
Afamelanotide Is Associated with Dose-Dependent Protective Effect from Liver Damage Related to Erythropoietic Protoporphyria
Abstract
:1. Introduction
2. Patients, Material, and Methods
2.1. Patients, Treatment Schedules, and Safety Measurements
2.2. Data Sources and Statistical Analysis
2.3. Assessment of Dose-Dependent Effects of Afamelanotide
2.4. Further Statistical Analyses
3. Results
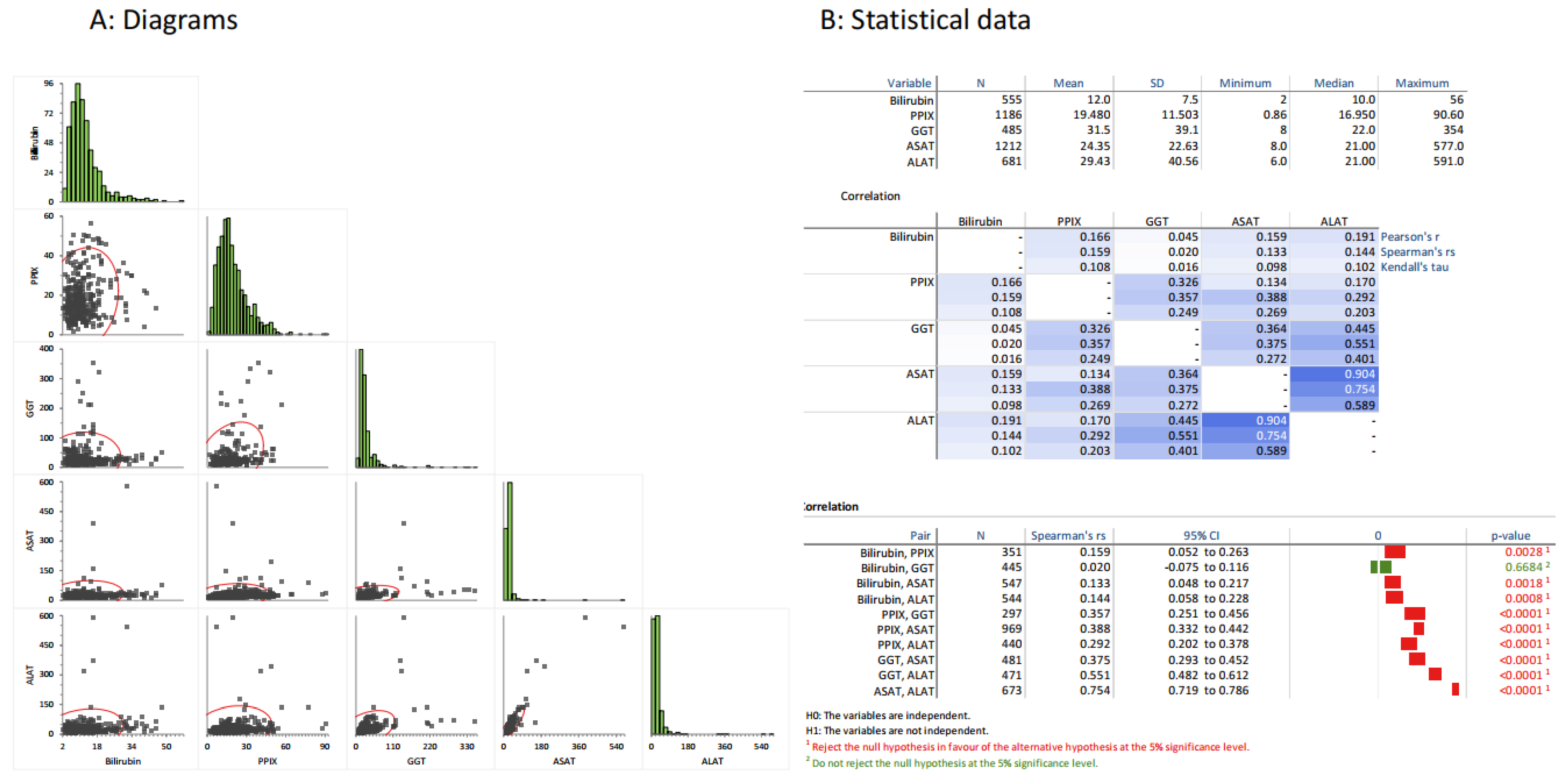
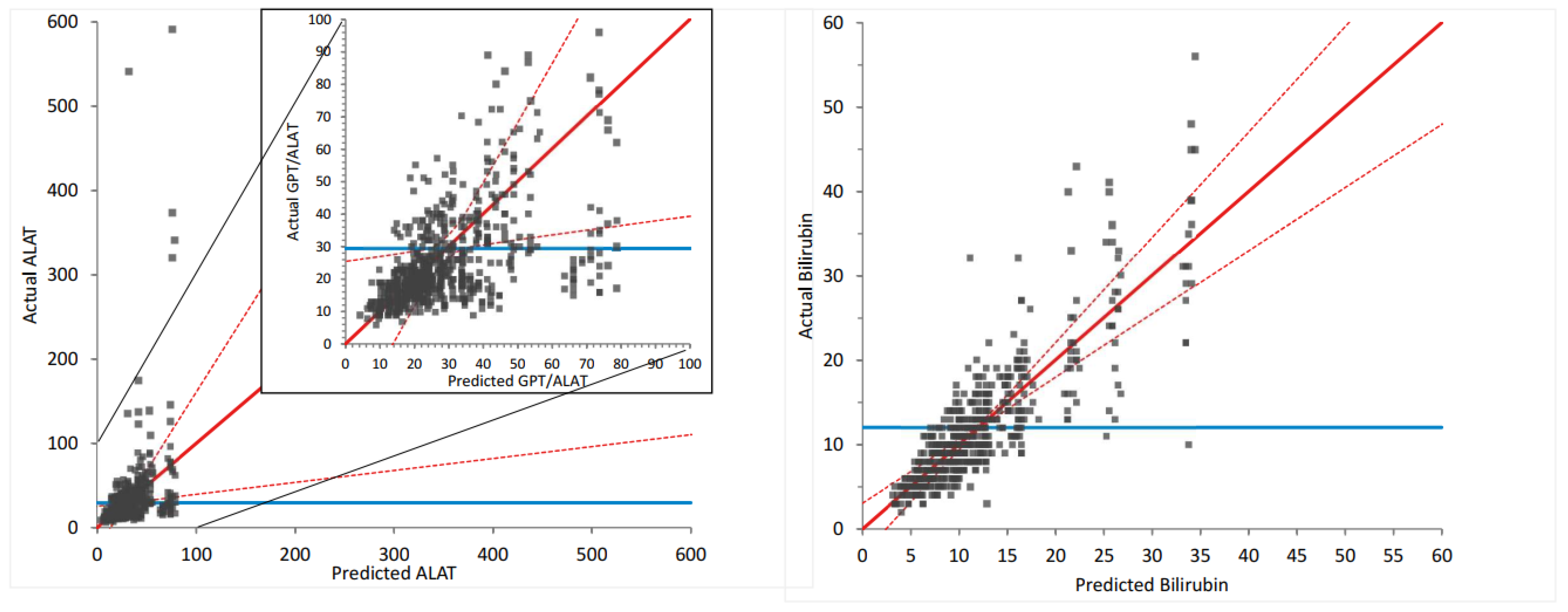
3.1. General Correlations between LFTs and PPIX
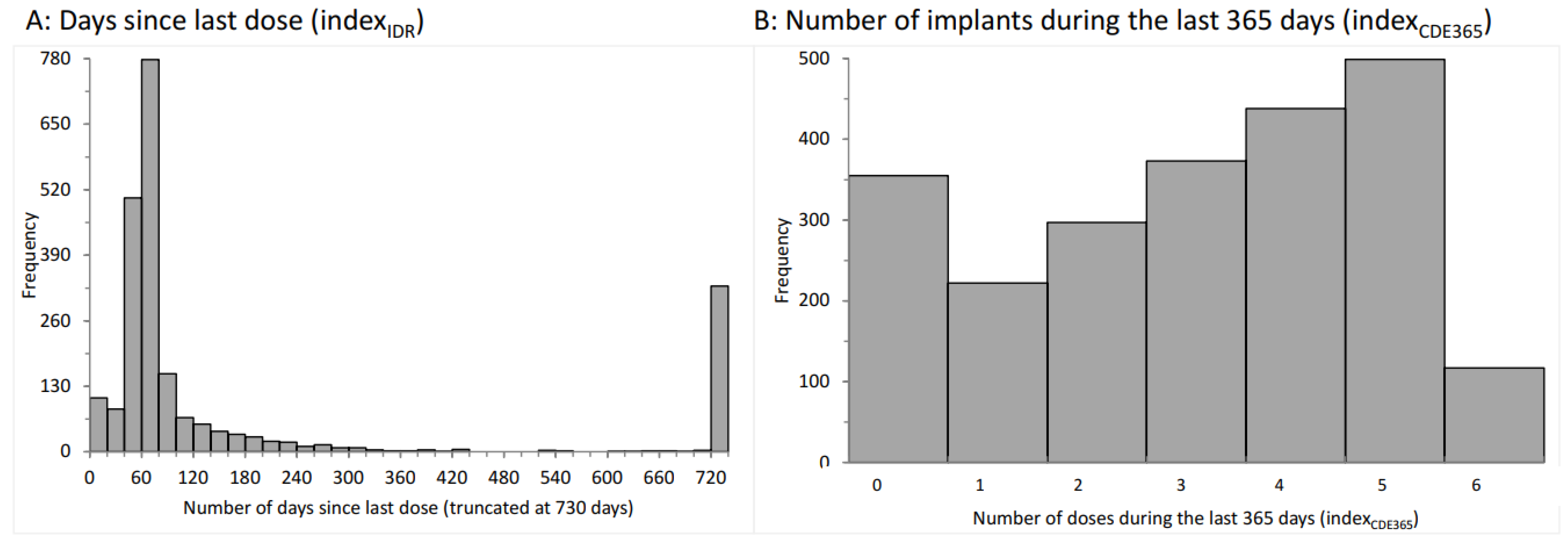
3.2. Distributions of the Indexidr and Indexcde
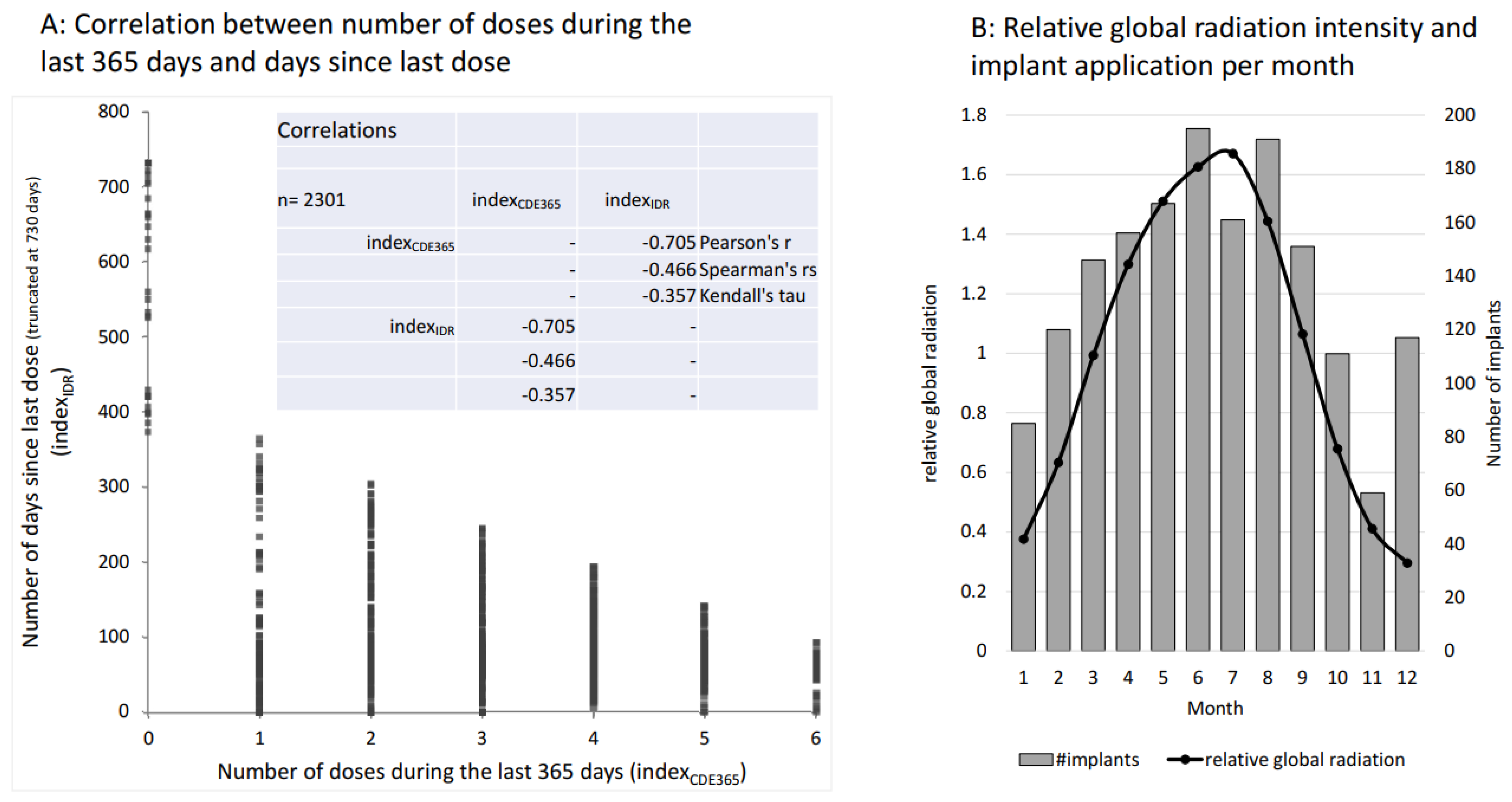
3.3. Global Radiation as an Independent Effector
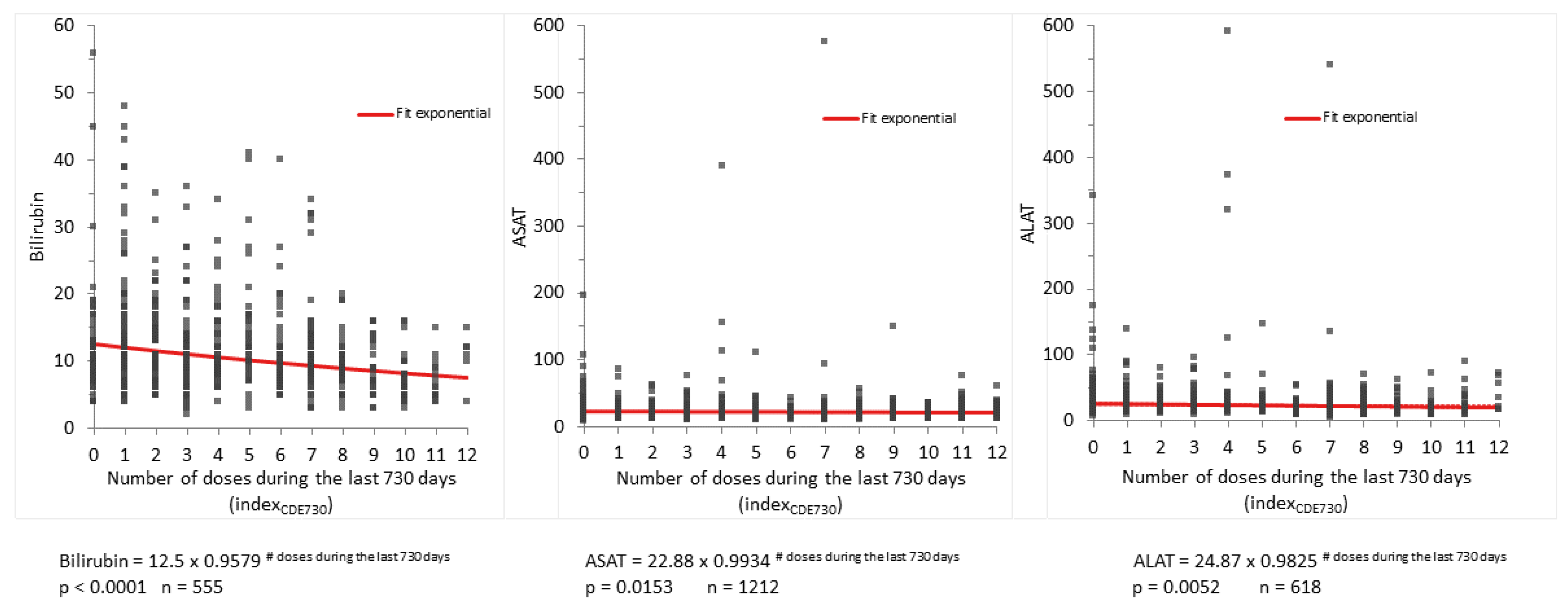
3.4. Immediate Dose-Response and Cumulative Dose Effect of Afamelanotide on PPIX Concentrations and LFTs (Table 1)
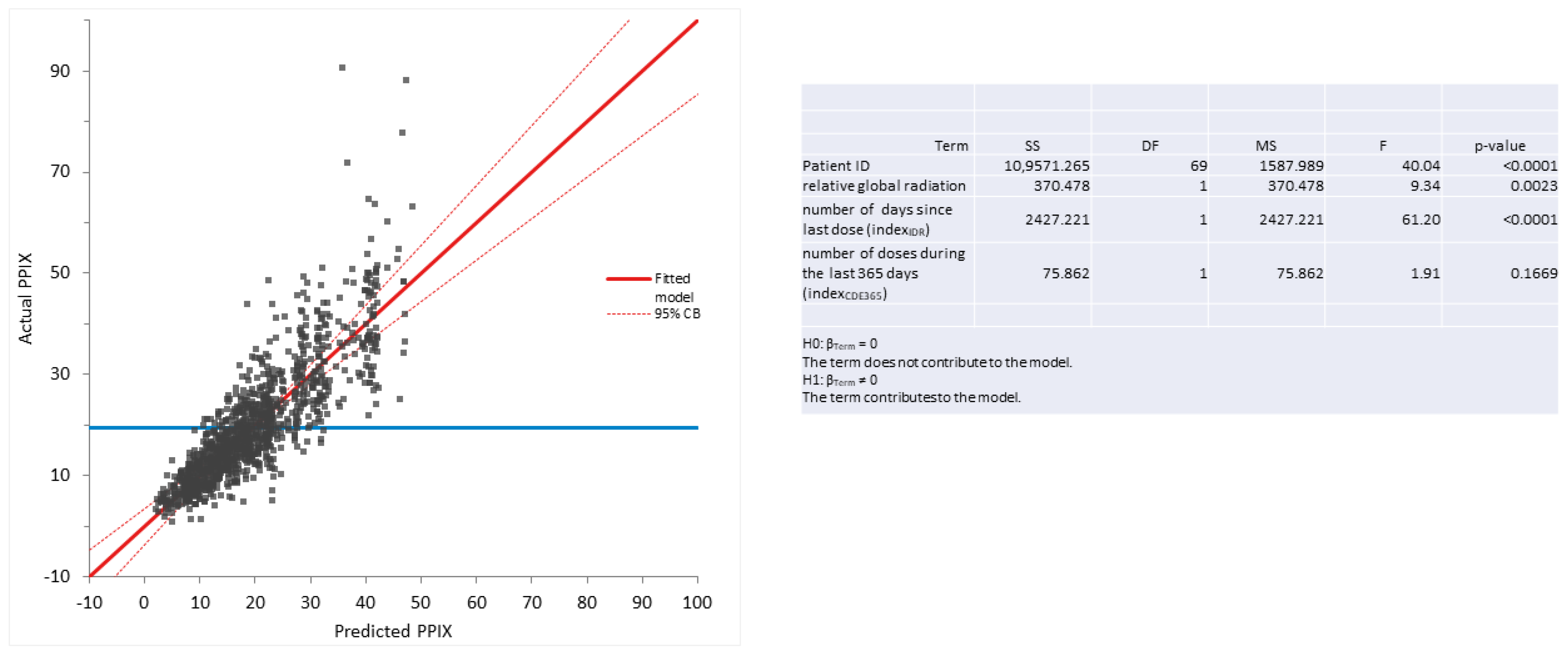
3.5. Influence of Global Radiation on PPIX Concentrations and LFTs as Assayed by Multilinear Regression Analysis (Table 1)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALAS2 | aminolevulinic acid synthase 2 |
| ALAT | alanine transaminase |
| ASAT | aspartate transaminase |
| CDE | cumulative dose effect |
| EMA | European medicine agency |
| EPP | erythropoietic protoporphyria |
| FDA | U.S. Food and Drug Administration |
| GGT | gamma-glutamyltransferase |
| IDR | immediate dose response |
| IκB | inhibitor of nuclear factor-kappa-B |
| LFT | liver function tests |
| MCR | melanocortin receptor |
| MSH | melanocyte-stimulating hormone |
| NF-κB | nuclear factor-kappa-B |
| PPIX | protoporphyrin |
| TGA | Therapeutic Goods Administration |
References
