
Syndecan-1: From a Promising Novel Cardiac Biomarker to a Surrogate Early Predictor of Kidney and Liver Injury in Patients with Acute Heart Failure

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Patients and Investigations
2.2. Statistical Analysis
2.3. Ethics
3. Results
3.1. Baseline Characteristics
3.2. Profile of Syndecan-1 in Acute HF
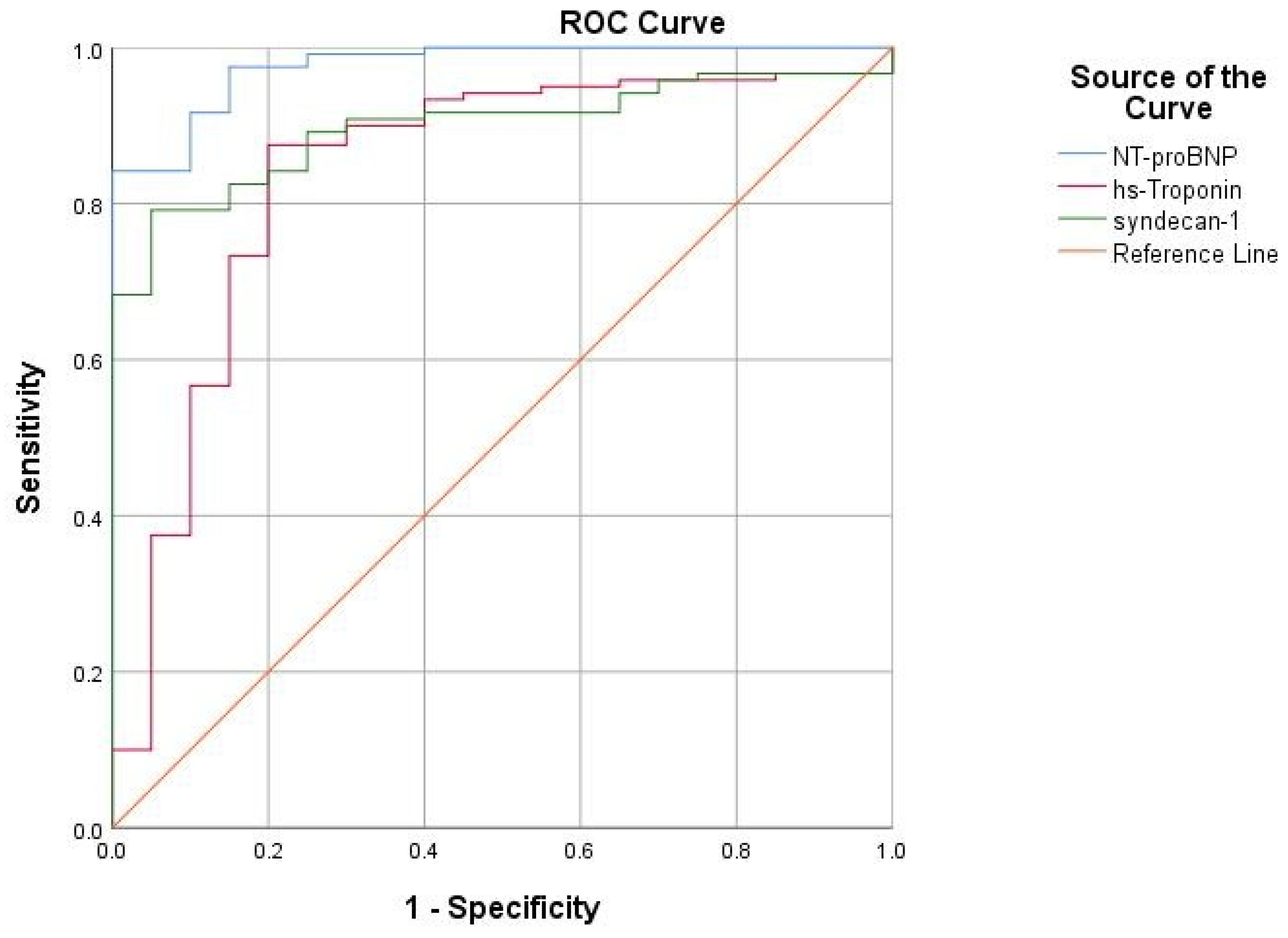
3.3. Diagnostic Performance of Syndecan-1 in Acute HF
3.4. Syndecan-1: Correlations with Echocardiographic Parameters in Acute HF
3.5. Syndecan-1: Potential Prognostic Role in Acute HF?
3.6. Syndecan-1 and the Risk Factors for HF
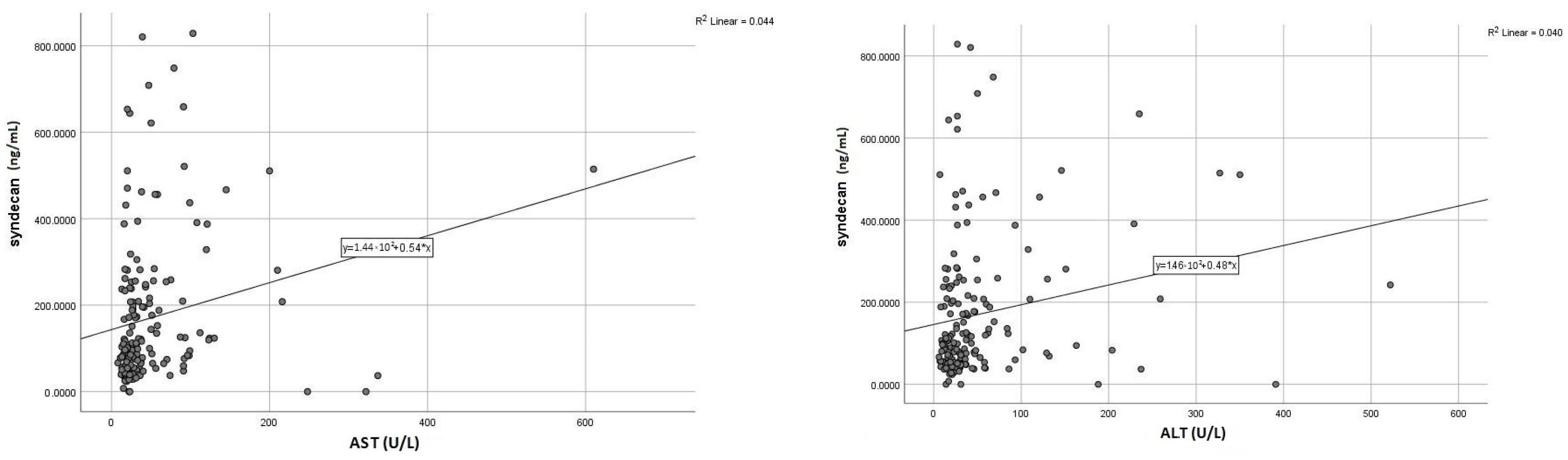
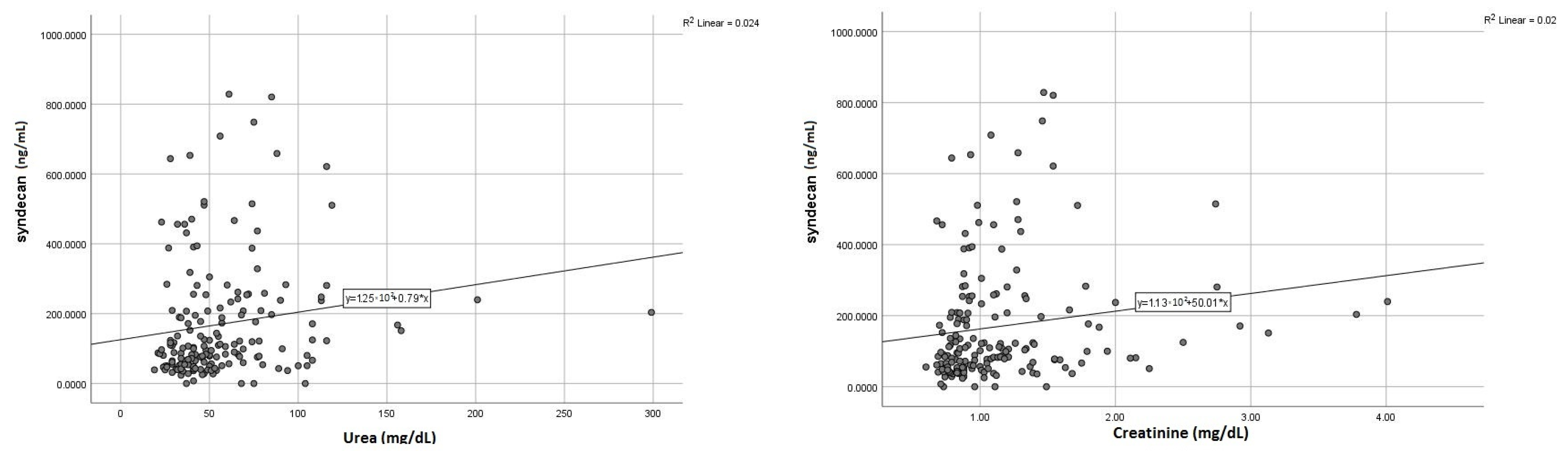
3.7. Syndecan-1: Surrogate Marker of Liver and Kidney Injury
3.8. Syndecan-1 and Metabolic Profile
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute heart failure. Nat. Rev. Dis. Prim. 2020, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Van Riet, E.E.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.A.; Rutten, F.H. Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Miftode, R.-S.; Costache, I.-I.; Cianga, P.; Petris, A.O.; Cianga, C.-M.; Maranduca, M.-A.; Miftode, I.-L.; Constantinescu, D.; Timpau, A.-S.; Crisan, A.; et al. The Influence of Socioeconomic Status on the Prognosis and Profile of Patients Admitted for Acute Heart Failure during COVID-19 Pandemic: Overestimated Aspects or a Multifaceted Hydra of Cardiovascular Risk Factors? Healthcare 2021, 9, 1700. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.E.; Januzzi, J.L., Jr. Established and Emerging Roles of Biomarkers in Heart Failure. Circ. Res. 2018, 123, 614–629. [Google Scholar] [CrossRef]
- Miftode, R.-S.; Constantinescu, D.; Cianga, C.-M.; Petris, A.-O.; Costache, I.-I.; Mitu, O.; Miftode, I.-L.; Mitu, I.; Timpau, A.-S.; Duca, S.-T.; et al. A Rising Star of the Multimarker Panel: Growth Differentiation Factor-15 Levels Are an Independent Predictor of Mortality in Acute Heart Failure Patients Admitted to an Emergency Clinical Hospital from Eastern Europe. Life 2022, 12, 1948. [Google Scholar] [CrossRef]
