1. Introduction
Conventional retinal photocoagulation (PC) is an established therapy that has become part of the standard treatment for various retinal and choroidal diseases, especially in diabetic retinopathy [
1]. The energy is converted into heat, leading to thermal damage of the retinal pigment epithelium (RPE), neuroretina and the choroid [
2]. A side effect of this therapy is irreversible damage to the retinal structures and associated scotomas as well as the development of RPE-related atrophic areas [
3]. This is particularly problematic in the treatment of macular pathologies, especially because the developing atrophic areas can expand over time and localized parafoveal laser foci can involve the fovea leading to a central scotoma [
4].
To avoid these undesirable side effects of laser therapy, photodisruptive selective retina therapy (SRT) with sparing of the photoreceptor layer was developed. SRT uses pulse durations below 5 µs, which results in selective RPE cell disruption by intracellular microbubble formation and does not affect the neuroretina or choroid. The microvaporization-induced local RPE defects are closed by the proliferation and migration of neighboring pigment epithelial cells [
5]. It is postulated that these remodeling processes contribute to the restructuring of the blood–retinal barrier, the improvement of metabolic functions of the RPE and therefore act as a rejuvenating therapy for the RPE [
6]. The regenerating RPE cells subsequently form a functional closed tissue structure. This defect closure in the treated area occurs usually within one to two weeks after irradiation [
7,
8,
9]. SRT has shown therapeutic success in central serous chorioretinopathy and diabetic macular edema [
8,
10,
11,
12]. No side effects or complications of this procedure have been reported so far [
5,
6,
12,
13]. One problem in the clinical application of SRT is that neither the optimal irradiation parameters nor the standard treatment strategies regarding the application geometry of laser foci, the number of spots and repetitive treatment regimens have been reported and so far are only based on common therapeutic regimes of conventional laser coagulation treatment [
8]. To facilitate the procedure, an SRT system with real-time feedback technology was developed with the idea of auto-stopping the laser when the microbubble formation is detected [
7,
14].
Central serous chorioretinopathy (CSC) is a common disease of the posterior segment of the eye, which typically presents with a dome-shaped neuroretinal detachment due to accumulation of subretinal fluid (SRF), retinal pigment epithelium (RPE) dysfunction, and hyperpermeability and thickening of the underlying choroid. Patients with CSC suffer from central vision loss, scotomas, micropsia or metamorphopsia, hypermetropisation, and reduced contrast sensitivity [
15]. The complex clinical picture and not conclusively clarified pathogenesis of this disease complicate the search for an optimal treatment method. To avoid long-term RPE damage caused by SRF, complete resolution of all fluid should be the primary goal of treatment; however, due to the high spontaneous remission rate with good visual prognosis, therapy should demonstrate a good safety profile [
16]. Peripheral retinal pathologies that present with leakage are commonly treated using thermal laser photocoagulation. However, due to the associated visual field defects caused by the destruction of the neurosensory retina, macular treatment by conventional thermal laser photocoagulation is problematic in CSC and contraindicated in the fovea [
10]. Half-dose photodynamic therapy (PDT), involving intravenous administration of verteporfin (Visudyne
® by Novartis, Basel, Switzerland), has proven to be a successful treatment for CSC [
17]. However, due to the persistent global verteporfin shortage, which remains a long-term concern, alternative treatments are urgently needed [
18]. SRT has already demonstrated efficacy in clinical studies, including its use in treating foveal central serous chorioretinopathy cases [
19,
20]. Furthermore, a network meta-analysis indirectly compared SRT with a placebo for CSC, and found a significant effect on the resolution of subretinal fluid [
21].
Some studies investigating the safety aspects of SRT already found no adverse effects during the observation period. Studies in which electrophysiological examinations were performed after SRT found no changes in electroretinography (ERG) and multifocal ERG, suggesting the absence of photoreceptor damage [
2,
22]. Furthermore, microperimetry after SRT showed no loss of retinal sensitivity and thus no scotomas [
20,
23]. Additionally, the oxygen consumption of photoreceptors remained unchanged after SRT, indicating that their function and metabolism were unaltered [
24].
An important factor regarding safety of the treatment is the long-term effect. In conventional laser therapy, the zone of lethal damage is not necessarily visible initially; however, as the laser-induced RPE atrophy continues to expand for years, a phenomenon called atrophic creep is observable [
25,
26]. In this study, the long-term effect of SRT on the human retina was evaluated using multimodal imaging over a period of three years.
3. Results
Our study followed up 36 subjects (eyes) of 33 patients with central serous chorioretinopathy who were treated with SRT. All of these eyes were monitored for one year, 20 (56%) for up to two years, and 10 (28%) for up to three years.
3.1. Demographic Data
A total of 29 (88%) males and four (12%) females affected with CSC was included in the study. Significantly more males were affected (p > 0.001). The right eye was affected in 13 (36%) cases while the left eye was affected in 23 (64%) cases (p = 0.132). The average age of subjects was 46.2 ± 8.6 years.
3.2. SRT Energy Characteristics
The average energy needed to see a visible whitening reaction for titration purposes was 179.4 ± 29.0 µJ (minimum 110 µJ, maximum 220 µJ). The average energy used for macular treatment was 143.3 ± 21.7 µJ (minimum 90 µJ, maximum 180 µJ).
