
Outcome of Continuous Positive Airway Pressure Adherence Based on Nasal Endoscopy and the Measurement of Nasal Patency—A Prospective Study
 and
and
Abstract
:1. Introduction
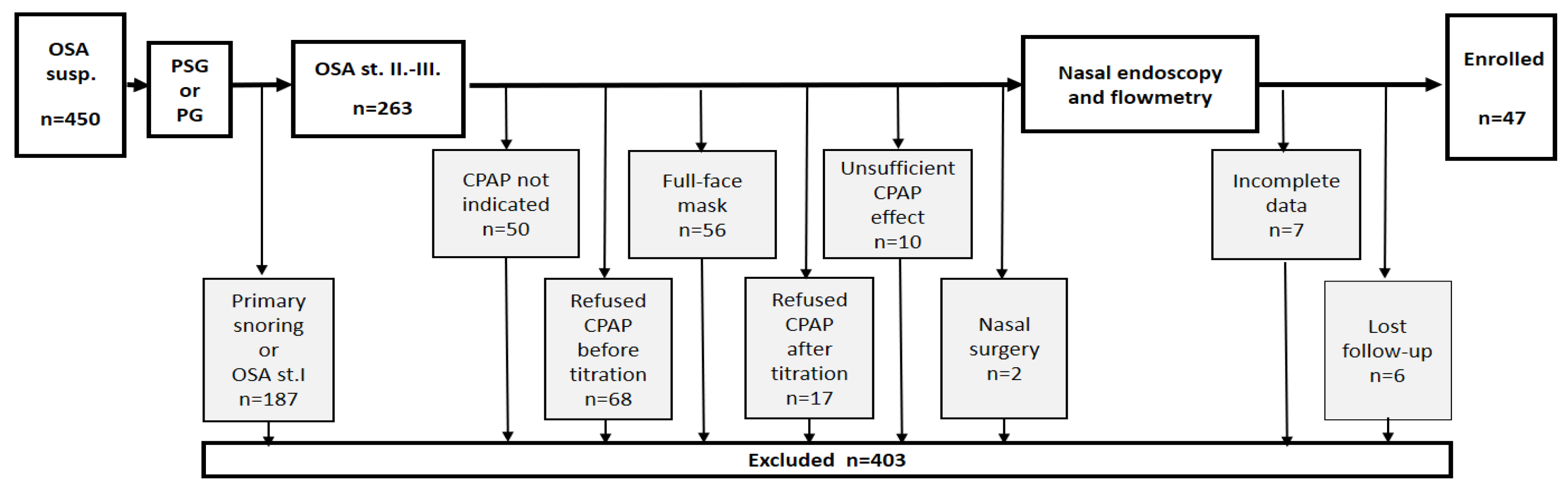
2. Material and Methods
2.1. Material
2.2. Methods
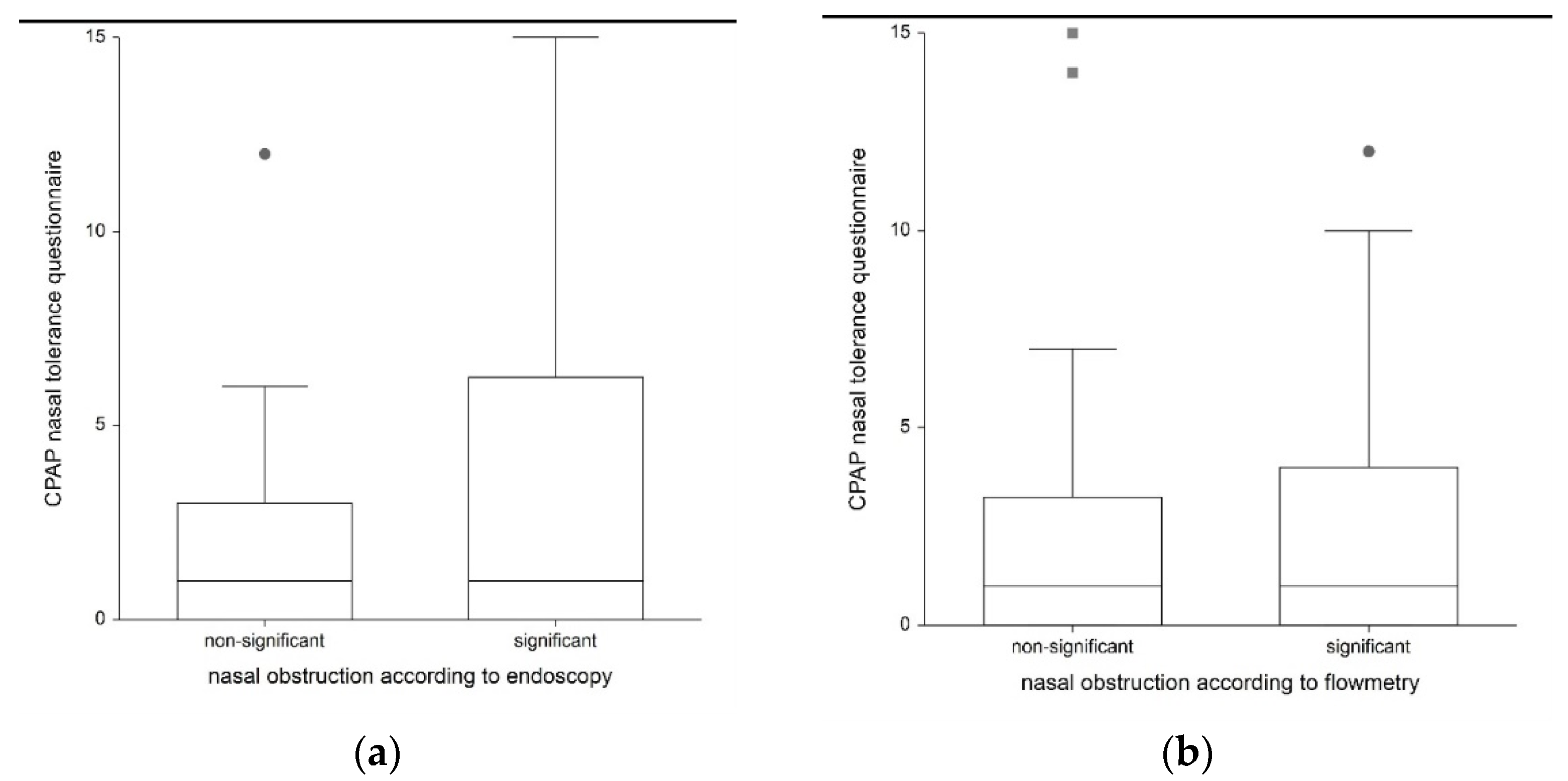
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AHI | apnea-hypopnea index |
| BMI | body mass index |
| CPAP | continuous positive airway pressure |
| ES6 | endoscopic score 6 |
| ICSD-3 | international classification of sleep disorders—third edition |
| OCST | out-of-center sleep testing |
| ODI | oxygen desaturation index |
| OSA | obstructive sleep apnea |
| PAP | positive airway pressure |
| PG | polygraphy |
| PSG | polysomnography |
| VAS | visual analogue scale |
References
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Gilat, H.; Vinker, S.; Buda, I.; Soudry, E.; Shani, M.; Bachar, G. Obstructive sleep apnea and cardiovascular comorbidities: A large epidemiologic study. Medicine 2014, 93, e45. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Ronald, J.; Delaive, K.; Walld, R.; Manfreda, J.; Kryger, M.H. What are obstructive sleep apnea patients being treated for prior to this diagnosis? Chest 2002, 121, 164–172. [Google Scholar] [CrossRef] [PubMed]
- de Sousa Michels, D.; da Mota Silveira Rodrigues, A.; Nakanishi, M.; Sampaio, A.L.L.; Venosa, A.R. Nasal involvement in obstructive sleep apnea syndrome. Int. J. Otolaryngol. 2014, 2014, 717419. [Google Scholar] [CrossRef]
- Oeverland, B.; Akre, H.; Skatvedt, O. Oral breathing in patients with sleep-related breathing disorders. Acta Otolaryngol. 2002, 122, 651–654. [Google Scholar] [CrossRef]
- Becker, H.F.; Jerrentrup, A.; Ploch, T.; Grote, L.; Penzel, T.; Sullivan, C.E.; Peter, J.H. Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive sleep apnea. Circulation 2003, 107, 68–73. [Google Scholar] [CrossRef]
- Slouka, D.; Kucera, R.; Gal, B.; Betka, J.; Skalova, A. Biomarkers—A possibility for monitoring of obstructive sleep apnea syndrome. Neuro Endocrinol. Lett. 2019, 40, 85–92. [Google Scholar]
- Levrini, L.; Sacchi, F.; Milano, F.; Polimeni, A.; Cozza, P.; Bernkopf, E.; Segu, M.; Italian dentist work group about OSAS Collaborators; Zucconi, M.; Vicini, C.; et al. Italian recommendations on dental support in the treatment of adult obstructive sleep apnea syndrome (OSAS). Ann Stomatol. 2016, 6, 81–86. [Google Scholar] [CrossRef]
- Slouka, D.; Honnerova, M.; Hrabe, V.; Matas, A. The prediction of treatment failure of the continuous positive airways pressure. Bratisl. Lek. Listy 2014, 115, 704–707. [Google Scholar] [CrossRef] [Green Version]
