
Effectiveness of SMILE Combined with Micro-Monovision in Presbyopic Patients: A Pilot Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Procedure
2.3. Surgery
2.4. Statistical Analysis
3. Results
3.1. Safety
3.2. Efficacy
3.3. Patient-Reported Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marcos, S. Ocular Ageing: Improving the Quality of Sight for Cataract and Presbyopia Sufferers. LYCHNOS (Noteb. Fund. Gen. CSIC) 2010, 2, 60–65. [Google Scholar]
- Jain, S.; Arora, I.; Azar, D.T. Success of Monovision in Presbyopes: Review of the Literature and Potential Applications to Refractive Surgery. Surv. Ophthalmol. 1996, 40, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Couch, D.G.; Archer, T.J. LASIK for Hyperopic Astigmatism and Presbyopia Using Micro-Monovision with the Carl Zeiss Meditec MEL80 Platform. J. Refract. Surg. 2009, 25, 37–58. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Yin, Y.; Wu, X.; Li, Y.; Xiang, A.; Lu, Y.; Fu, Q.; Hu, T.; Du, K.; Wen, D. Clinical Outcomes after Small-Incision Lenticule Extraction versus Femtosecond Laser-Assisted LASIK for High Myopia: A Meta-Analysis. PLoS ONE 2021, 16, e0242059. [Google Scholar] [CrossRef]
- Sambhi, R.-D.S.; Sambhi, G.D.S.; Mather, R.; Malvankar-Mehta, M.S. Dry Eye after Refractive Surgery: A Meta-Analysis. Can. J. Ophthalmol. 2020, 55, 99–106. [Google Scholar] [CrossRef]
- Kim, J.S.; Ra, H.; Rho, C.R. Retrospective Observational Study of Micro-Monovision Small Incision Lenticule Extraction (SMILE) for the Correction of Presbyopia and Myopia. Medicine 2018, 97, e13586. [Google Scholar] [CrossRef]
- Fu, D.; Zeng, L.; Zhao, J.; Miao, H.; Yu, Z.; Zhou, X. Safety and Satisfaction of Myopic Small-Incision Lenticule Extraction Combined with Monovision. BMC Ophthalmol. 2018, 18, 131. [Google Scholar] [CrossRef] [Green Version]
- Luft, N.; Siedlecki, J.; Sekundo, W.; Wertheimer, C.; Kreutzer, T.C.; Mayer, W.J.; Priglinger, S.G.; Dirisamer, M. Small Incision Lenticule Extraction (SMILE) Monovision for Presbyopia Correction. Eur. J. Ophthalmol. 2017, 28, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Almutairi, M.S.; Altoaimi, B.H.; Bradley, A. Impact of Monovision on Dynamic Accommodation of Early Presbyopes. Ophthal. Physl. Opt. 2020, 40, 47–59. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Burguera, N.; Piñero, D.P. Prediction of Visual Acuity and Contrast Sensitivity From Optical Simulations With Multifocal Intraocular Lenses. J. Refract. Surg. 2019, 35, 789–795. [Google Scholar] [CrossRef]
- Seijas, O.; de Liaño, P.G.; de Liaño, R.G.; Roberts, C.J.; Piedrahita-Alonso, E.; Diaz, E. Ocular Dominance Diagnosis and Its Influence in Monovision. Am. J. Ophthalmol. 2007, 144, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Dupps, W.J.; Kohnen, T.; Mamalis, N.; Rosen, E.S.; Koch, D.D.; Obstbaum, S.A.; Waring, G.O.; Reinstein, D.Z.; Stulting, R.D. Standardized Graphs and Terms for Refractive Surgery Results. J. Cataract. Refract. Surg. 2011, 37, 1–3. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Burguera, N.; Piñero, D.P. Long-Term Efficacy, Visual Performance and Patient Reported Outcomes with a Trifocal Intraocular Lens: A Six-Year Follow-Up. J. Clin. Med. 2021, 10, 2009. [Google Scholar] [CrossRef]
