
Bladder Neck Obstruction: Experience and Management in a Sperm Bank

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Semen Analysis
2.3. Statistical Analysis
3. Results
3.1. Semen Quality before Surgery
3.2. Semen Quality after Surgery
3.3. Ejaculatory Function
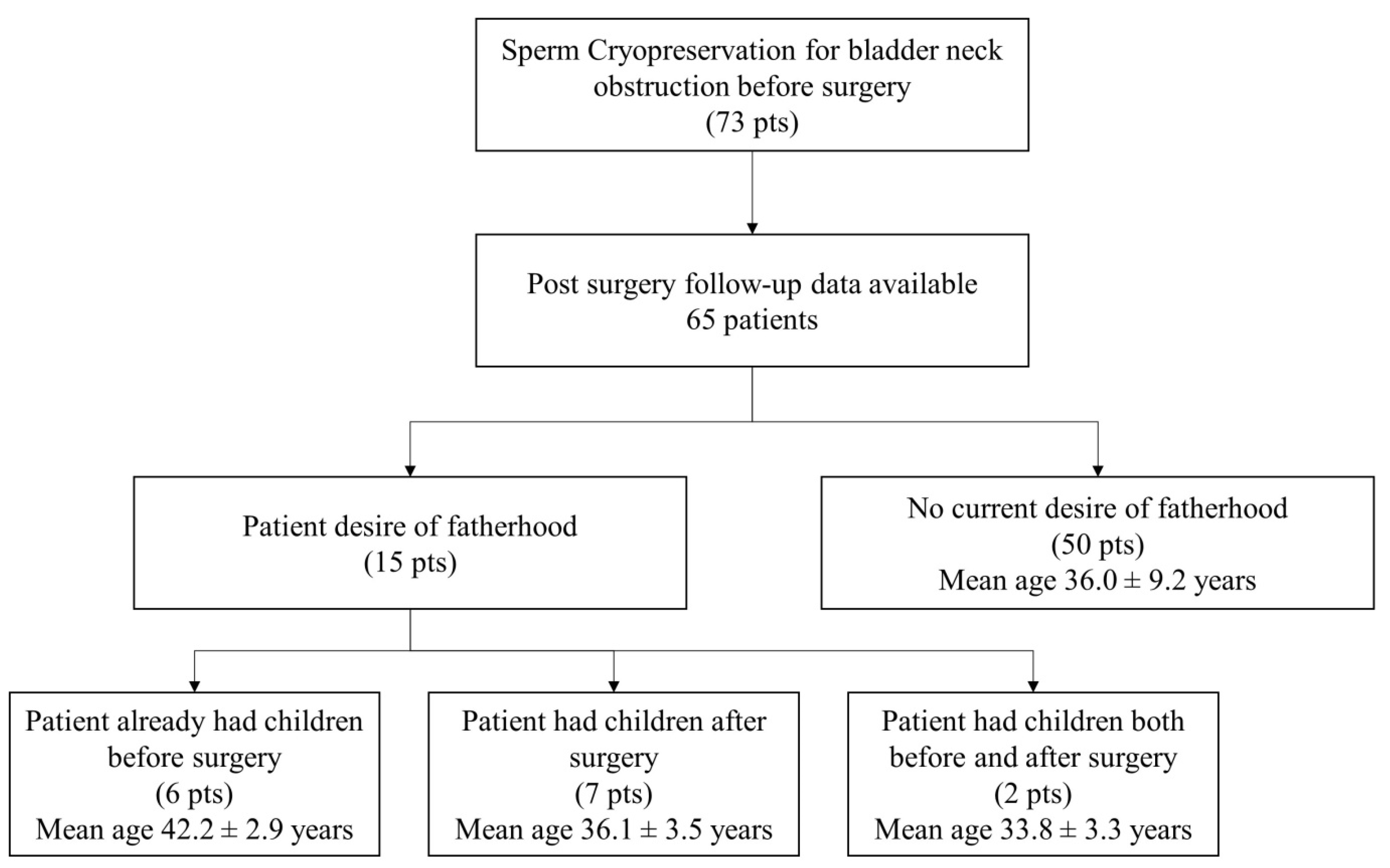
3.4. Fertility
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nitti, V.W. Primary bladder neck obstruction in men and women. Rev. Urol. 2005, 7 (Suppl. 8), S12–S17. [Google Scholar] [PubMed]
- Kaplan, S.A.; Ikeguchi, E.F.; Santarosa, R.P.; D’Alisera, P.M.; Hendricks, J.; Te, A.E.; Miller, M.I. Etiology of voiding dysfunction in men less than 50 years of age. Urology 1996, 47, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Nitti, V.W.; Lefkowitz, G.; Ficazzola, M.; Dixon, C.M. Lower urinary tract symptoms in young men: Videourodynamic findings and correlation with noninvasive measures. J. Urol. 2002, 168, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Kochakarn, W.; Lertsithichai, P. Unilateral transurethral incision for primary bladder neck obstruction: Symptom relief and fertility preservation. World J. Urol. 2003, 21, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S.A.; Te, A.E.; Jacobs, B.Z. Urodynamic evidence of vesical neck obstruction in men with misdiagnosed chronic nonbacterial prostatitis and the therapeutic role of endoscopic incision of the bladder neck. J. Urol. 1994, 152, 2063–2065. [Google Scholar] [CrossRef]
- Webster, G.D.; Lockhart, J.L.; Older, R.A. The evaluation of bladder neck dysfunction. J. Urol. 1980, 123, 196–198. [Google Scholar] [CrossRef]
- Trockman, B.A.; Gerspach, J.; Dmochowski, R.; Haab, F.; Zimmern, P.E.; Leach, G.E. Primary bladder neck obstruction: Urodynamic findings and treatment results in 36 men. J. Urol. 1996, 156, 1418–1420. [Google Scholar] [CrossRef]
- Neykov, K.G.; Panchev, P.; Georgiev, M. Late results after transurethral bladder neck incision. Eur. Urol. 1998, 33, 73–78. [Google Scholar] [CrossRef]
- Norlen, L.J.; Blaivas, J.G. Unsuspected proximal urethral obstruction in young and middle-aged men. J. Urol. 1986, 135, 972–976. [Google Scholar] [CrossRef]
- el-Baz, M.A.; Yousef, A.A.; Moustafa, H. Transurethral incision of the bladder neck: An objective and subjective evaluation of its efficacy. Int. Urol. Nephrol. 1995, 27, 717–721. [Google Scholar] [CrossRef]