- Slouka, D.; Honnerova, M.; Hosek, P.; Matas, A.; Slama, K.; Landsmanova, J.; Kucera, R. Risk factors for failure of continuous positive airway pressure treatment in patients with ostructive sleep apnoea. Biomed. Pap. 2018, 162, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Stepnowsky, C.J.; Moore, P.J. Nasal CPAP treatment for obstructive sleep apnea: Developing a new perspective on dosing strategies and compliance. J. Psychosom. Res. 2003, 54, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Kribbs, N.B.; Pack, A.I.; Kline, L.R.; Schwartz, A.R.; Schubert, N.M.; Redline, S.; Henry, J.N.; Getsy, J.E.; Dinges, D.F. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am. Rev. Respir. Dis. 1993, 147, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Slouka, D.; Honnerova, M.; Hosek, P.; Gal, B.; Trcka, O.; Kostlivy, T.; Landsmanova, J.; Havel, D.; Baneckova, M.; Kucera, R. Improved prediction of CPAP failure using T90, age and gender. J. Appl. Biomed. 2019, 17, 81. [Google Scholar] [CrossRef] [Green Version]
- Lam, A.S.; Collop, N.A.; Bliwise, D.L.; Dedhia, R.C. Validated Measures of Insomnia, Function, Sleepiness, and Nasal Obstruction in a CPAP Alternatives Clinic Population. J. Clin. Sleep Med. 2017, 13, 949–957. [Google Scholar] [CrossRef]
- Chowdhury, O.; Wedderburn, C.J.; Duffy, D.; Greenough, A. CPAP review. Eur. J. Pediatr. 2012, 171, 1441–1448. [Google Scholar] [CrossRef]
- Cai, Y.; Goldberg, A.N.; Chang, J.L. The Nose and Nasal Breathing in Sleep Apnea. Otolaryngol. Clin. N. Am. 2020, 53, 385–395. [Google Scholar] [CrossRef]
- Balztan, M.A.; Elkholi, O.; Wolkove, N. Evidence of interrelated side effects with reduced compliance in patients treated with nasal continuous positive airway pressure. Sleep Med. 2009, 10, 198–205. [Google Scholar] [CrossRef]
- Li, H.; Wang, P.; Chen, Y.; Lee, L.; Fang, T.; Lin, H. Critical appraisal and meta-analysis of nasal surgery for obstructive sleep apnea. Am. J. Rhinol. Allergy 2011, 25, 45–49. [Google Scholar] [CrossRef]
- Nakata, S.; Noda, A.; Yagi, H.; Yanagi, E.; Mimura, T.; Okada, T.; Misawa, H.; Nakashima, T. Nasal resistance for determinant factor of nasal surgery in CPAP failure patients with obstructive sleep apnea syndrome. Rhinology 2005, 43, 296–299. [Google Scholar]
