
Decreased Levels of Vitamin D in Bipolar Patients

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Assessment Scales
2.2. Mini International Neuropsychiatric Interview (MINI)
2.3. Hamilton Rating Scale for Depression (HRSD)
2.4. Young Mania Rating Scale (YMRS)
2.5. Clinical Global Impression-Severity (CGI-s)
2.6. Statistical Analyses
2.7. Plasma Preparation for Vitamin D Assessment
3. Results
3.1. Socio-Demographic and Clinical Data
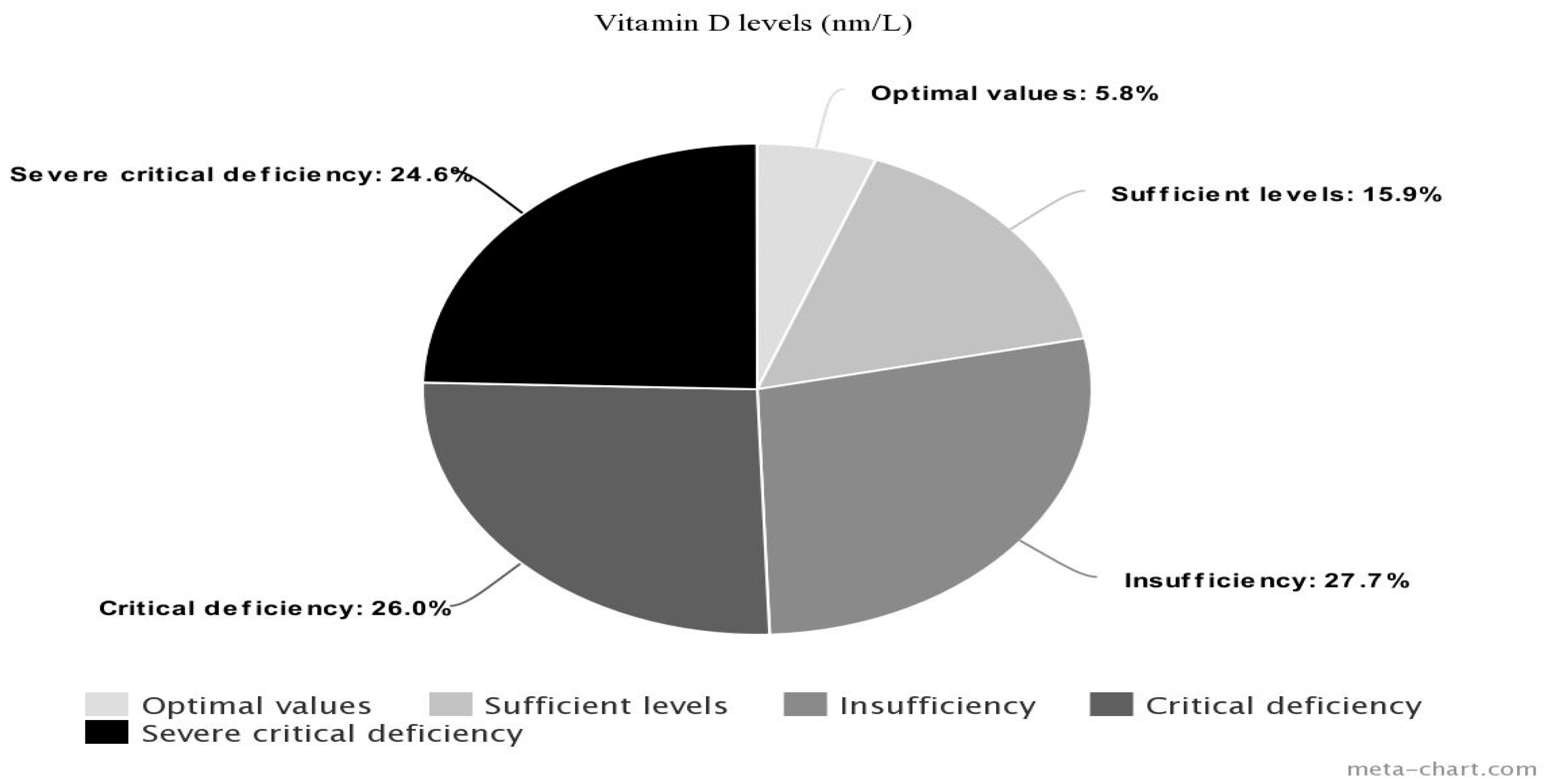
3.2. Vitamin D
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders—Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017; p. 24. [Google Scholar]
- Romera, I.; Perez, V.; Menchón, J.M.; Delgado-Cohen, H.; Polavieja, P.; Gilaberte, I. Social and occupational functioning impairment in patients in partial versus complete remission of a major depressive disorder episode. A six-month prospective epidemiological study. Eur. Psychiatry 2010, 25, 58–65. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; DSM-5; American Psychiatric Press: Washington, DC, USA, 2013; ISBN 9783801728038. [Google Scholar]
- Saveanu, R.V.; Nemeroff, C.B. Etiology of Depression: Genetic and Environmental Factors. Psychiatr. Clin. N. Am. 2012, 35, 51–71. [Google Scholar] [CrossRef] [PubMed]
- Long, S.-J.; Benton, D. Effects of Vitamin and Mineral Supplementation on Stress, Mild Psychiatric Symptoms, and Mood in Nonclinical Samples: A meta-analysis. Psychosom. Med. 2013, 75, 144–153. [Google Scholar] [CrossRef]
- O’Connell, K.S.; Coombes, B.J. Genetic contributions to bipolar disorder: Current status and future directions. Psychol. Med. 2021, 51, 2156–2167. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Carmassi, C.; Mucci, F.; Marazziti, D. Depression, Serotonin and Tryptophan. Curr. Pharm. Des. 2016, 22, 949–954. [Google Scholar] [CrossRef]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [Green Version]
- Marazziti, D.; Mucci, F.; Fontenelle, L.F. Immune system and obsessive-compulsive disorder. Psychoneuroendocrinology 2018, 93, 39–44. [Google Scholar] [CrossRef]
- Gordovez, F.J.A.; McMahon, F.J. The genetics of bipolar disorder. Mol. Psychiatry 2020, 25, 544–559. [Google Scholar] [CrossRef]
- Mucci, F.; Marazziti, D.; Della Vecchia, A.; Baroni, S.; Morana, P.; Carpita, B.; Mangiapane, P.; Morana, F.; Morana, B.; Dell’Osso, L. State-of-the-Art: Inflammatory and Metabolic Markers in Mood Disorders. Life 2020, 10, 82. [Google Scholar] [CrossRef]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2014, 99, 181–197. [Google Scholar] [CrossRef] [Green Version]
- Mangiapane, P.; Carbone, M.G.; Arone, A.; Massa, L.; Palermo, S.; Flamini, W.; Parra, E.; Morana, B.; Morana, F.; Bertini, G.; et al. Vitamin B12, homocysteine, and folic acid in patients suffering from bipolar disorders: Relationship with suicide. World J. Biol. Psychiatry 2022, 23, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Ford, A.H.; Flicker, L. Systematic review and meta-analysis of randomized placebo-controlled trials of folate and vitamin B12 for depression. Int. Psychogeriatr. 2015, 27, 727–737. [Google Scholar] [CrossRef]