- Rodríguez-Vallejo, M.; Ferrando, V.; Montagud, D.; Monsoriu, J.A.; Furlan, W.D. Stereopsis Assessment at Multiple Distances with an IPad Application. Displays 2017, 50, 35–40. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Tauste, A.; Albarrán, C.; Basterra, I.; Piñero, D. Fast Measure of Visual Acuity and Contrast Sensitivity Defocus Curves with an IPad Application. Open Ophthalmol. J. 2019, 13, 15–22. [Google Scholar] [CrossRef] [Green Version]
- González-Pérez, M.; Pérez-Garmendia, C.; Barrio, A.R.; García-Montero, M.; Antona, B. Spanish Cross-Cultural Adaptation and Rasch Analysis of the Convergence Insufficiency Symptom Survey (CISS). Transl. Vis. Sci. Technol. 2020, 9, 23. [Google Scholar] [CrossRef] [Green Version]
- Morlock, R.; Wirth, R.J.; Tally, S.R.; Garufis, C.; Heichel, C.W.D. Patient-Reported Spectacle Independence Questionnaire (PRSIQ): Development and Validation. Am. J. Ophthalmol. 2017, 178, 101–114. [Google Scholar] [CrossRef]
- Kimlin, J.A.; Black, A.A.; Wood, J.M. Older Drivers’ Self-reported Vision-related Night-driving Difficulties and Night-driving Performance. Acta Ophthalmol. 2020, 98, e513–e5192020. [Google Scholar] [CrossRef]
- Fernández, J.; Ribeiro, F.J.; Rodríguez-Vallejo, M.; Dupps, W.J.; Werner, L.; Srinivasan, S.; Kohnen, T. Standard for Collecting and Reporting Outcomes of IOL–Based Refractive Surgery: Update for Enhanced Monofocal, EDOF, and Multifocal IOLs. J. Cataract. Refract. Surg. 2022, 48, 1235–1241. [Google Scholar] [CrossRef]
- Zhang, T.; Sun, Y.; Weng, S.; Liu, M.; Zhou, Y.; Yang, X.; Stojanovic, A.; Liu, Q. Aspheric Micro-Monovision LASIK in Correction of Presbyopia and Myopic Astigmatism: Early Clinical Outcomes in a Chinese Population. J. Refract. Surg. 2016, 32, 680–685. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M. LASIK for Myopic Astigmatism and Presbyopia Using Non-Linear Aspheric Micro-Monovision with the Carl Zeiss Meditec MEL 80 Platform. J. Refract. Surg. 2011, 27, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Carp, G.I.; Archer, T.J.; Gobbe, M. LASIK for Presbyopia Correction in Emmetropic Patients Using Aspheric Ablation Profiles and a Micro-Monovision Protocol With the Carl Zeiss Meditec MEL 80 and VisuMax. J. Refract. Surg. 2012, 28, 531–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganesh, S.; Brar, S.; Gautam, M.; Sriprakash, K. Visual and Refractive Outcomes Following Laser Blended Vision Using Non-Linear Aspheric Micro-Monovision. J. Refract. Surg. 2020, 36, 300–307. [Google Scholar] [CrossRef]