- Inoue, A.; Chiba, S.; Matsuura, K.; Osafune, H.; Capasso, R.; Wada, K. Nasal function and CPAP compliance. Auris Nasus Larynx 2019, 46, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Elwany, S.; Bahgat, A.Y.; Ibrahim, M.; Bazak, R. Surgical correction of nasal obstruction in obstructive sleep apnea improves CPAP outcomes and compliance. Ir. J. Med. Sci. 2022, 191, 2723–2728. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.; Riaz, M.; Capasso, R.; Ruoff, C.M.; Guilleminault, C.; Kushida, C.A.; Certal, V. The effect of nasal surgery on continuous positive airway pressure device use and therapeutic treatment pressures: A systematic review and meta-analysis. Sleep 2015, 38, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, T.; Noda, A.; Nakata, S.; Yasuda, Y.; Soga, T.; Miyata, S.; Nakai, S.; Koike, Y. Influence of nasal resistance on initial acceptance of continuous positive airway pressure in treatment for obstructive sleep apnea syndrome. Respiration 2007, 74, 56–60. [Google Scholar] [CrossRef]
- Bengtsson, C.; Jonsson, L.; Theorell-Haglow, J.; Holmstrom, M.; Janson, C.; Lindberg, E. Sinonasal outcome test-22 and peak nasal inspiratory flow—Valuable tools in obstructive sleep apnoea. Rhinology 2020, 58, 341–348. [Google Scholar] [CrossRef]
- Awad, M.I.; Kacker, A. Nasal Obstruction Considerations in Sleep Apnea. Otolaryngol. Clin. N. Am. 2018, 51, 1003–1009. [Google Scholar] [CrossRef]
- Pretl, M.; Hobzova, M.; Honnerova, M.; Lnenicka, J.; Novak, V.; Sedlak, V.; Vyskocilova, J.; Sonka, K. Indikační kritéria pro léčbu poruch dýchání ve spánku pomocí přetlaku v dýchacích cestách u dospělých. Neurol. Praxi 2013, 14, 38–41. [Google Scholar]
- Knizek, Z.; Vodicka, J.; Jelinek, J.; Rezny, Z. Měření nosní průchodnosti pomocí flowmetrie a klasifikace endoskopického obrazu nosní dutiny. Otorhinolaryngol. Phoniatr. Otorinolaryngol. A Foniatr. 2019, 68, 143–149. [Google Scholar]
- Mladina, R. The role of maxillar morphology in the development of pathological septal deformities. Rhinology 1987, 25, 199–205. [Google Scholar]
- Mladina, R.; Skitarelić, N.; Poje, G.; Subaric, M. Clinical Implications of Nasal Septal Deformities. Balk. Med. J. 2015, 32, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, C.; Gillett, S.; Slack, R. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin. Otolaryngol. 2009, 34, 447–1454. [Google Scholar] [CrossRef] [PubMed]
- Schalek, P. Česká verze dotazníku kvality života pro pacienty s chronickou rinosinusitidou SNOT-22 (Sino-nasal outcome test). Otorinolaryngol. Foniatr. 2010, 59, 149–151. [Google Scholar]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58 (Suppl. S29), 1–464. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.Y.; Chen, Y.H.; Hu, S.W.; Lin, M.T.; Lee, P.L.; Chiang, A.A.; Tu, Y.K. In search of a better CPAP interface: A network meta-analysis comparing nasal masks, nasal pillows and oronasal masks. J. Sleep Res. 2022, 31, e13686. [Google Scholar] [CrossRef] [PubMed]
