
Ulceration and a White Lesion of the Tongue in a Male HIV Positive Patient: A Journey on the Avenue of Differential Diagnoses in Search of a Solution

 , ,
, ,
Abstract
:1. Introduction
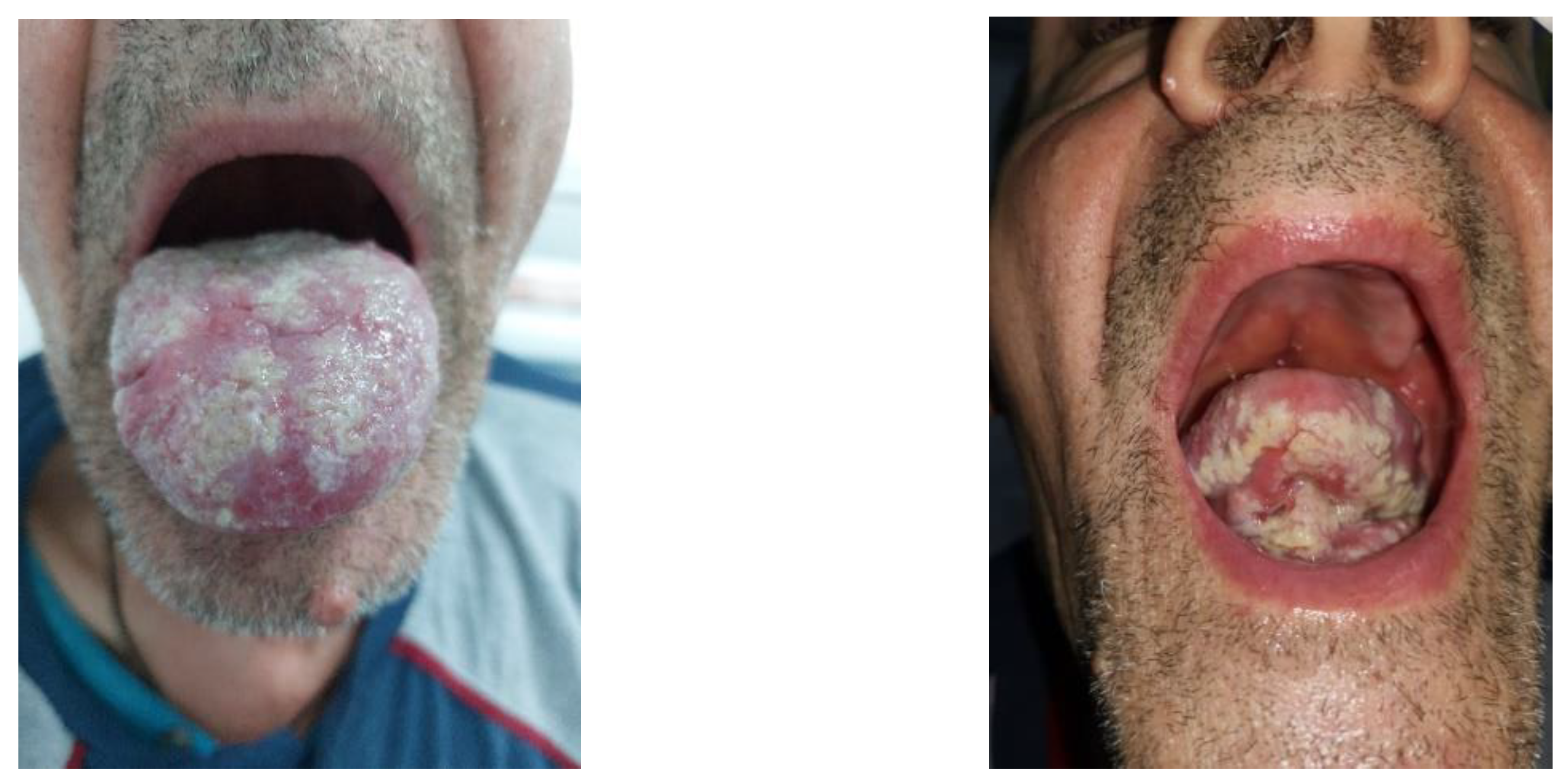
2. Case Presentation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|---|---|---|
| Hb [g/dL] | 12.3 | 14.3 | 14.5 | 14.6 | 11.8 | 13.7 | 13.8 | 11.4 |
| Serum Iron | 28.5 | 57.8 | 65.6 | 65.9 | 63.5 | 115.6 | 76.5 | 32.1 |
| Platelets × 103 | 202 | 196 | 188 | 242 | 217 | 237 | 208 | 184 |
| WBC/mm3 | 2840 | 3600 | 5250 | 5790 | 3410 | 4700 | 5800 | 4800 |
| Eos/mm3 | 154 | 266 | 168 | 92 | 51 | 169 | 116 | 130 |
| Lymph/mm3 | 430 | 1170 | 1390 | 1140 | 760 | 1560 | 1410 | 1110 |
| CD4/mm3 | 23 | 102 | 154 | 139 | 35 | 57 | 48 | 45 |
| ARN-HIV c/mL | 1,370,000 | 237 | ND | 270,707 | 10,482 | 20,166 | 109,497 | 233,000 |
| VDRL | 1/64 | 1/32 | 1/16 | 1/8 | 1/4 | / | / | ½ |
| TPHA | ++ | ++++ | +++ | +++ | + | + | + | + |
3. Discussion
3.1. Classification of Oral Lesions Related to HIV
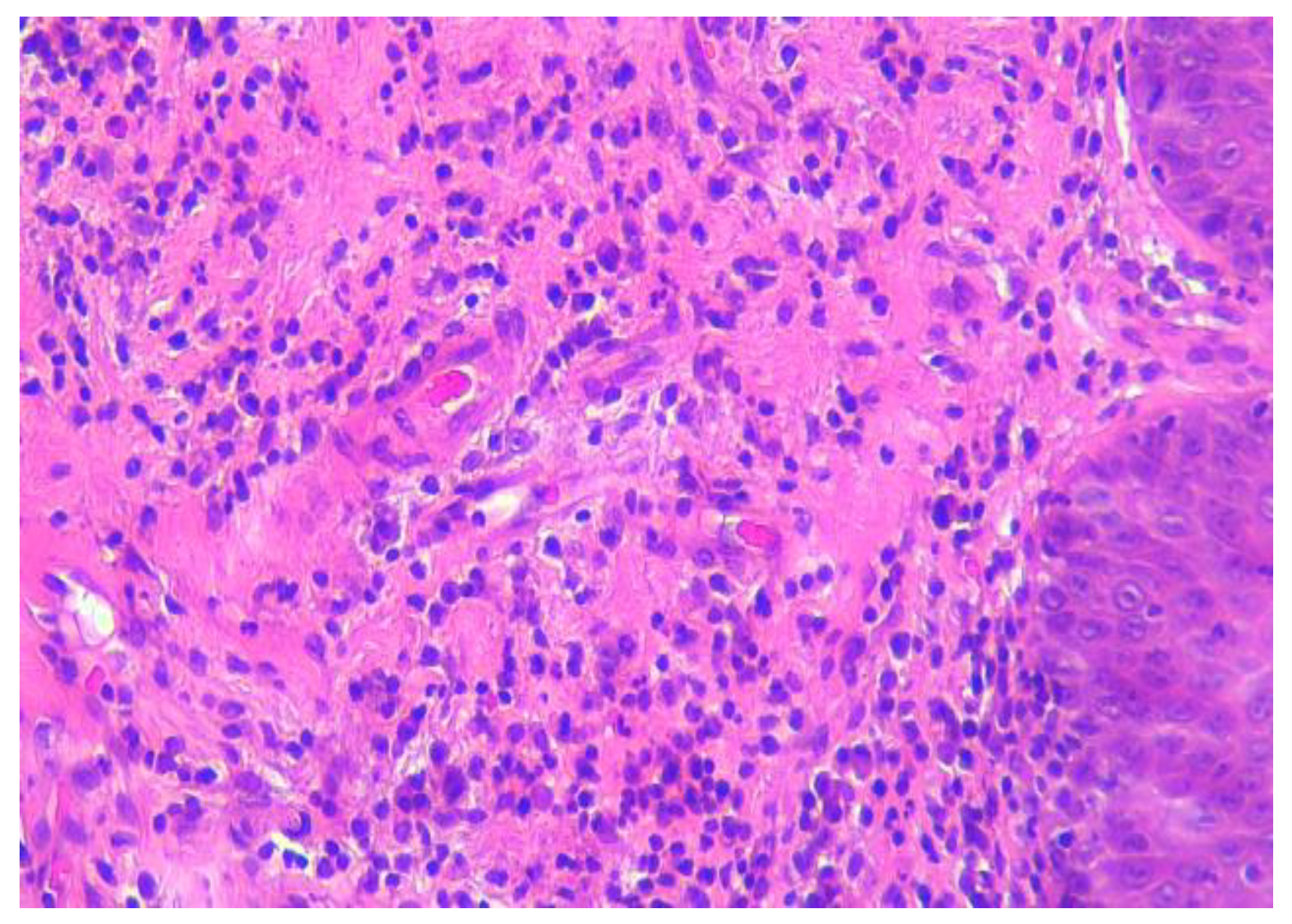
3.2. Oral Eosinophilic Granuloma
3.3. Syphilis and HIV Co-Infection
3.4. Differential Diagnoses of Oral White Lesions
3.5. Oral Lesions and Cannabidiol Use
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World. ReliefWeb. In Danger: UNAIDS Global AIDS Update 2022 [EN/RU]. Available online: https://reliefweb.int/report/world/danger-unaids-global-aids-update-2022-enru?gclid=CjwKCAiA85efBhBbEiwAD7oLQG5iYLIasRf4hSnUyxxPvpcNeKWprLBB_obc7dctjBuusVWETVKzbhoCXrQQAvD_BwE (accessed on 10 February 2023).
- Fonseca, R.R.S.; Laurentino, R.V.; Machado, L.F.A.; Gomes, C.E.V.S.; Menezes, T.O.A.; Pessoa, O.F.; Oliveira-Filho, A.B.; Carvalho, T.R.B.; Oliveira, P.G.F.P.; Tanaka, E.B.; et al. HIV Infection and Oral Manifestations: An Update. In Future Opportunities and Tools for Emerging Challenges for HIV/AIDS Control; Intech Open: London, UK, 2022. [Google Scholar] [CrossRef]
- Tappuni, A.R. The global changing pattern of the oral manifestations of HIV. Oral Dis. 2020, 26, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Pricop, R.; Cristea, V.C.; Gheorghe, I.; Tatu, A.L.; Mihaescu, G.; Chifiriuc, M.C. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) reveals the anaerobic Slakia exigua as unique etiology of a dental abscess. Biointerface Res. Appl. Chem 2017, 7, 1995–1997. [Google Scholar]