- Tromp, J.; van der Pol, A.; Klip, I.T.; de Boer, R.A.; Jaarsma, T.; van Gilst, W.H.; Voors, A.A.; van Veldhuisen, D.J.; van der Meer, P. Fibrosis marker syndecan-1 and outcome in patients with heart failure with reduced and preserved ejection fraction. Circ. Heart Fail. 2014, 7, 457–462. [Google Scholar] [CrossRef] [Green Version]
- Neves, F.M.; Meneses, G.C.; Sousa, N.E.; Menezes, R.R.; Parahyba, M.C.; Martins, A.M.; Libório, A.B. Syndecan-1 in acute decompensated heart failure—Association with renal function and mortality. Circ. J. 2015, 79, 1511–1519. [Google Scholar] [CrossRef] [Green Version]
- Miftode, R.S.; Şerban, I.L.; Timpau, A.S.; Miftode, I.L.; Ion, A.; Buburuz, A.M.; Costache, A.D.; Costache, I.I. Syndecan-1: A Review on Its Role in Heart Failure and Chronic Liver Disease Patients’ Assessment. Cardiol. Res. Pract. 2019, 2019, 4750580. [Google Scholar] [CrossRef] [Green Version]
- Schellings, M.W.; Vanhoutte, D.; van Almen, G.C.; Swinnen, M.; Leenders, J.J.; Kubben, N.; van Leeuwen, R.E.; Hofstra, L.; Heymans, S.; Pinto, Y.M. Syndecan-1 amplifies angiotensin II-induced cardiac fibrosis. Hypertension 2010, 55, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Frangogiannis, N.G. Syndecan-1: A critical mediator in cardiac fibrosis. Hypertension 2010, 55, 233–235. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Haller, C.A.; Wen, J.; Wang, P.; Chaikof, E.L. Decoupled syndecan 1 mRNA and protein expression is differentially regulated by angiotensin II in macrophages. J. Cell. Physiol. 2008, 214, 750–756. [Google Scholar] [CrossRef] [Green Version]
- Stepp, M.A.; Pal-Ghosh, S.; Tadvalkar, G.; Pajoohesh-Ganji, A. Syndecan-1 and Its Expanding List of Contacts. Adv. Wound Care 2015, 4, 235–249. [Google Scholar] [CrossRef] [Green Version]
- Ostrowski, S.R.; Pedersen, S.H.; Jensen, J.S.; Mogelvang, R.; Johansson, P.I. Acute myocardial infarction is associated with endothelial glycocalyx and cell damage and a parallel increase in circulating catecholamines. Crit. Care 2013, 17, 1. [Google Scholar] [CrossRef] [Green Version]
- Fuernau, G.; Jung, C.; Muench, P.; Desch, S.; Eitel, I.; Schuler, G.; Adams, V.; Figulla, H.R.; Thiele, H. Syndecan-1 and Heparan Sulfate in Acute Myocardial Infarction Complicated by Cardiogenic Shock—A Biomarker Substudy of the IABP-SHOCK II-Trial. Circulation 2018, 130, A18417. [Google Scholar]