3.3. Morphological Changes
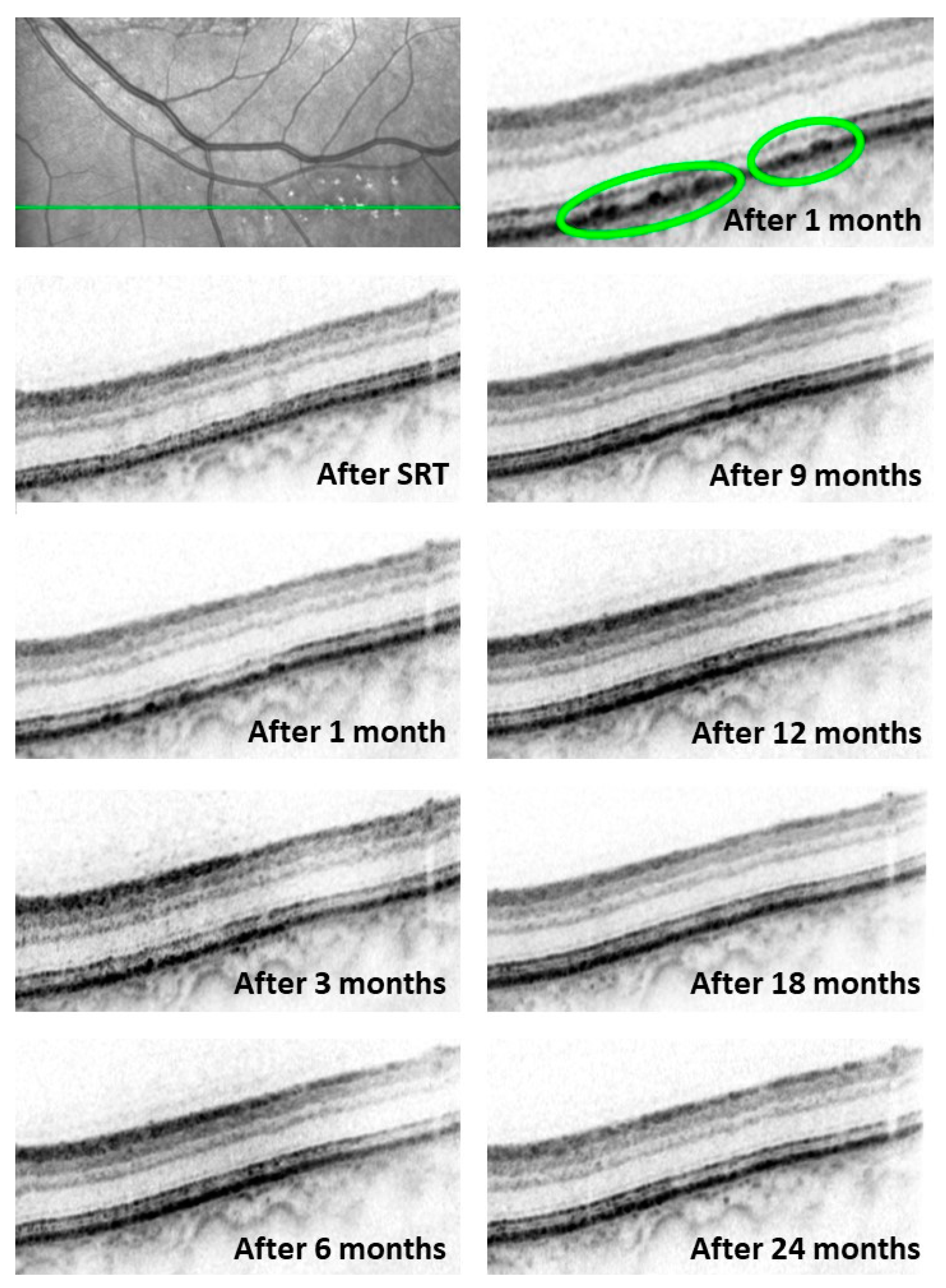
No changes in SD-OCT scans of the titration lesions were observed immediately after performing the SRT procedures. Dune-shaped thickenings of the RPE and consecutive changes in the interdigitation zone were seen one month after treatment. In some cases, isolated gaps in the RPE layer were seen adjacent to the dune-shaped thickenings. These changes in the RPE layer regressed over time and returned to a normal OCT morphology after 11.5 ± 9.3 months. Changes within the interdigitation zone disappeared after 17.7 ± 10.1 days and therefore could be observed for a longer period than those in the RPE layer (