- Catania, A.; Gatti, S.; Colombo, G.; Lipton, J.M. Targeting melanocortin receptors as a novel strategy to control inflammation. Pharmacol. Rev. 2004, 56, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-H.; Jawan, B.; Lee, T.-H.; Hung, K.-S.; Chou, W.-Y.; Lu, C.-N.; Liu, J.-K.; Chen, Y.-J. Single injection of naked plasmid encoding α-melanocyte-stimulating hormone protects against thioacetamide-induced acute liver failure in mice. Biochem. Biophys. Res. Commun. 2004, 322, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Chiao, H.; Foster, S.; Thomas, R.; Lipton, J.; Star, R.A. Alpha-melanocyte-stimulating hormone reduces endotoxin-induced liver inflammation. J. Clin. Investig. 1996, 97, 2038–2044. [Google Scholar] [CrossRef]
- Lee, T.H.; Jawan, B.; Chou, W.Y.; Lu, C.N.; Wu, C.L.; Kuo, H.M.; Concejero, A.M.; Wang, C.H. Alpha-melanocyte-stimulating hormone gene therapy reverses carbon tetrachloride induced liver fibrosis in mice. J. Gene Med. 2006, 8, 764–772. [Google Scholar] [CrossRef]
- Minder, A.-E.; Barman-Aksoezen, J.; Schmid, M.; Minder, E.I.; Zulewski, H.; Minder, C.E.; Schneider-Yin, X. Beyond pigmentation: Signs of liver protection during afamelanotide treatment in Swiss patients with erythropoietic protoporphyria, an observational study. Ther. Adv. Rare Dis. 2021, 2, 26330040211065453. [Google Scholar] [CrossRef]
- Minder, E.I.; Barman-Aksoezen, J.; Schneider-Yin, X. Pharmacokinetics and Pharmacodynamics of Afamelanotide and its Clinical Use in Treating Dermatologic Disorders. Clin. Pharm. 2017, 56, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Harms, J.; Lautenschlager, S.; Minder, C.E.; Minder, E.I. An alpha-melanocyte-stimulating hormone analogue in erythropoietic protoporphyria. N. Engl. J. Med. 2009, 360, 306–307. [Google Scholar] [CrossRef]
