
The Role of Oxidative Stress in the Aging Eye

1
Boston University Chobanian & Avedisian School of Medicine, Boston, MA 02118, USA
2
Department of Ophthalmology, Boston Medical Center, Boston, MA 02118, USA
*
Author to whom correspondence should be addressed.
Life 2023, 13(3), 837; https://doi.org/10.3390/life13030837
Submission received: 20 February 2023
/
Revised: 13 March 2023
/
Accepted: 14 March 2023
/
Published: 20 March 2023
(This article belongs to the Special Issue Eye Manifestations of Systemic Disease)
Abstract
:Given the expanding elderly population in the United States and the world, it is important to understand the processes underlying both natural and pathological age-related changes in the eye. Both the anterior and posterior segment of the eye undergo changes in biological, chemical, and physical properties driven by oxidative stress. With advancing age, changes in the anterior segment include dermatochalasis, blepharoptosis, thickening of the sclera, loss of corneal endothelial cells, and stiffening of the lens. Changes in the posterior segment include lowered viscoelasticity of the vitreous body, photoreceptor cell loss, and drusen deposition at the macula and fovea. Age-related ocular pathologies including glaucoma, cataracts, and age-related macular degeneration are largely mediated by oxidative stress. The prevalence of these diseases is expected to increase in the coming years, highlighting the need to develop new therapies that address oxidative stress and slow the progression of age-related pathologies.
1. Introduction
According to the U.S. Census Bureau, nearly a quarter of Americans will be older than 65 years of age by 2030, and the number of Americans 85 years of age and older will triple by 2060 [1]. In fact, the federal agency projects that by 2060, the elderly will outnumber children for the first time in U.S. history [1]. This expansion of the elderly population underscores the need for an understanding of the changes in the human body that occur as a result of the natural aging process.
Several of the most salient changes are vision-related, and the elderly often experience difficulties in their ability to accommodate to light, discriminate between colors, and view close objects [2]. The prevalence of eye conditions involving the eyelids, extraocular muscles, cornea, lens, and retina increases with age (Table 1) [3,4,5]. Given that vision impairment has been associated with problems performing activities of daily living and with psychiatric conditions [6,7], it is important to understand the changes that occur in the eye as a result of growing older. We present a review of the literature regarding the normal changes in ocular anatomy and function that are secondary to aging (Table 2 and Table 3). Our work discusses the role of oxidative stress in the pathophysiology of the three most common ocular pathologies that occur with aging, including cataracts, glaucoma, and macular degeneration.
2. External and Anterior Segment Changes
2.1. Eyelids and Lacrimal Glands
Aging in the face, including the eyelids, is driven by a lower regenerative capacity and upregulated degradative enzyme activity [8]. These changes cause collagen degradation, especially in the deep dermis. As aging continues, extracellular matrix components lose their interwoven organization and tight interactions [9].
Beyond tissue atrophy, the lower eyelid often undergoes horizontal lid laxity [4,8]. The anterior inferior periocular soft tissue and orbital fat pad expand in volume with aging [8,10], leading to a “sunken in” appearance to the eyes and pronouncing lid laxity. Continued lid laxity leads to ectropion, or eversion of the eyelid margin. However, if the pretarsal orbicularis muscle maintains its strength while the midface sags during the aging process, one instead experiences entropion, or inversion of the lower eyelid [4]. Either of these conditions can result in foreign body sensation, tearing, or corneal damage [8].
The upper eyelids can be impacted by dermatochalasis and blepharoptosis. Dermatochalasis is the product of external environmental insults and redundant upper eyelid skin [8]. Blepharoptosis, on the other hand, results from loss of muscle tone or dehiscence of the levator palpebrae superioris muscle and the Müller muscle [8,11]. Flament et al. compared digital photographs of women from six different ethnicities and found that as age progresses, the height of the eyes decreases due to the sagging of the upper eyelid and the angle between the eye length and the horizontal inter-pupillar line decreases from the sagging of the outer corner of the eyes [12].
Dry eye is common among the elderly due to age-related changes in the lacrimal and meibomian glands. Histopathologic changes in lacrimal glands include atrophy, fibrosis, ductal dilation, and proliferation, as well as lymphocytic and fatty infiltration [13,14,15,16,17]. Similarly, meibomian glands undergo atrophy [13,15]. The pathogenesis of dry eye also involves oxidative stress, as the lacrimal glands of aged mice showed an accumulation of 8-hydroxydeoxyguanosine and lipofuscin-like inclusions, among other oxidative stress biomarkers [18]. Over time, the ocular surface and tear film become compromised [18]. These changes manifest as diminished tear production, resulting in a loss of contrast sensitivity and functional visual acuity, as well as dry eye symptoms including burning, epiphora, and foreign body sensation [13,14,15,16,17].
2.2. Sclera
There exists conflicting data on the association between changes in the thickness of the sclera and age [19,20,21,22]. However, an increase in the stiffness and rigidity of the sclera is well established and has been attributed to a decrease in connective tissue and extracellular matrix components, including diminution of elastin fibers, decorin, and biglycan [23,24]. Additionally, the sclera stiffens with age due to elevated fibril crosslinks and tropocollagen molecules per fibril [23]. The formation of senile scleral plaques (calcium sulfate or calcium phosphate at the insertions of medial and lateral rectus muscles) may also contribute to increased scleral rigidity in older patients [25,26]. Individuals of African descent appear to experience a faster rate of increase in age-related rigidity compared to individuals of European descent, which may be linked to greater glaucoma prevalence in elderly African Americans [27].
2.3. Cornea
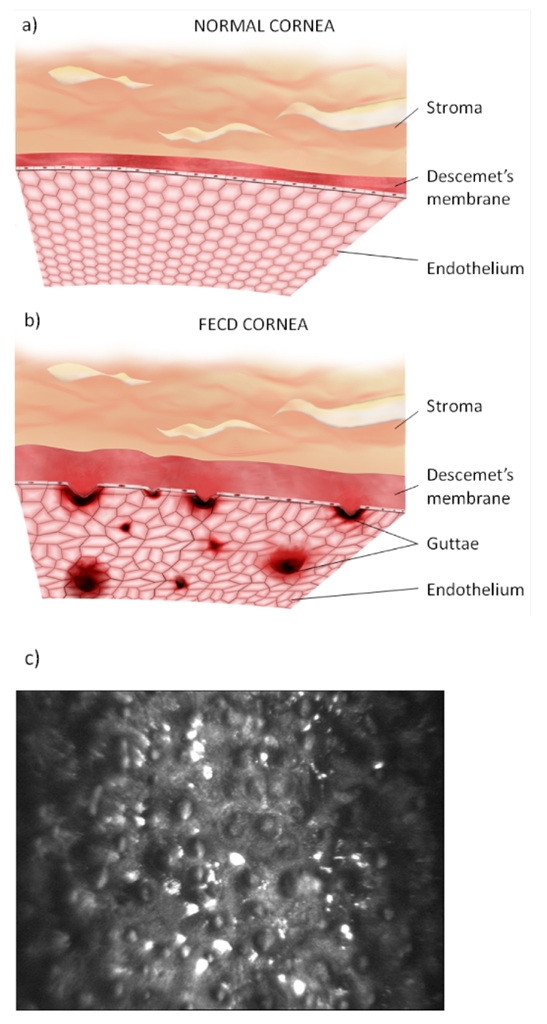
The aging cornea undergoes alterations in both optical and physical properties, degeneration, and a reduction in immunological capacity [4,26]. Histologic changes in the cornea include thickening of the Descemet’s and epithelial basement membranes, in addition to decreases in the corneal stromal cell density as well as corneal endothelial cell and conjunctival keratocyte numbers [28]. Fuchs’ dystrophy is an age-related loss of corneal endothelial cells accompanied by the deposition of extracellular material (guttae) on Descemet’s membrane (Figure 1) [28,29]. The decline in corneal endothelial cells leads to hypertrophy in the remaining endothelial cells as a compensatory response [4,28]. As endothelial cell counts fall below critical levels, they lose the ability to adequately dehydrate the cornea, resulting in edema and lower corneal clarity [28].
Previous studies have demonstrated an increased prevalence of astigmatism with advancing age and a shift from with-the-rule to against-the-rule astigmatism [4,30,31]. Against-the-rule astigmatism, characterized by a steeper horizontal corneal curvature, results from altered mechanical properties of the eyelid, corneal stroma, Descemet’s membrane, and extraocular muscles [30].
Corneal degenerative changes are visibly evident throughout the corneal layers [4]. The deposition of white-grey lipid opacities in the peripheral cornea is termed arcus senilis [32]. Cornea farinata is identified throughout the corneal stroma by its small, grey, and opaque appearance [33]. Central and posterior corneal stroma may have crocodile shagreen, which is characterized by classic polygonal opacities akin to crocodile skin [34]. While each of these conditions are usually asymptomatic, their incidence rates are directly proportional to age.
The cornea also becomes immunocompromised with age. Animal studies have shown phagocytic dysfunction and a loss of phagocytically active cells in the corneas of older mice, resulting in impaired recovery from gram-negative bacterial infections [35]. Older mice were also found to have a defective response to Pseudomonas infection due to decreased upregulation of intercellular adhesion molecule 1, delaying infiltration of polymorphonuclear cells into the cornea and allowing for unchecked bacterial growth [36]. These immunological changes found in mouse models may have implications for the human population. Infectious keratitis presents more severely in the elderly population compared to the younger population [37]. Constantinou et al. found that the majority of corneal ulcers among the elderly are secondary to non-healing microbial keratitis caused by Pseudomonas aeruginosa [38].
2.4. Trabecular Meshwork
The trabecular meshwork (TM) undergoes changes in shape, cellularity, and pigmentation as a function of age. A reduction in the TM height leads to the meshwork assuming a rhomboid shape in older eyes [26,39,40]. The cellularity of the TM declines linearly with a loss of 0.58% of cells per year and a 47% decline in absolute cell number over an 81-year study period [41]. The number of TM stem cells was also found to diminish over time [42]. These changes, in conjunction with an increase in extracellular components and the narrowing of aqueous humor outflow tracts, are responsible for greater resistance to aqueous humor outflow with age [43]. Elevated intraocular pressure, resulting in part from obstructed aqueous outflow, accounts for the higher prevalence of glaucoma in older patients. Lastly, prior studies have reported TM hyperpigmentation due to increased melanin in older patients [4,44].
