
Tension-Type Headache in Children and Adolescents
 ,
,
Abstract
:1. Introduction
2. Epidemiology
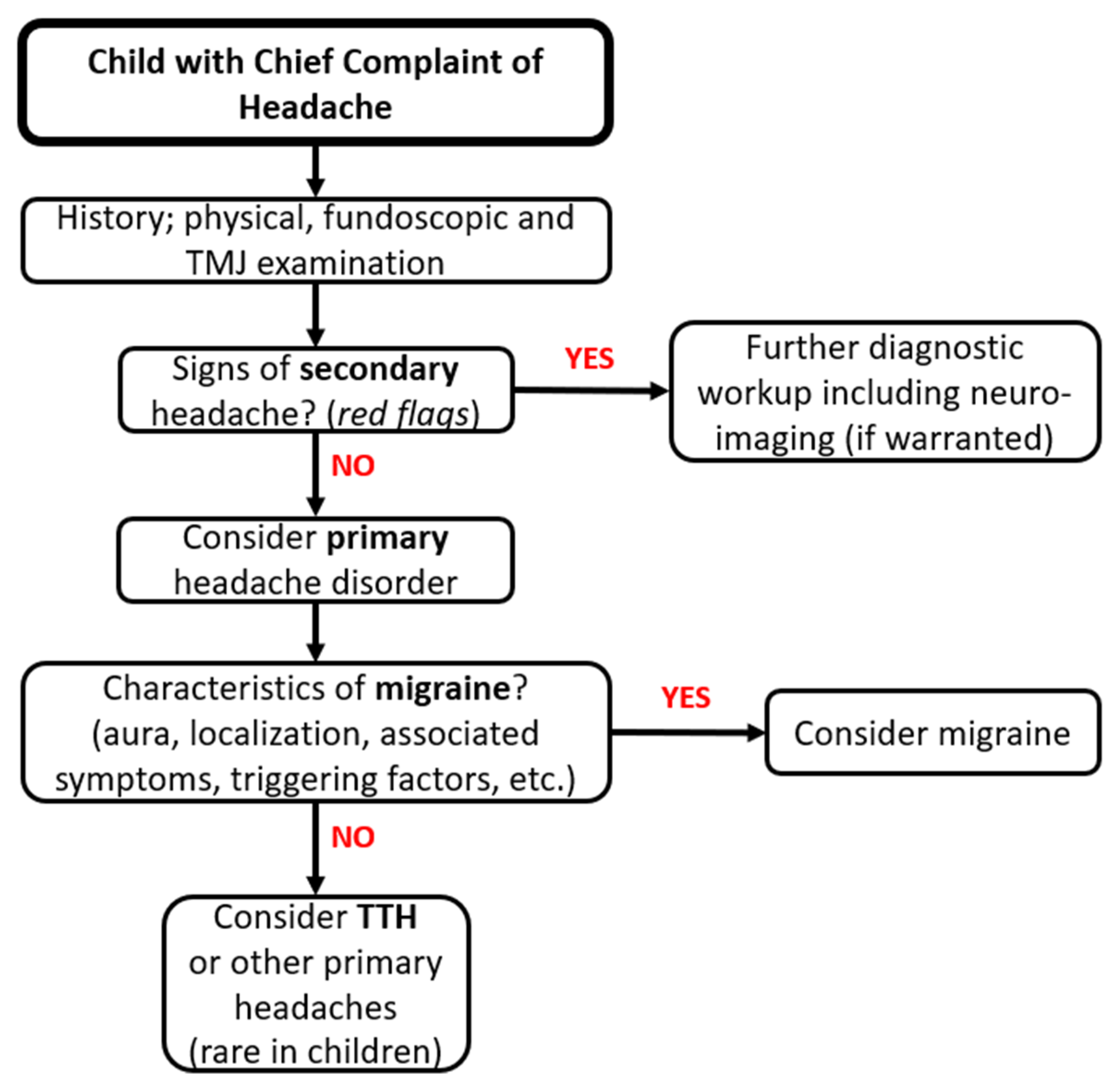
3. Differential Diagnosis
- -
- Severe and sudden onset headache.
