
Pramipexole Augmentation for Treatment-Resistant Unipolar and Bipolar Depression in the Real World: A Systematic Review and Meta-Analysis
 , , ,
, , ,
Abstract
:1. Introduction
Aims of the Study
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Population
2.4. Outcome Measures
2.5. Safety Measures
2.6. Data Extraction
2.7. Statistical Analysis
3. Results
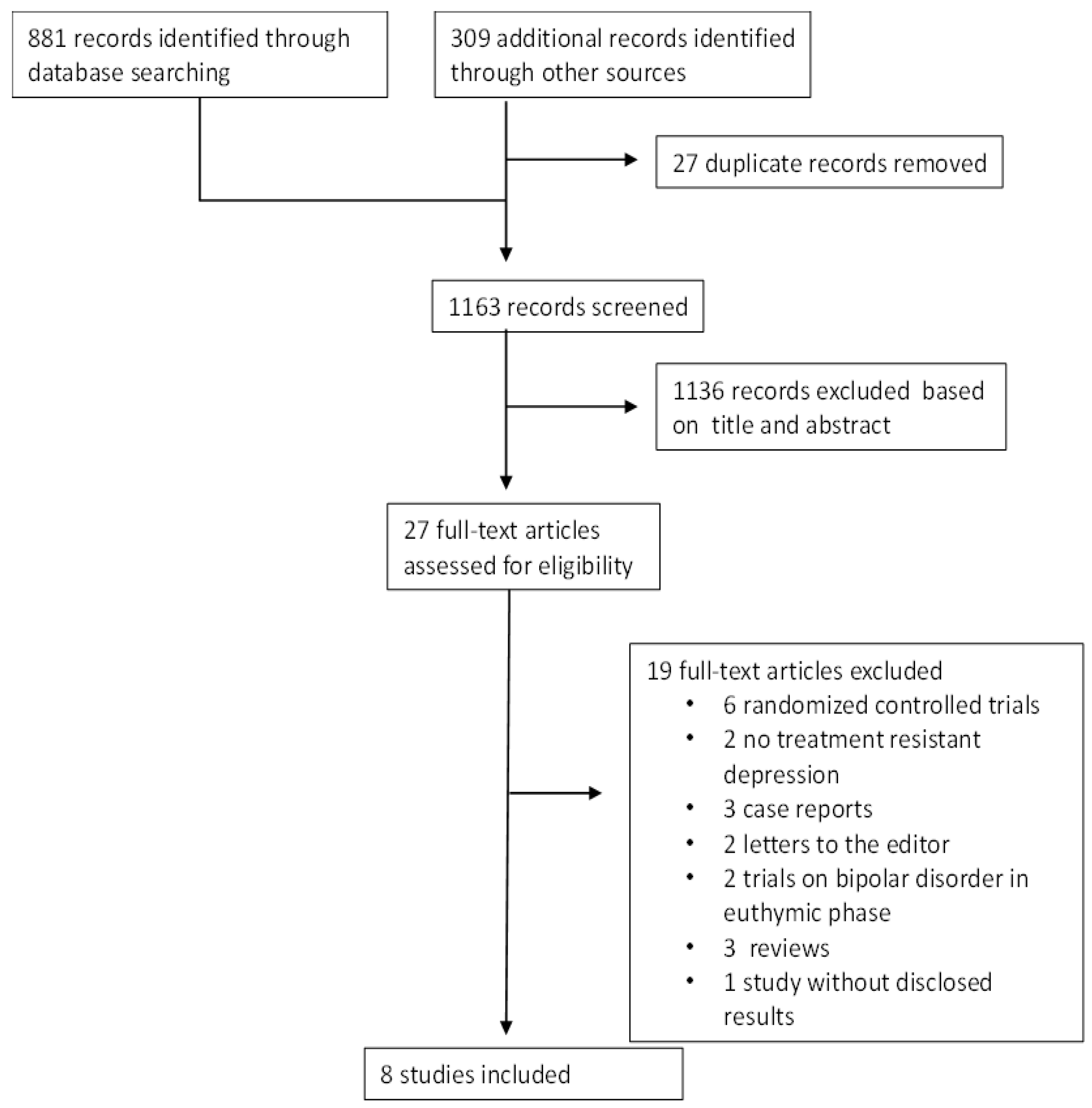
3.1. Selected Studies
3.2. Study Characteristics
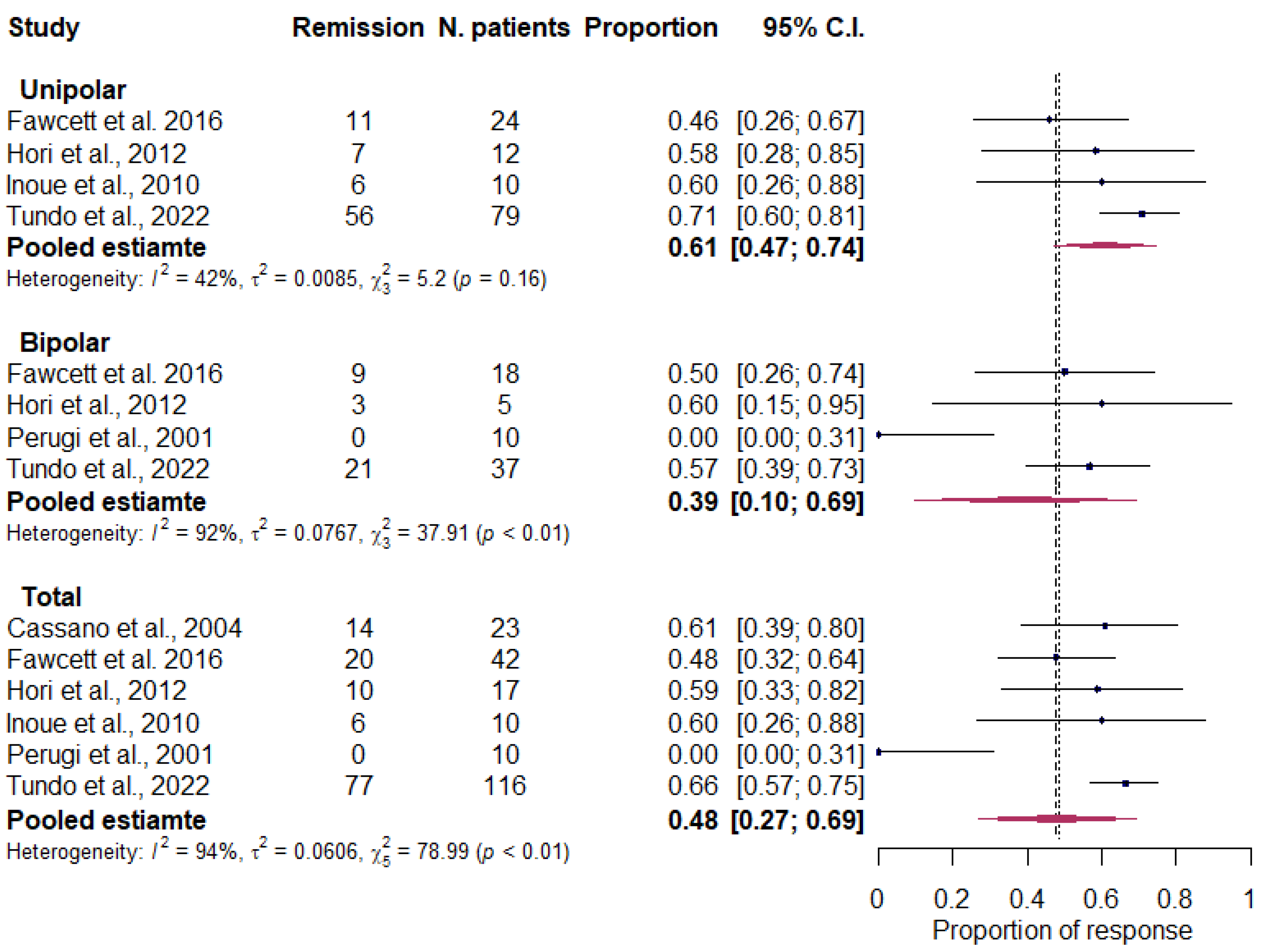
3.3. Outcome Measures
- Treatment response
- b.
- Treatment remission
3.4. Safety Measure
- Drop-outs due to any adverse event
- b.
- Drop-outs due to any reason
- c.
- (Hypo)mania onset
- d.