- Langendonk, J.G.; Balwani, M.; Anderson, K.E.; Bonkovsky, H.L.; Anstey, A.V.; Bissell, D.M.; Bloomer, J.; Edwards, C.; Neumann, N.J.; Parker, C.; et al. Afamelanotide for Erythropoietic Protoporphyria. N. Engl. J. Med. 2015, 373, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Balwani, M.; Bloomer, J.; Desnick, R. Porphyrias Consortium of the NIH-Sponsored Rare Diseases Clinical Research Network. Erythropoietic Protoporphyria, Autosomal Recessive. 2012 Sep 27 [updated 2017 Sep 7]. In GeneReviews®; Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2017. [Google Scholar]
- Puy, H.; Gouya, L.; Deybach, J.C. Porphyrias. Lancet 2010, 375, 924–937. [Google Scholar] [CrossRef]
- Schneider-Yin, X.; Minder, E.I. Erythropoietic Protoporphyria and X-Linked Dominant Protoporphyria; Ferreira, G.C., Ed.; World Scientific Publishing Company: Singapore, 2013; pp. 299–328. [Google Scholar]
- Whatley, S.D.; Ducamp, S.; Gouya, L.; Grandchamp, B.; Beaumont, C.; Badminton, M.N.; Elder, G.H.; Holme, S.A.; Anstey, A.V.; Parker, M.; et al. C-terminal deletions in the ALAS2 gene lead to gain of function and cause X-linked dominant protoporphyria without anemia or iron overload. Am. J. Hum. Genet 2008, 83, 408–414. [Google Scholar] [CrossRef]
- Yien, Y.Y.; Ducamp, S.; van der Vorm, L.N.; Kardon, J.R.; Manceau, H.; Kannengiesser, C.; Bergonia, H.A.; Kafina, M.D.; Karim, Z.; Gouya, L.; et al. Mutation in human CLPX elevates levels of delta-aminolevulinate synthase and protoporphyrin IX to promote erythropoietic protoporphyria. Proc. Natl. Acad. Sci. USA 2017, 114, E8045–E8052. [Google Scholar] [CrossRef] [PubMed]
- Gschnait, F.; Konrad, K.; Honigsmann, H.; Denk, H.; Wolff, K. Mouse model for protoporphyria. I. The liver and hepatic protoporphyrin crystals. J. Investig. Dermatol. 1975, 65, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, J.R.; Phillips, M.J.; Davidson, D.L.; Klatskin, G.; Bloome. Hepatic disease in erythropoietic protoporphyria. Am. J. Med. 1975, 58, 869–882. [Google Scholar] [CrossRef] [PubMed]