p = 0.0033). Changes in the RPE and interdigitation zone morphology at the baseline and over 24 months are presented in
Figure 1.
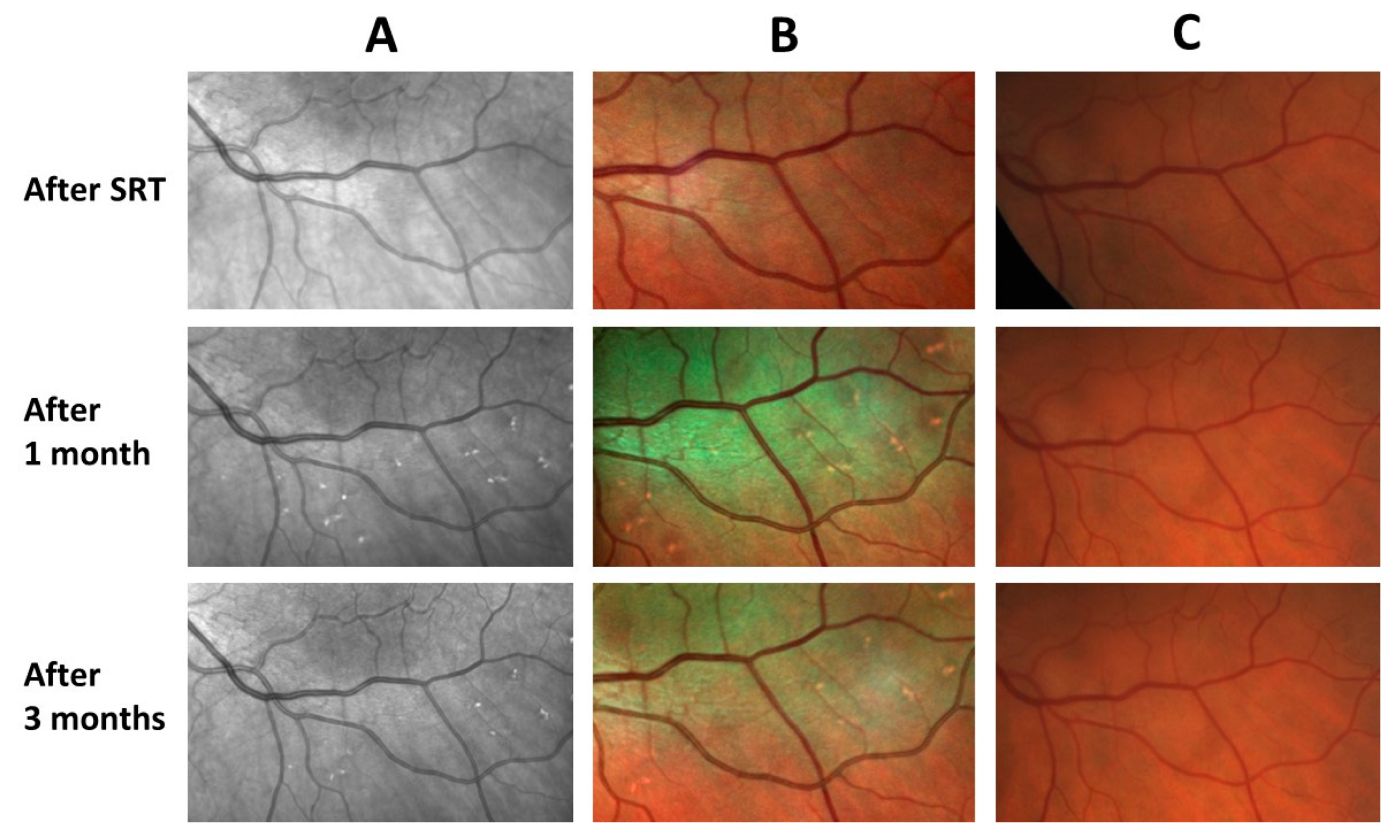
The SRT lesions were not visible either clinically or in the fundus photography. The lesions appeared as brightly reflecting areas in infrared and multicolor images (
Figure 2).
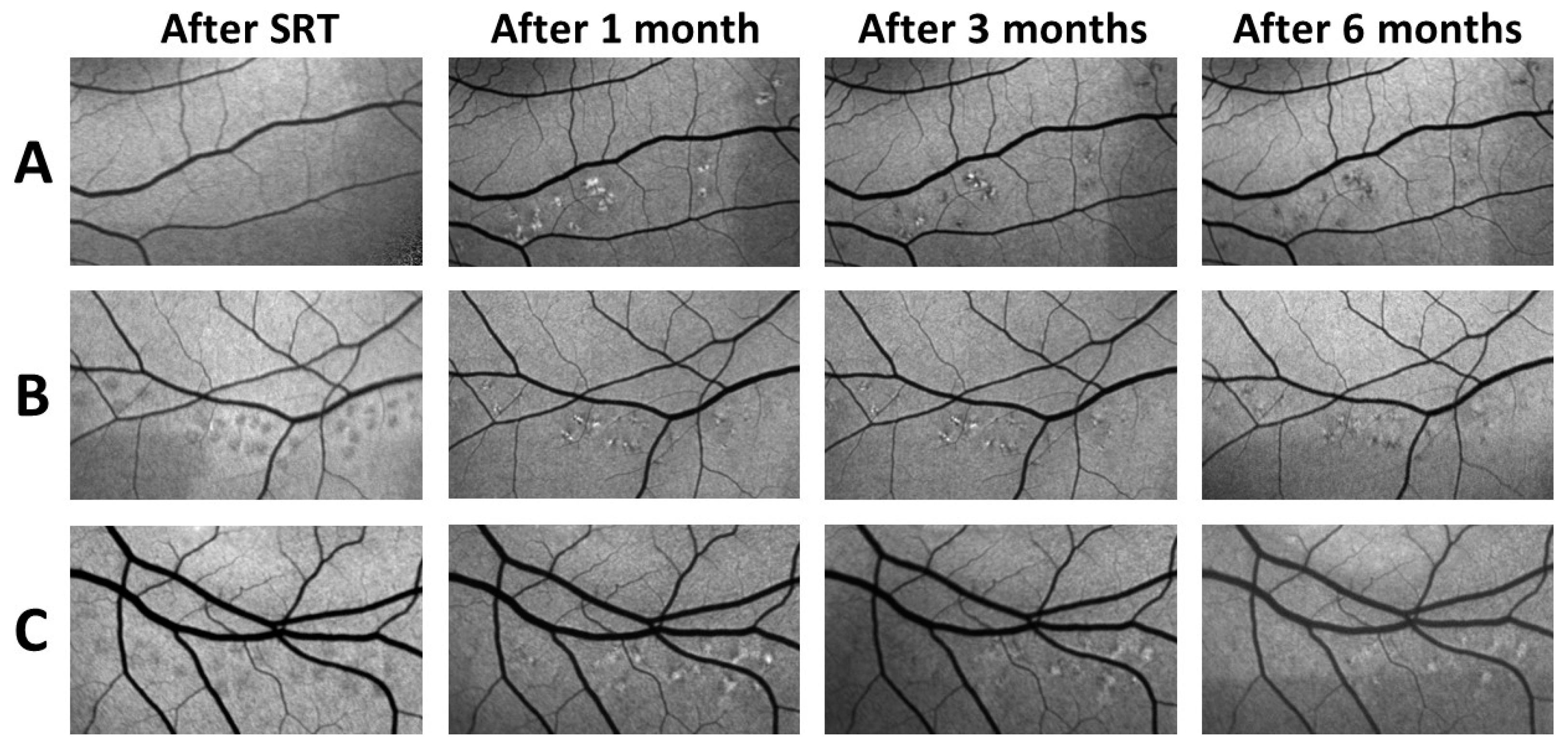
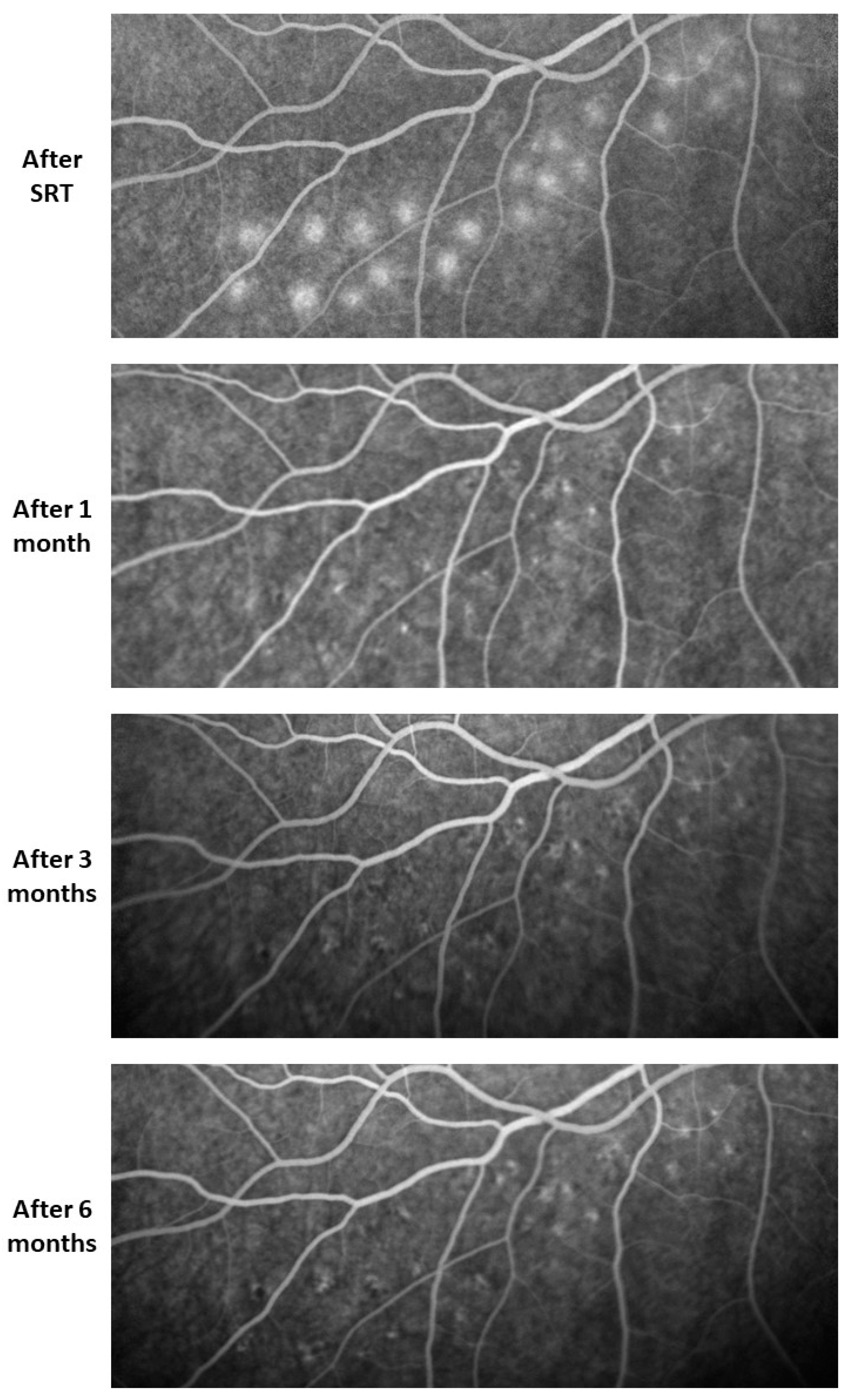
Fundus autofluorescence showed a diverse pattern of alterations induced by SRT which varied from patient to patient. In most subjects, areas of increased autofluorescence were observed immediately after SRT; however, in some patients this effect was