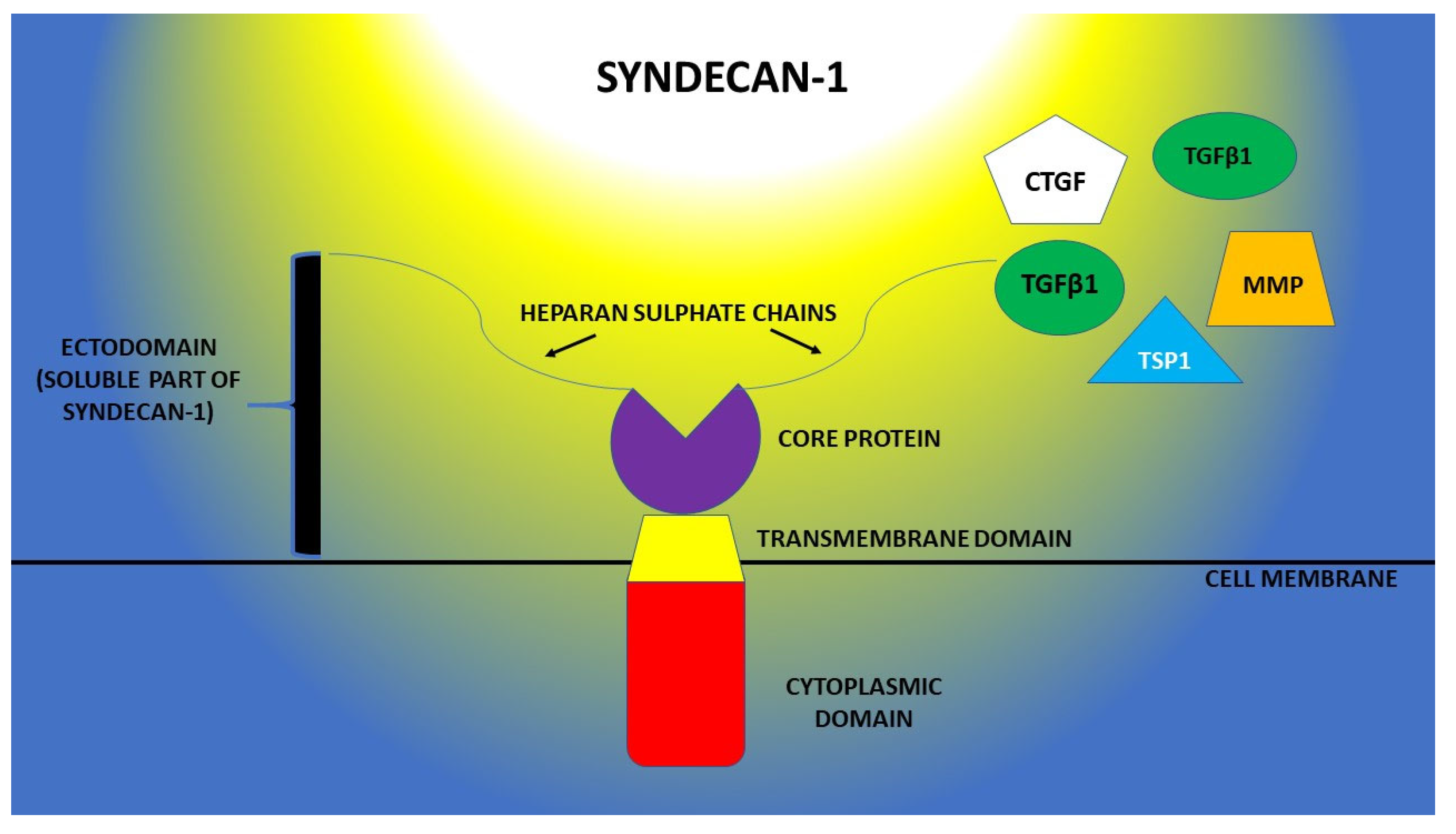
- Regős, E.; Abdelfattah, H.H.; Reszegi, A.; Szilák, L.; Werling, K.; Szabó, G.; Kiss, A.; Schaff, Z.; Kovalszky, I.; Baghy, K. Syndecan-1 inhibits early stages of liver fibrogenesis by interfering with TGFβ1 action and upregulating MMP14. Matrix Biol. 2018, 68, 474–489. [Google Scholar] [CrossRef]
- Szatmári, T.; Dobra, K. The role of syndecan-1 in cellular signaling and its effects on heparan sulfate biosynthesis in mesenchymal tumors. Front. Oncol. 2013, 3, 310. [Google Scholar] [CrossRef] [Green Version]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P.; Acute Dialysis Quality Initiative Workgroup. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [Green Version]
- Camps-Vilaró, A.; Delgado-Jiménez, J.F.; Farré, N.; Tizón-Marcos, H.; Álvarez-García, J.; Cinca, J.; Dégano, I.R.; Marrugat, J. Estimated Population Prevalence of Heart Failure with Reduced Ejection Fraction in Spain, According to DAPA-HF Study Criteria. J. Clin. Med. 2020, 9, 2089. [Google Scholar] [CrossRef]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.; Crespo-Leiro, M.G.; Harjola, V.P.; Parissis, J.; Laroche, C.; Piepoli, M.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Hear. Fail. 2017, 19, 1574–1585. [Google Scholar] [CrossRef] [Green Version]
- Jirak, P.; Pistulli, R.; Lichtenauer, M.; Wernly, B.; Paar, V.; Motloch, L.J.; Rezar, R.; Jung, C.; Hoppe, U.C.; Schulze, P.C.; et al. Expression of the Novel Cardiac Biomarkers sST2, GDF-15, suPAR, and H-FABP in HFpEF Patients Compared to ICM, DCM, and Controls. J. Clin. Med. 2020, 9, 1130. [Google Scholar] [CrossRef] [Green Version]
- Curry, F.E.; Adamson, R.H. Endothelial glycocalyx: Permeability barrier and mechanosensor. Ann. Biomed. Eng. 2012, 40, 828–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wernly, B.; Fuernau, G.; Masyuk, M.; Muessig, J.M.; Pfeiler, S.; Bruno, R.R.; Desch, S.; Muench, P.; Lichtenauer, M.; Kelm, M.; et al. Syndecan-1 Predicts Outcome in Patients with ST-Segment Elevation Infarction Independent from Infarct-related Myocardial Injury. Sci. Rep. 2019, 