- Casanova-Gonzalez, M.J.; Trapero-Marugan, M.; Jones, E.A.; Moreno-Otero, R. Liver disease and erythropoietic protoporphyria: A concise review. World J. Gastroenterol. 2010, 16, 4526–4531. [Google Scholar] [CrossRef] [PubMed]
- Anstey, A.V.; Hift, R.J. Liver disease in erythropoietic protoporphyria: Insights and implications for management. Gut 2007, 56, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Ardalan, Z.S.; Chandran, S.; Vasudevan, A.; Angus, P.W.; Grigg, A.; He, S.; Macdonald, G.A.; Strasser, S.I.; Tate, C.J.; Kennedy, G.A.; et al. Management of Patients With Erythropoietic Protoporphyria-Related Progressive Liver Disease. Liver Transpl. 2019, 25, 1620–1633. [Google Scholar] [CrossRef]
- Yoshida, A.; Hagiwara, S.; Watanabe, T.; Nishida, N.; Ida, H.; Sakurai, T.; Komeda, Y.; Yamao, K.; Takenaka, M.; Enoki, E.; et al. Erythropoietic Protoporphyria-related Hepatopathy Successfully Treated with Phlebotomy. Intern. Med. 2018, 57, 2505–2509. [Google Scholar] [CrossRef]
- Minder, E.I.; Schneider-Yin, X. Afamelanotide (CUV1647) in dermal phototoxicity of erythropoietic protoporphyria. Expert Rev. Clin. Pharmacol. 2015, 8, 43–53. [Google Scholar] [CrossRef]
- Minder, E.I.; Harms, J.; Lautenschlager, S.; Schneider-Yin, X.; Deybach, J.C.; Minder, C.E. A double-blind, randomized, controlled phase III trial of afamelanotide (an alpha-MSH analogue) in erythropoietic protoporphyria (EPP)-preliminary data on a Swiss cohort of patients and a model to determine efficacy in EPP. In Proceedings of the Berzelius Symposium 81-Porphyrins and Porphyrias, Stockholm, Sweden, 14–18 June 2009. [Google Scholar]
- Biolcati, G.; Marchesini, E.; Sorge, F.; Barbieri, L.; Schneider-Yin, X.; Minder, E.I. Long-term observational study of afamelanotide in 115 patients with erythropoietic protoporphyria. Br. J. Dermatol. 2015, 172, 1601–1612. [Google Scholar] [CrossRef]