- Andrade, R.G.S.; Piccin, V.S.; Nascimento, J.A.; Viana, F.M.L.; Genta, P.R.; Lorenzi-Filho, G. Impact of the type of mask on the effectiveness of and adherence to continuous positive airway pressure treatment for obstructive sleep apnea. J. Bras. Pneumol. 2014, 40, 658–668. [Google Scholar] [CrossRef]
- Andrade, R.G.S.; Viana, F.M.; Nascimento, J.A.; Drager, L.F.; Moffa, A.; Brunoni, A.R.; Genta, P.R.; Lorenzi-Filho, G. Nasal vs Oronasal CPAP for OSA Treatment: A Meta-Analysis. Chest 2018, 153, 665–674. [Google Scholar] [CrossRef]
- Balsalobre, L.; Pezato, R.; Mangussi-Gomes, J.; Gregorio, L.; Haddad, F.L.M.; Gregorio, L.C.; Fujita, R. What is the Impact of Positive Airway Pressure in Nasal Polyposis? An Experimental Study. Int. Arch. Otorhinolaryngol. 2019, 23, 147–151. [Google Scholar] [CrossRef] [Green Version]
- Lansky, M.; Plzak, J.; Ondrova, M.; Janousek, P.; Kraus, J.; Minarik, R. Doporučený diagnostický a terapeutický postup pro pracoviště zajišťující diagnostiku a chirurgickou léčbu poruch dýchání ve spánku u dospělých pacientů. Otorinolaryngol. Foniatr. 2013, 62, 48–49. [Google Scholar]
- Schoustra, E.; Maanen, P.V.; Haan, C.D.; Ravesloot, M.J.L.; de Vries, N. The Role of Isolated Nasal Surgery in Obstructive Sleep Apnea Therapy-A Systematic Review. Brain Sci. 2022, 12, 1446. [Google Scholar] [CrossRef]
- Rosow, D.E.; Stewart, M.G. Is nasal surgery an effective treatment for obstructive sleep apnea? Laryngoscope. 2010, 120, 1496–1497. [Google Scholar] [CrossRef]
- Liu, H.; Lin, Y.; Kuan, Y.; Huang, Y.; Hou, W.; Liou, T.; Chen, H. Intranasal corticosteroid therapy in the treatment of obstructive sleep apnea: A meta-analysis of randomized controlled trials. Am. J. Rhinol. Allergy 2016, 30, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Kiely, J.L.; Nolan, P.; McNicholas, W.T. Intranasal corticosteroid therapy for obstructive sleep apnoea in patients with co-existing rhinitis. Thorax 2004, 59, 50–55. [Google Scholar] [PubMed]
- Charakorn, N.; Hirunwiwatkul, P.; Chirakalwasan, N.; Chaitusaney, B.; Prakassajjatham, M. The effects of topical nasal steroids on continuous positive airway pressure compliance in patients with obstructive sleep apnea: A systematic review and meta-analysis. Sleep Breath. 2017, 21, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, A.L.; Chang, Y.F.; Soose, R.J.; Gillman, G.S. The impact of nasal surgery on sleep quality: A prospective outcomes study. Otolaryngol. Head Neck Surg. 2014, 151, 868–873. [Google Scholar] [CrossRef]