- -
- Very early onset of headache (i.e., in preschool age), especially considering that brain tumors are relatively more common in younger children than in older ones, while primary headaches are less common.
- -
- Focal neurological signs (e.g., ataxia or cognitive impairment), papilledema or other clinical signs suggestive of raised intracranial pressure (e.g., early morning headache, vomiting in the morning, pain disturbing sleep and headache worsened by cough or Valsalva) [26].
- -
- Atypical presentations, which should lead clinicians to suspect secondary headaches or other rarer primary headaches (e.g., cluster headaches, SUNCT, co-existing different forms of primary headaches) [29].
- -
- Headache awakening the child from sleep or consistently occurring first thing in the morning, especially if refractory to usual acute treatment. In these cases, screening for hypertension, obstructive sleep apneas, sleep bruxism or other sleep or general health conditions should also be considered [29].
- -
- Accelerated course, change in characteristics over weeks or days.
- -
- Post-traumatic headache [26].
- -
- Headache associated with personality or behavior changes.
- -
- Underlying history of neurocutaneous syndromes, systemic illness (e.g., known malignancy with possible metastases, hypercoagulopathy) or drugs or toxic substances exposure.
- -
- Headache associated with malaise and fever, which could be due to an infection. In these cases, the physical examination should include maneuvers that investigate meningeal inflammation (neck stiffness, Brudzinski and Kernig signs). However, in most cases, headache with fever is due to infections of the upper respiratory tract, such as sinusitis, based on incidental radiological findings [30,31].
4. Psychopathology Features and Developmental Pathways
5. Developmental Trajectories in Children and Adolescents
6. Treatment Strategies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swain, M.S.; Henschke, N.; Kamper, S.J.; Gobina, I.; Ottová-Jordan, V.; Maher, C.G. An International Survey of Pain in Adolescents. BMC Public Health 2014, 14, 447. [Google Scholar] [CrossRef] [Green Version]
- Obermeier, V.; Murawski, M.; Heinen, F.; Landgraf, M.N.; Straube, A.; von Kries, R.; Ruscheweyh, R. Total Health Insurance Costs in Children with a Migraine Diagnosis Compared to a Control Group. J. Headache Pain 2021, 22, 140. [Google Scholar] [CrossRef] [PubMed]
- Guidetti, V.; Galli, F.; Fabrizi, P.; Giannantoni, A.S.; Napoli, L.; Bruni, O.; Trillo, S. Headache and Psychiatric Comorbidity: Clinical Aspects and Outcome in an 8-Year Follow-up Study. Cephalalgia Int. J. Headache 1998, 18, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Wöber, C.; Wöber-Bingöl, C. Clinical Management of Young Patients Presenting with Headache. Funct. Neurol. 2000, 15 (Suppl. S3), 89–105. [Google Scholar] [PubMed]
- Antonaci, F.; Voiticovschi-Iosob, C.; Di Stefano, A.L.; Galli, F.; Ozge, A.; Balottin, U. The Evolution of Headache from Childhood to Adulthood: A Review of the Literature. J. Headache Pain 2014, 15, 15. [Google Scholar] [CrossRef] [Green Version]
- Mier, R.W.; Dhadwal, S. Primary Headaches. Dent. Clin. N. Am. 2018, 62, 611–628. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd Edition (Beta Version). Cephalalgia Int. J. Headache 2013, 33, 629–808. [Google Scholar] [CrossRef] [Green Version]