absent. One month later, these lesions appeared as areas of increased FAF with partial decreased FAF. In the following examinations, different patterns were observed. In some cases, the foci faded continuously; in some patients, the lesions with mixed increased and decreased FAF faded gradually, whereas in others a constant increase in autofluorescence persisted but subsided over time. However, most patients showed reduced FAF in the later follow-ups (
Figure 3). In the further follow-up period, the changes remained constant or regressed. Furthermore, no RPE atrophies developed in the observed period of three years (
Figure 4).
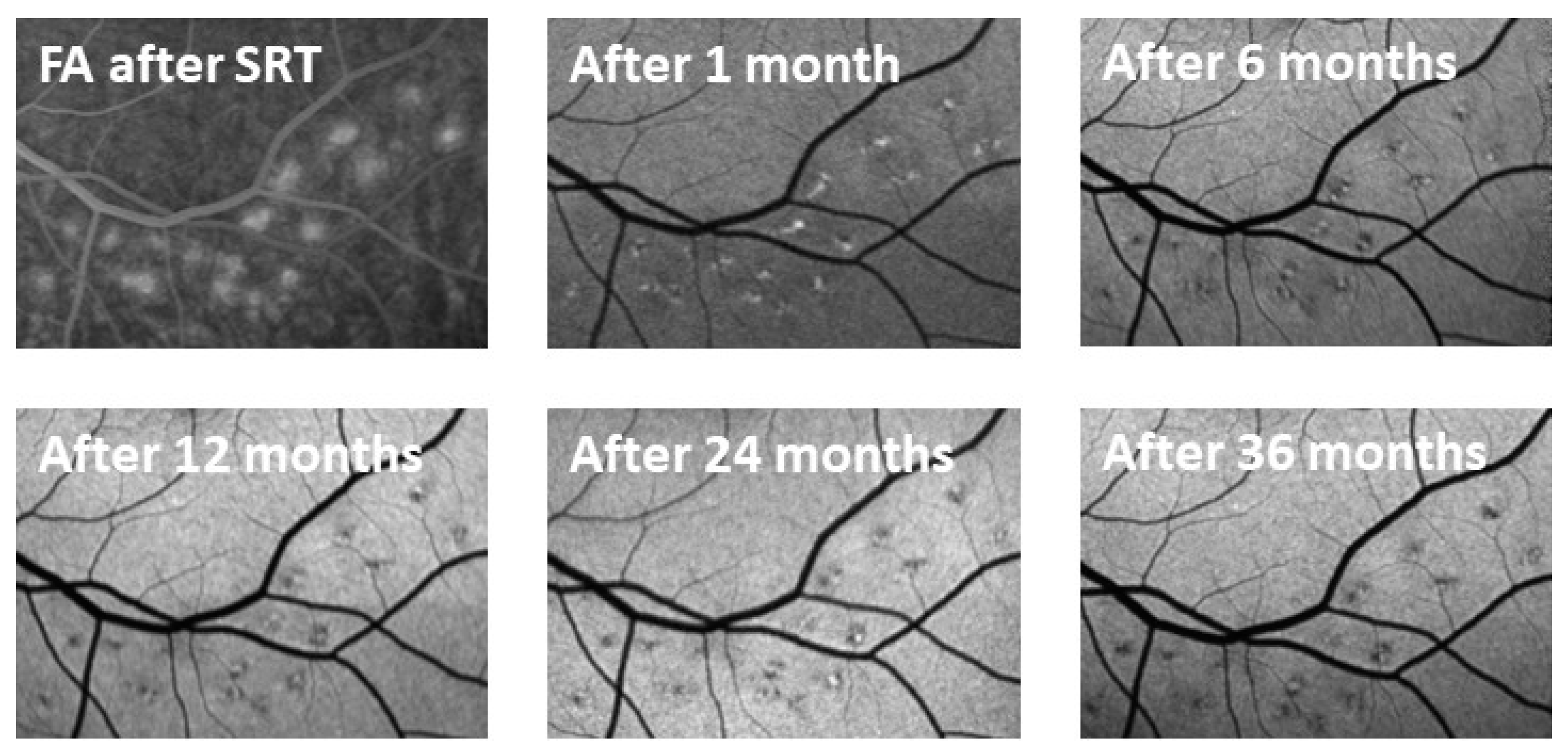
