
Immunoglobulin G4-Related Disease-Associated Dermatitis with Pruritus: A Positive Response to Dupilumab
 ,
,
Abstract
:1. Introduction
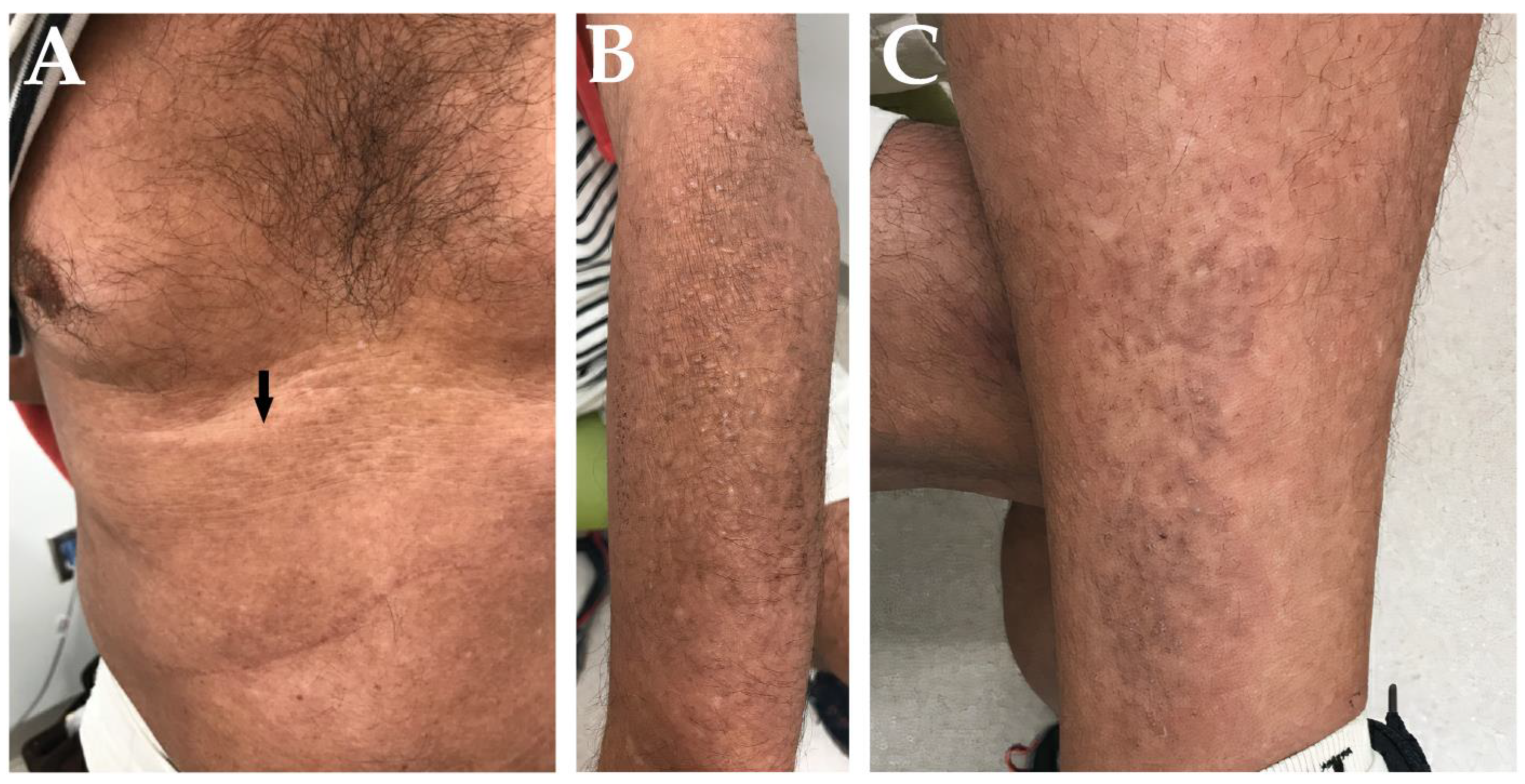
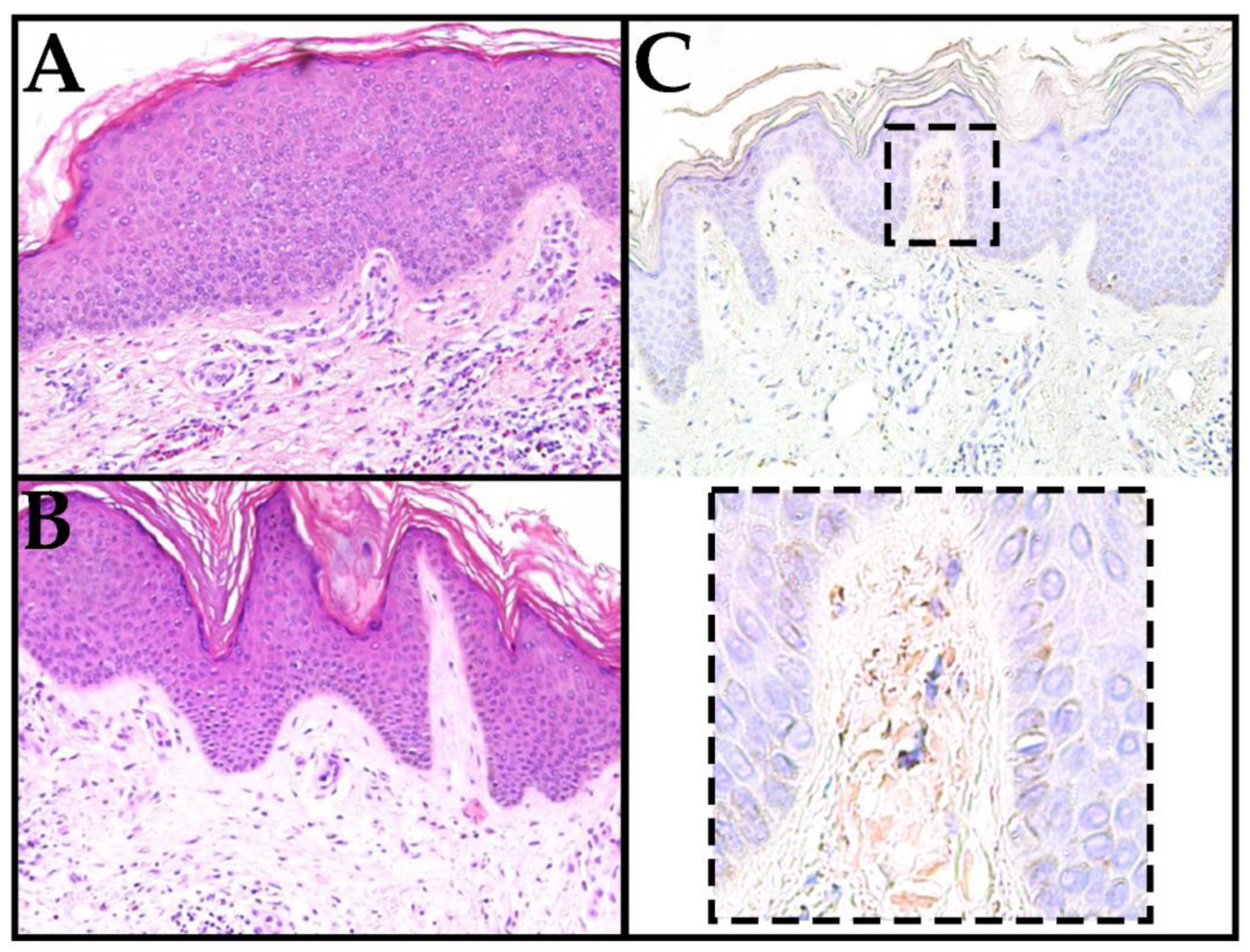
2. Case Report
3. Discussion
4. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| 4/16 | 1/17 | 11/19 | 6/20 | 8/20 | 11/20 | 1/21 | 3/21 | 9/21 | 2/22 | Units | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| BUN | 68 | 61 | 51 | 45 | 79 | 45 | 48 | 41 | 43 | 47 | mg/dL |
| CR | 2.8 | 3.1 | 2.4 | 2.1 | 3.1 | 2.7 | 2.6 | 2.7 | 2.8 | 2.7 | mg/dL |
| eGFR | 23.0 | 20.0 | 27.0 | 32.0 | 20.0 | 23.5 | 24.6 | 23.5 | 22.3 | 23.3 | mL/min/1.73 sqm |
| Bili (Total) | 0.5 | 0.6 | 0.8 | 0.8 | 0.6 | 0.7 | 0.8 | 0.8 | 0.9 | 1.1 | mg/dL |
| AST | 24 | 23 | 27 | 19 | 31 | 21 | 14 | 20 | 21 | 21 | U/L |
| ALT | 35 | 31 | 25 | 24 | 42 | 24 | 17 | 20 | 20 | 20 | U/L |
| ALP | 88 | 84 | 86 | 82 | 69 | 84 | 93 | 81 | 116 | 119 | U/L |
References
- Wisniowski-Yáñez, A.; Zavala-García, G.; Hernández-Molina, G.; González-Duarte, A.; la Mora, J.D.-D.; Ángeles-Ángeles, A.; Martín-Nares, E. Amyloid A amyloidosis secondary to immunoglobulin G4–related disease. Rheumatology 2020, 60, e97–e98. [Google Scholar] [CrossRef] [PubMed]