- Li, H.; Lin, Y.; Chen, N.; Lee, L.; Fang, T.; Wang, P. Improvement in quality of life after nasal surgery alone for patients with obstructive sleep apnea and nasal obstruction. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 429–433. [Google Scholar] [CrossRef] [Green Version]
- Iwata, N.; Nakata, S.; Inada, H.; Kimura, A.; Hirata, M.; Yasuma, F. Clinical indication of nasal surgery for the CPAP intolerance in obstructive sleep apnea with nasal obstruction. Auris Nasus Larynx 2020, 47, 1018–1022. [Google Scholar] [CrossRef]
- Poirier, J.; George, C.; Rotenberg, B. The effect of nasal surgery on nasal continuous positive airway pressure compliance. Laryngoscope 2014, 124, 317–319. [Google Scholar] [CrossRef]
- Pniak, T.; Matousek, P.; Strympl, P.; Novak, V.; Kominek, P. Obstrukční spánková apnoe a CPAP—Má význam řešit nosní průchodnost? Česká A Slov. Neurol. A Neurochir. 2012, 2, 222–226. [Google Scholar]
- van Egmond, M.M.H.T.; Rovers, M.M.; Tillema, A.H.J.; van Neerbeek, N. Septoplasty for nasal obstruction due to a deviated nasal septum in adults: A systematic review. Rhinology 2018, 56, 195–208. [Google Scholar] [CrossRef] [Green Version]
- Shin, C.H.; Jang, Y.J. Factors affecting the complication rate of septoplasty: Analysis of 1506 consecutive cases of single surgeon. Facial Plast. Surg. 2022; Online Ahead of Print. [Google Scholar] [CrossRef]
- Titirungruang, C.K.; Charakorn, N.; Chaitusaney, B.; Hirunwiwatkul, P. Is postoperative nasal packing after septoplasty safe? A systematic review and meta-analysis of randomized controlled studies. Rhinology 2021, 59, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.; Chang, E.T.; Neighbors, C.L.P.; Noller, M.W.; Mack, D.; Capasso, R.; Kushida, C.A. Thirty-five alternatives to positive airway pressure therapy for obstructive sleep apnea: An overview of meta-analyses. Expert Rev. Respir. Med. 2018, 12, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Friedman, M.; Chang, H.W.; Gurpinar, B. The efficacy of multilevel surgery of the upper airway in adults with obstructive sleep apnea/hypopnea syndrome. Laryngoscope 2008, 118, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Shelgikar, A.V.; Aronovich, S.; Stanley, J.J. Multidisciplinary Alternatives to CPAP Program for CPAP-Intolerant Patients. J. Clin. Sleep Med. 2017, 13, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Kempfle, J.S.; BuSaba, N.Y.; Dobrowski, J.M.; Westover, M.B.; Bianchi, M.T. A cost-effectiveness analysis of nasal surgery to increase continuous positive airway pressure adherence in sleep apnea patients with nasal obstruction. Laryngoscope 2017, 127, 977–983. [Google Scholar] [CrossRef] [Green Version]