- Fernández, J.; Molina-Martín, A.; Rocha-de-Lossada, C.; Rodríguez-Vallejo, M.; Piñero, D.P. Clinical Outcomes of Presbyopia Correction with the Latest Techniques of PresbyLASIK: A Systematic Review. Eye 2022, 37, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kohnen, T.; Böhm, M.; Herzog, M.; Hemkeppler, E.; Petermann, K.; Lwowski, C. Near Visual Acuity and Patient-Reported Outcomes in Presbyopic Patients after Bilateral Multifocal Aspheric Laser in Situ Keratomileusis Excimer Laser Surgery. J. Cataract. Refr. Surg. 2020, 46, 944–952. [Google Scholar] [CrossRef]
- Fu, D.; Zhao, J.; Zeng, L.; Zhou, X. One Year Outcome and Satisfaction of Presbyopia Correction Using the PresbyMAX® Monocular Ablation Profile. Front. Med. 2020, 7, 589275. [Google Scholar] [CrossRef]
- Nanavaty, M.A.; Daya, S.M. Refractive Lens Exchange versus Phakic Intraocular Lenses. Curr. Opin. Ophthalmol. 2012, 23, 54–61. [Google Scholar] [CrossRef]
- Djodeyre, M.R.; Ortega-Usobiaga, J.; Beltran, J.; Druchkiv, V.; Baviera-Sabater, J.; Bouza-Miguens, C. Bilateral Refractive Lens Exchange With Trifocal Intraocular Lens for Hyperopia in Patients Younger Than 40 Years: A Case–Control Study. J. Refract. Surg. 2021, 37, 524–531. [Google Scholar] [CrossRef]
- Thylefors, J.; Jakobsson, G.; Zetterberg, M.; Sheikh, R. Retinal Detachment after Cataract Surgery: A Population-based Study. Acta Ophthalmol. 2022, 100, e1595–e15992022. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Tauste, A.; Piñero, D.P. From Presbyopia to Cataracts: A Critical Review on Dysfunctional Lens Syndrome. J. Ophthalmol. 2018, 2018, 4318405. [Google Scholar] [CrossRef]
- Fernández, J.; Burguera, N.; Rocha-de-Lossada, C.; Rachwani-Anil, R.; Rodríguez-Vallejo, M. Objective Cataract Grading Methods and Expected Contrast Sensitivity Reestablishment with Multifocal Intraocular Lenses. Int. Ophthalmol. 2023, 1–8. [Google Scholar] [CrossRef]
- Sevik, M.O.; Turhan, S.A.; Toker, E. Clinical Outcomes with a Low Add Multifocal and an Extended Depth of Focus Intraocular Lenses Both Implanted with Mini-Monovision. Eye 2021, 36, 1168–1177. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Tauste, A.; Piñero, D.P. New Approach for the Calculation of the Intraocular Lens Power Based on the Fictitious Corneal Refractive Index Estimation. J. Ophthalmol. 2019, 2019, 2796126. [Google Scholar] [CrossRef]
- Lwowski, C.; Keer, K.V.; Adas, M.; Schwarz, L.; Hinzelmann, L.; Pawlowicz, K.; Kohnen, T. Ray-Tracing Calculation Using Scheimpflug Tomography of Diffractive Extended Depth of Focus IOLs Following Myopic LASIK. J. Refract. Surg. 2021, 37, 231–239. [Google Scholar] [CrossRef]
- Schmid, R.; Luedtke, H. A Novel Concept of Correcting Presbyopia: First Clinical Results with a Phakic Diffractive Intraocular Lens. Clin. Ophthalmol. Auckl. N. Z. 2020, 14, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- BV, O. Clinical Trial With Artiflex Presbyopic. Available online: https://clinicaltrials.gov/ct2/show/NCT04632784 (accessed on 14 March 2023).