Leakage and thus the destruction of RPE cells were observed in FA performed immediately after SRT at the lesions where higher energy was used. One month later, there was no longer any leakage visible in FA. Hyperfluorescent spots interspersed with hypofluorescent areas were observed. These changes diminished over the months (
Figure 5).
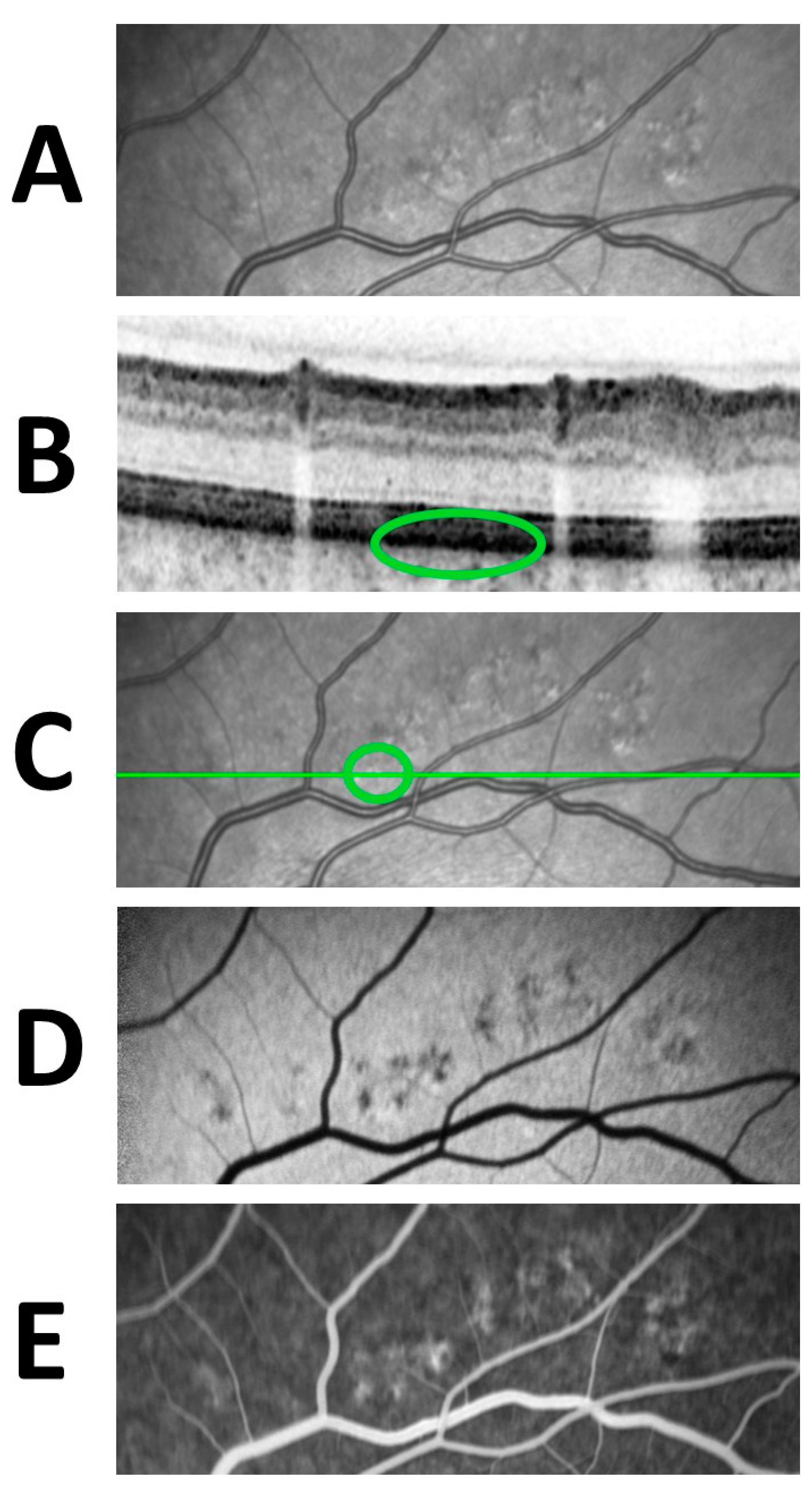
Taking into consideration the combined changes in various imaging techniques, it was observed that the hypo-autofluorescent areas seen in FAF are seen as hyperfluorescent areas in FA (
Figure 6). These transmitted choroidal hyperfluorescence, so-called window defects, decreased in size during the follow-up.