- Suicide attempt
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factor, 2001, systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Bell, E.; Bassett, D.; Boyce, P.; Bryant, R.; Hazell, P.; Hopwood, M.; Lyndon, B.; Mulder, R.; Porter, R.; et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust. N. Z. J. Psychiatry 2021, 55, 7–117. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Depression and Other Common Mental Disorder: Global Health Estimates; License: CCBY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2017; p. 24. [Google Scholar]
- GBD. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [PubMed]
- Yatham, L.N.; Kennedy, S.H.; Parikh, S.V.; Schaffer, A.; Bond, D.J.; Frey, B.N.; Sharma, V.; Goldstein, B.I.; Rej, S.; Beaulieu, S.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder: Update 2013. Bipolar Disord. 2018, 20, 97–170. [Google Scholar] [CrossRef] [PubMed]
- Judd, L.L.; Akiskal, H.S.; Schettler, P.J.; Endicott, J.; Maser, J.; Solomon, D.A.; Leon, A.C.; Rice, J.A.; Keller, M.B. The Long-term Natural History of the Weekly Symptomatic Status of Bipolar I Disorder. Arch. Gen. Psychiatry 2002, 59, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Judd, L.L.; Akiskal, H.S.; Schettler, P.J.; Coryell, W.; Endicott, J.; Maser, J.D.; Solomon, D.A.; Leon, A.C.; Keller, M.B. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch. Gen. Psychiatry 2003, 60, 261–269. [Google Scholar] [CrossRef]
- Cleare, A.; Pariante, C.; Young, A.; Anderson, I.; Christmas, D.; Cowen, P.; Dickens, C.; Ferrier, I.; Geddes, J.; Gilbody, S.; et al. Evidence-based guidelines for treating depressive disorders with antidepressants: A revision of the 2008 British Association for Psychopharmacology guidelines. J. Psychopharmacol. 2015, 29, 459–525. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Depression in Adults: Treatment and Management, NICE Guideline; National Institute for Health and Care Excellence: London, UK, 2022. [Google Scholar]
- Pacchiarotti, I.; Bond, D.J.; Baldessarini, R.J.; Nolen, W.A.; Grunze, H.; Licht, R.W.; Post, R.M.; Berk, M.; Goodwin, G.M.; Sachs, G.S.; et al. The International Society for Bipolar Disorders (ISBD) task force report on antidepressant use in bi-polar disorders. Am. J. Psychiatry 2013, 170, 1249–1262. [Google Scholar] [CrossRef]
- Tundo, A.; Calabrese, J.R.; Proietti, L.; de Filippis, R. Short-term antidepressant treatment of bipolar depression: Are ISBD recommendations useful in clinical practice? J. Affect. Disord. 2015, 171, 155–160. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Rush, A.; Wisniewski, S.; Nierenberg, A.A.; Warden, D.; Ritz, L.; Norquist, G.; Howland, R.H.; Lebowitz, B.; McGrath, P.; et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: Implications for clinical practice. Am. J. Psychiatry 2006, 163, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcome in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef]
- Bowden, C.; Perlis, R.; Thase, M.; Ketter, T.; Ostacher, M.; Calabrese, J.; Reilly-Harrington, N.; Gonzalez, J.; Singh, V.; Nierenberg, A.; et al. Aims and results of the NIMH systematic treatment enhancement program for bipolar disorder (STEP-BD). CNS Neurosci. Ther. 2012, 18, 243–249. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA). Guideline on Clinical Investigation of Medicinal Products in the Treatment of Depression; EMA/CHMP/185423/2010 Rev 2; European Medicines Agency: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Nuñez, N.A.; Joseph, B.; Pahwa, M.; Kumar, R.; Resendez, M.G.; Prokop, L.J.; Veldic, M.; Seshadri, A.; Biernacka, J.M.; Frye, M.A.; et al. Augmentation strategies for treatment resistant major depression: A systematic review and network meta-analysis. J. Affect. Disord. 2022, 302, 385–400. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, G. Treatment resistant depression: What are the options? BMJ 2018, 363, 102018. [Google Scholar] [CrossRef] [PubMed]
- Yadid, G.; Friedman, A. Dynamics of the dopaminergic system as a key component to the understanding of depression. Prog. Brain Res. 2008, 172, 265–286. [Google Scholar]
- Papakostas, G.I.; Petersen, T.; Pava, J.; Masson, E.; Worthington, J.J.; Alpert, J.; Fava, M.; Nierenberg, A.A. Hopelessness and suicidal ideation in outpatients with treatment-resistant depression: Prevalence and impact on treatment outcome. J. Nerv. Ment. Dis. 2003, 191, 444–449. [Google Scholar] [CrossRef]
