

Patterns of Care in Patients with Basilar Artery Occlusion (BAO): A Population-Based Study
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Design
2.2. Patients’ Characteristics and Data Elements
2.3. Statistical Analysis
3. Results
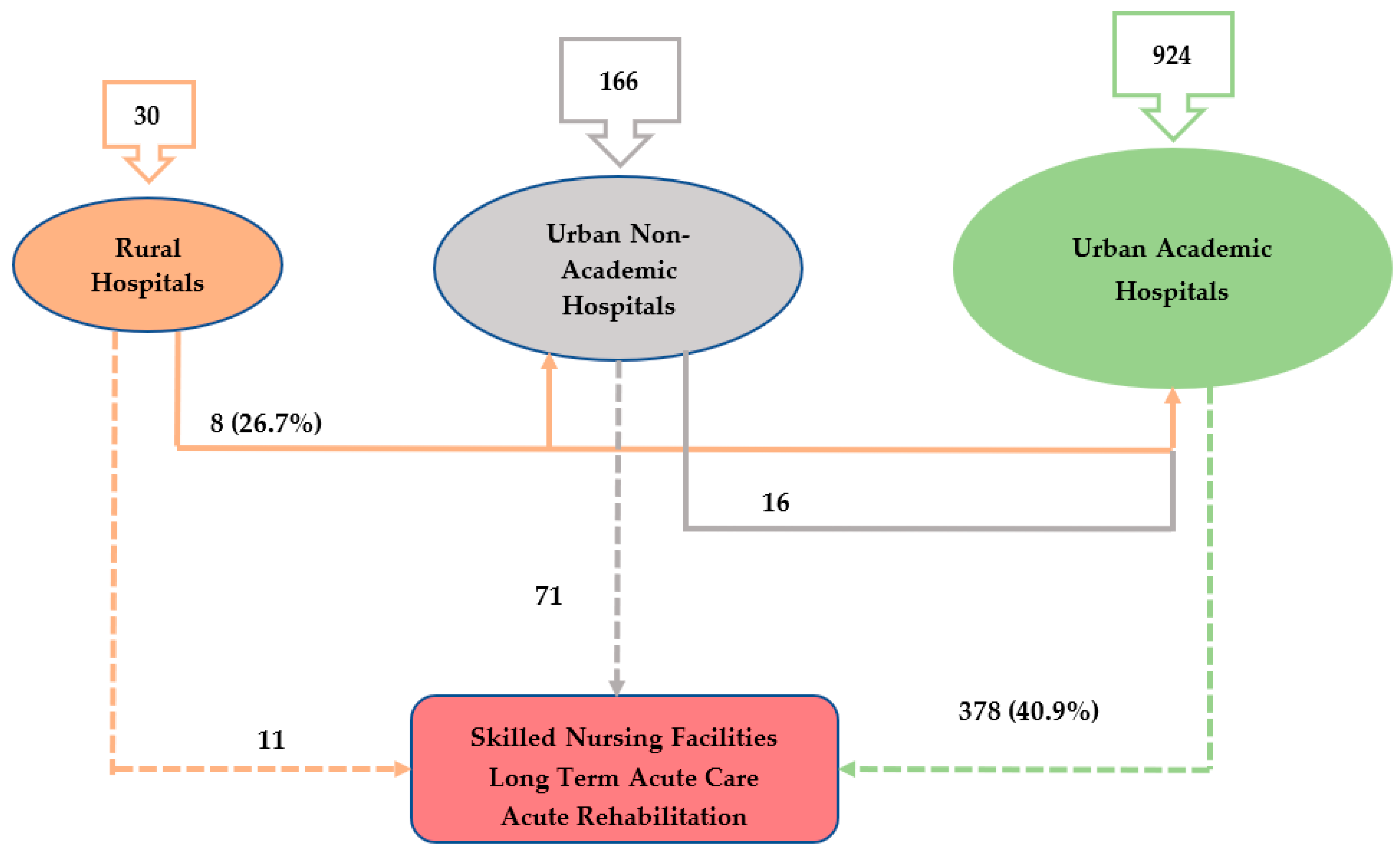
Patient Flow and Hospital Characteristics:
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Ovbiagele, B.; Goldstein, L.B.; Higashida, R.T.; Howard, V.J.; Johnston, S.C.; Khavjou, O.A.; Lackland, D.T.; Lichtman, J.H.; Mohl, S.; Sacco, R.L.; et al. Forecasting the future of stroke in the United States: A policy statement from the American Heart Association and American Stroke Association. Stroke 2013, 44, 2361–2375. [Google Scholar] [CrossRef] [Green Version]
- Mattle, H.P.; Arnold, M.; Lindsberg, P.J.; Schonewille, W.J.; Schroth, G. Basilar artery occlusion. Lancet Neurol. 2011, 10, 1002–1014. [Google Scholar] [CrossRef]
- Schonewille, W.J.; Wijman, C.A.; Michel, P.; Rueckert, C.M.; Weimar, C.; Mattle, H.P.; Engelter, S.T.; Tanne, D.; Muir, K.W.; Molina, C.A.; et al. Treatment and outcomes of acute basilar artery occlusion in the Basilar Artery International Cooperation Study (BASICS): A prospective registry study. Lancet Neurol. 2009, 8, 724–730. [Google Scholar] [CrossRef]
- Liu, X.; Dai, Q.; Ye, R.; Zi, W.; Liu, Y.; Wang, H.; Zhu, W.; Ma, M.; Yin, Q.; Li, M.; et al. Endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion (BEST): An open-label, randomised controlled trial. Lancet Neurol. 2020, 19, 115–122. [Google Scholar] [CrossRef]
- Langezaal, L.C.; van der Hoeven, E.J.; Mont’Alverne, F.J.; de Carvalho, J.J.; Lima, F.O.; Dippel, D.W.; van der Lugt, A.; Lo, R.T.; Boiten, J.; Nijeholt, G.J.L.À.; et al. Endovascular therapy for stroke due to basilar-artery occlusion. N. Engl. J. Med. 2021, 384, 1910–1920. [Google Scholar] [CrossRef]
- National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue Plasminogen Activator for Acute Ischemic Stroke. N. Engl. J. Med. 1995, 333, 1581–1588. [Google Scholar] [CrossRef]
- Pagola, J.; Ribo, M.; Alvarez-Sabin, J.; Rubiera, M.; Santamarina, E.; Maisterra, O.; Delgado-Mederos, R.; Ortega, G.; Quintana, M.; Molina, C.A. Thrombolysis in anterior versus posterior circulation strokes: Timing of recanalization, ischemic tolerance, and other differences. J. Neuroimaging 2011, 21, 108–112. [Google Scholar] [CrossRef]
- Kumar, G.; Shahripour, R.B.; Alexandrov, A.V. Recanalization of acute basilar artery occlusion improves outcomes: A meta-analysis. J. Neurointerventional Surg. 2015, 7, 868–874. [Google Scholar] [CrossRef]