3.4. SRT Lesion Characteristics
An average of 27.6 ± 7.0 test lesions was applied (minimum 14, maximum 42). Of all the applied lesions, 15.9 ± 8.3 (58 ± 28%) were visible in the initial fluorescein angiography performed directly after irradiation. The fluorescein angiography directly after SRT showed no visible test lesions in three cases. No initial fluorescein angiography was performed on three patients due to earlier described adverse effects following FA.
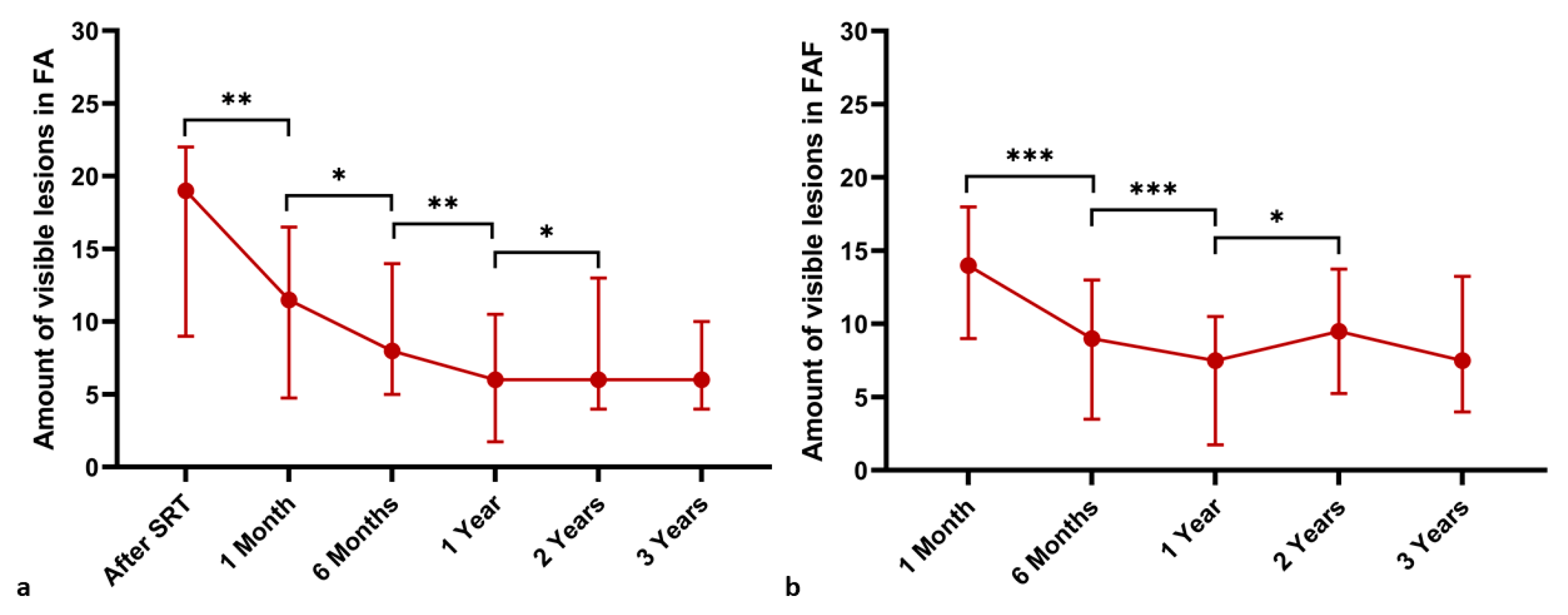
The number of visible SRT test lesions in FAF and FA was examined at the baseline, at one- and six-month as well as one-, two- and three-year follow-up examinations. Fundus autofluorescence was performed prior to the SRT treatment at the baseline but was not repeated right after the procedure. A significant decrease in the number of visible test lesions in FA and FAF was observed between each follow-up examination for up to two years (
p < 0.05). Changes in the number of visible lesions in the baseline and follow-up FAF and FA examinations are presented in
Figure 7 and
Table 1.