- Schlaepfer, T.; Ågren, H.; Monteleone, P.; Gasto, C.; Pitchot, W.; Rouillon, F.; Nutt, D.; Kasper, S. The hidden third: Improving outcome in treatment-resistant depression. J. Psychopharmacol. 2012, 26, 587–602. [Google Scholar] [CrossRef]
- Olfson, M.; Amos, T.B.; Benson, C.; McRae, J.; Marcus, S.C. Prospective service use and health care costs of Medicaid beneficiaries with treatment-resistant depression. J. Manag. Care Spec. Pharm. 2018, 24, 226–236. [Google Scholar] [CrossRef]
- Sachs, G.S. Treatment-resistant bipolar depression. Psychiatr. Clin. N. Am. 1996, 19, 215–236. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Yatham, L.N.; Grunze, H.; Vieta, E.; Young, A.H.; Blier, P.; Tohen, M.; Kasper, S.; Moeller, H.J. The CINP guideline on the definition and evidence-based inter-vention for treatment-resistant bipolar disorder. Int. J. Neuropsychopharmacol. 2020, 23, 230–256. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, M.J. Antidepressants in bipolar depression: An enduring controversy. Int. J. Bipolar. Disord. 2018, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Lyall, L.M.; Penades, N.; Smith, D.J. Changes in prescribing for bipolar disorder between 2009 and 2016: Nation-al-level data linkage study in Scotland. Br. J. Psychiatry 2019, 215, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Rhee, T.G.; Olfson, M.; Nierenberg, A.A.; Wilkinson, A.T. 20-year trends in the pharmacologic treatment of bipolar disorder by psychiatrists in outpatient care settings. Am. J. Psychiatry 2020, 177, 706–715. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Grunze, H.; Vieta, E.; Young, A.; Yatham, L.; Blier, P.; Kasper, S.; Moeller, H.J. The international college of neuro-psychopharmacology (CINP) treatment guidelines for bipolar disorders in adults (CINP-BD-2017), part 3: The clinical guidelines. Int. J. Neu-Ropsychophermacol. 2017, 20, 180–195. [Google Scholar] [CrossRef]
- Voineskos, D.; Daskalakis, Z.J.; Blumberg, D.M. Management of treatment-resistant depression: Challenges and strategies. Neuropsychiatr. Dis. Treat. 2020, 16, 221–234. [Google Scholar] [CrossRef]
- Ruberto, V.L.; Jha, M.K.; Murrough, J.W. Pharmacological treatments for patients with treatment-resistant depression. Phar-maceutical 2020, 13, 116. [Google Scholar] [CrossRef]
- Cowen, P.J. Backing into the future: Pharmacological approaches to the management of resistant depression. Psychol. Med. 2017, 47, 2569–2577. [Google Scholar] [CrossRef]
- Dold, M.; Kasper, S. Evidence-based pharmacotherapy of treatment-resistant unipolar depression. Int. J. Psychiatry Clin. Pract. 2017, 21, 13–23. [Google Scholar] [CrossRef]
- Tundo, A.; De Filippis, R.; Proietti, L. Pharmacologic approaches to treatment resistant depression: Evidences and personal experience. World J. Psychiatry 2015, 5, 330–341. [Google Scholar] [CrossRef]
- Mahase, E. Esketamine is approved in Europe for treating resistant major depressive disorder. BMJ 2019, 367, l7069. [Google Scholar] [CrossRef]
- Bahji, A.; Zarate, C.A.; Vazquez, G.H. Efficacy and safety of racemic ketamine and esketamine for depression: A systematic review and meta-analysis. Expert Opin. Drugs Saf. 2022, 21, 853–866. [Google Scholar] [CrossRef] [PubMed]
- Diaz, A.P.; Fernandes, B.S.; Quevedo, J.; Sanches, M.; Soares, J.C. Treatment-resistant bipolar depression: Concept and challenges for novel interventions. Braz. J. Psychiatry 2022, 44, 178–186. [Google Scholar] [CrossRef]
- Belmaker, R.H.; Wald, D. Haloperidol in normal. Br. J. Psychiatry 1997, 131, 222–223. [Google Scholar] [CrossRef]
- Silvestrone, T. Dopamine in manic depressive illness. A pharmacological synthesis. J. Affect. Disord. 1985, 8, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.J.; Ogilvie, A.D.; Goodwin, G.M.; Ebmeier, K.P. Clinical and psychometric correlates of dopamine D2 binding in depres-sion. Psychol Med. 1997, 27, 1247–1256. [Google Scholar] [CrossRef]
- Ashok, A.H.; Marques, T.R.; Jauhar, S.; Nour, M.M.; Goodwin, G.M.; Young, A.H.; Howes, O.D. The dopamine hypothesis of bipolar affective disorder: The state of the art and implications for treatment. Mol. Psychiatry 2017, 22, 666–679. [Google Scholar] [CrossRef]
- Zhao, F.; Cheng, Z.; Piao, J.; Cui, R.; Li, B. Dopamine Receptors: Is It Possible to Become a Therapeutic Target for Depression? Front. Pharmacol. 2022, 13, 947785. [Google Scholar] [CrossRef]