- Packer, M.; Alfonso, J.F.; Aramberri, J.; Elies, D.; Fernandez, J.; Mertens, E. Performance and Safety of the Extended Depth of Focus Implantable Collamer® Lens (EDOF ICL) in Phakic Subjects with Presbyopia. Clin. Ophthalmol. Auckl. N. Z. 2020, 14, 2717–2730. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, S.L.; Herman, W.K.; Alfieri, C.D.; Castleberry, K.A.; Parks, M.M.; Birch, E.E. Stereoacuity and Foveal Fusion in Adults with Long-Standing Surgical Monovision. J. Am. Assoc. Pediatric. Ophthalmol. Strabismus 2001, 5, 342–347. [Google Scholar] [CrossRef]
- Romero, M.; Castillo, A.; Carmona, D.; Palomino, C. Visual Quality after Presbyopia Correction with Excimer Laser Ablation Using Micromonovision and Modulation of Spherical Aberration. J. Cataract. Refract. Surg. 2019, 45, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Quaia, C.; Optican, L.M.; Cumming, B.G. Binocular Summation for Reflexive Eye Movements. J. Vis. 2018, 18, 7. [Google Scholar] [CrossRef] [Green Version]
- Boström, K.J.; Warzecha, A.-K. Ocular Following Response to Sampled Motion. Vis. Res. 2009, 49, 1693–1701. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Median | Interquartile Range |
|---|---|---|
| Age | 45 | 5 |
| Sphere (D) | −2.88 | 2 |
| Cylinder (D) | −0.5 | 0.75 |
| SE (D) | −3.13 | 1.72 |
| Dominant Predicted SE (D) | −0.13 | 0.56 |
| Non-Dominant Predicted SE (D) | −0.94 | 0.63 |
| Photopic pupil diameter (mm) | 3.8 | 1.12 |
| Mesopic pupil diameter (mm) | 6.05 | 0.94 |
| Ruler pupil diameter (mm) | 4 | 0.5 |
| Axial Length (mm) | 24.60 | 1.27 |
| Mean Keratometry (D) | 43.25 | 0.89 |
| Variable | Preoperative | 6-Month | z, p-Value |
|---|---|---|---|
| Visual Acuity (logMAR) | |||
| Far (4 m) | −0.1 (0.2) | 0 (0.18) | 0.7, 0.48 |
| Intermediate (66 cm) | 0 (0.02) | −0.1 (0.15) | −1.63, 0.1 |