- Petridou, E.T.; Kousoulis, A.A.; Michelakos, T.; Papathoma, P.; Dessypris, N.; Papadopoulos, F.C.; Stefanadis, C. Folate and B12 serum levels in association with depression in the aged: A systematic review and meta-analysis. Aging Ment. Health 2015, 20, 965–973. [Google Scholar] [CrossRef]
- Bender, A.; Hagan, K.E.; Kingston, N. The association of folate and depression: A meta-analysis. J. Psychiatr. Res. 2017, 95, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Bičíková, M.; Dušková, M.; Vítků, J.; Kalvachová, B.; Řípová, D.; Mohr, P.; Stárka, L. Vitamin D in Anxiety and Affective Disorders. Physiol. Res. 2015, 64, S101–S103. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.B.; Brotchie, H.; Graham, R.K. Vitamin D and depression. J. Affect. Disord. 2017, 208 (Suppl. S2), 56–61. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Parra, E.; Palermo, S.; Barberi, F.M.; Buccianelli, B.; Ricciardulli, S.; Cappelli, A.; Mucci, F.; Dell’Osso, L. Vitamin D: A Pleiotropic Hormone with Possible Psychotropic Activities. Curr. Med. Chem. 2021, 28, 3843–3864. [Google Scholar] [CrossRef] [PubMed]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef] [Green Version]
- Diaz, G.D.; Paraskeva, C.; Thomas, M.G.; Binderup, L.; Hague, A. Apoptosis is induced by the active metabolite of vitamin D3 and its analogue EB1089 in colorectal adenoma and carcinoma cells: Possible implications for prevention and therapy. Cancer Res. 2000, 60, 2304–2312. [Google Scholar] [PubMed]
- Chun, R.F.; Liu, P.T.; Modlin, R.L.; Adams, J.S.; Hewison, M. Impact of vitamin D on immune function: Lessons learned from genome-wide analysis. Front. Physiol. 2014, 5, 151. [Google Scholar] [CrossRef] [Green Version]
- Bivona, G.; Gambino, C.M.; Iacolino, G.; Ciaccio, M. Vitamin D and the nervous system. Neurol. Res. 2019, 41, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Chabas, J.-F.; Alluin, O.; Rao, G.; Garcia, S.; Lavaut, M.-N.; Risso, J.J.; Legre, R.; Magalon, G.; Khrestchatisky, M.; Marqueste, T.; et al. Vitamin D2Potentiates Axon Regeneration. J. Neurotrauma 2008, 25, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Neveu, I.; Naveilhan, P.; Jehan, F.; Baudet, C.; Wion, D.; De Luca, H.F.; Brachet, P. 1,25-Dihydroxyvitamin D3 regulates the synthesis of nerve growth factor in primary cultures of glial cells. Mol. Brain Res. 1994, 24, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Bianco, J.I.; McGrath, J.J.; Eyles, D.W. 1,25-Dihydroxyvitamin D3 induces nerve growth factor, promotes neurite outgrowth and inhibits mitosis in embryonic rat hippocampal neurons. Neurosci. Lett. 2003, 343, 139–143. [Google Scholar] [CrossRef]