2.5. Ciliary Body
The ciliary body is subject to changes in the morphology, cellularity, and collagen content of its stroma [26]. The muscle has a tendency to shorten and widen while its internal apical edge moves forward over time [45]. The nasal and temporal maximum ciliary muscle thickness increases with age [46]. Additionally, the diameter of the unaccommodated ciliary muscle decreases during the aging process [47]. Histologically, the ciliary body loses vascularization and cellularity while accumulating collagen [26].
2.6. Crystalline Lens
The lens undergoes age-dependent changes in geometric parameters. The radii of curvature, lens volume, surface area, cross-sectional area, diameter, lens thickness, and weight linearly increase as a function of time [46,48].
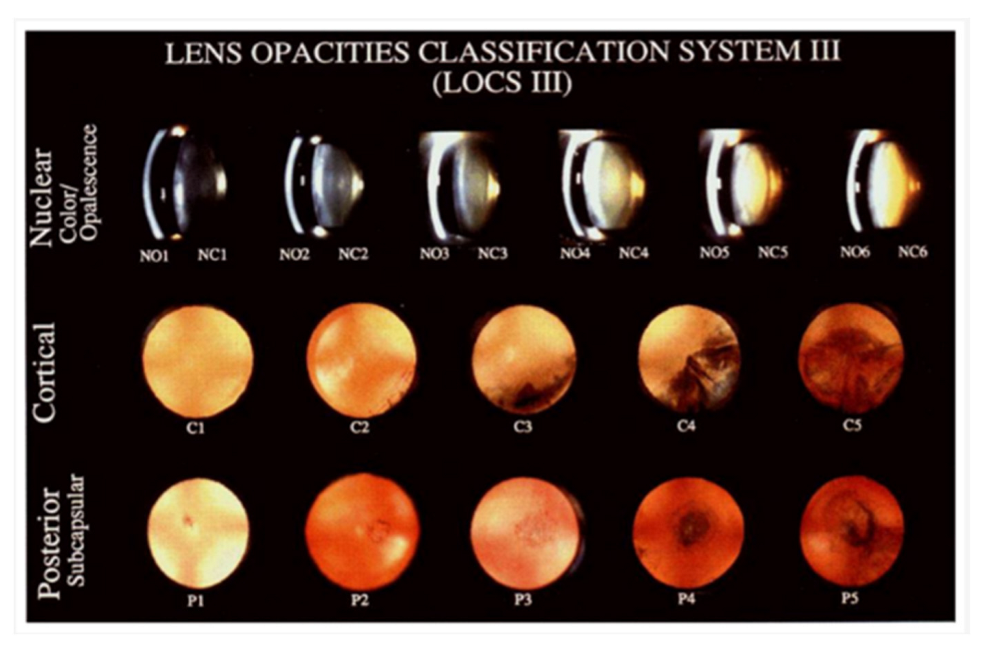
The elderly may have “blue blindness” from the yellowing of the aging crystalline lens [4]. This yellowing increases the absorption of light with shorter wavelengths, including blue light, impairing circadian photoreception [49,50]. Given that blue light is partially responsible for melatonin suppression, the lowered blue light transmittance can lead to mental health disorders in the elderly, including insomnia and depression [50]. Nuclear sclerotic cataracts, posterior subcapsular cataracts, and Morgagnian cataracts arise from age-dependent crystalline lens changes (Figure 2) [26,51]. Cataractogenesis is driven by elevated oxidative stress and the accumulation of oxidized lens proteins [52]. Age-related cataract formation is discussed in greater detail in Section 4.3 of this paper.
Changes in both the ciliary body and lens result in presbyopia, the natural loss of accommodative ability with age. While the contractility and the ring diameter of the ciliary body are unaffected by age [45,53], there is an age-linked reduction in forward ciliary body movement, which is compensated for by greater centripetal ciliary movement [54,55]. Lenticular changes contributing to presbyopia include a 450-fold elevation in stiffness, particularly in the nucleus [56,57]. Biochemical shifts underlying this increased stiffness include an accumulation of cholesterol, dihydrosphingomyelin, and sphingomyelin, as well as a decline in phosphatidylcholines in lens fiber cell membranes and α-crystallin proteins in lens fiber cells. These changes collectively result in decreased membrane and lens flexibility [57,58].
3. Posterior Segment Aging Changes
3.1. Vitreous Humor
Age-related changes to the vitreous humor are the result of structural changes to its component collagen fibrils and hyaluronic acid [4]. Aggregates of type II collagen occupy fluid-filled lacunae and promote liquefaction of the vitreous body [59,60]. With increasing age, these collagenous fibrils gain motility [59]. When over half of the vitreous body has undergone liquefaction, the posterior vitreous cortex detaches from the retina in a condition known as posterior vitreous detachment (PVD), which may be complicated by a retinal tear from vitreoretinal adhesions or anterior contraction of the vitreous body in up to 14% of cases [4,26,59,61]. Other complications of PVD include intraocular hemorrhage, rhegmatogenous retinal detachment, an epiretinal membrane, and macular holes [62,63].
The vitreous body experiences other structural and physical changes as well. The vitreous base undergoes thickening, particularly in its temporal and posterior portions, and the resulting vitreoretinal traction is involved in the development of retinal tears and rhegmatogenous retinal detachment [61,64]. Stiffness, dehydration, and mobility of the vitreous humor increase as a function of age, while viscoelasticity decreases as liquefaction progresses [63,65,66].
3.2. Retina and Retinal Pigment Epithelium
Aging in the retina is characterized by neuronal cell degradation, morphological changes in the retinal layers, and retinal vascular changes. Neuronal cell loss involves a depletion of retinal ganglion cells and photoreceptors, with a greater decline in rods than cones [4,26,67,68,69]. Animal studies have found a shorter outer segment length of rod photoreceptors, but no age-related changes in disc density [70]. There is also an age-linked reduction in the density of rod bipolar cells, which synapse with rod photoreceptor cells [71].
There are several age-dependent microvascular changes as well, especially in disease states. The total retinal blood vessel area, as well as the number of vessels, bifurcation points, and termination points diminish with age [72,73]. The basement membranes of the retinal capillaries undergo thickening and vacuolization, processes that are accelerated by the presence of diabetes [74]. While aging decreases both the number of supportive pericytes and endothelial cells, diabetes only leads to a loss of pericytes [74].
The retinal pigment epithelium (RPE) rests atop Bruch’s membrane and interacts with the vascular choriocapillaris and photoreceptor cells for nutrient and waste exchange. RPE cells outside of the macula increase in width and decrease in height with advancing age [26,75], leading to a generalized thinning of the peripheral RPE layer. The cytoplasm of RPE cells decreases in volume [4], and the cells become progressively vacuolated and pleiomorphic with respect to size, shape, nuclei, and pigmentation [4,75]. Melanin and lipofuscin, two types of pigment molecules found within RPE cells, also undergo age-related changes [76]. There is a tendency for lipofuscin to accumulate with age, and the main fluorophore of lipofuscin, A2E, causes oxidative stress and damages membrane-bound organelles, potentially injuring RPE cells [26,76,77,78]. Lipofuscin also suppresses the antioxidant capacity of melanin [76,79]. Melanin antioxidant properties also diminish due to age-specific photobleaching of melanosomes [76,80]. Lastly, melanin pigmentation of the peripheral retina declines in older patients [4,75,76].
3.3. Choroid
Although changes in the choroidal vascularity index and stroma-to-vessel volume are age-independent, the mean thickness, vessel volume, and stroma volume are lower in the elderly population [81,82]. Furthermore, the choriocapillaris density and diameter diminish as a function of age, and this process is pronounced in patients with early age-related macular degeneration (AMD) [26,83]. Choroidal melanocytes show an age-related fusion of melanosomes into rosettes, an accumulation of irregular lipofuscin granules that bind to melanosomes, and an overall loss of melanosomes [84].
3.4. Macula and Fovea
The macula undergoes anatomical changes secondary to oxidative damage that may predispose elderly patients to AMD [85]. In contrast to peripheral RPE cells, macular RPE cells increase in height over time [26]. Furthermore, Bruch’s membrane thickens and calcifies, which impairs the diffusion of amino acids and other macromolecules [26,83,85,86,87]. Debris from the metabolic turnover of RPE cells, which is mainly composed of lipofuscin and fatty acids, collects on Bruch’s membrane. Subretinal deposits known as drusen appear as yellowish-white opacities between the basal lamina of the RPE and the inner collagenous layer of Bruch’s membrane [4,88]. Age-dependent drusen are the hallmark of AMD, which will be discussed in Section 4.4 of this review (Figure 3) [89]. In contrast to histological studies that report a thickening of the retinal layers over time, an optical coherence tomography segmentation technique was used to demonstrate that the combined retinal pigment epithelium and Bruch’s membrane layer thickness linearly decreases with age at the central subfield, inner macula, and outer macula [90]. Macular vascular flow declines with age, which is secondary to a decreased number of vessels and flow velocity [4,91]. Foveal blood flow is diminished in the elderly due to a lower density and diameter of choroidal vasculature supplying the area [88,92].
3.5. Optic Nerve
Age-related changes of the optic nerve include swelling of axons at the lamina cribrosa, a reduction in nerve fiber density, and an increase in connective tissue composition such as elastic fibers [4,93,94,95,96]. Furthermore, neural rim volume and minimum rim width of the optic nerve head appear to decline with advancing age [97]. Patients with glaucoma have a significantly higher loss of disc rim compared to non-glaucomatous patients [94]. Older patients have been shown to have lower perfusion of the optic nerve head compared to younger patients [98].