9, 18367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sueta, D.; Hokimoto, S. Could Circulatory Syndecan-1 Be a Predictable Biomarker for Acute Kidney Injury in Patients with Acute Decompensated Heart Failure? Circ. J. 2015, 79, 1444–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miftode, R.S.; Aursulesei, V.; Miftode, I.L.; Darie, A.S.; Buburuz, A.M.; Ion, A.; Costache, A.D.; Costache, I.I. Syndecan-1: New Perspectives of Risk and Prognostic Assessment in Heart Failure. Ann. Vasc. Med. Res. 2018, 5, 1083. [Google Scholar]
- Vanmassenhove, J.; Vanholder, R.; Nagler, E.; Van Biesen, W. Urinary and serum biomarkers for the diagnosis of acute kidney injury: An in-depth review of the literature. Nephrol. Dial. Transplant. 2013, 28, 254–273. [Google Scholar] [CrossRef] [Green Version]
- Regős, E.; Karászi, K.; Reszegi, A.; Kiss, A.; Schaff, Z.; Baghy, K.; Kovalszky, I. Syndecan-1 in Liver Diseases. Pathol. Oncol. Res. 2020, 26, 813–819. [Google Scholar] [CrossRef]
- Constantinescu, A.A.; Vink, H.; Spaan, J.A. Endothelial cell glycocalyx modulates immobilization of leukocytes at the endothelial surface. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1541–1547. [Google Scholar] [CrossRef] [Green Version]
- Tromp, J.; Westenbrink, B.D.; Ouwerkerk, W.; van Veldhuisen, D.J.; Samani, N.J.; Ponikowski, P.; Metra, M.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; et al. Identifying pathophysiological mechanisms in heart failure with reduced versus preserved ejection fraction. J. Am. Coll. Cardiol. 2018, 72, 1081–1090. [Google Scholar] [CrossRef]
- Timpau, A.-S.; Miftode, R.-S.; Leca, D.; Timpau, R.; Miftode, I.-L.; Petris, A.O.; Costache, I.I.; Mitu, O.; Nicolae, A.; Oancea, A.; et al. A Real Pandora’s Box in Pandemic Times: A Narrative Review on the Acute Cardiac Injury Due to COVID-19. Life 2022, 12, 1085. [Google Scholar] [CrossRef]
- Lionte, C.; Sorodoc, V.; Haliga, R.E.; Bologa, C.; Ceasovschih, A.; Petris, O.R.; Coman, A.E.; Stoica, A.; Sirbu, O.; Puha, G.; et al. Inflammatory and Cardiac Biomarkers in Relation with Post-Acute COVID-19 and Mortality: What We Know after Successive Pandemic Waves. Diagnostics 2022, 12, 1373. [Google Scholar] [CrossRef]