- Ibi, M.; Sawada, H.; Nakanishi, M.; Kume, T.; Katsuki, H.; Kaneko, S.; Shimohama, S.; Akaike, A. Protective effects of 1α,25-(OH)2D3 against the neurotoxicity of glutamate and reactive oxygen species in mesencephalic culture. Neuropharmacology 2001, 40, 761–771. [Google Scholar] [CrossRef]
- Garcion, E.; Wion-Barbot, N.; Montero-Menei, C.N.; Berger, F.; Wion, D. New clues about vitamin D functions in the nervous system. Trends Endocrinol. Metab. 2002, 13, 100–105. [Google Scholar] [CrossRef]
- Spiro, A.; Buttriss, J.L. Vitamin D: An overview of vitamin D status and intake in Europe. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef] [Green Version]
- Nerhus, M.; Berg, A.O.; Kvitland, L.R.; Dieset, I.; Hope, S.; Dahl, S.R.; Weibell, M.A.; Romm, K.L.; Faerden, A.; Andreassen, O.A.; et al. Low vitamin D is associated with negative and depressive symptoms in psychotic disorders. Schizophr. Res. 2016, 178, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Borges-Vieira, J.G.; Cardoso, C.K.S. Efficacy of B-vitamins and vitamin D therapy in improving depressive and anxiety disorders: A systematic review of randomized controlled trials. Nutr. Neurosci. 2023, 26, 187–207. [Google Scholar] [CrossRef]
- Modan-Moses, D.; Levy-Shraga, Y.; Pinhas-Hamiel, O.; Kochavi, B.; Enoch-Levy, A.; Vered, I.; Stein, D. High prevalence of vitamin D deficiency and insufficiency in adolescent inpatients diagnosed with eating disorders. Int. J. Eat. Disord. 2015, 48, 607–614. [Google Scholar] [CrossRef]
- Marazziti, D.; Barberi, F.M.; Fontenelle, L.; Buccianelli, B.; Carbone, M.G.; Parra, E.; Palermo, S.; Massa, L.; Tagliarini, C.; Della Vecchia, A.; et al. Decreased vitamin D levels in obsessive-compulsive disorder patients. CNS Spectr. 2021, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Terock, J.; Hannemann, A.; Van der Auwera, S.; Janowitz, D.; Spitzer, C.; Bonk, S.; Völzke, H.; Grabe, H.J. Posttraumatic stress disorder is associated with reduced vitamin D levels and functional polymorphisms of the vitamin D binding-protein in a population-based sample. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 96, 109760. [Google Scholar] [CrossRef] [PubMed]
- Siracusano, M.; Riccioni, A.; Abate, R.; Benvenuto, A.; Curatolo, P.; Mazzone, L. Vitamin D Deficiency and Autism Spectrum Disorder. Curr. Pharm. Des. 2020, 26, 2460–2474. [Google Scholar] [CrossRef]
- Black, L.J.; Jacoby, P.; Allen, K.L.; Trapp, G.S.; Hart, P.H.; Byrne, S.M.; Mori, T.A.; Beilin, L.J.; Oddy, W.H. Low vitamin D levels are associated with symptoms of depression in young adult males. Aust. N. Z. J. Psychiatry 2013, 48, 464–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, Y.S.; Kim, S.; Jeong, J.-H.; Jung, Y.-E.; Kim, M.-D.; Bahk, W.-M. Vitamin D Deficiency/Insufficiency among Inpatients with Depressive Symptoms. Clin. Psychopharmacol. Neurosci. 2019, 17, 121–124. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Hoogendijk, W.; Lips, P.; Heijboer, A.C.; Schoevers, R.; van Hemert, A.M.; Beekman, A.T.; Smit, J.H.; Penninx, B.W. The association between low vitamin D and depressive disorders. Mol. Psychiatry 2013, 19, 444–451. [Google Scholar] [CrossRef]