- Lammers, C.H.; Diaz, J.; Schwartz, J.C.; Sokoloff, P. Selective increase of dopamine D3 receptor gene as a common effect of chronic antidepressant treat-ment. Mol. Psychiatry 2020, 5, 736–767. [Google Scholar]
- Dunlop, B.W.; Nemeroff, C.B. The role of dopamine in the pathophysiology of depression. Arch. Gen. Psychiatry 2007, 64, 327–337. [Google Scholar] [CrossRef]
- Muscat, R.; Papp, M.; Willner, P. Antidepressant-like model effects of dopamine agonists in an animal model of depression. Biol. Psychiatry 1992, 31, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Willner, P.; Lapas, S.; Cheeta, S.; Muscat, R. Reversal of stress-induced anhedonia by the dopamine receptor agonist, pramipexole. Psychopharmachology 1994, 115, 454–462. [Google Scholar] [CrossRef]
- Maj, J.; Rogoz, Z.; Skuza, G.; Kolodziejczyk, K. Antidepressant effect of pramipexole, a novel dopamine receptor agonist. J Neural Transm 1997, 104, 525–533. [Google Scholar] [CrossRef]
- Chiba, S.; Numakawa, T.; Ninomiya, M.; Yoon, H.S.; Kunugi, H. Carbegoline, a dopamine receptor agonist, has an antidepres-sant-like property and enhances brain-derived neurotrophic factor signaling. Psychopharmacology 2010, 211, 291–301. [Google Scholar] [CrossRef]
- Sarchiapone, M.; Carli, V.; Camardese, G.; Cuomo, C.; Di Giuda, D.; Calcagni, M.-L.; Focacci, C.; De Risio, S. Dopamine transporter binding in depressed patients with anhedonia. Psychiatry Res. 2006, 147, 243–248. [Google Scholar] [CrossRef]
- Hori, H.; Kunugi, H. The efficacy of pramipexole, a dopamine receptor agonist, as an adjunctive treatment in treat-ment-resistant depression: An open-label trial. Sci. World J. 2012, 2012, 372474. [Google Scholar] [CrossRef]
- Antonini, A.; Barone, P.; Ceravolo, R.; Fabbrini, G.; Tinazzi, M. Role of pramipexole in the management of Parkinson’s disease. CNS Drugs 2010, 24, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Aurora, R.N.; Kristo, D.A.; Bista, S.R.; Rowley, J.A.; Zak, R.S.; Casey, K.R.; Lamm, C.I.; Tracy, S.L.; Rosenberg, R.S. The treatment of restless legs syndrome and periodic limb movement disorder in adult- an update for 2012: Practice parameters with an evidence-based systematic review and meta-analyses: An American Academy of sleep medicine clinical practice guideline. Sleep 2012, 35, 1039–1062. [Google Scholar] [CrossRef] [PubMed]
- Piercey, M. Pharmacology of pramipexole, a dopamine D3-preferring agonist in treating Parkinson’s Disease. Clin. Nueropharmachol. 1998, 21, 141–151. [Google Scholar]
- Motyl, J.; Przykaza, Ł.; Boguszewski, P.M.; Kosson, P.; Strosznajder, J.B. Pramipexole and Fingolimod exert neuroprotection in a mouse model of Parkinson’s disease by activation of sphingosine kinase 1 and Akt kinase. Neuropharmacology 2018, 135, 139–150. [Google Scholar] [CrossRef]
- Escalona, R.; Fawcett, J. Pramipexole in Treatment Resistant-Depression, Possible Role of Inflammatory Cytokines. Neuropsychopharmacology 2017, 42, 363. [Google Scholar] [CrossRef] [PubMed]
- Castro-Hernandez, J.; Adlard, P.A.; Finkelstein, D.I. Pramipexole restores depressed transmission in the ventral hippocampus following MPTP-lesion. Sci. Rep. 2017, 14, 44426. [Google Scholar] [CrossRef] [PubMed]
- Martens, M.A.G.; Kaltenboeck, A.; Halahakoon, D.C.; Browning, M.; Cowen, P.J.; Harmer, C.J. An experimental medicine investigation on the effects of subacute pramipexole treatment on emotional information processing in healthy volunteers. Pharmaceuticals 2021, 14, 800. [Google Scholar] [CrossRef]
- Jiang, D.Q.; Jiang, L.L.; Wang, Y.; Li, M.X. The role of pramipexole in the treatment of patients with depression and Parkinson’s disease: A meta-analysis of randomized controlled trials. Asian J. Psychiatry 2021, 61, 102691. [Google Scholar] [CrossRef] [PubMed]
- Tundo, A.; de Filippis, R.; De Crescenzo, F. Pramipexole in the treatment of unipolar and bipolar depression. Acta Psychiatr. Scand. 2019, 140, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; US Department of Health, Education, and Welfare Publication (ADM) 76-338; National Institute of Mental Health: Rockville, MD, USA, 1976; pp. 218–222. [Google Scholar]
- Huwaldt, J.A. Plot Digitzer (Version 2.6.8). 2001. Available online: http://plotdigitizer.sourceforge.net (accessed on 31 December 2022).