- Takayama, R.; Ueno, T.; Saeki, H. Immunoglobulin G4-related disease and its skin manifestations. J. Dermatol. 2017, 44, 288–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charrow, A.; Imadojemu, S.; Stephen, S.; Ogunleye, T.; Takeshita, J.; Lipoff, J.B. Cutaneous manifestations of IgG4-related disease (RD): A systematic review. J. Am. Acad. Dermatol. 2016, 75, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, A.; Mohandas, N.; Gottlieb, A. Cutaneous and systemic IgG4-related disease: A review for dermatologists. Dermatol. Online J. 2019, 25, 1. [Google Scholar] [CrossRef]
- Bennett, A.E.; Fenske, N.A.; Rodriguez-Waitkus, P.; Messina, J.L. IgG4-related skin disease may have distinct systemic manifestations: A systematic review. Int. J. Dermatol. 2016, 55, 1184–1195. [Google Scholar] [CrossRef] [PubMed]
- Shirakashi, M.; Yoshifuji, H.; Kodama, Y.; Chiba, T.; Yamamoto, M.; Takahashi, H.; Uchida, K.; Okazaki, K.; Ito, T.; Kawa, S.; et al. Factors in glucocorticoid regimens associated with treatment response and relapses of IgG4-related disease: A multicentre study. Sci. Rep. 2018, 8, 10262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weidner, T.; Illing, T.; Elsner, P. Primary Localized Cutaneous Amyloidosis: A Systematic Treatment Review. Am. J. Clin. Dermatol. 2017, 18, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Kaltoft, B.; Schmidt, G.; Lauritzen, A.F.; Gimsing, P. Primary localised cutaneous amyloidosis--a systematic review. Dan. Med. J. 2013, 60, A4727. [Google Scholar] [PubMed]
- Mehrotra, K. Primary Cutaneous Amyloidosis: A Clinical, Histopathological and Immunofluorescence Study. J. Clin. Diagn. Res. 2017, 11, WC01–WC05. [Google Scholar] [CrossRef] [PubMed]