- Khoury, Z.H.; Meeks, V. The influence of antiretroviral therapy on HIV-related oral manifestations. J. Natl. Med. Assoc. 2021, 113, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Tugizov, S.; Pandiyan, P.; Jin, G.; Rakshit, S.; Vyakarnam, A.; Naglik, J.R. Innate immune mechanisms to oral pathogens in oral mucosa of HIV-infected individuals. Oral Dis. 2020, 26, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Janier, M.; Unemo, M.; Dupin, N.; Tiplica, G.S.; Potočnik, M.; Patel, R. 2020 European guideline on the management of syphilis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 574–588. [Google Scholar] [CrossRef] [PubMed]
- Brănișteanu, D.E.; Pintilie, A.; Dimitriu, A.; Cerbu, A.; Ciobanu, D.; Oanţă, A.; Tatu, A.L. Clinical, laboratory and therapeutic profile of lichen planus. Med. Surg. J. 2017, 121, 25–32. [Google Scholar]
- Oranges, T.; Janowska, A.; Vitali, S.; Loggini, B.; Izzetti, R.; Romanelli, M.; Dini, V. Dermatoscopic and ultra-high frequency ultrasound evaluation in cutaneous postradiation angiosarcoma. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e741. [Google Scholar] [CrossRef]
- Benitez, B.; Mülli, J.; Tzankov, A.; Kunz, C. Traumatic ulcerative granuloma with stromal eosinophilia—Clinical case report, literature review, and differential diagnosis. World J. Surg. Onc. 2019, 17, 184. [Google Scholar] [CrossRef]
- Didona, D.; Paolino, G.; Donati, M.; Didona, B.; Calvieri, S. Eosinophilic ulcer of the tongue—Case report. An. Bras. Dermatol. 2015, 90, 88–90. [Google Scholar] [CrossRef] [Green Version]
- Sharma, B.; Koshy, G.; Kapoor, S. Traumatic Ulcerative Granuloma with Stromal Eosinophila: A Case Report and Review of Pathogenesis. J. Clin. Diagn. Res. 2016, 10, ZD07–ZD09. [Google Scholar] [CrossRef]