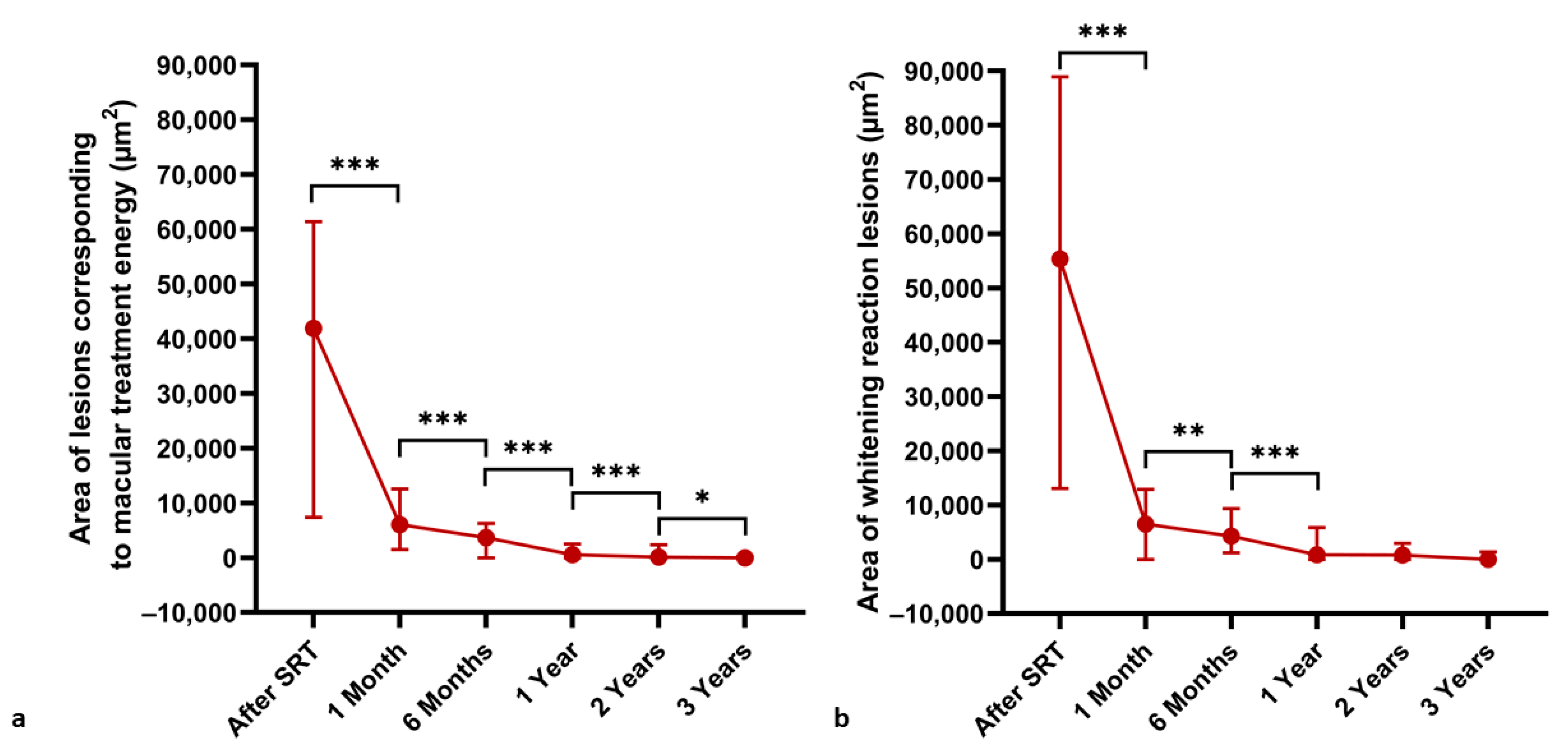
The SRT spot size was measured over time at titration lesions corresponding to macular treatment energy and lesions with visible whitening reaction for titration purposes (
Figure 8). A steady significant decrease in the area (µm
2) of lesions corresponding to the treatment energy was observed between all examinations (
p < 0.05). Meanwhile, the area (µm
2) of visible whitening reaction lesions decreased over time up to the one-year follow-up examination and then stabilized (
p < 0.01).
Correlation analysis showed no significant correlation between the energy used for macular treatment and the size of the corresponding titration lesions at one-, three-, six-, twelve- and twenty-four-month follow-up examinations (r = −0.14–+0.09; p > 0.3). Subject age showed no significant correlation with the amount of energy required to see a visible whitening reaction of the titration lesions (r = 0.08; p = 0.507), treatment energy (r = 0.14; p = 0.227) or the number of visible lesions in FA at the baseline (r = −0.16; p = 0.212). Age was not associated with area of lesions corresponding with macular treatment energy at the baseline or any of the follow-up examinations (r = −0.32–+0.05; p > 0.09). The Mann–Whitney U test showed no significant difference between males and females in the distribution of visible titration lesions in FA (15.9 ± 8.4; median 19, IQR 13 vs. 15.3 ± 6.9; median 17, IQR 14; p = 0.64), the area of lesions corresponding to macular treatment energy (44,331 ± 35,497; median 44,071, IQR 58,478 vs. 29,046 ± 11,686 µm; median 29,633, IOR 23,000; p = 0.16), and visible whitening lesions (54,022 ± 38,431; median 55,659, IQR 77,432 vs. 40,947 ± 30,933 µm; median 44,873, IQR 55,504, p = 0.41) at the baseline as well as the energy needed to reach the visible whitening effect (179.3 ± 29.5; median 180, IQR 40 vs. 177.5 ± 31.5 µJ; median 185, IQR 63; p = 1.0).
4. Discussion
In this study, the effect of SRT treatment on healthy retina in cCSC was evaluated in multimodal imaging over time. Analysis of OCT images showed dune-shaped thickenings in the RPE layer and irregularities in the interdigitation zone one month after SRT treatment. All of these changes regressed over time and normal morphology of the retina in OCT images was observed in an average of 17.7 ± 10.1 months. Our study shows no evidence of RPE atrophy after SRT irradiation. Correlation analysis showed no correlation between absolute energy and the effect of SRT. This shows that there is no critical absolute energy needed to see the effect of SRT and underlines the importance of titration because different energy values are needed in each individual due to anatomic differences, for example, in the pigmentation of the fundus. Furthermore, age and sex had no influence over the SRT effect; therefore, there is no need to adjust the treatment energy for these variables.
As previously reported in various animal studies, histological examinations have shown that RPE defects caused by performing SRT laser treatment are closed through hypertrophy and migration of the neighboring cells. This remodeling process usually lasts about one week or up to four weeks in the longest cases yet reported [
7,
9,
24]. Thickenings in the RPE layer observed in OCT images of our subjects were consistent with the findings reported in animal studies. Consequently, these data suggest that an analogous remodeling process occurs in both humans and animals. However, morphological changes in OCT images were observed over a significantly longer time period in the subjects of this study. This indicates that the regenerative process of the RPE and retina induced by SRT treatment takes longer in humans than in animals. This is also consistent with another study showing changes in OCT morphology for up to six months in patients treated with SRT [
12].
