011, 81, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Eibl-Lindner, K.; Fürweger, C.; Nentwich, M.; Foerster, P.; Wowra, B.; Schaller, U.; Muacevic, A. Robotic radiosurgery for the treatment of medium and large uveal melanoma. Melanoma Res. 2016, 26, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Siedlecki, J.; Reiterer, V.; Leicht, S.; Foerster, P.; Kortüm, K.; Schaller, U.; Priglinger, S.; Fuerweger, C.; Muacevic, A.; Eibl-Lindner, K. Incidence of secondary glaucoma after treatment of uveal melanoma with robotic radiosurgery versus brachytherapy. Acta Ophthalmol. 2017, 95, e734–e739. [Google Scholar] [CrossRef]
- Sekac, J.; Ferkova, S.L.; Kollarova, A.; Kusenda, P.; Furda, R.; Gregus, M. Secondary glaucoma in small versus large uveal melanoma patients treated with stereotactic radiosurgery on linear accelerator. Bratisl. Med. J. 2019, 120, 945–949. [Google Scholar] [CrossRef]
- Modorati, G.M.; Dagan, R.; Mikkelsen, L.H.; Andreasen, S.; Ferlito, A.; Bandello, F. Gamma Knife Radiosurgery for Uveal Melanoma: A Retrospective Review of Clinical Complications in a Tertiary Referral Center. Ocul. Oncol. Pathol. 2019, 6, 115–122. [Google Scholar] [CrossRef]
- Mazzini, C.; Pieretti, G.; Vicini, G.; Nicolosi, C.; Scoccianti, S.; Pertici, M.; Greto, D.; Desideri, I.; Bordi, L.; Pecchioli, G.; et al. Clinical outcomes and secondary glaucoma after gamma-knife radiosurgery and Ruthenium-106 brachytherapy for uveal melanoma: A single institution experience. Ocul. Oncol. Pathol. 2019, 6, 115–122. [Google Scholar] [CrossRef]
- Shields, C.L.; Shields, J.A.; Karlsson, U.; Markoe, A.M.; Brady, L.W. Reasons for enucleation after plaque radiotherapy for posterior uveal melanoma. Clinical findings. Ophthalmology 1989, 96, 919–924. [Google Scholar] [CrossRef]
- Klingenstein, A.; Fürweger, C.; Nentwich, M.M.; Schaller, U.C.; Foerster, P.I.; Wowra, B.; Muacevic, A.; Eibl, K.H. Quality of life in the follow-up of uveal melanoma patients after Cyber-Knife treatment. Melanoma Res. 2013, 23, 481–488. [Google Scholar] [CrossRef]
- Bosch, T.V.D.; Vaarwater, J.; Verdijk, R.; Muller, K.; Kiliç, E.; Paridaens, D.; de Klein, A.; Naus, N. Risk factors associated with secondary enucleation after fractionated stereotactic radiotherapy in uveal melanoma. Acta Ophthalmol. 2015, 93, 555–560. [Google Scholar] [CrossRef]
- Süsskind, D.; Dürr, C.; Paulsen, F.; Kaulich, T.; Bartz-Schmidt, K.U. Endoresection with adjuvant ruthenium brachytherapy for selected uveal melanoma patients–The tuebingen experience. Acta Ophthalmol. 2016, 95, e727–e733. [Google Scholar] [CrossRef] [PubMed]
- Peyman, G.A.; Cohen, S.B. Ab interno resection of uveal melanoma. Int. Ophthalmol. 1986, 9, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.J.; Peyman, G.A.; Raichand, S. Internal eye wall resection for posterior uveal melanoma. Jpn. J. Ophthalmol. 1993, 37, 287–292. [Google Scholar] [PubMed]
- Schmidt, J.C.; Brieden-Azvedo, S.; Nietgen, G.W. Therapy of radiation resistant malignant uveal melanoma with endoresection by pars plana vitrectomy in two patients. Klin Monbl Augenheilkd. 2001, 218, 800–804. [Google Scholar] [CrossRef] [PubMed]