4. Age-Related Eye Disease and the Role of Oxidative Stress
4.1. Role of Oxidative Stress in Aging
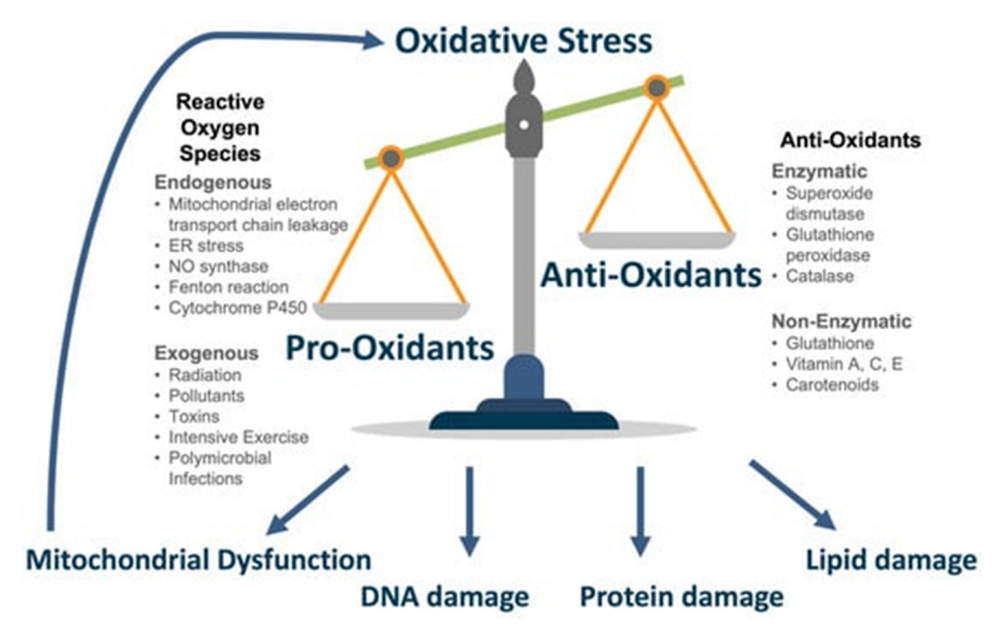
According to the free radical theory of aging, both the natural processes of aging and age-linked diseases are driven by the accumulation of reactive oxygen species (ROS), such as superoxide, hydrogen peroxide, and hydroxyl radicals, from aerobic metabolism [99]. ROS mediate oxidative stress through the chemical modification and damage of connective tissue fibers, DNA, proteins, and lipids [99]. This age-dependent increase in ROS is also accompanied by diminished antioxidant levels, including superoxide dismutase, Vitamin C, and Vitamin E [99]. Oxidative stress plays a significant role in several of the most common age-linked eye diseases (Figure 4) [100].
4.2. Cataracts
The 2010 United States prevalence for cataracts was 15.45% in individuals aged 60–64 years and 68.30% for individuals aged 80 years or older [101]. Patients commonly present with a painless progressive decline in visual acuity. Other symptoms, including photophobia, monocular diplopia, myopic shift, and impaired color vision, are based on the type of age-related cataract—nuclear sclerotic, cortical, or posterior subcapsular [102].
Clinical history and ocular examination are used to diagnose cataracts. Nuclear sclerotic cataracts develop as the lens fibers increase in number and become compressed with age. The lens may appear yellow, and the patient may experience a myopic shift, reduced color discrimination, and worsened visual acuity. Wedge-shaped spokes within the peripheral lens cortex are pathognomonic of cortical cataracts, which appear white. Patients with cortical cataracts may present asymptomatically, especially when the central visual axis is spared. In contrast, patients with posterior subcapsular cataracts commonly complain of glare intolerance. On the slit lamp exam, there are granular opacities in the central posterior cortex under the posterior capsule [102].
Oxidative stress underlies the pathogenesis of cataract formation. There is an accumulation of ROS through the upregulation of pro-oxidant enzymes in the lens, such as nicotinamide adenine dinucleotide phosphate oxidase and xanthine oxidase. ROS chemically modify other macromolecules including lipids and proteins. These chemical modifications include oxidation, deamidation, racemization, glycation, methylation, and truncation [52,103,104,105,106,107,108,109]. Affected proteins may form insoluble complexes that contribute to cataractogenesis [52]. ROS also cause DNA damage and lipid peroxidation in lens epithelial cells [109,110]. Additionally, the rise in oxidants leads to the depletion of antioxidants, including reduced glutathione and ascorbate [111]. The Antioxidants for the Prevention of Cataracts (APC) study investigated the impact of antioxidant supplementation with vitamin C, vitamin E, and beta carotene on self-reported cataract extraction. There was no significant difference in the rate of cataract surgery between those receiving vitamin supplementation and those in the placebo group over a 15-year follow-up period [112].
Age-related ion-pump disruption of transmembrane Na+/K+-ATPase and Ca2+-ATPase also contributes to cataract formation by increasing intracellular sodium, calcium, and water content. This leads to lens swelling and opacification [52,113]. The high levels of intracellular calcium promote ROS generation and the release of apoptotic factors leading to cell death [114,115].
4.3. Glaucoma
The global prevalence of glaucoma is expected to reach 111.8 million by 2040, with a greater disease burden in Asia and Africa [116]. Primary open-angle glaucoma is common with increasing age [117] and is more prevalent in Black and Hispanic/Latino patients [117,118]. The optic nerve damage of glaucoma may be secondary to ocular hypertension or ischemia of the optic nerve head and, when left untreated, can progress to irreversible loss of peripheral vision and blindness [119]. Diagnosis is made with a battery of visual tests including perimetry, gonioscopy, intraocular pressure testing, optical coherence tomography for evaluation of the retinal nerve fiber layer and ganglion cell thickness, and pachymetry [120].
While the pathology of glaucoma is multifactorial, a diminished response to oxidative stress, mediated by an accumulation of reactive oxygen species, plays a role in disease progression. Enzymatic and nonenzymatic antioxidants counteract ROS. While enzymatic antioxidants, such as superoxide dismutase and glutathione peroxidase, increase in activity with age [121], the levels of nonenzymatic antioxidants, such as vitamin C and vitamin E, decline over time [122,123,124]. There is lowered enzymatic antioxidant activity in the trabecular meshwork and depressed total antioxidant activity in the aqueous humor of patients with glaucoma [125]. As a result, studies have demonstrated elevated levels of oxidative stress markers, including protein carbonyls, advanced glycation end products, malondialdehyde, and DNA damage markers, in aqueous humor samples [125,126,127].
The impaired response to oxidative stress is partially due to mitochondrial dysfunction. The mitochondria of metabolically active tissues, such as the retina and optic nerve, are responsible for energy generation, cell survival and death, and ROS production and consumption [128]. Therefore, mitochondrial DNA mutations and slowed mitophagy lead to age-related increases in ROS production [129,130]. Overall, oxidative stress decreases the number of trabecular meshwork cells and causes aqueous humor outflow resistance to rise, resulting in higher intraocular pressure (IOP) [131]. Elevated IOP causes optic nerve pathology including compression of the lamina cribrosa, obstruction of axoplasmic flow, disruption of retrograde transport to retinal ganglion cells (RGCs), and apoptosis of RGCs [119,131].
Chaudhry et al. reviewed studies investigating nutritional supplementation on glaucoma progression. Supplementation with lutein and zeaxanthin, nitric oxide synthase, crocin, zinc, ginkgo biloba, curcumin, or flavonoids decreased RGC loss or extended RGC lifespan. Additionally, treatment with nicotinamide, flavonoids, resveratrol, crocin, ginkgo biloba, or alpha-tocopherol was found to significantly improve ocular blood flow or protect against ischemia [132].
4.4. Age-Related Macular Degeneration
The national prevalence of AMD, based on the 2005–2008 National Health and Nutrition Examination Survey, is 6.5% [133]. It is estimated that the global prevalence of AMD will reach 288 million by 2040 [134]. Risk factors include advancing age, smoking, and hypertension [135]. Early AMD may be asymptomatic, while patients in the late stages of the disease may experience blurry vision, central vision loss, visual distortion, and central scotoma. In addition to clinical history and a fundoscopic examination, diagnosis involves imaging with fluorescein angiography and optical coherence tomography [135].
AMD is classified by early, intermediate, and late stages of disease [136]. Early stages feature drusen deposits. During intermediate stages, these drusen increase in size, number, and pigmentation. Late stages of AMD may be “wet” or “dry”. Wet AMD involves the formation of new abnormal choroidal vessels that are leaky and lead to edema or hemorrhage. Choroidal neovascularization (CNV) is due to the upregulation of angiogenic factors, such as vascular endothelial growth factor (VEGF), after vascular loss and infiltration by macrophages and foreign body giant cells [137]. These vessels may form anastomoses with retinal vessels in advanced stages of neovascular AMD [138]. Intravitreal injections of anti-VEGF medications are the gold standard treatment for CNV in wet AMD. Geographic atrophy is characteristic of late-stage dry AMD [136]. The areas of hypopigmentation seen on fundoscopic exams of patients with geographic atrophy represent degeneration of retinal photoreceptors, RPE, and choriocapillaris [135].
Oxidative stress underlies the pathophysiology of AMD [139]. Harmful reactive oxygen intermediates are produced at the retina from oxygen consumption, irradiation, oxidation of the fatty acids of the photoreceptor outer segment membrane, photosensitizers at the neurosensory retina and the RPE, and RPE phagocytosis [140,141,142]. With advancing age, there is an increased formation of ROS and a decrease in antioxidant levels, resulting in retinal damage.
Several studies have investigated dietary nutrition treatment in AMD. In a follow-up study to the Age-Related Eye Disease Study 2 (AREDS2), there was a significantly lower risk of the development of late AMD in patients receiving supplementation with lutein/zeaxanthin, which are known to defend against ROS at the macula [143,144]. Feng et al. found that dietary lutein improves macular pigment optical density, visual acuity, and contrast sensitivity. The increase in macular pigment optical density appeared to be dose- and treatment duration-dependent [145]. In a randomized controlled trial, the addition of docosahexaenoic acid, lutein, zeaxanthin, resveratrol, and hydroxytyrosol to the original age-related eye disease (ARED) formula (intervention group) reduced inflammatory cytokine levels in patients with unilateral wet AMD compared to subjects receiving the original ARED formulation alone (control group). However, there was no significant improvement in visual acuity after one year between the two groups [146]. Supplementation with oral Macuprev®, which includes lutein, zeaxanthin, N-acetylcysteine, as well as vitamins D3, B12 and C, among other components, was found to increase the amplitude density from multifocal electroretinogram at the central macular area in patients with intermediate AMD, indicating that Macuprev® supplementation may improve macular function [147]. In this disease process, lipoproteins are deposited as drusen at Bruch’s membrane. It has been hypothesized that supplementation with lutein and zeaxanthin modify high- and low-density lipoproteins, which decreases their uptake by RPE uptake receptors, thereby lowering drusen volume at Bruch’s membrane and the risk for neovascularization in AMD [148].
Previous studies have shown an age-dependent accumulation of mitochondrial damage as well as a rise in the levels of lipid peroxidation, advanced glycation end products, lipofuscin, carboxyethylpyrrole proteins, and 8-oxo-7,8-dihydro-2′-deoxyguanosine [149,150,151]. Murine models showed that mice with lower levels of superoxide dismutase, an antioxidant, had higher ROS levels and developed AMD characteristics including drusen, thickened Bruch’s membrane, and CNV [152,153]. ROS also upregulate VEGF levels in the RPE, leading to the CNV seen in wet AMD [154,155]. Cigarette smoking, a high-fat diet, and excess light exposure have been identified as sources of ROS and modifiable environmental risk factors for AMD [154].