- Stewart, R.; Hirani, V. Relationship Between Vitamin D Levels and Depressive Symptoms in Older Residents From a National Survey Population. Psychosom. Med. 2010, 72, 608–612. [Google Scholar] [CrossRef]
- Manzanos, I.; Martino, P.; Audisio, E.; Bonet, J. Vitamin D: Between the Brightness of the sun and the Darkness of Depression. Rev. Colomb. Psiquiatr. 2020, 38, 199–205. [Google Scholar] [CrossRef]
- Khan, B.; Shafiq, H.; Abbas, S.; Jabeen, S.; Khan, S.A.; Afsar, T.; Almajwal, A.; Alruwaili, N.W.; Al-Disi, D.; Alenezi, S.; et al. Vitamin D status and its correlation to depression. Ann. Gen. Psychiatry 2022, 21, 32. [Google Scholar] [CrossRef]
- Altunsoy, N.; Yüksel, R.N.; Yirun, M.C.; Kılıçarslan, A.; Aydemir, Ç. Exploring the relationship between vitamin D and mania: Correlations between serum vitamin D levels and disease activity. Nord. J. Psychiatry 2018, 72, 221–225. [Google Scholar] [CrossRef]
- Boerman, R.; Cohen, D.; Schulte, P.F.; Nugter, A. Prevalence of Vitamin D Deficiency in Adult Outpatients With Bipolar Disorder or Schizophrenia. J. Clin. Psychopharmacol. 2016, 36, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-Y.; Huang, M.-C.; Chiu, C.C.; Cheng, Y.-C.; Kuo, C.-J.; Chen, P.-Y.; Kuo, P.-H. The interactions between vitamin D and neurofilament light chain levels on cognitive domains in bipolar disorder. BJPsych Open 2022, 8, e207. [Google Scholar] [CrossRef]
- Cereda, G.; Enrico, P.; Ciappolino, V.; Delvecchio, G.; Brambilla, P. The role of vitamin D in bipolar disorder: Epidemiology and influence on disease activity. J. Affect. Disord. 2020, 278, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Grønli, O.; Kvamme, J.M.; Jorde, R.; Wynn, R. Vitamin D deficiency is common in psychogeriatric patients, independent of diagnosis. BMC Psychiatry 2014, 14, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sikoglu, E.M.; Navarro, A.A.L.; Starr, D.; Dvir, Y.; Nwosu, B.U.; Czerniak, S.M.; Rogan, R.C.; Castro, M.C.; Edden, R.A.; Frazier, J.A.; et al. Vitamin D3Supplemental Treatment for Mania in Youth with Bipolar Spectrum Disorders. J. Child Adolesc. Psychopharmacol. 2015, 25, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Vellekkatt, F.; Menon, V. Efficacy of vitamin D supplementation in major depression: A meta-analysis of randomized controlled trials. J. Postgrad. Med. 2018, 65, 74–80. [Google Scholar] [CrossRef]
- Kaviani, M.; Nikooyeh, B.; Zand, H.; Yaghmaei, P.; Neyestani, T.R. Effects of vitamin D supplementation on depression and some involved neurotransmitters. J. Affect. Disord. 2020, 269, 28–35. [Google Scholar] [CrossRef]