- Corrigan, M.H.; Denahan, A.Q.; Wright, C.E.; Ragual, R.J.; Evans, D.L. Comparison of pramipexole, fluoxetine, and placebo in patients with major depression. Depress Anxiety 2000, 11, 58–65. [Google Scholar] [CrossRef]
- Zarate, C.A., Jr.; Payne, J.L.; Singh, J.; Quiroz, J.A.; Luckenbaugh, D.A.; Denicoff, K.D.; Charney, D.S.; Manji, H.K. Pramipexole for bipolar II depression: A placebo-controlled proof of concept study. Biol. Psychiatry 2004, 56, 54–60. [Google Scholar] [CrossRef]
- Mah, L.; Zarate Jr, C.A.; Nugent, A.C.; Singh, J.B.; Manji, H.K.; Drevets, W.C. Neural mechanisms of antidepressant efficacy of the dopamine receptor agonist pramipexole in treatment of bipolar depression. Int. J. Neuropsychopharmacol. 2011, 14, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Cusin, C.; Iovieno, N.; Iosifescu, D.V.; Nierenberg, A.A.; Fava, M.; Rush, A.J.; Perlis, R.H. A randomized, double-blind, placebo-controlled trial of pramipexole augmentation in treatment-resistant major depressive disorder. J. Clin. Psychiatry. 2013, 74, e636–e641. [Google Scholar] [CrossRef] [PubMed]
- Franco-Chaves, J.A.; Mateus, C.F.; Luckenbaugh, D.A.; Martinez, P.E.; Mallinger, A.G.; Zarate, C.A., Jr. Combining a dopamine agonist and selective serotonin reuptake inhibitor for the treatment of depression: A double-blind, randomized pilot study. J. Affect. Disord. 2013, 149, 319–325. [Google Scholar] [CrossRef]
- Goldberg, J.F.; Burdick, K.E.; Endick, C.J. Preliminary randomized, double-blind, placebo-controlled trial of pramipexole added to mood stabilizers for treatment-resistant bipolar depression. Am. J. Psychiatry 2004, 161, 564–566. [Google Scholar] [CrossRef] [PubMed]
- El-Mallakh, R.S.; Penagaluri, P.; Kantamneni, A.; Gao, Y.; Roberts, R.J. Long-term use of pramipexole in bipolar depression: A naturalistic retrospective chart review. Psychiatr. Q. 2010, 81, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Ventorp, F.; Lindahl, J.; van Westen, D.; Jensen, J.; Björkstrand, J.; Lindqvist, D. Preliminary evidence of efficacy and target engagement of pramipexole in anhedonic depression. Psych. Res. Clin. Pract. 2022, 4, 42–47. [Google Scholar] [CrossRef]
- Akdeniz, F.; Aldemir, E.; Vahip, S. The role of low-dose pramipexole in the treatment of treatment-resistant bipolar depression: A case report. Turk. J. Psychiatry 2009, 20, 94–98. [Google Scholar]
- Gupta, S.; Vincent, J.L.; Frank, B. Pramipexole: Augmentation in the treatment of depressive symptoms. CNS Spectr. 2006, 11, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Hori, T.; Tsutsumi, K.; Asada, T. Pramipexole-induced peripheral edema in a patient with Bipolar Depression. J. Neuropsychiatry Clin. Neurosci. 2011, 23, E20. [Google Scholar] [CrossRef]
- Ostow, M. Pramipexole for depression. Am. J. Psychiatry. 2002, 159, 320–321. [Google Scholar] [CrossRef]
- Burdick, K.E.; Braga, R.J.; Nnadi, C.U.; Shaya, Y.; Stearns, W.H.; Malhotra, A.K. Placebo-controlled adjunctive trial of pramipexole in patients with bipolar disorder: Targeting cognitive dysfunction. J. Clin. Psychiatry. 2012, 73, 103–112. [Google Scholar] [CrossRef] [PubMed]
- NCT02397837. Targeting Cognition in Bipolar Disorder with Pramipexole (PRAM-BD). Available online: https://clinicaltrials.gov/ct2/show/NCT02397837 (accessed on 7 August 2018).
- Dell’Osso, B.; Ketter, T.A. Assessing efficacy/effectiveness and safety/tolerability profiles of adjunctive pramipexole in bipolar depression: Acute versus long-term data. Int. Clin. Psychopharmacol. 2013, 28, 297–304. [Google Scholar] [CrossRef]
- NCT00893841. Bipolar Study of Seroquel XR with Pramipexole Dihydrochloride. Available online: https://clinicaltrials.gov/ct2/show/NCT00893841 (accessed on 7 August 2018).