- Lingaraju, N.; Gaddelingiah, Y.B.; Shivalingu, M.M.; Khanum, N. Eosinophilic ulcer of the tongue: A rare and confusing clinical entity. BMJ Case Rep. 2015, 2015, bcr2015210107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugaya, N.; Martignago, F.; Pinto, D.; Migliari, D. Recurrent Oral Eosinophilic Ulcers of the Oral Mucosa. A Case Report. Open Dent. J. 2018, 12, 19–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corti, M. Oral Cavity and HIV Infection. On. J. Dent. Oral Health 2020, 3, OJDOH.MS.ID.000556. [Google Scholar] [CrossRef]
- Hamie, L.; Hamie, M.; Kurban, M.; Abbas, O. Eosinophilic ulcer of the oral mucosa: An update on clinicopathologic features, pathogenesis, and management. Int. J. Dermatol. 2022, 61, 1359–1363. [Google Scholar] [CrossRef]
- Bortoluzzi, M.C.; Passador-Santos, F.; Capella, D.L.; Manfro, G.; Nodari, R.J.; Presta, A.A. Eosinophilic ulcer of oral mucosa: A case report. Ann. Stomatol. 2012, 3, 11–13. [Google Scholar]
- Setti, G.; Martella, E.; Mancini, C.; Vescovi, P.; Magnoni, C.; Bellini, P.; Giovannacci, I.; Meleti, M. Self-healing CD30- T-clonal proliferation of the tongue: Report of an extremely rare case. BMC Oral Health 2019, 19, 186. [Google Scholar] [CrossRef] [Green Version]
- Sah, K.; Chandra, S.; Singh, A.; Singh, S. Eosinophilic ulcer of the tongue masquerading as malignant ulcer: An unexplored distinct pathology. J. Oral Maxillofac. Pathol. 2017, 21, 321. [Google Scholar] [CrossRef] [Green Version]
- Levin, N.A.; Patterson, J.W.; Yao, L.L.; Wilson, B.B. Resolution of patch-type granuloma annulare lesions after biopsy. J. Am. Acad. Dermatol. 2002, 46, 426–429. [Google Scholar] [CrossRef]
- Kluger, N.; Jegou, M.H. Psoriasis and reverse Koebner response after tattooing. Ann. Dermatol. Venereol. 2018, 145, 48–49. [Google Scholar] [CrossRef] [Green Version]
- Nwabudike, L.C.; Tatu, A.L. Reply to Happle R. et al. Koebner’s sheep in Wolf’s clothing: Does the isotopic response exists as a distinct phenomenon? J. Eur. Acad. Dermatol. Venereol. 2018, 32, e336–e337. [Google Scholar] [CrossRef]
- Happle, R.; Kluger, N. Answer to Tatu AL, Nwabudike LC: Koebner’s sheep in Wolf’s clothing—Does the isotopic response exist as a distinct phenomenon? J. Eur. Acad. Dermatol. Venereol. 2018, 32, e337. [Google Scholar] [CrossRef] [PubMed]
- Nwabudike, L.C.; Tatu, A.L. Reply to Gambichler T et al.: Altered epigenetic pathways and cell cycle dysregulation in healthy appearing skin of patients with koebnerized squamous cell carcinomas following skin surgery. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e3–e4. [Google Scholar] [CrossRef] [Green Version]