- Bornfeld, N.; Talies, S.; Anastassiou, G.; Schilling, H.; Schüler, A.; A Horstmann, G. Endoscopic resection of malignant melanomas of the uvea after preoperative stereotactic single dose convergence irradiation with the Leksell gamma knife. Ophthalmologe 2002, 99, 338–344. [Google Scholar] [CrossRef]
- Bechrakis, N.E.; Höcht, S.; Martus, P.; Kreusel, K.M.; Heese, J.; Foerster, M.H. Endoresection following proton beam irradiation of large uveal melanomas. Ophthalmologe 2004, 101, 370–376. [Google Scholar] [CrossRef]
- Schilling, H.; Bornfeld, N.; Talies, S.; Anastassiou, G.; Schüler, A.; Horstmann, G.A.; Jurklies, B. Endoresection of large uveal melanomas after pretreatment by single-dose stereotactic convergence irradiation with the leksell gamma knife–first experience on 46 cases. Klin Monbl Augenheilkd. 2006, 22, 513–520. [Google Scholar] [CrossRef]
- Ferreyra, H.A.; Goldbaum, M.H.; Weinreb, R.N. Endoresection of irradiated choroidal melanoma as a treatment for intractable vitreous hemorrhage and secondary blood-induced glaucoma. Semin. Ophthalmol. 2008, 23, 135–138. [Google Scholar] [CrossRef]
- Kertes, P.J.; Johnson, J.C.; Peyman, G.A. Internal resection of posterior uveal melanomas. Br. J. Ophthalmol. 1998, 82, 1147–1153. [Google Scholar] [CrossRef]
- Rice, J.C.; Stannard, C.; Cook, C.; Lecuona, K.; Myer, L.; Scholtz, R.P. Brachytherapy and endoresection for choroidal melanoma: A cohort study. Br. J. Ophthalmol. 2014, 98, 86–91. [Google Scholar] [CrossRef]
- García-Arumí, J.; Zapata, M.A.; Balaguer, O.; Fonollosa, A.; Boixadera, A.; Martinez-Castillo, V. Endoresection in high posterior choroidal melanomas: Long-term outcome. Br. J. Ophthalmol. 2008, 92, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- García-Arumí, J.; Sararols, L.; Martinez, V.; Corcostegui, B. Vitreoretinal surgery and endoresection in high posterior choroidal melanomas. Retina 2001, 21, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Diener-West, M.; Earle, J.D.; Fine, S.L.; Hawkins, B.S.; Moy, C.S.; Reynolds, S.M.; Schachat, A.P.; Straatsma, B.R.; Collaborative Ocular Melanoma Study Group. The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma, III: Initial mortality findings. COMS Report No. 18. Arch. Ophthalmol. 2001, 119, 969–982. [Google Scholar] [PubMed]
- Bechrakis, N.E.; Petousis, V.; Willerding, G.; Krause, L.; Wachtlin, J.; Stroux, A.; Foerster, M.H. Ten-year results of transscleral resection of large uveal melanomas: Local tumour control and metastatic rate. Br. J. Ophthalmol. 2010, 94, 460–466. [Google Scholar] [CrossRef]
- Relimpio-López, I.; Garrido-Hermosilla, A.M.; Espejo, F.; Gessa-Sorroche, M.; Coca, L.; Domínguez, B.; Díaz-Granda, M.J.; Ponte, B.; Cano, M.J.; de la Rúa, E.R.; et al. Clinical Outcomes after Surgical Resection Combined with Brachytherapy for Uveal Melanomas. Cancers 2019, 11, 856. [Google Scholar] [CrossRef]
- Anand, K.; Roszik, J.; Gombos, D.; Upshaw, J.; Sarli, V.; Meas, S.; Lucci, A.; Hall, C.; Patel, S. Pilot Study of Circulating Tumor Cells in Early-Stage and Metastatic Uveal Melanoma. Cancers 2019, 11, 856. [Google Scholar] [CrossRef]