- Hedlund, H.; Ek, A. Ejaculation and sexual function after endoscopic bladder neck incision. Br. J. Urol. 1985, 57, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.T.; Nordling, J.; Meyhoff, H.H.; Jacobsen, O.; Hald, T. Functional bladder neck obstruction. Late results after endoscopic bladder neck incision. Scand. J. Urol. Nephrol. 1980, 14, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Delaere, K.P.; Debruyne, F.M.; Moonen, W.A. Extended bladder neck incision for outflow obstruction in male patients. Br. J. Urol. 1983, 55, 225–228. [Google Scholar] [CrossRef]
- Christensen, M.G.; Nordling, J.; Andersen, J.T.; Hald, T. Functional bladder neck obstruction. Results of endoscopic bladder neck incision in 131 consecutive patients. Br. J. Urol. 1985, 57, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Moisey, C.U.; Stephenson, T.P.; Evans, C.A. A subjective and urodynamic assessment of unilateral bladder neck incision for bladder neck obstruction. Br. J. Urol. 1982, 54, 114–117. [Google Scholar] [CrossRef]
- Mobb, G.E.; Moisey, C.U. Long-term follow-up of unilateral bladder neck incision. Br. J. Urol. 1988, 62, 160–162. [Google Scholar] [CrossRef]
- Ferlin, A.; Calogero, A.E.; Krausz, C.M.; Lombardo, F.; Paoli, D.; Rago, R.; Scarica, C.; Simoni, M.; Foresta, C.; Rochira, V.; et al. Management of male factor infertility: Position statement from the Italian Society of Andrology and Sexual Medicine (SIAMS): Endorsing Organization: Italian Society of Embryology, Reproduction, and Research (SIERR). J. Endocrinol. Invest. 2022, 45, 1085–1113. [Google Scholar] [CrossRef]
- Minhas, S.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropoulos, K.; Gül, M.; et al. European Association of Urology Guidelines on Male Sexual and Reproductive Health: 2021 Update on Male Infertility. Eur Urol. 2021, 80, 603–620. [Google Scholar] [CrossRef]
- Yığman, M.; Yığman, F.; Tangal, S.; Haliloğlu, A.H.; Çağlar, G.S. Pre-test anxiety levels and postoperative pain in non-obstructive azoospermic patients: Is klinefelter syndrome a predisposing factor? Urol. J. 2022, 89, 280–284. [Google Scholar] [CrossRef]
- Gilbert, K.; Nangia, A.K.; Dupree, J.M.; Smith, J.F.; Mehta, A. Fertility preservation for men with testicular cancer: Is sperm cryopreservation cost effective in the era of assisted reproductive technology? Urol. Oncol. 2018, 36, e1–e92. [Google Scholar] [CrossRef]
- Pallotti, F.; Barbonetti, A.; Rastrelli, G.; Santi, D.; Corona, G.; Lombardo, F. The impact of male factors and their correct and early diagnosis in the infertile couple’s pathway: 2021 perspectives. J. Endocrinol. Invest. 2022, 45, 1807–1822. [Google Scholar] [CrossRef] [PubMed]
- Paoli, D.; Pelloni, M.; Lenzi, A.; Lombardo, F. Cryopreservation of Sperm: Effects on Chromatin and Strategies to Prevent Them. Adv. Exp. Med. Biol. 2019, 1166, 149–167. [Google Scholar] [PubMed]