- Tatu, A.L.; Nadasdy, T.; Nwabudike, L.C. Koebner phenomenon with lichen planus in an area of previous vitiligo after COVID-19 vaccination and the creation of a locus minoris resistentiae. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e265–e266. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Gómez, N.; Hermosa-Gelbard, Á.; Carrillo-Gijón, R.; Jaén, P. Secondary Syphilis Mimicking Lichen Planus in a Patient with HIV Coinfection. Actas Dermosifiliogr. 2016, 107, 612–614. [Google Scholar] [CrossRef] [PubMed]
- Eyer-Silva, W.A.; Leite Freire, M.A.; Horta-Araujo, C.A.; Rosa da Silva, G.A.; Cunha Pinto, J.F.; Almeida Ferry, F.R. Secondary Syphilis Presenting as Glossodynia, Plaques en Prairie Fauchée, and a Split Papule at the Oral Commissure: Case Report and Review. Case Rep. Med. 2017, 2017, 1980798. [Google Scholar] [CrossRef] [Green Version]
- Ivars Lleó, M.; Clavo Escribano, P.; Menéndez Prieto, B. Atypical Cutaneous Manifestations in Syphilis. Actas Dermosifiliogr. 2016, 107, 275–283. [Google Scholar] [CrossRef]
- Solis, R.N.; Kuhn, B.T.; Farwell, D.G. An Unusual Case of Tertiary Syphilis Behaving Like Tongue Squamous Cell Carcinoma. J. Investig. Med. High Impact Case Rep. 2018, 20, 2324709618820355. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.H.; Vargo, R.J.; Bilodeau, E.A.; Anderson, K.M.; Trzcinska, A.; Canterbury, C.R.; Fantasia, J.E.; Rawal, Y.B. Oral Manifestations of Syphilis: A Review of the Clinical and Histopathologic Characteristics of a Reemerging Entity with Report of 19 New Cases. Head Neck Pathol. 2021, 15, 787–795. [Google Scholar] [CrossRef]
- Bittencourt, M.J.; Brito, A.C.; Nascimento, B.A.; Carvalho, A.H.; Drago, M.G. Nodular tertiary syphilis in an immunocompetent patient. An. Bras. Dermatol. 2016, 91, 528–530. [Google Scholar] [CrossRef] [Green Version]
- Al Khabbaz, F.A.; Ali, M.M.; Al Awadhi, A. A Rare Case Report: Five Variants of Lichen Planus in a Young Male Patient. Cureus 2022, 14, e27080. [Google Scholar] [CrossRef]