- Deuschl, G.; Beghi, E.; Fazekas, F.; Varga, T.; Christoforidi, K.A.; Sipido, E.; Bassetti, C.L.; Vos, T.; Feigin, V.L. The Burden of Neurological Diseases in Europe: An Analysis for the Global Burden of Disease Study 2017. Lancet Public Health 2020, 5, e551–e567. [Google Scholar] [CrossRef]
- Ashina, S.; Mitsikostas, D.D.; Lee, M.J.; Yamani, N.; Wang, S.-J.; Messina, R.; Ashina, H.; Buse, D.C.; Pozo-Rosich, P.; Jensen, R.H.; et al. Tension-Type Headache. Nat. Rev. Dis. Primer 2021, 7, 24. [Google Scholar] [CrossRef]
- Genc, D.; Vaičienė-Magistris, N.; Zaborskis, A.; Şaşmaz, T.; Tunç, A.Y.; Uluduz, D.; Wöber, C.; Wöber-Bingöl, Ç.; Steiner, T.J. The Burden Attributable to Headache Disorders in Children and Adolescents in Lithuania: Estimates from a National Schools-Based Study. J. Headache Pain 2021, 22, 24. [Google Scholar] [CrossRef]
- Steiner, T.J.; Stovner, L.J.; Birbeck, G.L. Migraine: The Seventh Disabler. Headache J. Head Face Pain 2013, 53, 227–229. [Google Scholar] [CrossRef] [Green Version]
- Pacheva, I.; Milanov, I.; Ivanov, I.; Stefanov, R. Evaluation of Diagnostic and Prognostic Value of Clinical Characteristics of Migraine and Tension Type Headache Included in the Diagnostic Criteria for Children and Adolescents in International Classification of Headache Disorders—Second Edition. Int. J. Clin. Pract. 2012, 66, 1168–1177. [Google Scholar] [CrossRef]
- Onofri, A.; Pensato, U.; Rosignoli, C.; Wells-Gatnik, W.; Stanyer, E.; Ornello, R.; Chen, H.Z.; De Santis, F.; Torrente, A.; Mikulenka, P.; et al. Primary Headache Epidemiology in Children and Adolescents: A Systematic Review and Meta-Analysis. J. Headache Pain 2023, 24, 8. [Google Scholar] [CrossRef] [PubMed]
- Wilkes, M.J.; Mendis, M.D.; Bisset, L.; Leung, F.T.; Sexton, C.T.; Hides, J.A. The Prevalence and Burden of Recurrent Headache in Australian Adolescents: Findings from the Longitudinal Study of Australian Children. J. Headache Pain 2021, 22, 49. [Google Scholar] [CrossRef]
- Wöber-Bingöl, Ç. Epidemiology of Migraine and Headache in Children and Adolescents. Curr. Pain Headache Rep. 2013, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Balottin, U.; Termine, C.; Nicoli, F.; Quadrelli, M.; Ferrari-Ginevra, O.; Lanzi, G. Idiopathic Headache in Children under Six Years of Age: A Follow-up Study. Headache 2005, 45, 705–715. [Google Scholar] [CrossRef]
- Casucci, G.; Terlizzi, R.; Cevoli, S. Headache in School Age. Neurol. Sci. 2014, 35, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Anttila, P.; Metsähonkala, L.; Aromaa, M.; Sourander, A.; Salminen, J.; Helenius, H.; Alanen, P.; Sillanpää, M. Determinants of Tension-Type Headache in Children. Cephalalgia 2002, 22, 401–408. [Google Scholar] [CrossRef]
- Wöber-Bingöl, Ç.; Wöber, C.; Uluduz, D.; Uygunoğlu, U.; Aslan, T.S.; Kernmayer, M.; Zesch, H.-E.; Gerges, N.T.; Wagner, G.; Siva, A.; et al. The Global Burden of Headache in Children and Adolescents—Developing a Questionnaire and Methodology for a Global Study. J. Headache Pain 2014, 15, 86. [Google Scholar] [CrossRef] [Green Version]
- Parisi, P.; Papetti, L.; Spalice, A.; Nicita, F.; Ursitti, F.; Villa, M.P. Tension-Type Headache in Paediatric Age. Acta Paediatr. 2011, 100, 491–495. [Google Scholar] [CrossRef]
- Zewde, Y.Z.; Zebenigus, M.; Demissie, H.; Tekle-Haimanot, R.; Uluduz, D.; Şaşmaz, T.; Bozdag, F.; Steiner, T.J. The Prevalence of Headache Disorders in Children and Adolescents in Ethiopia: A Schools-Based Study. J. Headache Pain 2020, 21, 108. [Google Scholar] [CrossRef]