- Cassano, P.; Lattanzi, L.; Soldani, F.; Navari, S.; Battistini, G.; Gemignani, A.; Cassano, G.B. Pramipexole in treatment-resistant depression: An extended follow-up. Depress. Anxiety 2004, 20, 131–138. [Google Scholar] [CrossRef]
- Inoue, T.; Kitaichi, Y.; Masui, T.; Nakagawa, S.; Boku, S.; Tanaka, T.; Suzuki, K.; Nakato, Y.; Usui, R.; Koyama, T. Pramipexole for stage 2 treatment-resistant major depression: An open study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 1446–1449. [Google Scholar] [CrossRef]
- Lattanzi, L.; Dell'Osso, L.; Cassano, P.; Pini, S.; Rucci, P.; Houck, P.R.; Gemignani, A.; Battistini, G.; Bassi, A.; Abelli, M.; et al. Pramipexole in treatment-resistant depression: A 16-week naturalistic study. Bipolar. Disord. 2002, 4, 307–314. [Google Scholar] [CrossRef]
- Perugi, G.; Toni, C.; Ruffolo, G.; Frare, F.; Akiskal, H. Adjunctive dopamine agonists in treatment-resistant bipolar II depression: An open case series. Pharmacopsychiatry 2001, 34, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Sporn, J.; Ghaemi, S.N.; Sambur, M.; Rankin, M.; Recht, J.; Sachs, G.; Rosenbaum, J.; Fava, M. Pramipexole augmentation in the treatment of unipolar and bipolar depression: A retrospective chart review. Ann. Clin. Psychiatry 2000, 12, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, J.; Rush, A.J.; Vukelich, J.; Diaz, S.H.; Dunklee, L.; Romo, P.; Yarns, B.C.; Escalona, R. Clinical Experience with High-Dosage Pramipexole in Patients With Treatment-Resistant Depressive Epi-sodes in Unipolar and Bipolar Depression. Am. J. Psychiatry 2016, 173, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Tundo, A.; Betro’, S.; Iommi, M.; de Filippis, R. Efficacy and safety of 24-week pramipexole augmentation in patients with treatment resistant depression. A retrospective cohort study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2022, 112, 110425. [Google Scholar] [CrossRef]
- Corrigan-Curay, J.; Sacks, L.; Woodcock, J. Real-world evidence and real-world data for evaluating drug safety and effec-tiveness. JAMA 2018, 320, 867–868. [Google Scholar] [CrossRef]
- Caldiroli, A.; Capuzzi, E.; Tagliabue, I.; Capellazzi, M.; Marcatili, M.; Mucci, F.; Colmegna, F.; Clerici, M.; Buoli, M.; Dakanalis, A. Augmentative pharmacological strategies in treatment-resistant major depression: A comprehensive review. Int. J. Mol. Sci. 2021, 22, 1370. [Google Scholar] [CrossRef]
- Zhou, X.; Ravindran, A.V.; Qin, B.; Del Giovane, C.; Li, Q.; Bauer, M.; Liu, Y.; Fang, Y.; da Silva, T.; Zhang, Y.; et al. Comparative efficacy, acceptability, and tolerability of augmentation agents in treatment-resistant depression: Systematic review and network meta-analysis. J. Clin. Psychiatry 2015, 76, e487–e498. [Google Scholar] [CrossRef]
- Carter, B.; Strawbridge, R.; Husain, M.I.; Jones, B.D.M.; Short, R.; Cleare, A.J.; Tsapekos, D.; Patrick, F.; Marwood, L.; Taylor, R.W.; et al. Relative effectiveness of augmentation treatments for treatment-resistant depression: A systematic review and network meta-analysis. Int. Rev. Psychiatry 2020, 32, 477–490. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: A systematic review and network-analysis. Lancet 2018, 391, 1357–1366. [Google Scholar] [CrossRef]
- Aizenstein, H.J.; Baskys, A.; Boldrini, M.; Butters, M.A.; Diniz, B.S.; Jaiswal, M.K.; Jellinger, K.A.; Kruglov, L.S.; Meshandin, I.A.; Mijajlovic, M.D.; et al. Vascular depression consensus report—A critical update. BMC Med. 2016, 14, 161. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, K.A. Pathomechanisms of vascular depression in older adult. Int. J. Mol. Sci. 2022, 23, 12496. [Google Scholar] [CrossRef]
- Cooper, C.; Katona, C.; Lyketsos, K.; Blazer, D.; Brodaty, H.; Rabins, P.; Lima, C.A.D.M.; Livingston, G. A systematic review of treatments for refractory depression in older people. Am. J. Psychiatry. 2011, 168, 681–688. [Google Scholar] [CrossRef]