- Lomelí-Martínez, S.M.; González-Hernández, L.A.; Ruiz-Anaya, A.d.J.; Lomelí-Martínez, M.A.; Martínez-Salazar, S.Y.; Mercado González, A.E.; Andrade-Villanueva, J.F.; Varela-Hernández, J.J. Oral Manifestations Associated with HIV/AIDS Patients. Medicina 2022, 58, 1214. [Google Scholar] [CrossRef] [PubMed]
- Lo, A.K.; Dawson, C.W.; Lung, H.L.; Wong, K.L.; Young, L.S. The Role of EBV-Encoded LMP1 in the NPC Tumor Microenvironment: From Function to Therapy. Front. Oncol. 2021, 11, 640207. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.; Medford, S.; Islam, S.; Ramsingh, C.; Christopher, M. Extranodal lymphoma of the tongue, a very rare entity-report of two cases with literature review. Int. J. Surg. Case Rep. 2019, 54, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Xu, X.; Wang, Y.; Zeng, M.S.; Yuan, Y. EBV latent membrane proteins promote hybrid epithelial-mesenchymal and extreme mesenchymal states of nasopharyngeal carcinoma cells for tumorigenicity. PLoS Pathog. 2021, 17, e1009873. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, S.; Veloza, L.; Wang, L.; López, M.; López-Guillermo, A.; Marginet, M.; Martínez, A.; Balagué, O.; Campo, E. HHV8-positive, EBV-positive Hodgkin lymphoma-like large B cell lymphoma: Expanding the spectrum of HHV8 and EBV-associated lymphoproliferative disorders. Int. J. Hematol. 2020, 112, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Arbune, M.; Padurariu-Covit, M.-D.; Rebegea, L.-F.; Lupasteanu, G.; Arbune, A.-A.; Stefanescu, V.; Tatu, A.-L. AIDS Related Kaposi’s Sarcoma: A 20-Year Experience in a Clinic from the South-East of Romania. J. Clin. Med. 2021, 10, 5346. [Google Scholar] [CrossRef] [PubMed]
- Bellocchio, L.; Inchingolo, A.D.; Inchingolo, A.M.; Lorusso, F.; Malcangi, G.; Santacroce, L.; Scarano, A.; Bordea, I.R.; Hazballa, D.; D’Oria, M.T.; et al. Cannabinoids Drugs and Oral Health-From Recreational Side-Effects to Medicinal Purposes: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 8329. [Google Scholar] [CrossRef]
- Liu, C.; Qi, X.; Yang, D.; Neely, A.; Zhou, Z. The effects of cannabis use on oral health. Oral Dis. 2020, 26, 1366–1374. [Google Scholar] [CrossRef]