Complement system dysfunction also contributes to the pathophysiology of AMD [131]. Intermediate- and late-stage AMD patients were found to have greater levels of complement activation in the intercapillary septa and Bruch’s membrane compared to early-stage and healthy patients [156]. Complement factors C3a and C5a promote mast cell degranulation and the subsequent atrophy of the extracellular matrix seen in geographic atrophy. The atrophy of the extracellular matrix is mediated by released proteinases such as tryptase [136,157]. Other proteolytic enzymes cause choroidal atrophy and thinning as well as the CNV formation seen in wet AMD [136,158]. The deposition of oxidation products, complement proteins, and membrane attack complexes within soft drusen leads to a local inflammatory response [136].
5. Conclusions
The structural and functional changes that occur during the natural aging process at both the anterior and posterior segments of the eye lead to several visual deficits among the elderly and affect their activities of daily life as well as their mental health. The oxidative stress driving these changes is also present in age-related ocular pathologies including glaucoma, cataracts, and macular degeneration. Understanding the biochemical processes underlying these age-related changes is key to discovering therapeutic targets that may prevent or slow the progression of these changes in the eye.
Author Contributions
Conceptualization, D.G. and S.N.; writing—original draft preparation, D.G.; writing—review and editing, D.G. and S.N.; supervision, S.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Census Bureau. The U.S. Joins Other Countries with Large Aging Populations. Available online: https://www.census.gov/library/stories/2018/03/graying-america.html (accessed on 7 November 2022).
- Aging and Your Eyes|National Institute on Aging. Available online: https://www.nia.nih.gov/health/aging-and-your-eyes (accessed on 7 November 2022).
- Klein, R.; Klein, B.E.K. The Prevalence of Age-Related Eye Diseases and Visual Impairment in Aging: Current Estimates. Investig. Opthalmol. Vis. Sci. 2013, 54, ORSF5–ORSF13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvi, S.M. Ageing changes in the eye. Postgrad. Med. J. 2006, 82, 581–587. [Google Scholar] [CrossRef]
- Eye Health Data and Statistics|National Eye Institute. Available online: https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-statistics (accessed on 6 February 2023).
- Shmuely-Dulitzki, Y.; Rovner, B.W. Screening for Depression in Older Persons With Low Vision: Somatic Eye Symptoms and the Geriatric Depression Scale. Am. J. Geriatr. Psychiatry 1997, 5, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Quillen, D.A. Common Causes of Vision Loss in Elderly Patients. Am. Fam. Physician 1999, 60, 99–108. Available online: https://www.aafp.org/pubs/afp/issues/1999/0701/p99.html (accessed on 7 November 2022).
- Ko, A.C.; Korn, B.S.; Kikkawa, D.O. The aging face. Surv. Ophthalmol. 2016, 62, 190–202. [Google Scholar] [CrossRef]
- Naylor, E.C.; Watson, R.E.; Sherratt, M.J. Molecular aspects of skin ageing. Maturitas 2011, 69, 249–256. [Google Scholar] [CrossRef]
- Darcy, S.J.; Miller, T.A.; Goldberg, R.A.; Villablanca, J.P.; Demer, J.L.; Rudkin, G.H. Magnetic Resonance Imaging Characterization of Orbital Changes with Age and Associated Contributions to Lower Eyelid Prominence. Plast. Reconstr. Surg. 2008, 122, 921–929. [Google Scholar] [CrossRef]
- Wendell Damasceno, R.; Avgitidou, G.; Belfort R., R., Jr.; Correa Dantas, P.E.; M Holbach, L.; M Heindl, L. Eyelid aging: Pathophysiology and clinical management. Arq. Bras. Oftalmol. 2015, 78, 328–331. [Google Scholar] [CrossRef] [Green Version]
- Flament, F.; Francois, G.; Seyrek, I.; Saint-Leger, D. Age-related changes to characteristics of the human eyes in women from six different ethnicities. Ski. Res. Technol. 2020, 26, 520–528. [Google Scholar] [CrossRef]
- de Paiva, C.S. Effects of Aging in Dry Eye. Int. Ophthalmol. Clin. 2017, 57, 47–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bukhari, A.A.; Basheer, N.A.; Joharjy, H.I. Age, Gender, and Interracial Variability of Normal Lacrimal Gland Volume Using MRI. Ophthalmic Plast. Reconstr. Surg. 2014, 30, 388–391. [Google Scholar] [CrossRef]
- Obata, H.; Yamamoto, S.; Horiuchi, H.; Machinami, R. Histopathologic Study of Human Lacrimal Gland. Ophthalmology 1995, 102, 678–686. [Google Scholar] [CrossRef]
- Nasu, M.; Matsubara, O.; Yamamoto, H. Post-mortem prevalence of lymphocytic infiltration of the lacrymal gland: A comparative study in autoimmune and non-autoimmune diseases. J. Pathol. 1984, 143, 11–15. [Google Scholar] [CrossRef]
- El-Fadaly, A.B.; El-Shaarawy, E.A.; Rizk, A.A.; Nasralla, M.M.; Shuaib, D.M. Age-related alterations in the lacrimal gland of adult albino rat: A light and electron microscopic study. Ann. Anat.-Anat. Anz. 2014, 196, 336–351. [Google Scholar] [CrossRef]
- Kitazawa, K.; Inomata, T.; Shih, K.; Hughes, J.-W.B.; Bozza, N.; Tomioka, Y.; Numa, K.; Yokoi, N.; Campisi, J.; Dana, R.; et al. Impact of aging on the pathophysiology of dry eye disease: A systematic review and meta-analysis. Ocul. Surf. 2022, 25, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Vurgese, S.; Panda-Jonas, S.; Jonas, J.B. Scleral Thickness in Human Eyes. PLoS ONE 2012, 7, e29692. [Google Scholar] [CrossRef]
- Coudrillier, B.; Tian, J.; Alexander, S.P.; Myers, K.; Quigley, H.A.; Nguyen, T.D. Biomechanics of the Human Posterior Sclera: Age- and Glaucoma-Related Changes Measured Using Inflation Testing. Investig. Opthalmol. Vis. Sci. 2012, 53, 1714–1728. [Google Scholar] [CrossRef]
- Ebneter, A.; Häner, N.U.; Zinkernagel, M.S. Metrics of the normal anterior sclera: Imaging with optical coherence tomography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 1575–1580. [Google Scholar] [CrossRef] [Green Version]
- Read, S.A.; Alonso-Caneiro, D.; Vincent, S.J.; Bremner, A.; Fothergill, A.; Ismail, B.; McGraw, R.; Quirk, C.J.; Wrigley, E. Anterior eye tissue morphology: Scleral and conjunctival thickness in children and young adults. Sci. Rep. 2016, 6, 33796. [Google Scholar] [CrossRef] [Green Version]
- Boote, C.; Sigal, I.A.; Grytz, R.; Hua, Y.; Nguyen, T.D.; Girard, M.J. Scleral structure and biomechanics. Prog. Retin. Eye Res. 2019, 74, 100773. [Google Scholar] [CrossRef]
- A Rada, J.; Achen, V.R.; Penugonda, S.; Schmidt, R.W.; A Mount, B. Proteoglycan composition in the human sclera during growth and aging. Investig. Opthalmol. Vis. Sci. 2000, 41, 1639–1648. [Google Scholar]
- Cogan, D.G.; Kuwabara, T. Focal Senile Translucency of the Sclera. Arch. Ophthalmol. 1959, 62, 604–610. [Google Scholar] [CrossRef]
- Grossniklaus, H.E.; Nickerson, J.M.; Edelhauser, H.F.; Bergman, L.A.M.K.; Berglin, L. Anatomic Alterations in Aging and Age-Related Diseases of the Eye. Investig. Opthalmol. Vis. Sci. 2013, 54, ORSF23–ORSF27. [Google Scholar] [CrossRef]
- Fazio, M.A.; Grytz, R.; Morris, J.S.; Bruno, L.; Girkin, C.A.; Downs, J.C. Human Scleral Structural Stiffness Increases More Rapidly With Age in Donors of African Descent Compared to Donors of European Descent. Investig. Opthalmol. Vis. Sci. 2014, 55, 7189–7198. [Google Scholar] [CrossRef] [PubMed]
- Gipson, I.K. Age-Related Changes and Diseases of the Ocular Surface and Cornea. Investig. Opthalmol. Vis. Sci. 2013, 54, ORSF48–ORSF53. [Google Scholar] [CrossRef] [Green Version]
- Wojcik, K.A.; Kaminska, A.; Blasiak, J.; Szaflik, J.; Szaflik, J.P. Oxidative Stress in the Pathogenesis of Keratoconus and Fuchs Endothelial Corneal Dystrophy. Int. J. Mol. Sci. 2013, 14, 19294–19308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namba, H.; Sugano, A.; Murakami, T.; Utsunomiya, H.; Nishitsuka, K.; Ishizawa, K.; Kayama, T.; Yamashita, H. Age-Related Changes in Astigmatism and Potential Causes. Cornea 2020, 39, S34–S38. [Google Scholar] [CrossRef]
- Shao, X.; Zhou, K.-J.; Pan, A.-P.; Cheng, X.-Y.; Cai, H.-X.; Huang, J.; Yu, A.-Y. Age-Related Changes in Corneal Astigmatism. J. Refract. Surg. 2017, 33, 696–703. [Google Scholar] [CrossRef]
- Munjal, A.; Kaufman, E.J. “Arcus Senilis,” StatPearls. 2022. Available online: https://www-ncbi-nlm-nih-gov.ezproxy.bu.edu/books/NBK554370/ (accessed on 11 November 2022).