- Vellekkatt, F.; Menon, V.; Rajappa, M.; Sahoo, J. Effect of adjunctive single dose parenteral Vitamin D supplementation in major depressive disorder with concurrent vitamin D deficiency: A double-blind randomized placebo-controlled trial. J. Psychiatr. Res. 2020, 129, 250–256. [Google Scholar] [CrossRef]
- Hansen, J.P.; Pareek, M.; Hvolby, A.; Schmedes, A.; Toft, T.; Dahl, E.; Nielsen, C.T. Vitamin D3 supplementation and treatment outcomes in patients with depression (D3-vit-dep). BMC Res. Notes 2019, 12, 203. [Google Scholar] [CrossRef] [Green Version]
- Marsh, W.K.; Penny, J.L.; Rothschild, A.J. Vitamin D supplementation in bipolar depression: A double blind placebo controlled trial. J. Psychiatr. Res. 2017, 95, 48–53. [Google Scholar] [CrossRef]
- Li, G.; Mbuagbaw, L.; Samaan, Z.; Falavigna, M.; Zhang, S.; Adachi, J.D.; Cheng, J.; Papaioannou, A.; Thabane, L. Efficacy of Vitamin D Supplementation in Depression in Adults: A Systematic Review. J. Clin. Endocrinol. Metab. 2014, 99, 757–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowda, U.; Mutowo, M.P.; Smith, B.J.; Wluka, A.E.; Renzaho, A.M.N. Vitamin D supplementation to reduce depression in adults: Meta-analysis of randomized controlled trials. Nutrition 2015, 31, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–33. [Google Scholar] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Busner, J.; Targum, S.D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry 2007, 4, 28. [Google Scholar]
- Moghaddam, B.; Bolinao, M.L.; Stein-Behrens, B.; Sapolsky, R. Glucocortcoids mediate the stress-induced extracellular accumulation of glutamate. Brain Res. 1994, 655, 251–254. [Google Scholar] [CrossRef]
- Kalueff, A.V.; Eremin, K.O.; Tuohimaa, P. Mechanisms of neuroprotective action of vitamin D(3). Biochemistry 2004, 69, 738–741. [Google Scholar] [CrossRef]
- Alghamdi, S.; Alsulami, N.; Khoja, S.; Alsufiani, H.; Tayeb, H.O.; Tarazi, F.I. Vitamin D Supplementation Ameliorates Severity of Major Depressive Disorder. J. Mol. Neurosci. 2020, 70, 230–235. [Google Scholar] [CrossRef]
- Zhu, C.; Zhang, Y.; Wang, T.; Lin, Y.; Yu, J.; Xia, Q.; Zhu, P.; Zhu, D.M. Vitamin D supplementation improves anxiety but not depression symptoms in patients with vitamin D deficiency. Brain Behav. 2020, 10, e01760. [Google Scholar] [CrossRef]
- Omidian, M.; Mahmoudi, M.; Abshirini, M.; Eshraghian, M.R.; Javanbakht, M.H.; Zarei, M.; Hasani, H.; Djalali, M. Effects of vitamin D supplementation on depressive symptoms in type 2 diabetes mellitus patients: Randomized placebo-controlled double-blind clinical trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2375–2380. [Google Scholar] [CrossRef] [PubMed]