- Miftode, E.; Luca, C.; Manciuc, C.; Vâtă, A.; Hunea, I.; Miftode, L.; Bădescu, A.; Dorneanu, O. COVID-19: A Course through Stormy Waters. Med. Surg. J. Rev. Med. Chir. 2020, 124, 351–362. [Google Scholar]
- Gopal, S. Syndecans in Inflammation at a Glance. Front. Immunol. 2020, 11, 227. [Google Scholar] [CrossRef] [Green Version]
- Soto, Y.; Mesa, N.; Alfonso, Y.; Pérez, A.; Batlle, F.; Griñán, T.; Pino, A.; Viera, J.; Frómeta, M.; Brito, V.; et al. Targeting arterial wall sulfated glycosaminoglycans in rabbit atherosclerosis with a mouse/human chimeric antibody. MAbs 2014, 6, 1340–1346. [Google Scholar] [CrossRef] [Green Version]
- Miranda, C.H.; de Carvalho Borges, M.; Schmidt, A.; Marin-Neto, J.A.; Pazin-Filho, A. Evaluation of the endothelial glycocalyx damage in patients with acute coronary syndrome. Atherosclerosis 2016, 247, 184–188. [Google Scholar] [CrossRef]
- Tran-Dinh, A.; Diallo, D.; Delbosc, S.; Varela-Perez, L.M.; Dang, Q.B.; Lapergue, B.; Burillo, E.; Michel, J.B.; Levoye, A.; Martin-Ventura, J.L.; et al. HDL and endothelial protection. Br. J. Pharmacol. 2013, 169, 493–511. [Google Scholar] [CrossRef] [Green Version]
- Vo, S.; Charnaux, N.; Richard, B. Syndecan-1 is overexpressed during atherogenesis. Atherosclerosis 2015, 241, e76. [Google Scholar] [CrossRef]
- Mitu, O.; Crisan, A.; Redwood, S.; Cazacu-Davidescu, I.-E.; Mitu, I.; Costache, I.-I.; Onofrei, V.; Miftode, R.-S.; Costache, A.-D.; Haba, C.M.S.; et al. The Relationship between Cardiovascular Risk Scores and Several Markers of Subclinical Atherosclerosis in an Asymptomatic Population. J. Clin. Med. 2021, 10, 955. [Google Scholar] [CrossRef]
- Von Haehling, S.; Ebner, N.; Dos Santos, M.R.; Springer, J.; Anker, S.D. Muscle wasting and cachexia in heart failure: Mechanisms and therapies. Nat. Rev. Cardiol. 2017, 14, 323–341. [Google Scholar] [CrossRef]