- Saver, J.L.; Fonarow, G.; Smith, E.; Reeves, M.J.; Grau-Sepulveda, M.V.; Pan, W.; Olson, D.; Hernandez, A.F.; Peterson, E.D.; Schwamm, L. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA 2013, 309, 2480–2488. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; Van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; Van Der Lugt, A.; De Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Sarraj, A.; Pujara, D.; Grotta, J.C. Endovascular thrombectomy for acute ischemic strokes: Current US access paradigms and optimization methodology. Stroke 2020, 51, 1207–1217. [Google Scholar] [CrossRef]
- Rinaldo, L.; Brinjikji, W.; A McCutcheon, B.; Bydon, M.; Cloft, H.; Kallmes, D.F.; A Rabinstein, A. Hospital transfer associated with increased mortality after endovascular revascularization for acute ischemic stroke. J. Neurointerv. Surg. 2017, 9, 1166–1172. [Google Scholar] [CrossRef]
- Froehler, M.T.; Saver, J.L.; Zaidat, O.O.; Jahan, R.; Aziz-Sultan, M.A.; Klucznik, R.P.; Haussen, D.C.; Hellinger, F.R.; Yavagal, D.R.; Yao, T.L.; et al. Interhospital transfer before thrombectomy is associated with delayed treatment and worse outcome in the STRATIS registry (systematic evaluation of patients treated with neurothrombectomy devices for acute ischemic stroke). Circulation 2017, 136, 2311–2321. [Google Scholar] [CrossRef]
- Leira, E.C.; Hess, D.C.; Torner, J.C.; Adams, H.P. Rural-urban differences in acute stroke management practices: A modifiable disparity. Arch. Neurol. 2008, 65, 887–891. [Google Scholar] [CrossRef] [Green Version]
- Gonzales, S.; Mullen, M.T.; Skolarus, L.; Thibault, D.P.; Udoeyo, U.; Willis, A.W. Progressive rural–urban disparity in acute stroke care. Neurology 2017, 88, 441–448. [Google Scholar] [CrossRef] [Green Version]
- The Agency for Healthcare Research and Quality. HCUP Nationwide Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). 2007. Available online: https://www.hcup-us.ahrq.gov/db/nation/nis/NIS_2007_INTRODUCTION.pdf (accessed on 5 July 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Adeoye, O.; Albright, K.C.; Carr, B.G.; Wolff, C.; Mullen, M.T.; Abruzzo, T.; Ringer, A.; Khatri, P.; Branas, C.; Kleindorfer, D. Geographic access to acute stroke care in the United States. Stroke 2014, 45, 3019–3024. [Google Scholar] [CrossRef] [Green Version]