- Durand, L.; Bouvier, R.; Burillon, C.; Mutti, P. Cornea farinata. Report of a case: Clinical, histologic and ultrastructural study. J. Fr. Ophtalmol. 1990, 13, 449–455. [Google Scholar]
- Belliveau, M.J.; Brownstein, S.; Agapitos, P.; Font, R.L. Ultrastructural Features of Posterior Crocodile Shagreen of the Cornea. Surv. Ophthalmol. 2009, 54, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Hazlett, L.D.; Kreindler, F.B.; Berk, R.S.; Barrett, R. Aging alters the phagocytic capability of inflammatory cells induced into cornea. Curr. Eye Res. 1990, 9, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Hobden, J.A.; Masinick, S.A.; Barrett, R.P.; Hazlett, L.D. Aged mice fail to upregulate ICAM-1 after Pseudomonas aeruginosa corneal infection. Investig. Ophthalmol. Vis. Sci. 1995, 36, 1107–1114. [Google Scholar]
- van der Meulen, I.J.; van Rooij, J.; Nieuwendaal, C.P.; Van Cleijnenbreugel, H.; Geerards, A.J.; Remeijer, L. Age-related Risk Factors, Culture Outcomes, and Prognosis in Patients Admitted With Infectious Keratitis to Two Dutch Tertiary Referral Centers. Cornea 2008, 27, 539–544. [Google Scholar] [CrossRef]
- Constantinou, M.; Jhanji, V.; Tao, L.W.; Vajpayee, R.B. Clinical review of corneal ulcers resulting in evisceration and enucleation in elderly population. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 247, 1389–1393. [Google Scholar] [CrossRef]
- McMenamin, P.; Lee, W.R.; Aitken, D.A. Age-related Changes in the Human Outflow Apparatus. Ophthalmology 1986, 93, 194–209. [Google Scholar] [CrossRef]
- Choi, W.; Bae, H.W.; Cho, H.; Kim, E.W.; Kim, C.Y.; Seong, G.J. Evaluation of the Relationship Between Age and Trabecular Meshwork Height to Predict the Risk of Glaucoma. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, J.; Murphy, C.; Polansky, J.; Juster, R. Age-related changes in trabecular meshwork cellularity. Investig. Opthalmol. Vis. Sci. 1981, 21, 714–727. Available online: https://pubmed-ncbi-nlm-nih-gov.ezproxy.bu.edu/7298275/ (accessed on 9 November 2022).
- Sundaresan, Y.; Veerappan, M.; Ramasamy, K.S.; Chidambaranathan, G.P. Identification, quantification and age-related changes of human trabecular meshwork stem cells. Eye Vis. 2019, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, M.; Segawa, K.; Urakawa, Y. Age-related changes in the trabecular meshwork of the normal human eye. Jpn. J. Ophthalmol. 1987, 31, 558–569. Available online: https://pubmed-ncbi-nlm-nih-gov.ezproxy.bu.edu/3448324/ (accessed on 9 November 2022).
- Cracknell, K.P.; Grierson, I.; Hogg, P.; Majekodunmi, A.A.; Watson, P.; Marmion, V. Melanin in the trabecular meshwork is associated with age, POAG but not Latanoprost treatment. A masked morphometric study. Exp. Eye Res. 2006, 82, 986–993. [Google Scholar] [CrossRef]
- Pardue, M.T.; Sivak, J.G. Age-Related Changes in Human Ciliary Muscle. Optom. Vis. Sci. 2000, 77, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Corradetti, G.; Song, A.; Pardeshi, A.; Sultan, W.; Lee, J.Y.; Yu, F.; Zhang, L.; Chen, S.; Chopra, V.; et al. Age- and refraction-related changes in anterior segment anatomical structures measured by swept-source anterior segment OCT. PLoS ONE 2020, 15, e0240110. [Google Scholar] [CrossRef]
- A Strenk, S.; Semmlow, J.L.; Strenk, L.M.; Munoz, P.; Gronlund-Jacob, J.; Demarco, J.K. Age-related changes in human ciliary muscle and lens: A magnetic resonance imaging study. Investig. Opthalmol. Vis. Sci. 1999, 40, 1162–1169. [Google Scholar]
- Martinez-Enriquez, E.; de Castro, A.; Mohamed, A.; Sravani, N.G.; Ruggeri, M.; Manns, F.; Marcos, S. Age-Related Changes to the Three-Dimensional Full Shape of the Isolated Human Crystalline Lens. Investig. Opthalmol. Vis. Sci. 2020, 61, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, K.H.; Gibson, G.A. Intraocular lens short wavelength light filtering. Clin. Exp. Optom. 2010, 93, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.L.; Mainster, M.A. Circadian photoreception: Ageing and the eye’s important role in systemic health. Br. J. Ophthalmol. 2008, 92, 1439–1444. [Google Scholar] [CrossRef] [Green Version]
- Zaki, W.M.D.W.; Mutalib, H.A.; Ramlan, L.A.; Hussain, A.; Mustapha, A. Towards a Connected Mobile Cataract Screening System: A Future Approach. J. Imaging 2022, 8, 41. [Google Scholar] [CrossRef]
- Wishart, T.F.; Flokis, M.; Shu, D.Y.; Das, S.J.; Lovicu, F.J. Hallmarks of lens aging and cataractogenesis. Exp. Eye Res. 2021, 210, 108709. [Google Scholar] [CrossRef] [PubMed]
- Richdale, K.; Sinnott, L.T.; Bullimore, M.A.; Wassenaar, P.A.; Schmalbrock, P.; Kao, C.-Y.; Patz, S.; Mutti, N.O.; Glasser, A.; Zadnik, K. Quantification of Age-Related and per Diopter Accommodative Changes of the Lens and Ciliary Muscle in the Emmetropic Human Eye. Investig. Opthalmol. Vis. Sci. 2013, 54, 1095–1105. [Google Scholar] [CrossRef] [Green Version]
- Croft, M.A.; Glasser, A.; Heatley, G.; McDonald, J.; Ebbert, T.; Dahl, D.B.; Nadkarni, N.V.; Kaufman, P.L. Accommodative Ciliary Body and Lens Function in Rhesus Monkeys, I: Normal Lens, Zonule and Ciliary Process Configuration in the Iridectomized Eye. Investig. Opthalmol. Vis. Sci. 2006, 47, 1076–1086. [Google Scholar] [CrossRef] [PubMed]
- Tamm, E.; Croft, M.A.; Jungkunz, W.; Lütjen-Drecoll, E.; Kaufman, P.L. Age-Related Loss of Ciliary Muscle Mobility in the Rhesus Monkey. Arch. Ophthalmol. 1992, 110, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Heys, K.R.; Cram, S.L.; Truscott, R.J.W. Massive increase in the stiffness of the human lens nucleus with age: The basis for presbyopia? Mol. Vis. 2004, 10, 956–963. [Google Scholar]
- Heys, K.R.; Friedrich, M.G.; Truscott, R.J.W. Presbyopia and heat: Changes associated with aging of the human lens suggest a functional role for the small heat shock protein, α-crystallin, in maintaining lens flexibility. Aging Cell 2007, 6, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Grami, V.; Marrero, Y.; Tang, D.; Yappert, M.C.; Rasi, V.; Borchman, D. Human Lens Phospholipid Changes with Age and Cataract. Investig. Opthalmol. Vis. Sci. 2005, 46, 1682–1689. [Google Scholar] [CrossRef] [PubMed]
- Lumi, X.; Hawlina, M.; Glavač, D.; Facskó, A.; Moe, M.C.; Kaarniranta, K.; Petrovski, G. Ageing of the vitreous: From acute onset floaters and flashes to retinal detachment. Ageing Res. Rev. 2015, 21, 71–77. [Google Scholar] [CrossRef]
- Bishop, P.N.; Holmes, D.F.; Kadler, K.E.; McLeod, D.; Bos, K.J. Age-related changes on the surface of vitreous collagen fibrils. Investig. Opthalmol. Vis. Sci. 2004, 45, 1041–1046. [Google Scholar] [CrossRef] [Green Version]
- Sebag, J. Ageing of the vitreous. Eye 1987, 1, 254–262. [Google Scholar] [CrossRef]
- Gastaud, P.; Paoli, V.; Freton, A. Le vieillissement du vitré. J. Fr. D’ophtalmologie 2012, 35, 371–377. [Google Scholar] [CrossRef]
- Walton, K.A.; Meyer, C.H.; Harkrider, C.J.; Cox, T.A.; Toth, C.A. Age-Related Changes in Vitreous Mobility as Measured by Video B Scan Ultrasound. Exp. Eye Res. 2002, 74, 173–180. [Google Scholar] [CrossRef]
- Teng, C.; Chi, H. Vitreous Changes and the Mechanism of Retinal Detachment. Am. J. Ophthalmol. 1957, 44, 335–356. [Google Scholar] [CrossRef]
- Levin, M.; Cohen, N. The effects of aging on the mechanical properties of the vitreous. J. Biomech. 2021, 119, 110310. [Google Scholar] [CrossRef]
- Schulz, A.; Wahl, S.; Rickmann, A.; Ludwig, J.; Stanzel, B.V.; von Briesen, H.; Szurman, P. Age-Related Loss of Human Vitreal Viscoelasticity. Transl. Vis. Sci. Technol. 2019, 8, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnel, S.; Mohand-Said, S.; Sahel, J.-A. The aging of the retina. Exp. Gerontol. 2003, 38, 825–831. [Google Scholar] [CrossRef]
- Gao, H.; Hollyfield, J.G. Aging of the human retina. Differential loss of neurons and retinal pigment epithelial cells. Investig. Opthalmol. Vis. Sci. 1992, 33, 1–17. [Google Scholar]
- A Curcio, C.; Millican, C.L.; A Allen, K.; E Kalina, R. Aging of the human photoreceptor mosaic: Evidence for selective vulnerability of rods in central retina. Investig. Opthalmol. Vis. Sci. 1993, 34, 3278–3296. [Google Scholar]
- Cunea, A.; Jeffery, G. The ageing photoreceptor. Vis. Neurosci. 2007, 24, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, P.; Nag, T.C.; Wadhwa, S. Age-related decrease in rod bipolar cell density of the human retina: An immunohistochemical study. J. Biosci. 2007, 32, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Yamamoto, Y.; Marugame, A.; Ogura, M.; Saito, A.; Ohta, K.; Fukumoto, M.; Murata, T. Age-Related Decrease of the Retinal Vasculature Area Identified with a Novel Computer-Aided Analysis System. Tohoku J. Exp. Med. 2012, 228, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Orlov, N.V.; Coletta, C.; Van Asten, F.; Qian, Y.; Ding, J.; AlGhatrif, M.; Lakatta, E.; Chew, E.; Wong, W.; Swaroop, A.; et al. Age-related changes of the retinal microvasculature. PLoS ONE 2019, 14, e0215916. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, E.; Ripandelli, G.; Taurone, S.; Feher, J.; Plateroti, R.; Kovacs, I.; Magliulo, G.; Orlando, M.P.; Micera, A.; Battaglione, E.; et al. Age and diabetes related changes of the retinal capillaries: An ultrastructural and immunohistochemical study. Int. J. Immunopathol. Pharmacol. 2015, 29, 40–53. [Google Scholar] [CrossRef] [Green Version]
- Friedman, E. The Retinal Pigment Epithelium. Arch. Ophthalmol. 1968, 79, 315–320. [Google Scholar] [CrossRef]