Alterations were never seen in fundus photography. Changes seen in OCT correlated with altered areas observed in FA and FAF, that were also visible in infrared and multicolor images. The FAF technique is based on the emission of short wavelength autofluorescence by lipofuscin in RPE cells. As a consequence of photoreceptor phagocytosis, lipofuscin accumulates in RPE cells [
27]. Thus, FAF is an indicator of metabolism in the cells [
15]. As previously reported, decreased FAF can be detected immediately after SRT treatment. Framme et al. attributed this effect to a blockade to autofluorescence caused by the destruction of RPE cells and a focal edema [
27]. This provides a good explanation for reduced FAF in the areas where SRT was performed, because edematous changes at the tips of the outer photoreceptor segments were also found in histological examinations up to seven days after SRT laser treatment in animals [
9,
24]. Furthermore, lipofuscin in a solution, after RPE cell destruction, shows decreased autofluorescence [
26]. This could also partly explain the initial decline in FAF. In this study, a decreased FAF was also observed after SRT and can be explained by RPE destruction and an intraretinal edema, as mentioned above.
Many studies observed a switch in FAF after one week; lesions showed increased autofluorescence and remained stable for up to 15 months. The authors attributed this to an increased RPE metabolism and the corresponding increase in fluorophore concentration [
27]. However, the reported descriptions of FAF changes one month after SRT are mixed. Another group found increased FAF at the areas of irradiation only in a few lesions three months after SRT was performed [
11]. Other studies reported a disappearance of the lesions in FAF after three months, but the subtle changes described in our work can still be seen in the figures of these studies [
12,
14]. None of these studies provided an explanation for the mixed autofluorescence in the treated spots which sometimes persist over several years.
In this study, a complete or partial increase in FAF of some SRT lesions was observed after one month. However, at six months and onwards the same spots showed primarily a decreased autofluorescence with portions of increased FAF. A study on Chinchilla Bastard rabbits revealed a similar freckled pattern of SRT lesions in FAF as early as seven days after SRT [
28]. This shows again the analogous processes in both humans and animals, which occur sooner in animals.
Increased FAF may result from an increase in intracellular lipofuscin. This is a byproduct of RPE cell debris being phagocytized by other RPE cells as well as accumulated photoreceptor outer segments being phagocytized by regenerated RPE cells. Microglia originating from the neuroretina and macrophages originating from the choriocapillaris are also attracted and contribute to removal of the debris. This explanation was proposed by previous studies to justify similar changes observed in FAF after conventional laser treatment [
12]. Histological studies in animal models showed hypertrophic RPE cells of various sizes and heights with enhanced phagocytic activity, which resulted in intracellularly cellular debris in the first days following SRT irradiation [
2,
9]. This explains the increased FAF observed after one month in this study. In porcine organ cultures, closure of SRT-induced defects caused by migration and proliferation were observed within five days. However, those cells showed an altered morphology and SRT treatment increased active MMP expression, resulting in the pathologically swollen Bruch’s membrane becoming thinner [
6]. It is stated that this leads to a restored and rejuvenated RPE but may also explain altered FAF due to altered morphology and metabolism.
In this study, FA images showed hyperfluorescent areas because of an enhanced transmission of choroidal fluorescence, a so-called window defect, in the areas of reduced FAF. Usually, this corresponds to RPE atrophy [
15]. However, in this study OCT imaging showed no RPE atrophy in the irradiated areas. This phenomenon could be explained by findings from cell culture studies. When pigmented primary human RPE cells are cultured, they rapidly lose pigment granules as they are shared between daughter cells; this occurs because critical components of the melanogenesis pathway are no longer expressed in adult human RPE [
29]. Animal studies also described a layer of hypopigmented and hyperpigmented RPE cells with apical melanin granules covering the defect 14 days after SRT [
2,
9].
A combination of the above-mentioned factors could explain the altered FAF and window-defects. Following SRT, the RPE defect is closed by the hypertrophy and migration of surrounding cells. These cells phagocytose RPE debris, resulting in increased lipofuscin uptake, leading to an increase in FAF. However, the regenerating RPE cells show reduced or no intracellular melanin, because adult RPE cells are no longer able to synthesize it. Thus, window defects are in seen in FA in these areas. Furthermore, the rejuvenated RPE cells show an increased active MMP expression and altered morphology, which also results in a change in FAF. It is particularly important to note that no RPE atrophies developed throughout the observed period after laser treatment.
All of this shows that while changes in the FAF are observed over three years, they do not represent RPE atrophy but rather regenerative processes. The RPE monolayer regenerated and photoreceptors remained intact in all cases during the observation period of three years. In contrast to continuous-wave laser treatment, where scarring processes and expanding atrophic creep are observed, changes in the FAF after SRT have even been shown to shrink over time. Interestingly, this also applies to the irradiated spots with a barely visible whitening reaction, which are necessary for titration. This indicates that SRT may have an even wider therapeutic range than previously assumed.
SRT has been shown to thin a pathologically thickened Bruch membrane, regenerate the rejuvenated RPE and lead to decreased vascular endothelial growth factor (VEGF) release and increased release of the VEGF antagonist, pigment epithelium-derived factor (PEDF) [
6]. Thus, SRT could also be a promising therapy option for age-related macular degeneration (AMD). However, it is essential to ensure that no damage to the RPE and photoreceptors occurs through treatment when applying irradiation in the fovea. The LEAD trial treated AMD patients using a 532-nm Q-switched neodymium-doped yttrium–aluminum–garnet laser with ultra-short 3-nanosecond pulse durations along the vascular arcades. Not only did the study fail its primary endpoint of inhibiting conversion of intermediate to neovascular AMD, the treatment also led to deep retinal hemorrhages in 6.8% of the participants [
30]. This results in photoreceptor and RPE damage and can potentially lead to the development of neovascularization, and therefore is contraindicated for macular and foveal treatment. In contrast, SRT has already been shown to slow the progression of intermediate AMD by improving mean retinal sensitivity measured by microperimetry and reducing the rate of change in drusen load in a pilot study. However, due to safety concerns, treatment was performed at least 1500 μm away from the center of the fovea in this study [
7]. Nevertheless, the results of our study emphasize the absence of RPE and photoreceptor damage even three years after SRT and thus support the idea that early maculopathies and other pathologies in the fovea may be treated with SRT as well.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}