- Wei, D.; Oxley, T.; Nistal, D.A.; Mascitelli, J.R.; Wilson, N.; Stein, L.; Liang, J.W.; Turkheimer, L.M.; Morey, J.; Schwegel, C.; et al. Mobile interventional stroke teams lead to faster treatment times for thrombectomy in large vessel occlusion. Stroke 2017, 48, 3295–3300. [Google Scholar] [CrossRef]
- Broocks, G.; Groffmann, M.; Meyer, L.; Elsayed, S.; Kniep, H.; Kemmling, A.; van Horn, N.; McDonough, R.; Faizy, T.D.; Bechstein, M.; et al. Higher baseline blood glucose is associated with reduced likelihood for successful recanalization in patients with basilar artery occlusion. J. Neurol. 2022, 269, 3286–3294. [Google Scholar] [CrossRef]
- Yue, F.; Wang, Z.; Pu, J.; Zhang, M.; Liu, Y.; Han, H.; Liu, W.; Wang, X.; Li, R.; Xue, D.; et al. HbA1c and clinical outcomes after endovascular treatment in patients with posterior circulation large vessel occlusion: A subgroup analysis of a nationwide registry (BASILAR). Ther. Adv. Neurol. Disord. 2020, 13, 1756286420981354. [Google Scholar] [CrossRef]
- Kang, D.; Jung, C.; Yoon, W.; Kim, S.K.; Baek, B.H.; Kim, J.; Park, M.S.; Kim, Y.W.; Hwang, Y.H.; Kim, B.J.; et al. Endovascular thrombectomy for acute basilar artery occlusion: A multicenter retrospective observational study. J. Am. Heart Assoc. 2018, 7, e009419. [Google Scholar] [CrossRef]
- Cao, J.; Mo, Y.; Chen, R.; Shao, H.; Xuan, J.; Peng, Y.; Zhu, X. Predictors of functional outcome and mortality in endovascular treatment for acute basilar artery occlusion: A single-centre experience. Front. Neurol. 2021, 12, 1823. [Google Scholar] [CrossRef]
- Lindsberg, P.J.; Sairanen, T.; Nagel, S.; Salonen, O.; Silvennoinen, H.; Strbian, D. Recanalization treatments in basilar artery occlusion—Systematic analysis. Eur. Stroke J. 2016, 1, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Nagel, S.; Schellinger, P.D.; Hartmann, M.; Juettler, E.; Huttner, H.B.; Ringleb, P.; Schwab, S.; Köhrmann, M. Therapy of acute basilar artery occlusion: Intraarterial thrombolysis alone vs bridging therapy. Stroke 2009, 40, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.; Jung, C.; Bae, Y.J.; Choi, B.S.; Kim, J.H.; Lee, S.H.; Chang, J.Y.; Kim, B.J.; Han, M.K.; Bae, H.J.; et al. A comparison between mechanical thrombectomy and intra-arterial fibrinolysis in acute basilar artery occlusion: Single center experiences. J. Stroke 2016, 18, 211. [Google Scholar] [CrossRef] [Green Version]
- Schulte-Altedorneburg, G.; Hamann, G.; Mull, M.; Kühne, D.; Liebetrau, M.; Weber, W.; Brückmann, H.; Mayer, T. Outcome of acute vertebrobasilar occlusions treated with intra-arterial fibrinolysis in 180 patients. Am. J. Neuroradiol. 2006, 27, 2042–2047. [Google Scholar] [PubMed]