- Park, P.; Kim, J.; Song, Y.; Lim, J.; Cho, S.; Won, T.; Han, D.; Kim, D.; Rhee, C.; Kim, H. Influencing factors on CPAP adherence and anatomic characteristics of upper airway in OSA subjects. Medicine 2017, 96, e8818. [Google Scholar] [CrossRef]
- Brimioulle, M.; Chaidas, K. Nasal function and CPAP use in patients with obstructive sleep apnoea: A systematic review. Sleep Breath. 2022, 26, 1321–1332. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Female | Male | Total | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 13 | n = 34 | n = 47 | |||||||||||||
| Mean | SD | Median | IQR | Range | Mean | SD | Median | IQR | Range | Mean | SD | Median | IQR | Range | |
| Age (years) | 61.6 | 17.7 | 61.5 | 18 | 49–74 | 54.2 | 26.9 | 55.0 | 16.8 | 36–74 | 56.3 | 10.7 | 56 | 17.0 | 36–74 |
| BMI (kg/m2) | 35.4 | 5.1 | 36.5 | 7.4 | 27.8–44.4 | 33.6 | 7.5 | 33.5 | 6.2 | 25.7–44.7 | 34.1 | 7.0 | 34.3 | 6.8 | 25.7–44.7 |
| AHI (n/h) | 40.0 | 34.2 | 43.4 | 22.9 | 18.6–119.2 | 55.2 | 26.8 | 57.9 | 33.0 | 18.5–95.8 | 51.0 | 23.7 | 47.4 | 36.1 | 18.5–119.2 |
| 30 > AHI ≥ 15(n) | 4 | 30.8% | 4 | 11.8% | 8 | 17.0% | |||||||||
| AHI ≥ 30 (n) | 9 | 69.2% | 30 | 88.2% | 39 | 83.0% | |||||||||
| ODI (n/h) | 40.3 | 26.4 | 31.7 | 22.6 | 18.5–118.7 | 51.9 | 23.0 | 55.1 | 36.3 | 16.0–116.0 | 48.6 | 24.2 | 45.2 | 34.0 | 16.0–118.7 |
| Basal O2 sat. (%) | 90.9 | 3.4 | 92.0 | 2.5 | 83.0–95.0 | 90.5 | 16.0 | 92.0 | 5.0 | 79.0–96.0 | 90.6 | 13.7 | 92.0 | 5.0 | 79.0–96.0 |
| Average low O2sat. (%) | 85.6 | 4.2 | 87.0 | 5.5 | 77.0–92.0 | 84.1 | 15.9 | 86.0 | 8.5 | 65.0–92.0 | 84.5 | 13.7 | 86.5 | 8.0 | 65.0–92.0 |
| T 90 (%) | 19.8 | 18.9 | 10.3 | 22.4 | 0.7–63.6 | 29.7 | 25.0 | 26.2 | 46.6 | 1.0–69.3 | 26.9 | 23.6 | 14.9 | 43.0 | 0.7–69.3 |
| Mean CPAP (cm H2O) | 10.5 | 1.8 | 10.6 | 2.0 | 6.0–13.0 | 10.1 | 3.1 | 10.0 | 3.75 | 6.0–18.0 | 10.3 | 2.8 | 10.0 | 3.0 | 6.0–18.0 |
| Group | Septal Deformity | Inferior Turbinate Hypertrophy |
|---|---|---|
| 1 | No | No |
| 2 | No | Yes |
| 3 | Non-significant (type 1,3,6) | No |
| 4 | Non-significant (type 1,3,6) | Yes |
| 5 | Significant (type 2,4,5) | No |
| 6 | Significant (type 2,4,5) | Yes |
| Group | Compliant | Non-Compliant | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 35 | n = 12 | ||||||||||
| Male | Female | Male | Female | ||||||||
| Gender | 28 | 74.3% | 7 | 25.7% | 8 | 66.7% | 4 | 33.3% | 0.713 | ||