- Ather, S.; Chan, W.; Chillar, A.; Aguilar, D.; Pritchett, A.M.; Ramasubbu, K.; Wehrens, X.H.; Deswal, A.; Bozkurt, B. Association of systolic blood pressure with mortality in patients with heart failure with reduced ejection fraction: A complex relationship. Am. Heart J. 2011, 161, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Frydland, M.; Ostrowski, S.R.; Møller, J.E.; Hadziselimovic, E.; Holmvang, L.; Ravn, H.B.; Jensen, L.O.; Pettersson, A.S.; Kjaergaard, J.; Lindholm, M.G.; et al. Plasma Concentration of Biomarkers Reflecting Endothelial Cell- and Glycocalyx Damage are Increased in Patients with Suspected ST-Elevation Myocardial Infarction Complicated by Cardiogenic Shock. Shock 2018, 50, 538–544. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Acute Heart Failure (No = 120) | Control Group (No = 53) | p-Value | |
|---|---|---|---|---|
| Mean ± STD | Mean ± STD | |||
| Age (years) | 66.4 ± 15.3 | 64 ± 11.9 | 0.526 | |
| In-hospital mortality rate: No, (%) | 21 (12.1%) | 0 (0%) | <0.001 | |
| Gender | Men | 71 (59.20%) | 33 (62.30%) | 0.438 |
| Women | 49 (40.80%) | 20 (37.70%) | ||
| Smoking: No, (%) | 48 (40%) | 19 (35.8%) | 0.605 | |
| Alcohol abuse: No, (%) | 75 (62.5%) | 22 (41.5%) | 0.012 | |
| Arterial hypertension: No, (%) | 60 (50%) | 34 (64.2%) | 0.085 | |
| Ischemic heart disease: No, (%) | 59 (49.2%) | 17 (32%) | 0.037 | |
| Diabetes mellitus No, (%) | 22 (18.3%) | 7 (13.2%) | 0.406 | |
| BMI > 30 kg/m2 N, (%) | 42 (35%) | 7 (13.2%) | 0.003 | |
| LVEF | 33.8 ± 13.9% | 52.2 ± 15.7 | 0.017 | |
| Anemia: No, (%) | 35 (29.2%) | 12(22.7%) | 0.377 | |
| Loop diuretics | 102 (85%) | 17 (32.1%) | <0.001 | |
| MRA | 83 (69.2%) | 9 (17%) | <0.001 | |
| Beta-blockers | 99 (82.5%) | 49 (92.5%) | 0.087 | |
| RAS inhibitor | 77 (64.2%) | 44 (83.1%) | 0.012 | |
| Biomarker | Patient Group | No. | Median (IQR:25–75) | p-Value |
|---|---|---|---|---|
| Syndecan-1 (ng/mL) | Acute HF | 120 | 121.4 (69.3–257.9) | 0.015 |
| Control group | 53 | 72.1 (41.4–135.8) | ||
| NT-proBNP (pg/mL) | Acute HF | 120 | 5440 (2812–12791) | <0.01 |
| Control group | 53 | 107.8 (41.3–325.2) | ||
| High-sensitive Troponin (ng/L) | Acute HF | 120 | 40.1 (12.4–179.5) | <0.01 |
| Control group | 53 | 2.2 (1.1–5.4) |
| Area under the Curve | ||||
|---|---|---|---|---|
| Test Result Variable(s) | Area | p | Asymptotic 95% Confidence Interval | |
| Lower Bound | Upper Bound | |||
| NT-proBNP | 0.976 | <0.0001 | 0.952 | 1.000 |
| hs-troponin | 0.839 | <0.0001 | 0.733 | 0.944 |