- Lenze, E.J.; Mulsant, B.H.; Blumberger, D.M.; Karp, J.F.; Newcomer, J.W.; Anderson, S.; Dew, M.A.; A Butters, M.; A Stack, J.; E Begley, A.; et al. Efficacy, safety, and tolerability of augmentation pharmacotherapy with aripiprazole for treatment-resistant depression in late life: A randomised, double-blind, placebo-controlled trial. Lancet 2015, 386, 2404–2412. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.; Ye, R.; Zhang, B. Efficacy and safety of pramipexole extended-release in Parkinson’s disease: A review based on meta-analysis of randomized controlled trials. Eur. J. Neurol. 2017, 24, 835–843. [Google Scholar] [CrossRef]
- Aiken, C.B. Pramipexole in psychiatry: A systematic review of the literature. J. Clin. Psychiatry 2007, 68, 1230–1236. [Google Scholar] [CrossRef]
- Czernecki, V.; Pillon, B.; Houeto, J.L.; Pochon, J.B.; Levy, R.; Dubois, B. Motivation, reward and Parkinson’s disease: Influence of dopatherapy. Neuropsychologia 2002, 40, 2257–2267. [Google Scholar] [CrossRef] [PubMed]
- Berman, R.; E Thase, M.; Trivedi, M.H.; A Hazel, J.; Marler, S.V.; McQuade, R.D.; Carson, W.; A Baker, R.; Marcus, R.N. Long term safety and tolerability of open-label aripiprazole augmentation of antidepressant therapy in major depressive disorder. Neuropsychiatr. Dis. Treat. 2011, 7, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.; Frey, M.; Dunn, R. Pramipexole in refractory bipolar depression. Am. J. Psychiatry 1999, 156, 798. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Design | Participants (n) | Females | Age Mean, Years (SD) | Age at Onset Mean, Years (SD) | Diagnoses | Pramipexole Mean Maximum Dose | Trial Duration (Weeks) | Outcome Measure | Response Criteria | Remission Criteria |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cassano et al., 2004 [80] | Prospective | 23 | 69.5% | 52.8 (12.5) | 35.1 (16) | 11 MDD; 12 BD | 0.99 | 48 | LIFE | Not reported | Depression score ≤ 2 |
| Hori et al., 2012 [49] | Open-label trial | 17 | 58.8% | 36.2 (9.2) | 28.1 (7.6) | 12 MDD; 5 BD | 1.6 | 12 | HDRS | >50% total score reduction | Total score ≤ 7 |
| Inoue et al., 2010 [81] | Open-label trial | 10 | 40% | 43.7 (11.4) | 39.6 (11.5) | 10 MDD | 1.3 | 8 | MADRS | >50% total score reduction | Total score < 10 |
| Lattanzi et al., 2002 [82] | Prospective | 31 | 67.7% | 53.7 (13.5) | 32 (15.3) | 14 MDD; 17 BD | 0.95 | 16 | MADRS | >50% total score reduction | Not reported |
| Perugi et al., 2001 [83] | Retrospective | 10 | 60% | 55 (15.9) | 34.2 (14.8) | 10 BD | 1.23 | 17.6 | CGI | Improvement score = 2 | Improvement score = 1 |
| Sporn et al., 2000 [84] | Retrospective | 32 | 53.1% | 41.5 (14) | 22.3 (10.8) | 20 MDD; 12 BD | 0.69 | 24.4 | CGI | Improvement score ≤ 2 | Not reported |
| Fawcett et al., 2016 [85] | Case series | 42 | 50% | 53.97 (13) | NR | 24 MDD; 18 BD | 2.18 | 69 | Clinical | Clinical assessment | Clinical assessment |
| Tundo et al., 2022 [86] | Prospective | 116 | 56% | 62.2 (13.3) | 44.4 (17.9) | 79 MDD; 37 BD | 1.03 | 24 | HDRS | >50% total score reduction | Total score < 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tundo, A.; Betro’, S.; de Filippis, R.; Marchetti, F.; Nacca, D.; Necci, R.; Iommi, M. Pramipexole Augmentation for Treatment-Resistant Unipolar and Bipolar Depression in the Real World: A Systematic Review and Meta-Analysis. Life 2023, 13, 1043. https://doi.org/10.3390/life13041043
Tundo A, Betro’ S, de Filippis R, Marchetti F, Nacca D, Necci R, Iommi M. Pramipexole Augmentation for Treatment-Resistant Unipolar and Bipolar Depression in the Real World: A Systematic Review and Meta-Analysis. Life. 2023; 13(4):1043. https://doi.org/10.3390/life13041043
Chicago/Turabian StyleTundo, Antonio, Sophia Betro’, Rocco de Filippis, Fulvia Marchetti, Daniele Nacca, Roberta Necci, and Marica Iommi. 2023. "Pramipexole Augmentation for Treatment-Resistant Unipolar and Bipolar Depression in the Real World: A Systematic Review and Meta-Analysis" Life 13, no. 4: 1043. https://doi.org/10.3390/life13041043