| Mean | SD | Median | IQR | Range | Mean | SD | Median | IQR | Range | ||
| Age (years) | 55.7 | 11.1 | 54.0 | 18 | 36–74 | 57.8 | 9.7 | 56.5 | 11.8 | 36–72 | 0.427 |
| BMI (kg/m2) | 34.3 | 7.7 | 34.7 | 7.6 | 25.7–44.7 | 33.5 | 4.2 | 32.8 | 6.3 | 28.3–43.2 | 0.621 |
| AHI (n/h) | 54.1 | 24.3 | 52.0 | 36.2 | 18.5–119.2 | 41.9 | 19.7 | 33.6 | 37.8 | 18.6–71.8 | 0.124 |
| 30 > AHI ≥ 15(n) | 4 | 11.4% | 4 | 33.3% | |||||||
| AHI ≥ 30 (n) | 31 | 88.6% | 8 | 66.7% | |||||||
| ODI (n/h) | 50.4 | 26.4 | 45.6 | 37.9 | 16.0–118.7 | 43.6 | 16.4 | 41.4 | 23.2 | 18.6–64.4 | 0.495 |
| Basal O2 saturation (%) | 90.1 | 15.7 | 91.0 | 5.3 | 79.0–96.0 | 92.1 | 2.7 | 93.0 | 2.8 | 86.0–95.0 | 0.066 |
| Average low O2 sat. (%) | 84.2 | 15.5 | 86.0 | 8.0 | 70.0–92.0 | 85.5 | 5.7 | 87.5 | 88.0 | 75.0–92.0 | 0.501 |
| T 90 (%) | 28.4 | 24.0 | 23.2 | 45.3 | 1.0–69.3 | 22.6 | 23.0 | 11.2 | 38.8 | 0.7–65.8 | 0.502 |
| Mean CPAP (cm H20) | 9.9 | 2.1 | 10.0 | 2.4 | 6.0–13.5 | 11.4 | 3.0 | 10.7 | 3.8 | 8.0–18.0 | 0.057 |
| ES6 | ≥4 | <4 | p | |||||||||
| N = 20 | N = 27 | |||||||||||
| Mean | SD | Median | IQR | Range | Mean | SD | Median | IQR | Range | |||
| CPAP compl. | 79.0% | 23.5 | 85.7 | 24.3 | 16.0–100.0 | 73.6 % | 26.8 | 86.4 | 35.6 | 0.0–100.0 | 0.498 | |
| questionnaire | 3.7 | 5.0 | 1.0 | 6.3 | 0.0–15.0 | 1.9 | 2.7 | 1.0 | 3.0 | 0.0–12.0 | 0.588 | |
| Flow measurement | <4.57 V | ≥4.57 V | ||||||||||
| N = 21 | N = 26 | |||||||||||
| CPAP compl. | 79.7 % | 18.1 | 87.0 | 24.4 | 38.0–100.0 | 72.9 % | 29.9 | 86.1 | 41.7 | 0.0–100.0 | 0.754 | |
| questionnaire | 2.9 | 3.9 | 1.0 | 4.0 | 0.0–12.0 | 2.5 | 4.0 | 1.0 | 3.3 | 0.0–15.0 | 0.657 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knížek, Z.; Kotulek, M.; Brothánková, P.; Pecháčková, E.; Klail, P.; Kostlivý, T.; Vodička, J. Outcome of Continuous Positive Airway Pressure Adherence Based on Nasal Endoscopy and the Measurement of Nasal Patency—A Prospective Study. Life 2023, 13, 219. https://doi.org/10.3390/life13010219
Knížek Z, Kotulek M, Brothánková P, Pecháčková E, Klail P, Kostlivý T, Vodička J. Outcome of Continuous Positive Airway Pressure Adherence Based on Nasal Endoscopy and the Measurement of Nasal Patency—A Prospective Study. Life. 2023; 13(1):219. https://doi.org/10.3390/life13010219
Chicago/Turabian StyleKnížek, Zdeněk, Miloš Kotulek, Pavlína Brothánková, Eva Pecháčková, Pavel Klail, Tomáš Kostlivý, and Jan Vodička. 2023. "Outcome of Continuous Positive Airway Pressure Adherence Based on Nasal Endoscopy and the Measurement of Nasal Patency—A Prospective Study" Life 13, no. 1: 219. https://doi.org/10.3390/life13010219