| Near (40 cm) | −0.1 (0.2) | −0.05 (0.18) | 1.12, 0.66 |
| Stereopsis (arcsec) | |||
| Far (4 m) | 79 (178) | 119 (20) | 0.32, 0.75 |
| Intermediate (66 cm) | 79 (79) | 40 (9.75) | −1.63, 0.10 |
| Near (40 cm) | 79 (49) | 59 (39) | −1.00, 0.32 |
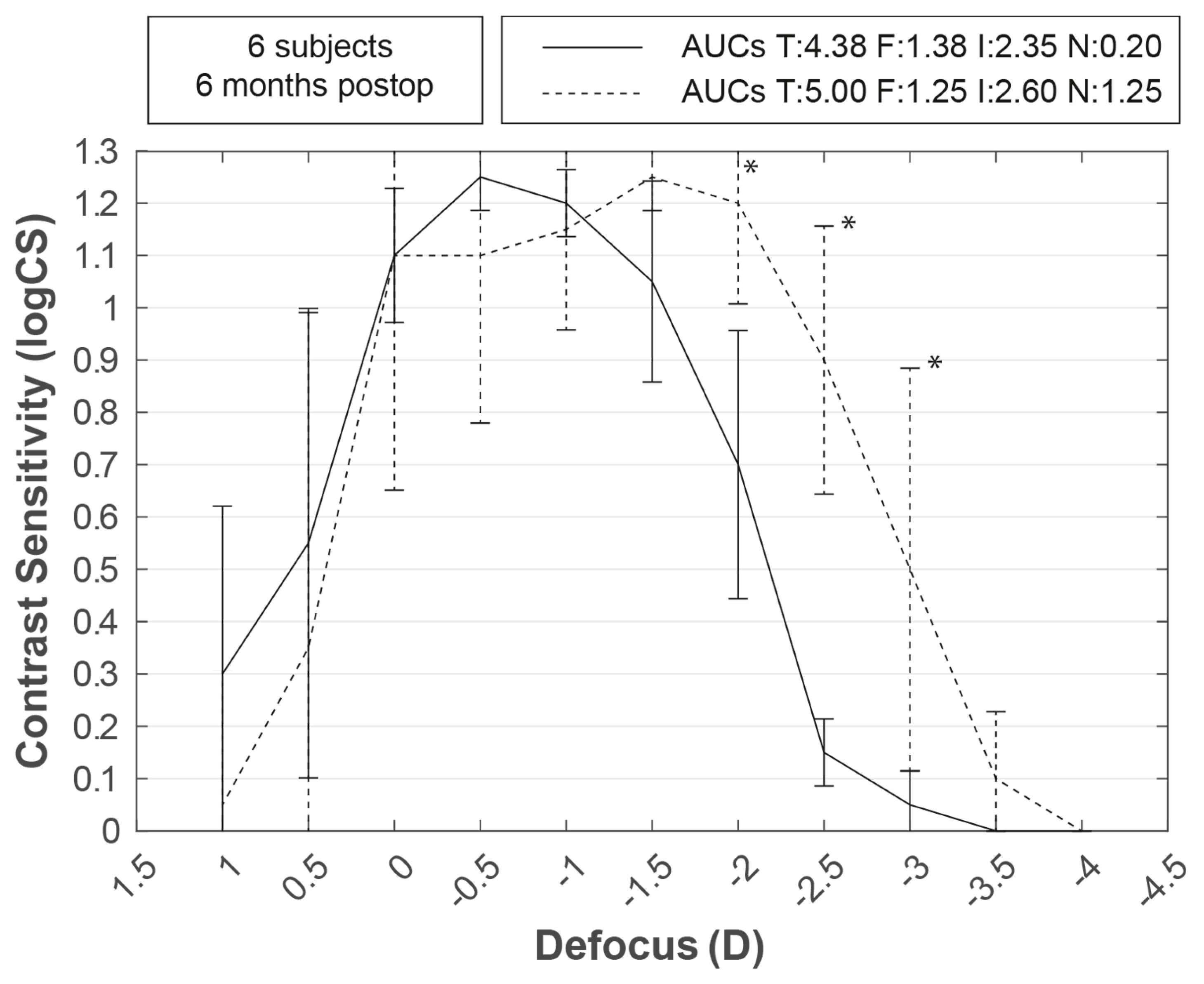
| Contrast Sensitivity (logCS) | |||
| Defocus −4.0 | 0 (0.03) | 0 (0.1) | 1, 0.32 |
| Defocus −3.5 | 0 (0.03) | 0.1 (0.38) | 1.63, 0.1 |
| Defocus −3.0 | 0.05 (0.1) | 0.5 (0.68) | 2.02, 0.04 |
| Defocus −2.5 | 0.15 (0.2) | 0.9 (0.58) | 2.04, 0.04 |
| Defocus −2.0 | 0.7 (0.4) | 1.2 (0.40) | 2.03, 0.04 |
| Defocus −1.5 | 1.05 (0.3) | 1.25 (0.18) | 1.60, 0.1 |
| Defocus −1.0 | 1.2 (0.12) | 1.15 (0.30) | 0, 1 |
| Defocus −0.5 | 1.25 (0.20) | 1.10 (0.50) | −1.60, 0.1 |
| Defocus 0.0 | 1.1 (0.38) | 1.10 (0.75) | −1, 0.32 |
| Defocus 0.5 | 0.55 (0.80) | 0.35 (1.02) | 2.22, 0.03 |
| Defocus 1.0 | 0.30 (0.55) | 0.05 (0.48) | −1.83, 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández, J.; Alonso-Aliste, F.; Burguera, N.; Hernández-Lucena, J.; Amián-Cordero, J.; Rodríguez-Vallejo, M. Effectiveness of SMILE Combined with Micro-Monovision in Presbyopic Patients: A Pilot Study. Life 2023, 13, 838. https://doi.org/10.3390/life13030838
Fernández J, Alonso-Aliste F, Burguera N, Hernández-Lucena J, Amián-Cordero J, Rodríguez-Vallejo M. Effectiveness of SMILE Combined with Micro-Monovision in Presbyopic Patients: A Pilot Study. Life. 2023; 13(3):838. https://doi.org/10.3390/life13030838
Chicago/Turabian StyleFernández, Joaquín, Federico Alonso-Aliste, Noemí Burguera, Julia Hernández-Lucena, Jonatan Amián-Cordero, and Manuel Rodríguez-Vallejo. 2023. "Effectiveness of SMILE Combined with Micro-Monovision in Presbyopic Patients: A Pilot Study" Life 13, no. 3: 838. https://doi.org/10.3390/life13030838