- Callejo, S.A.; Antecka, E.; Blanco, P.L.; Edelstein, C.; Burnier, M.N., Jr. Identification of circulating malignant cells and its correlation with prognostic factors and treatment in uveal melanoma. A prospective longitudinal study. Eye 2006, 21, 752–759. [Google Scholar] [CrossRef]
- Mazzini, C.; Pinzani, P.; Salvianti, F.; Scatena, C.; Paglierani, M.; Ucci, F.; Pazzagli, M.; Massi, D. Circulating tumor cells detection and counting in uveal melanomas by a filtration-based method. Cancers 2014, 6, 323–332. [Google Scholar] [CrossRef]
- Beasley, A.B.; Chen, F.K.; Isaacs, T.W.; Gray, E.S. Future perspectives of uveal melanoma blood based biomarkers. Br. J. Cancer 2022, 126, 1511–1528. [Google Scholar] [CrossRef]
- Suesskind, D.; Ulmer, A.; Schiebel, U.; Fierlbeck, G.; Spitzer, B.; Spitzer, M.S.; Bartz-Schmidt, K.U.; Grisanti, S. Circulating melanoma cells in peripheral blood of patients with uveal melanoma before and after different therapies and association with prognostic parameters: A pilot study. Acta Ophthalmol. 2009, 89, 17–24. [Google Scholar] [CrossRef]
- Damato, B.; Duke, C.; Coupland, S.E.; Hiscott, P.; Smith, P.A.; Campbell, I.; Douglas, A.; Howard, P. Cytogenetics of uveal melanoma: A 7-year clinical experience. Ophthalmology 2007, 114, 1925–1931.e1. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Ganguly, A.; A Materin, M.; Teixeira, L.; Mashayekhi, A.; Swanson, L.A.; Marr, B.P.; A Shields, J. Chromosome 3 analysis of uveal melanoma using fine-needle aspiration biopsy at the time of plaque radiotherapy in 140 consecutive cases. Am. J. Ophthalmol. 2007, 105, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Damato, B.; Dopierala, J.A.; Coupland, S.E. Genotypic profiling of 452 choroidal melanomas with multiplex ligation-dependent probe amplification. Clin. Cancer Res. 2010, 16, 6083–6092. [Google Scholar] [CrossRef]
- Onken, M.D.; Worley, L.A.; Char, D.H.; Augsburger, J.J.; Correa, Z.M.; Nudleman, E.; Aaberg, T.M., Jr. Collaborative Ocular Oncology Group report number 1: Prospective validation of a multi-gene prognostic assay in uveal melanoma. Ophthalmology 2012, 119, 1596–1603. [Google Scholar] [CrossRef]
- Rice, J.C.; Liebenberg, L.; Scholtz, R.P.; Torr, G. Fatal air embolism during endoresection of choroidal melanoma. Retin. Cases Brief Rep. 2014, 8, 127–129. [Google Scholar] [CrossRef]
- Huang, Y.; Wei, W.B. Acute pulmonary embolism caused by local resection of choroidal melanoma. Chin. Med. J. 2016, 129, 743–745. [Google Scholar] [CrossRef]
- Ruschen, H.; Romano, M.R.; Ferrara, M.; Loh, G.K.; Wickham, L.; Damato, B.E.; da Cruz, L. Perfluorocarbon syndrome–a possible, overlooked source of fatal gas embolism following uveal-melanoma endoresection. Eye 2022, 36, 2348–2349. [Google Scholar] [CrossRef] [PubMed]