- Högberg, G.; Hällström, T.; Gustafsson, S.A.; Gustafsson, T.; Klawitter, B.; Petersson, M. Depressed adolescents in a case-series were low in vitamin D and depression was ameliorated by vitamin D supplementation. Acta Paediatr. 2012, 101, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Khoraminya, N.; Tehrani-Doost, M.; Jazayeri, S.; Hosseini, A.; Djazayery, A. Therapeutic effects of vitamin D as adjunctive therapy to fluoxetine in patients with major depressive disorder. Aust. N. Z. J. Psychiatry 2012, 47, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Geng, C.; Shaikh, A.S.; Han, W.; Chen, D.; Guo, Y.; Jiang, P. Vitamin D and depression: Mechanisms, determination and application. Asia Pac. J. Clin. Nutr. 2019, 28, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Huang, T.; Lou, D.; Fu, R.; Ni, C.; Hong, J.; Ruan, L. Effect of vitamin D supplementation on the incidence and prognosis of depression: An updated meta-analysis based on randomized controlled trials. Front. Public Health 2022, 10, 903547. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiari-Dovvombaygi, H.; Izadi, S.; Moghaddam, M.Z.; Hashemzehi, M.; Hosseini, M.; Azhdari-Zarmehri, H.; Dinpanah, H.; Beheshti, F. Beneficial effects of vitamin D on anxiety and depression-like behaviors induced by unpredictable chronic mild stress by suppression of brain oxidative stress and neuroinflammation in rats. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2020, 394, 655–667. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Haussler, M.R.; Haussler, C.A.; Jurutka, P.W.; Thompson, P.D.; Hsieh, J.C.; Remus, L.S.; Selznick, S.H.; Whitfield, G.K. The vitamin D hormone and its nuclear receptor: Molecular actions and disease states. J. Endocrinol. 1997, 154, S57–S73. [Google Scholar]
- Cui, X.; Pelekanos, M.; Liu, P.-Y.; Burne, T.H.J.; McGrath, J.J.; Eyles, D.W. The vitamin D receptor in dopamine neurons; its presence in human substantia nigra and its ontogenesis in rat midbrain. Neuroscience 2013, 236, 77–87. [Google Scholar] [CrossRef]
- Melcangi, R.C.; Panzica, G. Neuroactive steroids: An update of their roles in central and peripheral nervous system. Psychoneuroendocrinology 2009, 34 (Suppl. S1), S1–S8. [Google Scholar] [CrossRef]
- Landel, V.; Stephan, D.; Cui, X.; Eyles, D.; Feron, F. Differential expression of vitamin D-associated enzymes and receptors in brain cell subtypes. J. Steroid Biochem. Mol. Biol. 2018, 177, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Marini, F.; Bartoccini, E.; Cascianelli, G.; Voccoli, V.; Baviglia, M.G.; Magni, M.V.; Garcia-Gil, M.; Albi, E. Effect of 1α,25-dihydroxyvitamin D3 in embryonic hippocampal cells. Hippocampus 2010, 20, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, H.A.; Rasouli, J.; Ciric, B.; Rostami, A.; Zhang, G.-X. 1,25-Dihydroxyvitamin D3 enhances neural stem cell proliferation and oligodendrocyte differentiation. Exp. Mol. Pathol. 2015, 98, 240–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, J.; Gurbani, G.S. Association of vitamin D deficiency and mood disorders: A systematic review. In Vitamin D Defciency; Fetodova, J., Ed.; IntetechOpen: London, UK, 2019. [Google Scholar]