| Syndecan-1 | 0.898 | <0.0001 | 0.845 | 0.951 |
| Echocardiographic Parameter | Syndecan-1 | |
|---|---|---|
| p | r | |
| LVEF | 0.663 | −0.040 |
| LVEDD | 0.567 | −0.053 |
| PAPs | 0.114 | 0.145 |
| E/e’ | 0.029 | 0.177 |
| Prognostic Parameter | Syndecan-1 | NT-proBNP | hs-Troponin | |||
|---|---|---|---|---|---|---|
| p | r | p | r | p | r | |
| In-hospital mortality | 0.185 | 0.129 | 0.093 | 0.154 | 0.071 | 0.166 |
| Total mortality at 1 month | 0.097 | 0.149 | 0.015 | 0.222 | 0.087 | 0.157 |
| Need for inotropic support | 0.024 | 0.206 | 0.461 | 0.064 | 0.989 | 0.001 |
| Non-invasive ventilation (CPAP) | 0.033 | 0.189 | 0.271 | 0.101 | 0.787 | 0.031 |
| Invasive ventilation (OTI) | 0.182 | 0.127 | 0.964 | 0.004 | 0.796 | 0.024 |
| Hospitalization duration | 0.205 | 0.106 | 0.545 | 0.049 | 0.307 | −0.094 |
| Biomarkers | Syndecan-1 < 121 ng/L | Syndecan-1 > 121 ng/L | p-Value | |
|---|---|---|---|---|
| Mortality Rate (%) | ||||
| NT-proBNP < 5440 pg/mL | 11.5% | 23.1% | <0.01 | |
| NT-proBNP > 5440 pg/mL | 15.4% | 50% | <0.01 | |
| Troponin < 40 ng/L | 15.4% | 23.1% | 0.04 | |
| Troponin > 40 ng/L | 15.4% | 46.1% | <0.01 | |
| Variable | Syndecan-1 (ng/mL) Mean ± STD | p |
|---|---|---|
| Alcoholic Non-alcoholic | 205.6 ± 203.9 | 0.457 |
| 179.8 ± 143.4 | ||
| Smoker Non-smoker | 202.9 ± 182.7 | 0.735 |
| 191.3 ± 184.3 | ||
| Pre-existing chronic liver disease Without pre-existing chronic liver disease | 209.5 ± 196.6 | 0.395 |
| 180.9 ± 146.8 | ||
| Hepatic cytolysis at admission Without hepatic cytolysis at admission | 222.3 ± 192.4 | 0.011 |
| 149.3 ± 158.4 | ||
| Pre-existing chronic kidney disease Without pre-existing chronic kidney disease | 207.9 ± 177.1 | 0.601 |
| 189.7 ± 187.2 | ||
| Acute kidney injury early after admission Without acute kidney injury early after admission | 213.1 ± 212.9 | 0.045 |
| 156.3 ± 153.5 | ||
| Pre-existing cancer pathology Without pre-existing cancer pathology | 255.2 ± 289.3 | 0.189 |
| 189.4 ± 168.1 | ||
| Systolic blood pressure <90 mmHg Systolic blood pressure ≥90 mmHg | 237.5 ± 203.1 | 0.036 |
| 159.9 ± 137.7 | ||
| Heart rate ≥100/min Heart rate <100/min | 235.9 ± 209.4 | 0.020 |
| 158.6 ± 146.4 | ||