- Kawatu, N.; Wa Somwe, S.; Ciccone, O.; Mukanzu, M.; Uluduz, D.; Şaşmaz, T.; Yalçın, B.N.B.; Wöber, C.; Steiner, T.J. The Prevalence of Primary Headache Disorders in Children and Adolescents in Zambia: A Schools-Based Study. J. Headache Pain 2022, 23, 118. [Google Scholar] [CrossRef]
- Battistella, P.A.; Fiumana, E.; Binelli, M.; Bertossi, E.; Battista, P.; Perakis, E.; Soriani, S. Primary Headaches in Preschool Age Children: Clinical Study and Follow-up in 163 Patients. Cephalalgia Int. J. Headache 2006, 26, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Özge, A.; Faedda, N.; Abu-Arafeh, I.; Gelfand, A.A.; Goadsby, P.J.; Cuvellier, J.C.; Valeriani, M.; Sergeev, A.; Barlow, K.; Uludüz, D.; et al. Experts’ Opinion about the Primary Headache Diagnostic Criteria of the ICHD-3rd Edition Beta in Children and Adolescents. J. Headache Pain 2017, 18, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seshia, S.S.; Abu-Arafeh, I.; Hershey, A.D. Tension-Type Headache in Children: The Cinderella of Headache Disorders! Can. J. Neurol. Sci. 2009, 36, 687–695. [Google Scholar] [CrossRef] [Green Version]
- Papetti, L.; Spalice, A.; Nicita, F.; Paolino, M.C.; Castaldo, R.; Iannetti, P.; Villa, M.P.; Parisi, P. Migraine Treatment in Developmental Age: Guidelines Update. J. Headache Pain 2010, 11, 267–276. [Google Scholar] [CrossRef] [Green Version]
- Lewis, D.W.; Ashwal, S.; Dahl, G.; Dorbad, D.; Hirtz, D.; Prensky, A.; Jarjour, I. Practice Parameter: Evaluation of Children and Adolescents with Recurrent Headaches: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2002, 59, 490–498. [Google Scholar] [CrossRef] [Green Version]
- Do, T.P.; Remmers, A.; Schytz, H.W.; Schankin, C.; Nelson, S.E.; Obermann, M.; Hansen, J.M.; Sinclair, A.J.; Gantenbein, A.R.; Schoonman, G.G. Red and Orange Flags for Secondary Headaches in Clinical Practice: SNNOOP10 List. Neurology 2019, 92, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Dooley, J. The Evaluation and Management of Paediatric Headaches. Paediatr. Child Health 2009, 14, 24–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Şenbil, N.; Gürer, Y.K.Y.; Üner, Ç.; Barut, Y. Sinusitis in Children and Adolescents with Chronic or Recurrent Headache: A Case–Control Study. J. Headache Pain 2008, 9, 33–36. [Google Scholar] [CrossRef] [Green Version]
- Abend, N.S.; Younkin, D.; Lewis, D.W. Secondary Headaches in Children and Adolescents. Semin. Pediatr. Neurol. 2010, 17, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.W.; Mathew, N.T. Handbook of Headache; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; ISBN 978-0-7817-5223-7. [Google Scholar]
- McAbee, G.N.; Morse, A.M.; Assadi, M. Pediatric Aspects of Headache Classification in the International Classification of Headache Disorders—3 (ICHD-3 Beta Version). Curr. Pain Headache Rep. 2016, 20, 7. [Google Scholar] [CrossRef]
- Monteith, T.S.; Sprenger, T. Tension Type Headache in Adolescence and Childhood: Where Are We Now? Curr. Pain Headache Rep. 2010, 14, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Silberstein, S.D. Twenty Questions About Headaches in Children and Adolescents. Headache J. Head Face Pain 1990, 30, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Borsook, D.; Maleki, N.; Becerra, L.; McEwen, B. Understanding Migraine through the Lens of Maladaptive Stress Responses: A Model Disease of Allostatic Load. Neuron 2012, 73, 219–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelman, L. The Biological Basis of Headache. Expert Rev. Neurother. 2011, 11, 363–378. [Google Scholar] [CrossRef]