- Wensink, D.; Wagenmakers, M.A.E.M.; Barman-Aksözen, J.; Friesema, E.C.H.; Wilson, J.H.P.; van Rosmalen, J.; Langendonk, J.G. Association of Afamelanotide With Improved Outcomes in Patients With Erythropoietic Protoporphyria in Clinical Practice. JAMA Dermatol. 2020, 156, 570–575. [Google Scholar] [CrossRef]
- Barman-Aksözen, J.; Nydegger, M.; Schneider-Yin, X.; Minder, A.E. Increased phototoxic burn tolerance time and quality of life in patients with erythropoietic protoporphyria treated with afamelanotide—A three years observational study. Orphanet J. Rare Dis. 2020, 15, 213. [Google Scholar] [CrossRef] [PubMed]
- Wensink, D.; Wagenmakers, M.A.; Wilson, J.P.; Langendonk, J.G. Erythropoietic protoporphyria in the Netherlands: Clinical features, psychosocial impact and the effect of afamelanotide. J. Dermatol. 2022, 50, 445–452. [Google Scholar] [CrossRef]
- Malik, I.A.; Triebel, J.; Posselt, J.; Khan, S.; Ramadori, P.; Raddatz, D.; Ramadori, G. Melanocortin receptors in rat liver cells: Change of gene expression and intracellular localization during acute-phase response. Histochem. Cell Biol. 2012, 137, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Harms, J.H.; Lautenschlager, S.; Minder, C.E.; Minder, E.I. Mitigating photosensitivity of erythropoietic protoporphyria patients by an agonistic analog of alpha-melanocyte stimulating hormone. Photochem. Photobiol. 2009, 85, 1434–1439. [Google Scholar] [CrossRef] [PubMed]
- R Foundation for Statistical Computing, R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 10 March 2023).
- EMA/265450/2019. Scenesse: EPAR-Procedural Steps Taken and Scientific Information after Authorisation 2019 [Updated 2019]. Available online: https://www.ema.europa.eu/documents/procedural-steps-after/scenesse-epar-procedural-steps-taken-scientific-information-after-authorisation_en.pdf (accessed on 30 May 2019).