- Bonilha, V.L. Age and disease-related structural changes in the retinal pigment epithelium. Clin. Ophthalmol. 2008, 2, 413–424. [Google Scholar] [CrossRef] [Green Version]
- Schütt, F.; Davies, S.; Kopitz, J.; Holz, F.G.; Boulton, M.E. Photodamage to human RPE cells by A2-E, a retinoid component of lipofuscin. Investig. Ophthalmol. Vis. Sci. 2000, 41, 2303–2308. [Google Scholar]
- Boulton, M.; Dontsov, A.; Jarvis-Evans, J.; Ostrovsky, M.; Svistunenko, D. Lipofuscin is a photoinducible free radical generator. J. Photochem. Photobiol. B Biol. 1993, 19, 201–204. [Google Scholar] [CrossRef]
- Boulton, M.; Docchio, F.; Dayhaw-Barker, P.; Ramponi, R.; Cubeddu, R. Age-related changes in the morphology, absorption and fluorescence of melanosomes and lipofuscin granules of the retinal pigment epithelium. Vis. Res. 1990, 30, 1291–1303. [Google Scholar] [CrossRef]
- Sarna, T.; Burke, J.M.; Korytowski, W.; Różanowska, M.; Skumatz, C.M.; Zaręba, A.; Zaręba, M. Loss of melanin from human RPE with aging: Possible role of melanin photooxidation. Exp. Eye Res. 2002, 76, 89–98. [Google Scholar] [CrossRef]
- Spaide, R.F. Age-Related Choroidal Atrophy. Am. J. Ophthalmol. 2009, 147, 801–810. [Google Scholar] [CrossRef]
- Zhou, H.; Dai, Y.; Shi, Y.; Russell, J.F.; Lyu, C.; Noorikolouri, J.; Feuer, W.J.; Chu, Z.; Zhang, Q.; de Sisternes, L.; et al. Age-Related Changes in Choroidal Thickness and the Volume of Vessels and Stroma Using Swept-Source OCT and Fully Automated Algorithms. Ophthalmol. Retin. 2019, 4, 204–215. [Google Scholar] [CrossRef]
- Ramrattan, R.S.; van der Schaft, T.L.; Mooy, C.M.; de Bruijn, W.C.; Mulder, P.G.; de Jong, P.T. Morphometric analysis of Bruch’s membrane, the choriocapillaris, and the choroid in aging. Investig. Ophthalmol. Vis. Sci. 1994, 35, 2857–2864. [Google Scholar]
- Nag, T.C. Ultrastructural changes in the melanocytes of aging human choroid. Micron 2015, 79, 16–23. [Google Scholar] [CrossRef]
- Ardeljan, D.; Chan, C.-C. Aging is not a disease: Distinguishing age-related macular degeneration from aging. Prog. Retin. Eye Res. 2013, 37, 68–89. [Google Scholar] [CrossRef] [Green Version]
- Hussain, A.; Starita, C.; Hodgetts, A.; Marshall, J. Macromolecular diffusion characteristics of ageing human Bruch’s membrane: Implications for age-related macular degeneration (AMD). Exp. Eye Res. 2010, 90, 703–710. [Google Scholar] [CrossRef]
- Hussain, A.A.; Rowe, L.; Marshall, J. Age-related alterations in the diffusional transport of amino acids across the human Bruch’s-choroid complex. J. Opt. Soc. Am. A 2002, 19, 166–172. [Google Scholar] [CrossRef]
- Harris, A.; Wirostko, B. Age-related macular degeneration and the aging eye. Clin. Interv. Aging 2008, ume 3, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Nittala, M.G.; Corvi, F.; Maram, J.; Velaga, S.B.; Haines, J.; Pericak-Vance, M.A.; Stambolian, D.; Sadda, S.R. Risk Factors for Progression of Age-Related Macular Degeneration: Population-Based Amish Eye Study. J. Clin. Med. 2022, 11, 5110. [Google Scholar] [CrossRef]
- Kadhim, Z.G.; Mohammad, N.K. Effect of aging and lifestyle on healthy macular photoreceptors and retinal pigment epithelium-Bruch membrane complex thickness. Eur. J. Ophthalmol. 2022, 33, 441–447. [Google Scholar] [CrossRef]
- Ito, Y.N.; Mori, K.; Young-Duvall, J.; Yoneya, S. Aging changes of the choroidal dye filling pattern in indocyanine green angiography of normal subjects. Retina 2001, 21, 237–242. [Google Scholar] [CrossRef]
- Grunwald, J.E.; Hariprasad, S.M.; Dupont, J. Effect of aging on foveolar choroidal circulation. Arch. Ophthalmol. 1998, 116, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Balazsi, A.; Rootman, J.; Drance, S.; Schulzer, M.; Douglas, G. The Effect of Age on the Nerve Fiber Population of the Human Optic Nerve. Am. J. Ophthalmol. 1984, 97, 760–766. [Google Scholar] [CrossRef]
- Moya, F.J.; Brigatti, L.; Caprioli, J. Effect of aging on optic nerve appearance: A longitudinal study. Br. J. Ophthalmol. 1999, 83, 567–572. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.M.; Miao, M.; Sadun, A.A. Age-related decline of human optic nerve axon populations. Age 1987, 10, 5–9. [Google Scholar] [CrossRef]
- Coleman-Belin, J.; Harris, A.; Chen, B.; Zhou, J.; Ciulla, T.; Verticchio, A.; Antman, G.; Chang, M.; Siesky, B. Aging Effects on Optic Nerve Neurodegeneration. Int. J. Mol. Sci. 2023, 24, 2573. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.B.; Lim, M.; Gajjar, A.; Evans, K.B.; Harwerth, R.S. Age-Associated Changes in the Retinal Nerve Fiber Layer and Optic Nerve Head. Investig. Opthalmol. Vis. Sci. 2014, 55, 5134–5143. [Google Scholar] [CrossRef]
- Boehm, A.G.; Koeller, A.U.; Pillunat, L.E. The Effect of Age on Optic Nerve Head Blood Flow. Investig. Opthalmol. Vis. Sci. 2005, 46, 1291–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickens, A.P. Ageing and the free radical theory. Respir. Physiol. 2001, 128, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Hurley, D.J.; Normile, C.; Irnaten, M.; O’Brien, C. The Intertwined Roles of Oxidative Stress and Endoplasmic Reticulum Stress in Glaucoma. Antioxidants 2022, 11, 886. [Google Scholar] [CrossRef]
- Cataract Tables|National Eye Institute. Available online: https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-statistics/cataract-data-and-statistics/cataract-tables (accessed on 18 November 2022).
- Asbell, P.A.; Dualan, I.; Mindel, J.; Brocks, D.; Ahmad, M.; Epstein, S. Age-related cataract. Lancet 2005, 365, 599–609. [Google Scholar] [CrossRef]
- Su, S.-P.; McArthur, J.D.; Truscott, R.J.; Aquilina, J.A. Truncation, cross-linking and interaction of crystallins and intermediate filament proteins in the aging human lens. Biochim. Biophys. Acta 2011, 1814, 647–656. [Google Scholar] [CrossRef]
- Truscott, R.J.; Mizdrak, J.; Friedrich, M.G.; Hooi, M.Y.; Lyons, B.; Jamie, J.; Davies, M.; Wilmarth, P.A.; David, L.L. Is protein methylation in the human lens a result of non-enzymatic methylation by S-adenosylmethionine? Exp. Eye Res. 2012, 99, 48–54. [Google Scholar] [CrossRef] [Green Version]
- Franke, S.; Dawczynski, J.; Strobel, J.; Niwa, T.; Stahl, P.; Stein, G. Increased levels of advanced glycation end products in human cataractous lenses. J. Cataract. Refract. Surg. 2003, 29, 998–1004. [Google Scholar] [CrossRef]
- Tweeddale, H.J.; Hawkins, C.L.; Janmie, J.F.; Truscott, R.J.W.; Davies, M.J. Cross-linking of lens crystallin proteins induced by tryptophan metabolites and metal ions: Implications for cataract development. Free. Radic. Res. 2016, 50, 1116–1130. [Google Scholar] [CrossRef] [PubMed]
- Hooi, M.Y.S.; Truscott, R.J.W. Racemisation and human cataract. d-Ser, d-Asp/Asn and d-Thr are higher in the lifelong proteins of cataract lenses than in age-matched normal lenses. Age 2010, 33, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Hains, P.G.; Truscott, R.J.W. Age-Dependent Deamidation of Lifelong Proteins in the Human Lens. Investig. Opthalmol. Vis. Sci. 2010, 51, 3107–3114. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Estrada, R.; Yappert, M.C.; Borchman, D. Oxidation-induced changes in human lens epithelial cells. Free. Radic. Biol. Med. 2006, 41, 1425–1432. [Google Scholar] [CrossRef]
- Tinaztepe, E.; Ay, M.; Eser, E. Nuclear and Mitochondrial DNA of Age-Related Cataract Patients Are Susceptible to Oxidative Damage. Curr. Eye Res. 2016, 42, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Richardson, R.B.; Ainsbury, E.A.; Prescott, C.R.; Lovicu, F.J. Etiology of posterior subcapsular cataracts based on a review of risk factors including aging, diabetes, and ionizing radiation. Int. J. Radiat. Biol. 2020, 96, 1339–1361. [Google Scholar] [CrossRef]
- Srinivasan, M.; Ravindran, R.D.; O’Brien, K.S.; Kim, U.R.; Wilkins, J.H.; Whitcher, J.P.; Lietman, T.M.; Gritz, D.C.; Keenan, J.D. Antioxidant Vitamins for Cataracts: 15-Year Follow-up of a Randomized Trial. Ophthalmology 2020, 127, 986–987. [Google Scholar] [CrossRef]
- Delamere, N.A.; Tamiya, S. Lens ion transport: From basic concepts to regulation of Na,K-ATPase activity. Exp. Eye Res. 2009, 88, 140–143. [Google Scholar] [CrossRef] [Green Version]
- Tanwar, J.; Singh, J.B.; Motiani, R.K. Molecular machinery regulating mitochondrial calcium levels: The nuts and bolts of mitochondrial calcium dynamics. Mitochondrion 2021, 57, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Brookes, P.; Yoon, Y.; Robotham, J.L.; Anders, M.W.; Sheu, S.-S. Calcium, ATP, and ROS: A mitochondrial love-hate triangle. Am. J. Physiol. Physiol. 2004, 287, C817–C833. [Google Scholar] [CrossRef]
- Tham, Y.-C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Allison, K.; Patel, D.G.; Greene, L. Racial and Ethnic Disparities in Primary Open-Angle Glaucoma Clinical Trials. JAMA Netw. Open 2021, 4, e218348. [Google Scholar] [CrossRef]
- Vajaranant, T.S.; Wu, S.; Torres, M.; Varma, R. The Changing Face of Primary Open-Angle Glaucoma in the United States: Demographic and Geographic Changes from 2011 to 2050. Am. J. Ophthalmol. 2012, 154, 303–314.e3. [Google Scholar] [CrossRef] [Green Version]
- Saccà, S.C.; Gandolfi, S.; Bagnis, A.; Manni, G.; Damonte, G.; Traverso, C.E.; Izzotti, A. From DNA damage to functional changes of the trabecular meshwork in aging and glaucoma. Ageing Res. Rev. 2016, 29, 26–41. [Google Scholar] [CrossRef] [PubMed]
- Recommendation: Primary Open-Angle Glaucoma: Screening|United States Preventive Services Taskforce. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/primary-open-angle-glaucoma-screening (accessed on 18 November 2022).