- Paoli, D.; Pallotti, F.; Lenzi, A.; Lombardo, F. Fatherhood and Sperm DNA Damage in Testicular Cancer Patients. Front. Endocrinol. 2018, 9, 506. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.S.; Tsai, Y.C.; Chen, J.J.; Peng, C.H.; Hsieh, J.H.; Wang, C.C. Modified transurethral incision of the bladder neck treating primary bladder neck obstruction in young men: A method to improve voiding function and to preserve antegrade ejaculation. Urol. Int. 2008, 80, 26–30. [Google Scholar] [CrossRef]
- Warwick, R.T. A urodynamic review of bladder outlet obstruction in the male and its clinical implications. Urol. Clin. N. Am. 1979, 6, 171–192. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age (Years) | Semen Volume (mL) | Sperm Concentration (×106/mL) | Total Sperm Number (×106) | Progressive Motility (%) | Abnormal Forms (%) | Leukocytes (×106) | |
|---|---|---|---|---|---|---|---|
| T0 (73 pts) | 36.0 ± 9.0 (37.2) | 3.3 ± 1.8 (3.0) | 101.3 ± 105.5 (77.0) | 335.8 ± 509.3 (215.6) | 43.3 ± 15.3 (50.0) | 83.5 ± 9.0 (83.0) | 1.0 ± 1.4 (0.6) |
| Semen Volume (mL) | Sperm Concentration (×106/mL) | Total Sperm Number (×106) | Progressive Motility (%) | Abnormal Forms (%) | Leukocytes (×106) | |
|---|---|---|---|---|---|---|
| T0 (25 pts) | 2.9 ± 1.7 (2.5) | 107.5 ± 118.8 (94.0) | 239.3 ± 206.4 (180.0) | 45.2 ± 15.0 (50.0) | 82.0 ± 10.7 (83.0) | 0.8 ± 0.7 (0.6) |
| T1 (25 pts) | 2.4 ± 1.7 (2.0) | 72.6 ± 59.3 (78.0) | 145.0 ± 127.5 (116.0) | 43.6 ± 18.7 (55.0) | 84.6 ± 8.7 (87.0) | 0.5 ± 0.3 (0.4) |
| p value | 0.159 | 0.058 | 0.015 | 0.806 | 0.049 | 0.031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirsch, M.N.; Pallotti, F.; Faja, F.; Buonacquisto, A.; Cicolani, G.; Conflitti, A.C.; Di Chiano, S.; Lenzi, A.; Lombardo, F.; Paoli, D. Bladder Neck Obstruction: Experience and Management in a Sperm Bank. Life 2023, 13, 842. https://doi.org/10.3390/life13030842
Hirsch MN, Pallotti F, Faja F, Buonacquisto A, Cicolani G, Conflitti AC, Di Chiano S, Lenzi A, Lombardo F, Paoli D. Bladder Neck Obstruction: Experience and Management in a Sperm Bank. Life. 2023; 13(3):842. https://doi.org/10.3390/life13030842
Chicago/Turabian StyleHirsch, Maria Neve, Francesco Pallotti, Fabiana Faja, Alessandra Buonacquisto, Gaia Cicolani, Anna Chiara Conflitti, Silvia Di Chiano, Andrea Lenzi, Francesco Lombardo, and Donatella Paoli. 2023. "Bladder Neck Obstruction: Experience and Management in a Sperm Bank" Life 13, no. 3: 842. https://doi.org/10.3390/life13030842