- Doss, M.O.; Frank, M. Hepatobiliary implications and complications in protoporphyria, a 20-year study. Clin. Biochem. 1989, 22, 223–229. [Google Scholar] [CrossRef]
- Anstey, A.V.; Hift, R.J. Liver disease in erythropoietic protoporphyria: Insights and implications for management. Postgrad. Med. J. 2007, 83, 739–748. [Google Scholar] [CrossRef]
- Wensink, D.; Coenen, S.; Wilson, J.P.; Wagenmakers, M.A.; Langendonk, J.G. Liver involvement in patients with erythropoietic protoporphyria. Dig. Liver Dis. 2021, 54, 515–520. [Google Scholar] [CrossRef]
- Wang, W.; Guo, D.-Y.; Lin, Y.-J.; Tao, Y.-X. Melanocortin regulation of inflammation. Front. Endocrinol. 2019, 10, 683. [Google Scholar] [CrossRef]
- Vándor, E.; Simon, G.; Anda, E.; Budavári, I. The effect of alpha-melanophor-stimulating hormone on liver regeneration and incorporation of amino acid in rats’ liver protein. Endokrinologie 1975, 66, 81–87. [Google Scholar]
- Lonati, C.; Carlin, A.; Leonardi, P.; Valenza, F.; Bosari, S.; Catania, A.; Gatti, S. Modulatory effects of NDP-MSH in the regenerating liver after partial hepatectomy in rats. Peptides 2013, 50, 145–152. [Google Scholar] [CrossRef]
- Brzoska, T.; Luger, T.A.; Maaser, C.; Abels, C.; Bohm, M. Alpha-melanocyte-stimulating hormone and related tripeptides: Biochemistry, antiinflammatory and protective effects in vitro and in vivo, and future perspectives for the treatment of immune-mediated inflammatory diseases. Endocr. Rev. 2008, 29, 581–602. [Google Scholar] [CrossRef] [PubMed]
- Schallreuter, K.U.; Kothari, S.; Chavan, B.; Spencer, J.D. Regulation of melanogenesis-controversies and new concepts. Exp. Dermatol. 2008, 17, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Todd, D.J. Erythropoietic protoporphyria. Br. J. Dermatol. 1994, 131, 751–766. [Google Scholar] [CrossRef] [PubMed]