- Sonig, A.; Lin, N.; Krishna, C.; Natarajan, S.K.; Mokin, M.; Hopkins, L.N.; Snyder, K.V.; Levy, E.I.; Siddiqui, A.H. Impact of transfer status on hospitalization cost and discharge disposition for acute ischemic stroke across the US. J. Neurosurg. 2016, 124, 1228–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; Berg, L.A.V.D.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; De Miquel, M.A.; Molina, C.A.; Rovira, A.; Román, L.S.; Serena, J.; Abilleira, S.; Ribo, M.; et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.-C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef]
- Writing Group for the BASILAR Group; Zi, W.; Qiu, Z.; Wu, D.; Li, F.; Liu, H.; Liu, W.; Huang, W.; Shi, Z.; Bai, Y.; et al. Assessment of endovascular treatment for acute basilar artery occlusion via a nationwide prospective registry. JAMA Neurol. 2020, 77, 561–573. [Google Scholar] [PubMed]
- Tao, C.; Qureshi, A.I.; Yin, Y.; Li, J.; Li, R.; Xu, P.; Sun, J.; Liao, G.; Yue, X.; Shi, H.; et al. Endovascular Treatment Versus Best Medical Management in Acute Basilar Artery Occlusion Strokes: Results From the ATTENTION Multicenter Registry. Circulation 2022, 146, 6–17. [Google Scholar] [CrossRef]
- Nguyen, T.N.; Strbian, D. Endovascular therapy for stroke due to basilar artery occlusion: A BASIC challenge at BEST. Stroke 2021, 52, 3410–3413. [Google Scholar] [CrossRef] [PubMed]
- Jovin, T.G.; Li, C.; Wu, L.; Wu, C.; Chen, J.; Jiang, C.; Shi, Z.; Gao, Z.; Song, C.; Chen, W.; et al. Trial of thrombectomy 6 to 24 hours after stroke due to basilar-artery occlusion. N. Engl. J. Med. 2022, 387, 1373–1384. [Google Scholar] [CrossRef]
- Tao, C.; Nogueira, R.G.; Zhu, Y.; Sun, J.; Han, H.; Yuan, G.; Wen, C.; Zhou, P.; Chen, W.; Zeng, G.; et al. Trial of endovascular treatment of acute basilar-artery occlusion. N. Engl. J. Med. 2022, 387, 1361–1372. [Google Scholar] [CrossRef]
- Alberts, M.J.; Range, J.; Spencer, W.; Cantwell, V.; Hampel, M.J. Availability of endovascular therapies for cerebrovascular disease at primary stroke centers. Interv. Neuroradiol. 2017, 23, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Pérez de la Ossa, N.; Carrera, D.; Gorchs, M.; Querol, M.; Millán, M.; Gomis, M.; Dorado, L.; López-Cancio, E.; Hernández-Pérez, M.; Chicharro, V.; et al. Design and validation of a prehospital stroke scale to predict large arterial occlusion: The rapid arterial occlusion evaluation scale. Stroke 2014, 45, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Nazliel, B.; Starkman, S.; Liebeskind, D.S.; Ovbiagele, B.; Kim, D.; Sanossian, N.; Ali, L.; Buck, B.; Villablanca, P.; Vinuela, F.; et al. A brief prehospital stroke severity scale identifies ischemic stroke patients harboring persisting large arterial occlusions. Stroke 2008, 39, 2264–2267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, B.S.; McMullan, J.T.; Sucharew, H.; Adeoye, O.; Broderick, J.P. Design and validation of a prehospital scale to predict stroke severity: Cincinnati Prehospital Stroke Severity Scale. Stroke 2015, 46, 1508–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hastrup, S.; Damgaard, D.; Johnsen, S.P.; Andersen, G. Prehospital acute stroke severity scale to predict large artery occlusion: Design and comparison with other scales. Stroke 2016, 47, 1772–1776. [Google Scholar] [CrossRef] [Green Version]
- Taqi, M.A.; Sodhi, A.; Suriya, S.S.; Quadri, S.A.; Farooqui, M.; Salvucci, A.A.; Stefansen, A.; Mortazavi, M.M.; Shepherd, D. Design, application and infield validation of a pre-hospital emergent large vessel occlusion screening tool: Ventura emergent large vessel occlusion score. J. Stroke Cerebrovasc. Dis. 2019, 28, 728–734. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | EVT | Non-EVT | p-Value | |
|---|---|---|---|---|
| n (% ) | n (% ) | n (% ) | ||
| 1120 (100) | 184 (16.43) | 936 (83.57) | ||
| Demographics | ||||
| Gender | 0.6804 | |||
| Male | 672 (60.05) | 113 (61.41) | 559 (59.79) | |
| Female | 447 (39.95) | 71 (38.59) | 376 (40.21) | |
| Age, mean ± SD | 65.99 ± 14.69 | 64.74 ± 16.68 | 66.24 ± 15.32 | 0.2057 |
| Race | 0.0474 | |||
| White | 662 (59.11) | 123 (66.85) | 539 (57.59) | |
| Black | 185 (16.52) | 19 (10.33) | 166 (17.74) | |
| Hispanic | 85 (7.59) | 15 (8.15) | 70 (7.48) | |
| Others | 92 (8.21) | 10 (5.43) | 82 (8.76) | |
| Unknown | 96 (8.57) | 17 (9.24) | 79 (8.44) | |
| Vascular Risk Factors (Comorbidities) | ||||
| Diabetes | 0.0519 | |||
| Yes | 429 (38.30) | 59 (32.07) | 370 (39.53) | |
| No | 691 (61.70) | 125 (67.93) | 566 (60.47) | |
| Hypertension | 0.1671 | |||
| Yes | 894 (79.82) | 140 (76.09) | 754 (80.56) | |
| No | 226 (20.18) | 44 (23.91) | 182 (19.44) | |
| Atrial fibrillation | <0.0001 | |||
| Yes | 219 (19.55) | 58 (31.52) | 161 (17.20) | |
| No | 901 (80.45) | 126 (68.48) | 775 (82.80) | |
| Congestive heart failure | 0.3829 | |||
| Yes | 114 (10.18) | 22 (11.96) | 92 (9.83) | |
| No | 1006 (89.82) | 162 (88.40) | 844 (90.17) | |
| Peripheral vascular disorders | ||||
| Yes | 167 (14.91) | 39 (21.20) | 128 (13.68) | 0.0088 |