- Humeda, Y.; Beasley, J.; Calder, K. Clinical resolution of generalized lichen amyloidosis with dupilumab: A new alternative therapy. Dermatol. Online J. 2020, 26, 18. [Google Scholar] [CrossRef]
- Ladizinski, B.; Lee, K.C. Lichen amyloidosis. Can. Med. Assoc. J. 2013, 186, 532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Torre, E.; Mattoo, H.; Mahajan, V.; Carruthers, M.; Pillai, S.; Stone, J.H. Prevalence of atopy, eosinophilia, and IgE elevation in IgG4-related disease. Allergy 2013, 69, 269–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beck, T.C.; Plante, J.; Robinson, I.; Khatskevich, K.; Forcucci, J.A.; Valdebran, M. Immunoglobulin G4-Related Disease-Associated Dermatitis with Pruritus: A Positive Response to Dupilumab. Life 2023, 13, 833. https://doi.org/10.3390/life13030833
Beck TC, Plante J, Robinson I, Khatskevich K, Forcucci JA, Valdebran M. Immunoglobulin G4-Related Disease-Associated Dermatitis with Pruritus: A Positive Response to Dupilumab. Life. 2023; 13(3):833. https://doi.org/10.3390/life13030833
Chicago/Turabian StyleBeck, Tyler C., John Plante, India Robinson, Katsiaryna Khatskevich, Jessica A. Forcucci, and Manuel Valdebran. 2023. "Immunoglobulin G4-Related Disease-Associated Dermatitis with Pruritus: A Positive Response to Dupilumab" Life 13, no. 3: 833. https://doi.org/10.3390/life13030833