- Dyb, G.; Stensland, S.; Zwart, J.-A. Psychiatric Comorbidity in Childhood and Adolescence Headache. Curr. Pain Headache Rep. 2015, 19, 5. [Google Scholar] [CrossRef] [Green Version]
- Fuh, J.-L.; Wang, S.-J.; Juang, K.-D.; Lu, S.-R.; Liao, Y.-C.; Chen, S.-P. Relationship between Childhood Physical Maltreatment and Migraine in Adolescents. Headache 2010, 50, 761–768. [Google Scholar] [CrossRef]
- Anda, R.; Tietjen, G.; Schulman, E.; Felitti, V.; Croft, J. Adverse Childhood Experiences and Frequent Headaches in Adults. Headache 2010, 50, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults. The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Yücel, B.; Kora, K.; Ozyalçín, S.; Alçalar, N.; Ozdemir, O.; Yücel, A. Depression, Automatic Thoughts, Alexithymia, and Assertiveness in Patients with Tension-Type Headache. Headache 2002, 42, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Braden, J.B.; Sullivan, M.D. Suicidal Thoughts and Behavior among Adults with Self-Reported Pain Conditions in the National Comorbidity Survey Replication. J. Pain Off. J. Am. Pain Soc. 2008, 9, 1106–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polese, D.; Belli, A.; Esposito, D.; Evangelisti, M.; Luchetti, A.; Di Nardo, G.; Parisi, P.; Bruni, O. Psychological Disorders, Adverse Childhood Experiences and Parental Psychiatric Disorders in Children Affected by Headache: A Systematic Review. Neurosci. Biobehav. Rev. 2022, 140, 104798. [Google Scholar] [CrossRef]
- Simons, L.E. Fear of Pain in Children and Adolescents with Neuropathic Pain and Complex Regional Pain Syndrome. Pain 2016, 157 (Suppl. S1), S90–S97. [Google Scholar] [CrossRef] [Green Version]
- Sharp, T.J.; Harvey, A.G. Chronic Pain and Posttraumatic Stress Disorder: Mutual Maintenance? Clin. Psychol. Rev. 2001, 21, 857–877. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.; Stovner, L.J. Epidemiology and Comorbidity of Headache. Lancet Neurol. 2008, 7, 354–361. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef] [Green Version]
- Sciruicchio, V.; Simeone, M.; Foschino Barbaro, M.G.; Tanzi, R.C.; Delussi, M.D.; Libro, G.; D’Agnano, D.; Basiliana, R.; de Tommaso, M. Pain Catastrophizing in Childhood Migraine: An Observational Study in a Tertiary Headache Center. Front. Neurol. 2019, 10, 114. [Google Scholar] [CrossRef]
- Vieira, R.V.d.A.; Vieira, D.C.; Gomes, W.B.; Gauer, G. Alexithymia and Its Impact on Quality of Life in a Group of Brazilian Women with Migraine without Aura. J. Headache Pain 2013, 14, 18. [Google Scholar] [CrossRef] [Green Version]
- Gatta, M.; Canetta, E.; Zordan, M.; Spoto, A.; Ferruzza, E.; Manco, I.; Addis, A.; Dal Zotto, L.; Toldo, I.; Sartori, S.; et al. Alexithymia in Juvenile Primary Headache Sufferers: A Pilot Study. J. Headache Pain 2011, 12, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Gatta, M.; Spitaleri, C.; Balottin, U.; Spoto, A.; Balottin, L.; Mangano, S.; Battistella, P.A. Alexithymic Characteristics in Pediatric Patients with Primary Headache: A Comparison between Migraine and Tension-Type Headache. J. Headache Pain 2015, 16, 98. [Google Scholar] [CrossRef] [Green Version]
- Galli, F.; Canzano, L.; Scalisi, T.G.; Guidetti, V. Psychiatric Disorders and Headache Familial Recurrence: A Study on 200 Children and Their Parents. J. Headache Pain 2009, 10, 187–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, C.S.; Knudsen, G.P.; Steingrímsdóttir, Ó.A. Twin Studies of Pain. Clin. Genet. 2012, 82, 331–340. [Google Scholar] [CrossRef] [Green Version]