- Lawler, T.; Liu, Y.; Christensen, K.; Vajaranant, T.S.; Mares, J. Dietary Antioxidants, Macular Pigment, and Glaucomatous Neurodegeneration: A Review of the Evidence. Nutrients 2019, 11, 1002. [Google Scholar] [CrossRef] [Green Version]
- Bourdel-Marchasson, I.; Delmas-Beauvieux, M.; Peuchant, E.; Richard-Harston, S.; Decamps, A.; Reignier, B.; Emeriau, J.; Rainfray, M. Antioxidant defences and oxidative stress markers in erythrocytes and plasma from normally nourished elderly Alzheimer patients. Age Ageing 2001, 30, 235–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, A.; Srivastava, A.; Sihota, R.; Kaur, J. Evaluation of Oxidative Stress Markers in Aqueous Humor of Primary Open Angle Glaucoma and Primary Angle Closure Glaucoma Patients. Curr. Eye Res. 2014, 39, 823–829. [Google Scholar] [CrossRef]
- Ghanem, A.A.; Arafa, L.F.; El-Baz, A. Oxidative Stress Markers in Patients with Primary Open-Angle Glaucoma. Curr. Eye Res. 2010, 35, 295–301. [Google Scholar] [CrossRef]
- Cáceres-Vélez, P.R.; Hui, F.; Hercus, J.; Bui, B.; Jusuf, P.R. Restoring the oxidative balance in age-related diseases—An approach in glaucoma. Ageing Res. Rev. 2022, 75, 101572. [Google Scholar] [CrossRef]
- Sorkhabi, R.; Ghorbanihaghjo, A.; Javadzadeh, A.; Rashtchizadeh, N.; Moharrery, M. Oxidative DNA damage and total antioxidant status in glaucoma patients. Mol. Vis. 2011, 17, 41–46. [Google Scholar] [PubMed]
- Nucci, C.; Di Pierro, D.; Varesi, C.; Ciuffoletti, E.; Russo, R.; Gentile, R.; Cedrone, C.; Duran, M.D.P.; Coletta, M.; Mancino, R. Increased malondialdehyde concentration and reduced total antioxidant capacity in aqueous humor and blood samples from patients with glaucoma. Mol. Vis. 2013, 19, 1841–1846. [Google Scholar] [PubMed]
- Pinazo-Durán, M.D.; Zanón-Moreno, V.; Gallego-Pinazo, R.; García-Medina, J.J. Oxidative stress and mitochondrial failure in the pathogenesis of glaucoma neurodegeneration. Prog. Brain Res. 2015, 220, 127–153. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.N.C.; Loomis, S.J.; Kang, J.H.; Allingham, R.R.; Gharahkhani, P.; Khor, C.C.; Burdon, K.P.; Aschard, H.; Chasman, D.I.; et al.; ANZRAG Consortium Genome-wide association analysis identifies TXNRD2, ATXN2 and FOXC1 as susceptibility loci for primary open-angle glaucoma. Nat. Genet. 2016, 48, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Mills, K.; le Cessie, S.; Noordam, R.; van Heemst, D. Ageing, age-related diseases and oxidative stress: What to do next? Ageing Res. Rev. 2019, 57, 100982. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Pan, X.; Zhao, X.; Luo, J.; Xu, M.; Bai, D.; Hu, Y.; Liu, X.; Yu, Q.; Gao, D. Autophagy and Age-Related Eye Diseases. BioMed Res. Int. 2019, 2019, 5763658. [Google Scholar] [CrossRef]
- Chaudhry, S.; Dunn, H.; Carnt, N.; White, A. Nutritional supplementation in the prevention and treatment of glaucoma. Surv. Ophthalmol. 2021, 67, 1081–1098. [Google Scholar] [CrossRef]
- Klein, R.; Chou, C.-F.; Klein, B.E.K.; Zhang, X.; Meuer, S.M.; Saaddine, J.B. Prevalence of Age-Related Macular Degeneration in the US Population. Arch. Ophthalmol. 2011, 129, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Stahl, A. The Diagnosis and Treatment of Age-Related Macular Degeneration. Dtsch. Ärzteblatt Int. 2020, 117, 513–520. [Google Scholar] [CrossRef]
- Armento, A.; Ueffing, M.; Clark, S.J. The complement system in age-related macular degeneration. Cell. Mol. Life Sci. 2021, 78, 4487–4505. [Google Scholar] [CrossRef]
- van Lookeren Campagne, M.; LeCouter, J.; Yaspan, B.L.; Ye, W. Mechanisms of age-related macular degeneration and therapeutic opportunities. J. Pathol. 2014, 232, 151–164. [Google Scholar] [CrossRef]
- Mitchell, P.; Liew, G.; Gopinath, B.; Wong, T.Y. Age-related macular degeneration. Lancet 2018, 392, 1147–1159. [Google Scholar] [CrossRef] [PubMed]
- Karunadharma, P.P.; Kapphahn, R.J.; Stahl, M.R.; Olsen, T.W.; Ferrington, D.A. Dissecting Regulators of Aging and Age-Related Macular Degeneration in the Retinal Pigment Epithelium. Oxidative Med. Cell. Longev. 2022, 2022, 609787. [Google Scholar] [CrossRef] [PubMed]
- Beatty, S.; Koh, H.-H.; Phil, M.; Henson, D.; Boulton, M. The Role of Oxidative Stress in the Pathogenesis of Age-Related Macular Degeneration. Surv. Ophthalmol. 2000, 45, 115–134. [Google Scholar] [CrossRef] [Green Version]
- Tate, D.J.; Miceli, M.V.; A Newsome, D. Phagocytosis and H2O2 induce catalase and metallothionein gene expression in human retinal pigment epithelial cells. Investig. Opthalmol. Vis. Sci. 1995, 36, 1271–1279. [Google Scholar]
- Delmelle, M. Retinal sensitized photodynamic damage to liposomes. Photochem. Photobiol. 1978, 28, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aal, E.-S.M.; Akhtar, H.; Zaheer, K.; Ali, R. Dietary Sources of Lutein and Zeaxanthin Carotenoids and Their Role in Eye Health. Nutrients 2013, 5, 1169–1185. [Google Scholar] [CrossRef] [Green Version]
- Chew, E.Y.; Clemons, T.E.; Agrón, E.; Domalpally, A.; Keenan, T.D.L.; Vitale, S.; Weber, C.; Smith, D.C.; Christen, W.; et al.; AREDS2 Research Group Long-term Outcomes of Adding Lutein/Zeaxanthin and ω-3 Fatty Acids to the AREDS Supplements on Age-Related Macular Degeneration Progression: AREDS2 Report 28. JAMA Ophthalmol 2022, 140, 692. [Google Scholar] [CrossRef]
- Feng, L.; Nie, K.; Jiang, H.; Fan, W. Effects of lutein supplementation in age-related macular degeneration. PLoS ONE 2019, 14, e0227048. [Google Scholar] [CrossRef] [Green Version]
- García-Layana, A.; Recalde, S.; Hernandez, M.; Abraldes, M.; Nascimento, J.; Hernández-Galilea, E.; Olmedilla-Alonso, B.; Escobar-Barranco, J.; Zapata, M.; Silva, R.; et al. A Randomized Study of Nutritional Supplementation in Patients with Unilateral Wet Age-Related Macular Degeneration. Nutrients 2021, 13, 1253. [Google Scholar] [CrossRef]
- Parravano, M.; Tedeschi, M.; Manca, D.; Costanzo, E.; Di Renzo, A.; Giorno, P.; Barbano, L.; Ziccardi, L.; Varano, M.; Parisi, V. Effects of Macuprev® Supplementation in Age-Related Macular Degeneration: A Double-Blind Randomized Morpho-Functional Study Along 6 Months of Follow-Up. Adv. Ther. 2019, 36, 2493–2505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGwin, G.; Kar, D.; Berlin, A.; Clark, M.E.; Swain, T.A.; Crosson, J.N.; Sloan, K.R.; Owsley, C.; Curcio, C.A. Macular and Plasma Xanthophylls Are Higher in Age-related Macular Degeneration than in Normal Aging: Alabama Study on Early Age-related Macular Degeneration 2 Baseline. Ophthalmol. Sci. 2022, 3, 100263. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, S.G.; Boulton, M.E. Consequences of oxidative stress in age-related macular degeneration. Mol. Asp. Med. 2012, 33, 399–417. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.L.; Lukas, T.J.; Yuan, M.; Neufeld, A.H. Increased mitochondrial DNA damage and down-regulation of DNA repair enzymes in aged rodent retinal pigment epithelium and choroid. Mol. Vis. 2008, 14, 644–651. [Google Scholar] [PubMed]
- Gu, X.; Meer, S.G.; Miyagi, M.; Rayborn, M.E.; Hollyfield, J.G.; Crabb, J.W.; Salomon, R. Carboxyethylpyrrole Protein Adducts and Autoantibodies, Biomarkers for Age-related Macular Degeneration. J. Biol. Chem. 2003, 278, 42027–42035. [Google Scholar] [CrossRef] [Green Version]
- Justilien, V.; Pang, J.-J.; Renganathan, K.; Zhan, X.; Crabb, J.W.; Kim, S.R.; Sparrow, J.R.; Hauswirth, W.W.; Lewin, A.S. SOD2 Knockdown Mouse Model of Early AMD. Investig. Opthalmol. Vis. Sci. 2007, 48, 4407–4420. [Google Scholar] [CrossRef] [Green Version]
- Imamura, Y.; Noda, S.; Hashizume, K.; Shinoda, K.; Yamaguchi, M.; Uchiyama, S.; Shimizu, T.; Mizushima, Y.; Shirasawa, T.; Tsubota, K. Drusen, choroidal neovascularization, and retinal pigment epithelium dysfunction in SOD1-deficient mice: A model of age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2006, 103, 11282–11287. [Google Scholar] [CrossRef] [Green Version]
- Tisi, A.; Feligioni, M.; Passacantando, M.; Ciancaglini, M.; Maccarone, R. The Impact of Oxidative Stress on Blood-Retinal Barrier Physiology in Age-Related Macular Degeneration. Cells 2021, 10, 64. [Google Scholar] [CrossRef]
- Wang, H.; Han, X.; Wittchen, E.S.; Hartnett, M.E. TNF-α mediates choroidal neovascularization by upregulating VEGF expression in RPE through ROS-dependent β-catenin activation. Mol. Vis. 2016, 22, 116–128. Available online: https://pmc/articles/PMC4736754/ (accessed on 11 February 2023).