| No | 953 (85.09) | 145 (78.80) | 808 (86.32) | |
| Coagulopathy | 0.12 | |||
| Yes | 59 (5.27) | 14 (7.61) | 45 (4.81) | |
| No | 1061 (94.73) | 170 (92.39) | 891 (95.19) | |
| Obstructive sleep apnea | 0.153 | |||
| Yes | 61 (5.45) | 6 (3.26) | 55 (5.88) | |
| No | 1059 (94.55) | 178 (96.74) | 881 (94.12) | |
| Social Risk Factors | ||||
| Alcohol | 0.3088 | |||
| Yes | 67 (5.98) | 14 (7.61) | 53 (5.66) | |
| No | 1053 (94.02) | 170 (92.39) | 883 (94.34) | |
| Tobacco exposure | 0.5887 | |||
| Yes | 223 (20.80) | 41 (22.28) | 192 (20.51) | |
| No | 887 (79.20) | 143 (77.72) | 744 (79.49) | |
| Drug Abuse | ||||
| Yes | 59 (5.27) | 6 (3.26) | 53 (5.66) | 0.1825 |
| No | 1061 (94.73) | 178 (96.74) | 883 (94.34) | |
| Location/teaching status of hospital | 0.0091 | |||
| Rural | ||||
| Urban /non-teaching | 30 (2.68) | 0 (0.00) | 30 (3.21) | |
| Urban/teaching | 166 (14.82) | 20 (10.87) | 146 (15.60) | |
| 924 (82.50) | 164 (89.13) | 760 (81.20) | ||
| Died during hospitalization | <0.0001 | |||
| Yes | 256 (22.86) | 65 (35.33) | 191 (20.41) | |
| No | 864 (77.14) | 119 (64.67) | 745 (79.59) | |
| Percutaneous endoscopic gastrostomy | <0.0001 | |||
| (PEG) tube placement | ||||
| Yes | 109 (9.73) | 36 (19.57) | 73 (7.80) | |
| No | 1011 (90.27) | 148 (80.43) | 863 (92.20) | |
| Tracheotomy procedure | <0.0001 | |||
| Yes | 73 (6.52) | 29 (15.76) | 44 (4.70) | |
| No | 1047 (93.48) | 155 (84.24) | 892 (95.30) |
| Disposition Other than Home | Length of Stay | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| Age | 1.033 | 0.256–1.058 | 0.462 | 1.45 | −0.85–2.058 | 0.62 |
| Sex | 0.520 | 0.169–1.600 | 0.254 | 1.21 | 0.45–1.75 | 0.31 |
| Cost | 0.45 | −2.45–1.43 | 0.598 | 1.67 | 0.76–3.87 | 0.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farooqui, M.; Ikram, A.; Suriya, S.; Qeadan, F.; Bzdyra, P.; Quadri, S.A.; Zafar, A. Patterns of Care in Patients with Basilar Artery Occlusion (BAO): A Population-Based Study. Life 2023, 13, 829. https://doi.org/10.3390/life13030829
Farooqui M, Ikram A, Suriya S, Qeadan F, Bzdyra P, Quadri SA, Zafar A. Patterns of Care in Patients with Basilar Artery Occlusion (BAO): A Population-Based Study. Life. 2023; 13(3):829. https://doi.org/10.3390/life13030829
Chicago/Turabian StyleFarooqui, Mudassir, Asad Ikram, Sajid Suriya, Fares Qeadan, Piotr Bzdyra, Syed A. Quadri, and Atif Zafar. 2023. "Patterns of Care in Patients with Basilar Artery Occlusion (BAO): A Population-Based Study" Life 13, no. 3: 829. https://doi.org/10.3390/life13030829