{kind=link}
| Total Patients (69: 29 M; 40 F) | Age: 45.09 ± 14.42 |
|---|---|
| Diagnoses | |
| BDI (27: 11 M, 16 F) | |
| BDII (15: 4 M, 11 F) | |
| Schizoaffective (16: 11 M, 5 F) | |
| MDD (11: 3 M, 8 F) | |
| Mood episode | |
| Manic (6: 4 M; 2 F) | |
| Hypomanic (7: 3 M, 4 F) | |
| Depressive (36: 12 M; 24 F) | |
| Mixed (20: 10 M, 10 F) | |
| Subjects | Values | N |
|---|---|---|
| Total sample | 14.58 ± 11.27 | 69 |
| Women | 14.48 ± 10.24 | 40 |
| Men | 14.72 ± 12.74 | 29 |
| Insufficiency | 15.70 ± 2.17 | 19 |
| Critical deficiency | 9.10 ± 1.49 | 18 |
| Severe critical deficiency | 4.92 ± 1.12 | 17 |
| Sufficient levels | 24.71 ± 3.40 | 11 |
| Optimal values | 47.17 ± 16.85 | 4 |
| H | df | p | |
|---|---|---|---|
| Diagnosis | 1.010 | 3 | 0.799 |
| Episode Type | 3.083 | 3 | 0.379 |
| Second Diagnosis Type | 1.275 | 3 | 0.735 |
| Pharmacological treatment association * | 9.046 | 8 | 0.338 |
| U | Z | p | |
|---|---|---|---|
| Gender | 553,000 | −0.87 | 0.930 |
| Psychosis | 574,500 | −0.18 | 0.985 |
| Acute onset | 370,500 | −0.399 | 0.690 |
| Bipolar condition | 493,000 | −0.835 | 0.404 |
| Psychiatric comorbidity | 472,000 | −1.097 | 0.273 |
| Lithium | 365,000 | −0.970 | 0.332 |
| Tricyclics | 17,500 | −1.761 | 0.078 |
| Mood stabilizer | 345,000 | −1.143 | 0.253 |
| Double mood stabilizer | 343,500 | −0.799 | 0.424 |
| Antipsychotic | 159,500 | −0.573 | 0.567 |
| Double antipsychotic | 374,000 | −1.057 | 0.291 |
| Antidepressant | 474,000 | −0.997 | 0.319 |
| Double antidepressant | 120,500 | −0.195 | 0.845 |
| Medical comorbidity | 488,500 | −0.955 | 0.340 |
| Smoking | 556,000 | −0.256 | 0.806 |
| Psychiatric family loading | 321,500 | −0.233 | 0.816 |
| Neurodevelopmental traits | 256,500 | −0.580 | 0.562 |
| Suicidal family loading | 171,500 | −1.304 | 0.192 |
| Substance Users | 325,500 | −1.355 | 0.175 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marazziti, D.; Mangiapane, P.; Carbone, M.G.; Morana, F.; Arone, A.; Massa, L.; Palermo, S.; Violi, M.; Bertini, G.; Massoni, L.; et al. Decreased Levels of Vitamin D in Bipolar Patients. Life 2023, 13, 883. https://doi.org/10.3390/life13040883
Marazziti D, Mangiapane P, Carbone MG, Morana F, Arone A, Massa L, Palermo S, Violi M, Bertini G, Massoni L, et al. Decreased Levels of Vitamin D in Bipolar Patients. Life. 2023; 13(4):883. https://doi.org/10.3390/life13040883
Chicago/Turabian StyleMarazziti, Donatella, Paola Mangiapane, Manuel Glauco Carbone, Florinda Morana, Alessandro Arone, Lucia Massa, Stefania Palermo, Miriam Violi, Giovanni Bertini, Leonardo Massoni, and et al. 2023. "Decreased Levels of Vitamin D in Bipolar Patients" Life 13, no. 4: 883. https://doi.org/10.3390/life13040883