- Heesterbeek, T.J.; Lechanteur, Y.T.E.; Lorés-Motta, L.; Schick, T.; Daha, M.R.; Altay, L.; Liakopoulos, S.; Smailhodzic, D.; Hollander, A.I.D.; Hoyng, C.B.; et al. Complement Activation Levels Are Related to Disease Stage in AMD. Investig. Opthalmol. Vis. Sci. 2020, 61, 18. [Google Scholar] [CrossRef] [Green Version]
- McLeod, D.S.; Bhutto, I.; Edwards, M.M.; Gedam, M.; Baldeosingh, R.; Lutty, G.A. Mast Cell-Derived Tryptase in Geographic Atrophy. Investig. Opthalmol. Vis. Sci. 2017, 58, 5887–5896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Bhutto, I.; McLeod, D.S.; Jing, T.; Sunness, J.S.; Seddon, J.M.; A Lutty, G. Increased choroidal mast cells and their degranulation in age-related macular degeneration. Br. J. Ophthalmol. 2016, 100, 720–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Endothelium and Descemet’s membranes from normal cornea (a) and cornea in Fuchs’ endothelial corneal dystrophy (FECD) (b) showing structural changes, including guttae formation, modification of the hexagonal endothelial cell mosaic and Descemet’s membrane thickening in FECD. A representative confocal microscopy image of endothelial guttae in an advanced stage of FECD obtained from a patient of the Department of Ophthalmology, Medical University of Warsaw, Warsaw, Poland is shown in part (c) [29].
Figure 1.
Endothelium and Descemet’s membranes from normal cornea (a) and cornea in Fuchs’ endothelial corneal dystrophy (FECD) (b) showing structural changes, including guttae formation, modification of the hexagonal endothelial cell mosaic and Descemet’s membrane thickening in FECD. A representative confocal microscopy image of endothelial guttae in an advanced stage of FECD obtained from a patient of the Department of Ophthalmology, Medical University of Warsaw, Warsaw, Poland is shown in part (c) [29].

Figure 2.
Cataract progression as measured by the Lens Opacities Classification System (LOCS) III grading system [51].
Figure 2.
Cataract progression as measured by the Lens Opacities Classification System (LOCS) III grading system [51].

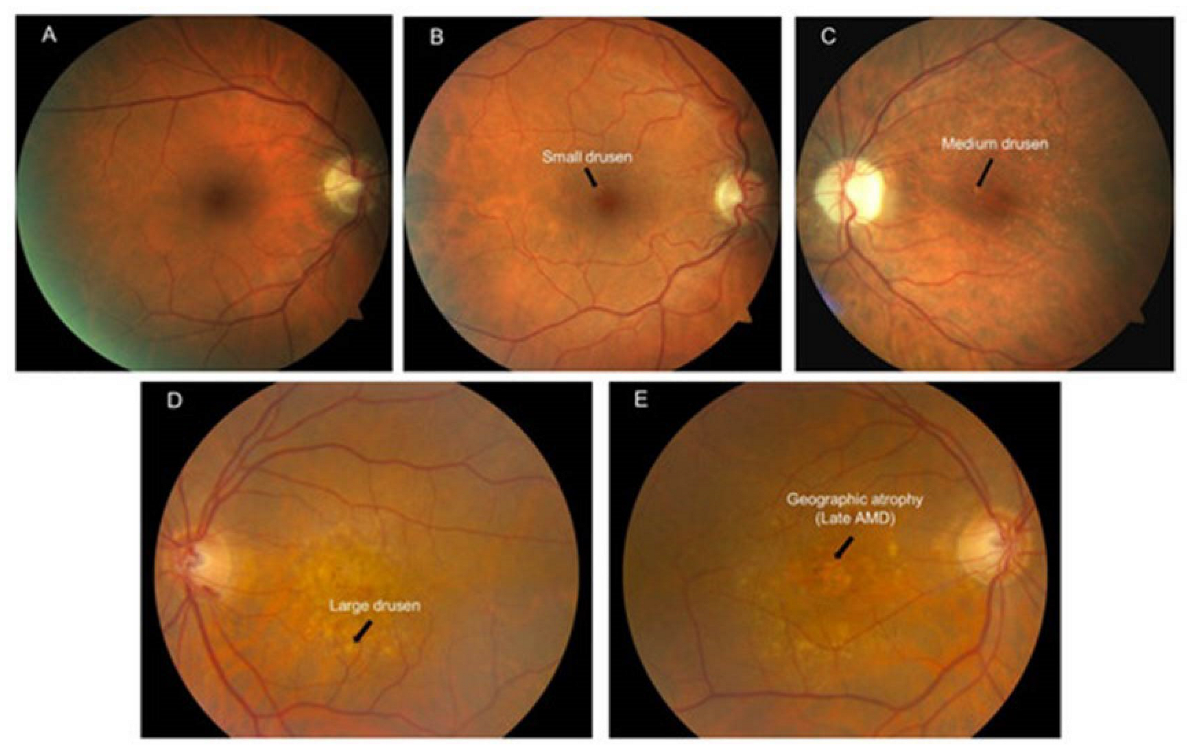
Figure 3.
Illustration of the Beckman’s clinical classification of AMD based on color fundus photos. (A) No apparent aging changes; (B) Normal aging changes; (C) Early AMD; (D) Intermediate AMD; (E) Late AMD as evidenced by geographic atrophy [89].
Figure 3.
Illustration of the Beckman’s clinical classification of AMD based on color fundus photos. (A) No apparent aging changes; (B) Normal aging changes; (C) Early AMD; (D) Intermediate AMD; (E) Late AMD as evidenced by geographic atrophy [89].

Figure 4.
The role of oxidative stress in age-related eye disease [100].
Figure 4.
The role of oxidative stress in age-related eye disease [100].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Current and future prevalence of age-related eye diseases in the United States.
| Disease | 2010 | 2030 | 2050 |
|---|---|---|---|
| Cataracts | 24,409,978 | 38,737,561 | 50,231,932 |
| Glaucoma | 2,719,379 | 4,284,823 | 6,290,760 |
| Age-Related Macular Degeneration | 2,069,403 | 3,664,044 | 5,442,265 |
Source: https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-statistics (accessed on 7 February 2023).
Table 2.
Summary of the age-related changes in the anterior segment of the eye that are discussed in the present work.
Table 2.
Summary of the age-related changes in the anterior segment of the eye that are discussed in the present work.
| Anatomical Feature | Age-Related Changes |
|---|---|
| Eyelids and Lacrimal Glands | Horizontal lid laxity |
| Ectropion | |
| Entropion | |
| Dermatochalasis | |
| Blepharoptosis | |
| Gland atrophy and fibrosis | |
| Sclera | Increase in stiffness and rigidity |
| Senile scleral plaques | |
| Cornea | Thickening of the Descemet’s and epithelial basement membranes |
| Decrease in corneal stromal density | |
| Decrease in corneal endothelial cell (Fuchs’ dystrophy) and conjunctival keratocyte numbers | |
| Shift from with-the-rule astigmatism to against-the-rule astigmatism | |
| Arcus senilis | |
| Cornea farinata | |
| Crocodile shagreen | |
| Phagocytic dysfunction and loss of phagocytically active cells | |
| Trabecular Meshwork | Reduction in height |
| Decrease in cellularity | |
| Increase in extracellular components | |
| Hyperpigmentation | |
| Ciliary Body | Shortening and widening of the muscle |
| Decrease in diameter | |
| Loss of vascularization and cellularity | |
| Crystalline Lens | Increase in radii of curvature, lens volume, surface area, cross-sectional area, diameter, lens thickness, and weight |
| Blue blindness | |
| Cataract formation | |
| Presbyopia secondary to increased stiffness |
Table 3.
Summary of the age-related changes in the posterior segment of the eye that are discussed in the present work.
Table 3.
Summary of the age-related changes in the posterior segment of the eye that are discussed in the present work.
| Anatomical Feature | Age-Related Changes |
|---|---|
| Vitreous Humor | Aggregation of collagenous fibrils |
| Thickening of the vitreous base | |
| Increased stiffness, dehydration, and mobility | |
| Retina and Retinal Pigment Epithelium | Neuronal cell loss |
| Diminished total retinal blood vessel area | |
| Decrease in the number of pericytes and endothelial cells | |
| Retinal pigment epithelium cell vacuolization and loss of cytoplasm | |
| Accumulation of lipofuscin | |
| Impaired melanin antioxidant properties | |
| Choroid | Lower mean thickness, vessel volume, and stroma volume |
| Diminished choriocapillaris density and diameter | |
| Loss of melanosomes within choroidal melanocytes | |
| Macula and Fovea | Increase in macular retinal pigment epithelium cell height |
| Thickening and calcification of Bruch’s membrane | |
| Drusen deposition | |
| Decline in macular vascular flow | |
| Optic Nerve | Reduction in nerve fiber density |
| Lower neural rim volume and minimum rim width | |
| Decreased perfusion of optic nerve head |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Goodman, D.; Ness, S. The Role of Oxidative Stress in the Aging Eye. Life 2023, 13, 837. https://doi.org/10.3390/life13030837
AMA Style
Goodman D, Ness S. The Role of Oxidative Stress in the Aging Eye. Life. 2023; 13(3):837. https://doi.org/10.3390/life13030837
Chicago/Turabian StyleGoodman, Deniz, and Steven Ness. 2023. "The Role of Oxidative Stress in the Aging Eye" Life 13, no. 3: 837. https://doi.org/10.3390/life13030837
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.