- Kendler, K.S. What Psychiatric Genetics Has Taught Us about the Nature of Psychiatric Illness and What Is Left to Learn. Mol. Psychiatry 2013, 18, 1058–1066. [Google Scholar] [CrossRef] [Green Version]
- Schur, E.A.; Noonan, C.; Buchwald, D.; Goldberg, J.; Afari, N. A Twin Study of Depression and Migraine: Evidence for a Shared Genetic Vulnerability. Headache 2009, 49, 1493–1502. [Google Scholar] [CrossRef]
- Fearon, P.; Hotopf, M. Relation between Headache in Childhood and Physical and Psychiatric Symptoms in Adulthood: National Birth Cohort Study. BMJ 2001, 322, 1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldie, K.E.; Poulton, R. Physical and Psychological Correlates of Primary Headache in Young Adulthood: A 26 Year Longitudinal Study. J. Neurol. Neurosurg. Psychiatry 2002, 72, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arruda, M.A.; Bigal, M.E. Behavioral and Emotional Symptoms and Primary Headaches in Children: A Population-Based Study. Cephalalgia 2012, 32, 1093–1100. [Google Scholar] [CrossRef]
- Naaijen, J.; Forde, N.J.; Lythgoe, D.J.; Akkermans, S.E.A.; Openneer, T.J.C.; Dietrich, A.; Zwiers, M.P.; Hoekstra, P.J.; Buitelaar, J.K. Fronto-Striatal Glutamate in Children with Tourette’s Disorder and Attention-Deficit/Hyperactivity Disorder. NeuroImage Clin. 2017, 13, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Genizi, J.; Khourieh Matar, A.; Schertz, M.; Zelnik, N.; Srugo, I. Pediatric Mixed Headache -The Relationship between Migraine, Tension-Type Headache and Learning Disabilities—In a Clinic-Based Sample. J. Headache Pain 2016, 17, 42. [Google Scholar] [CrossRef] [Green Version]
- MacGregor, E.A. Classification of Perimenstrual Headache: Clinical Relevance. Curr. Pain Headache Rep. 2012, 16, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Aegidius, K.L.; Zwart, J.-A.; Hagen, K.; Dyb, G.; Holmen, T.L.; Stovner, L.J. Increased Headache Prevalence in Female Adolescents and Adult Women with Early Menarche. The Head-HUNT Studies. Eur. J. Neurol. 2011, 18, 321–328. [Google Scholar] [CrossRef]
- Lieba-Samall, D.; Wöberl, C.; Frantall, S.; Brannathl, W.; Schmidtl, K.; Schrolnbergerl, C.; Wöber-Bingöll, Ç.; Group, P. Study Headache, Menstruation and Combined Oral Contraceptives: A Diary Study in 184 Women with Migraine. Eur. J. Pain 2011, 15, 852–857. [Google Scholar] [CrossRef]
- Kröner-Herwig, B.; Vath, N. Menarche in Girls and Headache—A Longitudinal Analysis. Headache J. Head Face Pain 2009, 49, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.T.; Behbehani, M. Ovarian Hormones and Migraine Headache: Understanding Mechanisms and Pathogenesis—Part I. Headache J. Head Face Pain 2006, 46, 3–23. [Google Scholar] [CrossRef]
- Kelman, L. Migraine Changes with Age: IMPACT on Migraine Classification. Headache J. Head Face Pain 2006, 46, 1161–1171. [Google Scholar] [CrossRef]
- Bille, B. Migraine and Tension-Type Headache in Children and Adolescents. Cephalalgia Int. J. Headache 1996, 16, 78. [Google Scholar] [CrossRef]
- Guidetti, V.; Galli, F. Evolution of Headache in Childhood and Adolescence: An 8-Year Follow-Up. Cephalalgia Int. J. Headache 1998, 18, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Tietjen, G.E. Childhood Maltreatment and Headache Disorders. Curr. Pain Headache Rep. 2016, 20, 26. [Google Scholar] [CrossRef]
- Faria, V.; Erpelding, N.; Lebel, A.; Johnson, A.; Wolff, R.; Fair, D.; Burstein, R.; Becerra, L.; Borsook, D. The Migraine Brain in Transition: Girls vs. Boys. Pain 2015, 156, 2212–2221. [Google Scholar] [CrossRef]