- McCullough, A.J.; Barron, D.; Mullen, K.D.; Petrelli, M.; Park, M.C.; Mukhtar, H.; Bickers, D.R. Fecal protoporphyrin excretion in erythropoietic protoporphyria: Effect of cholestyramine and bile acid feeding. Gastroenterology 1988, 94, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Tewari, A.; Marsden, J.; Naik, H.; Benton, E.C.; Sarkany, R. Oral cholestyramine is not an effective treatment for uncomplicated erythropoietic protoporphyria. J. Am. Acad. Dermatol. 2012, 67, 1383–1384. [Google Scholar] [CrossRef]
- Meerman, L.; Koopen, N.R.; Bloks, V.; van Goor, H.; Havinga, R.; Wolthers, B.G.; Kramer, W.; Stengelin, S.; Müller, M.; Kuipers, F.; et al. Biliary fibrosis associated with altered bile composition in a mouse model of erythropoietic protoporphyria. Gastroenterology 1999, 117, 696–705. [Google Scholar] [CrossRef]
- Abitbol, M.; Puy, H.; Sabate, J.M.; Guenet, J.L.; Deybach, J.C.; Montagutelli, X. Ursodesoxycholic acid and heme-arginate are unable to improve hematopoiesis and liver injury in an erythropoietic protoporphyria mouse model. Physiol Res. 2006, 55 (Suppl. S2), S93–S101. [Google Scholar] [CrossRef]
- Abitbol, M.; Bernex, F.; Puy, H.; Jouault, H.; Deybach, J.-C.; Guénet, J.-L.; Montagutelli, X. A mouse model provides evidence that genetic background modulates anemia and liver injury in erythropoietic protoporphyria. Am. J. Physiol. Gastrointest Liver Physiol. 2005, 288, G1208–G1216. [Google Scholar] [CrossRef]
- Barman-Aksozen, J.; Minder, E.I.; Schubiger, C.; Biolcati, G.; Schneider-Yin, X. In ferrochelatase-deficient protoporphyria patients, ALAS2 expression is enhanced and erythrocytic protoporphyrin concentration correlates with iron availability. Blood Cells Mol. Dis. 2015, 54, 71–77. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dependent Variable | Model p-Value | Independent Variables | |||
|---|---|---|---|---|---|
| Patient ID p-Value | Second Independent Variable | ||||
| Name | p Value | Effect | |||