- Rojanaporn, D.; Tipsuriyaporn, B.; Chulalaksiriboon, P.; Virankabutra, T.; Morakul, S.; Damato, B. Fatal Air Embolism after Choroidal Melanoma Endoresection without Air Infusion: A Case Report. Ocul. Oncol. Pathol. 2021, 7, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Oliver, S.C.N.; Leu, M.Y.; DeMarco, J.J.; Chow, P.E.; Lee, S.P.; McCannel, T.A. Attenuation of iodine 125 radiation with vitreous substitutes in the treatment of uveal melanoma. Arch. Ophthalmol. 2010, 128, 888–893. [Google Scholar] [CrossRef]
- Sadiq, S.A.; Pattinson, R.; Poole, H.M.; Bundy, C. Psychological distress and coping following eye removal surgery. Orbit 2019, 39, 175–182. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ID | Age * | Sex | Prior Treatments | BD (mm) ** | TK (mm) ** | Tumor Quadrant | RD ** | Surgical Approach | BCVA ** | BCVA *** | Eye Retention *** | M3 | 8qG | MT *** | Follow-Up Time (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| #1 | 22 | M | None | 13.0 × 15.0 | 6.9 | IT | Y | RF | 20/100 | 20/100 | Y | Y | N | N | 45.2 |
| #2 | 56 | M | None | 10.2 × 11.3 | 7.4 | ST | Y | RF | 20/100 | 20/125 | Y | Y | Y | N | 42.4 |
| #3 | 61 | M | None | 5.5 × 7.5 | 8.0 | T | N | TR | 20/20 | 20/20 | Y | Y | N | N | 40.3 |
| #4 | 68 | F | None | 10.7 × 11.6 | 6.5 | IT | N | RF | 20/50 | 20/63 | Y | N | N | N | 39.8 |
| #5 | 72 | M | BT | 10.9 × 15.4 | 6.4 | T | Y | RF | 20/100 | / | N | Y | Y | N | 38.9 |
| #6 | 73 | M | None | 8.8 × 9.7 | 6.2 | INa | Y | TR | HM | 20/400 | Y | N | N | N | 36.8 |
| #7 | 72 | F | None | 10.77 × 7.5 | 6.6 | IT | Y | TR | 20/63 | 20/63 | Y | N | N | N | 20.2 |
| #8 | 82 | M | None | 11.5 × 11.0 | 7.0 | Na | Y | TR | 20/100 | 20/400 | Y | Y | N | N | 16.0 |
| #9 | 92 | F | None | 13.4 × 12.3 | 10 | T | Y | TR | 20/400 | 20/100 | Y | Y | Y | N | 21.9 |
| #10 | 63 | F | None | 11.6 × 11.3 | 11.7 | I | Y | TR | 20/800 | CD | Y | Y | N | N | 12.7 |
| #11 | 70 | F | BT | 11.0 × 8.5 | 5.6 | Na | Y | TR | 20/80 | 20/50 | Y | N | Y | Y | 28.2 |
| #12 | 31 | F | None | 12.4 × 10.9 | 7.6 | T | Y | RF | 20/80 | 20/80 | Y | N | Y | N | 19.5 |
| #13 | 67 | F | GK | 8.9 × 8.5 | 8.0 | Na | Y | TR | 20/400 | CD | Y | N | N | N | 31.0 |
| #14 | 45 | F | None | 8.7 × 7.1 | 7.1 | SNa | N | TR | 20/50 | 20/50 | Y | Y | N | N | 21.6 |
| #15 | 50 | F | GK | 9.9 × 8.3 | 2.63 | T | N | RF | 20/50 | 20/32 | Y | Y | Y | N | 34.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzini, C.; Vicini, G.; Di Leo, L.; Massi, D.; Rizzo, S.; Giansanti, F. Anatomical and Functional Outcomes after Endoresection and Adjuvant Ruthenium Brachytherapy for Uveal Melanoma: A Single-Center Experience. Life 2023, 13, 902. https://doi.org/10.3390/life13040902
Mazzini C, Vicini G, Di Leo L, Massi D, Rizzo S, Giansanti F. Anatomical and Functional Outcomes after Endoresection and Adjuvant Ruthenium Brachytherapy for Uveal Melanoma: A Single-Center Experience. Life. 2023; 13(4):902. https://doi.org/10.3390/life13040902
Chicago/Turabian StyleMazzini, Cinzia, Giulio Vicini, Laura Di Leo, Daniela Massi, Stanislao Rizzo, and Fabrizio Giansanti. 2023. "Anatomical and Functional Outcomes after Endoresection and Adjuvant Ruthenium Brachytherapy for Uveal Melanoma: A Single-Center Experience" Life 13, no. 4: 902. https://doi.org/10.3390/life13040902