- Malter Cohen, M.; Jing, D.; Yang, R.R.; Tottenham, N.; Lee, F.S.; Casey, B.J. Early-Life Stress Has Persistent Effects on Amygdala Function and Development in Mice and Humans. Proc. Natl. Acad. Sci. USA 2013, 110, 18274–18278. [Google Scholar] [CrossRef] [Green Version]
- Lipton, R.B.; Manack, A.; Ricci, J.A.; Chee, E.; Turkel, C.C.; Winner, P. Prevalence and Burden of Chronic Migraine in Adolescents: Results of the Chronic Daily Headache in Adolescents Study (C-DAS): May 2011. Headache J. Head Face Pain 2011, 51, 693–706. [Google Scholar] [CrossRef]
- Raucci, U.; Boni, A.; Evangelisti, M.; Della Vecchia, N.; Velardi, M.; Ursitti, F.; Terrin, G.; Di Nardo, G.; Reale, A.; Villani, A.; et al. Lifestyle Modifications to Help Prevent Headache at a Developmental Age. Front. Neurol. 2021, 11, 618375. [Google Scholar] [CrossRef]
- Palermo, T.M.; Eccleston, C.; Lewandowski, A.S.; de C Williams, A.C.; Morley, S. Randomized Controlled Trials of Psychological Therapies for Management of Chronic Pain in Children and Adolescents: An Updated Meta-Analytic Review. Pain 2010, 148, 387–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarafino, E.P.; Goehring, P. Age Comparisons in Acquiring Biofeedback Control and Success in Reducing Headache Pain1. Ann. Behav. Med. 2000, 22, 10–16. [Google Scholar] [CrossRef]
- Andrasik, F.; Larsson, B.; Grazzi, L. Biofeedback Treatment of Recurrent Headaches in Children and Adolescents. In Headache and Migraine in Childhood and Adolescence; CRC Press: Boca Raton, FL, USA, 2001; ISBN 978-0-429-21805-7. [Google Scholar]
- Andrasik, F.; Grazzi, L.; Usai, S.; Bussone, G. Pharmacological Treatment Compared to Behavioural Treatment for Juvenile Tension-Type Headache: Results at Two-Year Follow-Up. Neurol. Sci. 2007, 28, S235–S238. [Google Scholar] [CrossRef] [PubMed]
- Sobe, H.; Richter, M.; Berner, R.; von der Hagen, M.; Hähner, A.; Röder, I.; Koch, T.; Sabatowski, R.; Klimova, A.; Gossrau, G. Functional Improvement in Children and Adolescents with Primary Headache after an Interdisciplinary Multimodal Therapy Program: The DreKiP Study. J. Headache Pain 2022, 23, 109. [Google Scholar] [CrossRef] [PubMed]
- Arndorfer, R.E.; Allen, K.D. Extending the Efficacy of a Thermal Biofeedback Treatment Package to the Management of Tension-Type Headaches in Children. Headache J. Head Face Pain 2001, 41, 183–192. [Google Scholar] [CrossRef]
- Grazzi, L.; Andrasik, F.; D’Amico, D.; Leone, M.; Moschiano, F.; Bussone, G. Electromyographic Biofeedback-Assisted Relaxation Training in Juvenile Episodic Tension-Type Headache: Clinical Outcome at Three-Year Follow-Up the in of and for on with at Is an as By. Cephalalgia 2001, 21, 798–803. [Google Scholar] [CrossRef]
- Karwautz, A.; Wöber, C.; Lang, T.; Böck, A.; Wagner-Ennsgraber, C.; Vesely, C.; Kienbacher, C.; Wöber-Bingöl, C. Psychosocial Factors in Children and Adolescents with Migraine and Tension-Type Headache: A Controlled Study and Review of the Literature. Cephalalgia 1999, 19, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Aromaa, M.; Sillanpää, M.; Rautava, P.; Helenius, H. Pain Experience of Children with Headache and Their Families: A Controlled Study. Pediatrics 2000, 106, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Anttila, P. Tension-Type Headache in Childhood and Adolescence. Lancet Neurol. 2006, 5, 268–274. [Google Scholar] [CrossRef]