- Andreis, K.; Billingsley, J.; Naimi Shirazi, K.; Wager-Miller, J.; Johnson, C.; Bradshaw, H.; Straiker, A. Cannabinoid CB1 receptors regulate salivation. Sci. Rep. 2022, 12, 14182. [Google Scholar] [CrossRef]





| GROUP | Cause |
|---|---|
| GROUP I: Oral manifestations strongly associated with HIV | Fungal infections Candidiasis
|
| Oral hairy leukoplakia | |
| Kaposi’s sarcoma | |
| Non-Hodgkin lymphoma | |
Periodontal disease
| |
| GROUP II: Oral manifestations frequently associated with HIV | Bacterial infections
|
Viral infections
| |
| Melanotic hyperpigmentation | |
Salivary gland disease
| |
| Ulcerations | |
| GROUP III: Oral manifestations seen in HIV infections | Viral infections
|
Fungal infections
| |
Bacterial infections
| |
| Drug reactions |
| Oral Leukoplakia | Oral Candidiasis | Oral Hairy Leukoplakia | |
|---|---|---|---|
| Etiology | Unknown | Candida albicans | Epstein–Barr Virus |
| Risk factors | Tobacco, alcohol | HIV, diabetes, antibiotics, corticosteroids, radiotherapy, chemotherapy | HIV immunosuppression |
| Lesions | Plate, white, adherent | White, creamy plaques, easily removable, with underlying erythema | White, hyperkeratotic plaques with vertical striations aspect, adherent, located on the lateral surfaces of the tongue |
| Pain | No | Yes | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbune, M.; Padurariu-Covit, M.-D.; Niculet, E.; Chiscop, I.; Arbune, A.-A.; Tatu, A.-L. Ulceration and a White Lesion of the Tongue in a Male HIV Positive Patient: A Journey on the Avenue of Differential Diagnoses in Search of a Solution. Life 2023, 13, 901. https://doi.org/10.3390/life13040901
Arbune M, Padurariu-Covit M-D, Niculet E, Chiscop I, Arbune A-A, Tatu A-L. Ulceration and a White Lesion of the Tongue in a Male HIV Positive Patient: A Journey on the Avenue of Differential Diagnoses in Search of a Solution. Life. 2023; 13(4):901. https://doi.org/10.3390/life13040901
Chicago/Turabian StyleArbune, Manuela, Monica-Daniela Padurariu-Covit, Elena Niculet, Iulia Chiscop, Anca-Adriana Arbune, and Alin-Laurențiu Tatu. 2023. "Ulceration and a White Lesion of the Tongue in a Male HIV Positive Patient: A Journey on the Avenue of Differential Diagnoses in Search of a Solution" Life 13, no. 4: 901. https://doi.org/10.3390/life13040901