| SaO2 ≥90% SaO2 <90% | 198.8 ± 188.3 | 0.709 |
| 181.1 ± 150.3 | ||
| LV ejection fraction <40% LV ejection fraction ≥40% | 200.6 ± 181.9 | 0.724 |
| 190.3 ± 186.2 | ||
| Fasting blood glucose ≥126 mg/dL Fasting blood glucose <126 mg/dL | 181.2 ± 169.4 | 0.486 |
| 162.7 ± 172.4 | ||
| Pre-existing diabetes Without pre-existing diabetes | 165.8 ± 119.3 | 0.395 |
| 202.7 ± 192.3 | ||
| C-reactive protein ≥0.5 mg/dL C-reactive protein <0.5 mg/dL | 175.4 ± 177.1 | 0.234 |
| 132.9 ± 141.0 | ||
| BMI <30 kg/m2 BMI ≥30 kg/m2 | 236.3 ± 201.2 | 0.041 |
| 180.0 ± 173.1 |
| Pathologic Serum Level at Discharge | Syndecan-1 at Admission | |
|---|---|---|
| p | r | |
| AST | 0.011 | 0.197 |
| ALT | 0.015 | 0.195 |
| Urea | 0.039 | 0.155 |
| Creatinine | 0.027 | 0.162 |
| Metabolic Parameter | Syndecan-1 | |
|---|---|---|
| p | R | |
| Total cholesterol | 0.079 | 0.161 |
| LDL-cholesterol | 0.240 | 0.108 |
| HDL-cholesterol | 0.016 | −0.219 |
| Triglyceride | 0.910 | 0.010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miftode, R.-S.; Costache, I.-I.; Constantinescu, D.; Mitu, O.; Timpau, A.-S.; Hancianu, M.; Leca, D.-A.; Miftode, I.-L.; Jigoranu, R.-A.; Oancea, A.-F.; et al. Syndecan-1: From a Promising Novel Cardiac Biomarker to a Surrogate Early Predictor of Kidney and Liver Injury in Patients with Acute Heart Failure. Life 2023, 13, 898. https://doi.org/10.3390/life13040898
Miftode R-S, Costache I-I, Constantinescu D, Mitu O, Timpau A-S, Hancianu M, Leca D-A, Miftode I-L, Jigoranu R-A, Oancea A-F, et al. Syndecan-1: From a Promising Novel Cardiac Biomarker to a Surrogate Early Predictor of Kidney and Liver Injury in Patients with Acute Heart Failure. Life. 2023; 13(4):898. https://doi.org/10.3390/life13040898
Chicago/Turabian StyleMiftode, Radu-Stefan, Irina-Iuliana Costache, Daniela Constantinescu, Ovidiu Mitu, Amalia-Stefana Timpau, Monica Hancianu, Daniela-Anicuta Leca, Ionela-Larisa Miftode, Raul-Alexandru Jigoranu, Alexandru-Florinel Oancea, and et al. 2023. "Syndecan-1: From a Promising Novel Cardiac Biomarker to a Surrogate Early Predictor of Kidney and Liver Injury in Patients with Acute Heart Failure" Life 13, no. 4: 898. https://doi.org/10.3390/life13040898