- Haag, G. Letter to the Editor Concerning Bendtsen L, Evers S, Linde M, Mitsikostas DD, Sandrini G, Schoenen J. EFNS Guideline on the Treatment of Tension-Type Headache—Report of an EFNS Task Force. Eur J Neurol 2010, 17, 1318–1325. [Google Scholar] [CrossRef]
- Carotenuto, M.; Esposito, M.; Pascotto, A. Cefalea di tipo tensivo: Diagnostica e terapia. G. Neuropsichiatr. Dellà Evol. 2012, 32, 29–37. [Google Scholar]
- Papetti, L.; Salfa, I.; Battan, B.; Moavero, R.; Termine, C.; Bartoli, B.; Di Nunzio, F.; Tarantino, S.; Alaimo Di Loro, P.; Vigevano, F.; et al. Features of Primary Chronic Headache in Children and Adolescents and Validity of Ichd 3 Criteria. Front. Neurol. 2019, 10, 92. [Google Scholar] [CrossRef] [Green Version]
- Hershey, A.D.; Powers, S.W.; Bentti, A.-L.; DeGrauw, T.J. Effectiveness of Amitriptyline in the Prophylactic Management of Childhood Headaches. Headache J. Head Face Pain 2000, 40, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Yurekli, V.A.; Akhan, G.; Kutluhan, S.; Uzar, E.; Koyuncuoglu, H.R.; Gultekin, F. The Effect of Sodium Valproate on Chronic Daily Headache and Its Subgroups. J. Headache Pain 2008, 9, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Grazzi, L.; Andrasik, F.; Usai, S.; Bussone, G. Magnesium as a Preventive Treatment for Paediatric Episodic Tension-Type Headache: Results at 1-Year Follow-Up. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2007, 28, 148–150. [Google Scholar] [CrossRef]


{kind=link}
| Infrequent Episodic TTH | Frequent Episodic TTH | Chronic TTH |
|---|---|---|
| A. At least 10 episodes of headache occurring on <1 day per month on average (<12 days per year) and fulfilling criteria B–D | A. At least 10 episodes of headache occurring on 1–14 days per month on average for >3 months (12 and <180 days per year) and fulfilling criteria B–D | A. Headache occurring on 15 days per month on average for >3 months (180 days per year), fulfilling criteria B–D |
| B. Lasting from 30 min to 7 days | B. Lasting hours to days, or unremitting | |
| C. At least two of the following four characteristics: 1. Bilateral location; 2. Pressing or tightening (non-pulsating) quality; 3. Mild or moderate intensity; 4. Not aggravated by routine physical activity such as walking or climbing stairs. | ||
| D. Both of the following: 1. No nausea or vomiting; 2. No more than one of photophobia or phonophobia. | D. Both of the following: 1. No more than one of photophobia, phonophobia or mild nausea; 2. Neither moderate or severe nausea nor vomiting. | |
| E. Not better accounted for by another ICHD-3 diagnosis. | ||
| Treatment Approaches | Ref. | |
|---|---|---|
| First line: Lifestyle modifications |
| [75] |
| Second line: Non-pharmacological treatments |
| [76,79] |
| Third line: Pharmacological therapy | Acute/abortive treatment:
| [27] |
Preventive/prophylaxis:
| [89] [90] [91] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baglioni, V.; Orecchio, S.; Esposito, D.; Faedda, N.; Natalucci, G.; Guidetti, V. Tension-Type Headache in Children and Adolescents. Life 2023, 13, 825. https://doi.org/10.3390/life13030825
Baglioni V, Orecchio S, Esposito D, Faedda N, Natalucci G, Guidetti V. Tension-Type Headache in Children and Adolescents. Life. 2023; 13(3):825. https://doi.org/10.3390/life13030825
Chicago/Turabian StyleBaglioni, Valentina, Silvia Orecchio, Dario Esposito, Noemi Faedda, Giulia Natalucci, and Vincenzo Guidetti. 2023. "Tension-Type Headache in Children and Adolescents" Life 13, no. 3: 825. https://doi.org/10.3390/life13030825