| PPIX | <0.0001 | <0.0001 | indexIDR | <0.0001 | 0.008376 |
| PPIX | <0.0001 | <0.0001 | indexCDE365 | <0.0001 | −0.8043 |
| PPIX | <0.0001 | <0.0001 | Relative global radiation | 0.0113 | −1.059 |
| ALAT | 0.0008 | 0.0008 | indexIDR | 0.1625 | 0.009162 |
| ALAT | 0.0003 | 0.0005 | indexCDE365 | 0.012 | −2.509 |
| ALAT | 0.001 | 0.0008 | Relative global radiation | 0.263 | −3.6 |
| ASAT | <0.0001 | <0.0001 | indexIDR | 0.1074 | 0.004727 |
| ASAT | <0.0001 | <0.0001 | indexCDE365 | 0.1606 | −0.5345 |
| ASAT | <0.0001 | <0.0001 | Relative global radiation | 0.4277 | −1.086 |
| Bilirubin | <0.0001 | <0.0001 | indexIDR | 0.9527 | −5.90 × 10−5 |
| Bilirubin | <0.0001 | <0.0001 | indexCDE365 | 0.0299 | −0.304 |
| Bilirubin | <0.0001 | <0.0001 | Relative global radiation | 0.5845 | 0.2239 |
| GGT | <0.0001 | <0.0001 | indexIDR | 0.2044 | 0.01082 |
| GGT | <0.0001 | <0.0001 | indexCDE365 | 0.1846 | −1.668 |
| GGT | <0.0001 | <0.0001 | Relative global radiation | 0.4821 | −2.475 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minder, A.-E.; Schneider-Yin, X.; Zulewski, H.; Minder, C.E.; Minder, E.I. Afamelanotide Is Associated with Dose-Dependent Protective Effect from Liver Damage Related to Erythropoietic Protoporphyria. Life 2023, 13, 1066. https://doi.org/10.3390/life13041066
Minder A-E, Schneider-Yin X, Zulewski H, Minder CE, Minder EI. Afamelanotide Is Associated with Dose-Dependent Protective Effect from Liver Damage Related to Erythropoietic Protoporphyria. Life. 2023; 13(4):1066. https://doi.org/10.3390/life13041066
Chicago/Turabian StyleMinder, Anna-Elisabeth, Xiaoye Schneider-Yin, Henryk Zulewski, Christoph E. Minder, and Elisabeth I. Minder. 2023. "Afamelanotide Is Associated with Dose-Dependent Protective Effect from Liver Damage Related to Erythropoietic Protoporphyria" Life 13, no. 4: 1066. https://doi.org/10.3390/life13041066