1. Introduction
Obstructive Sleep Apnea (OSA) is a state determined by repeated episodes of partial or complete airway obstruction over sleep [
1,
2]. Apnea–Hypopnea Index (AHI) or the number of apneas/hypopneas per hour of sleep is the basic metric for identifying OSA that this is evaluated by Polysomnography (PSG) or other shapes of sleep monitoring [
3]. The overall prevalence of OSA in adults (AHI ≥ 5 events/h) ranged from 9–38% in the public adult population and was more in men [
4]. In addition, the OSA prevalence was calculated to be 56.0% in patients with type 2 diabetes [
5].
Obesity, smoking, alcohol consumption, higher age, and male gender can be the risk factors for OSA [
6]. It has been shown the impact of ethnicity on the prevalence and severity of OSA that this impact can be related to ethnic differences in adipose tissue distributions [
7]. Apart from the environmental and demographical factors, the studies reported that genetic [
8,
9,
10,
11] and blood [
12,
13,
14,
15,
16,
17,
18,
19] factors could also affect the prevalence or development of OSA.
Ghrelin (a 28 amino acid hormone or orexigenic neuropeptide involving an n-octanoyl group on the serine in position 3) [
20] is known as an endocrine pathway in controlling nutrition and energy balance that is secreted by a large number of tissues, but its dominant source is the gastric mucosa [
21,
22]. Ghrelin is in both acylated and unacylated forms [
23]. Acylated ghrelin is the active shape of ghrelin [
24] (acylation is essential for the ghrelin binding and function [
25]) with some metabolic functions such as appetite stimulation, reduced insulin secretion from pancreatic, elevated growth hormone secretion, reduced body energy consumption, and environmental growth and metabolism, especially carbohydrates and fats [
22].
The OSA is related to hormonal features and is illustrated by high levels of ghrelin and leptin hormones that may provoke additional energy intake [
26]. In men with OSA, energy expenditure relative to body weight reduces with elevating severity of oxygen desaturation that can contribute to a positive energy balance [
27]. The studies [
28,
29] reported different results for blood levels of ghrelin in adults with OSA in comparison with controls. The relationship between OSA and plasma/serum levels of ghrelin is controversial [
30]. Obesity [
31], cardiovascular diseases [
32], diabetes and metabolic syndrome [
33], and hypertention [
34] are associated with blood ghrelin levels and on the other hand, OSA is related to these disorders or diseases [
35,
36,
37]. Therefore, finding a link between ghrelin levels with OSA development can be useful for prediction of related diseases with OSA and possible treatments.
The OSA cases treated by nasal Continuous Positive Airway Pressure (CPAP) require using CPAP therapy to stop the recurrence of symptoms [
38]. The changes in energy metabolism accrue after CPAP therapy for OSA [
39]. The studies [
40,
41,
42] reported the impact of CPAP therapy on the blood levels of ghrelin in adults with OSA with different results.
Based on our knowledge of English literature, there was a meta-analysis [
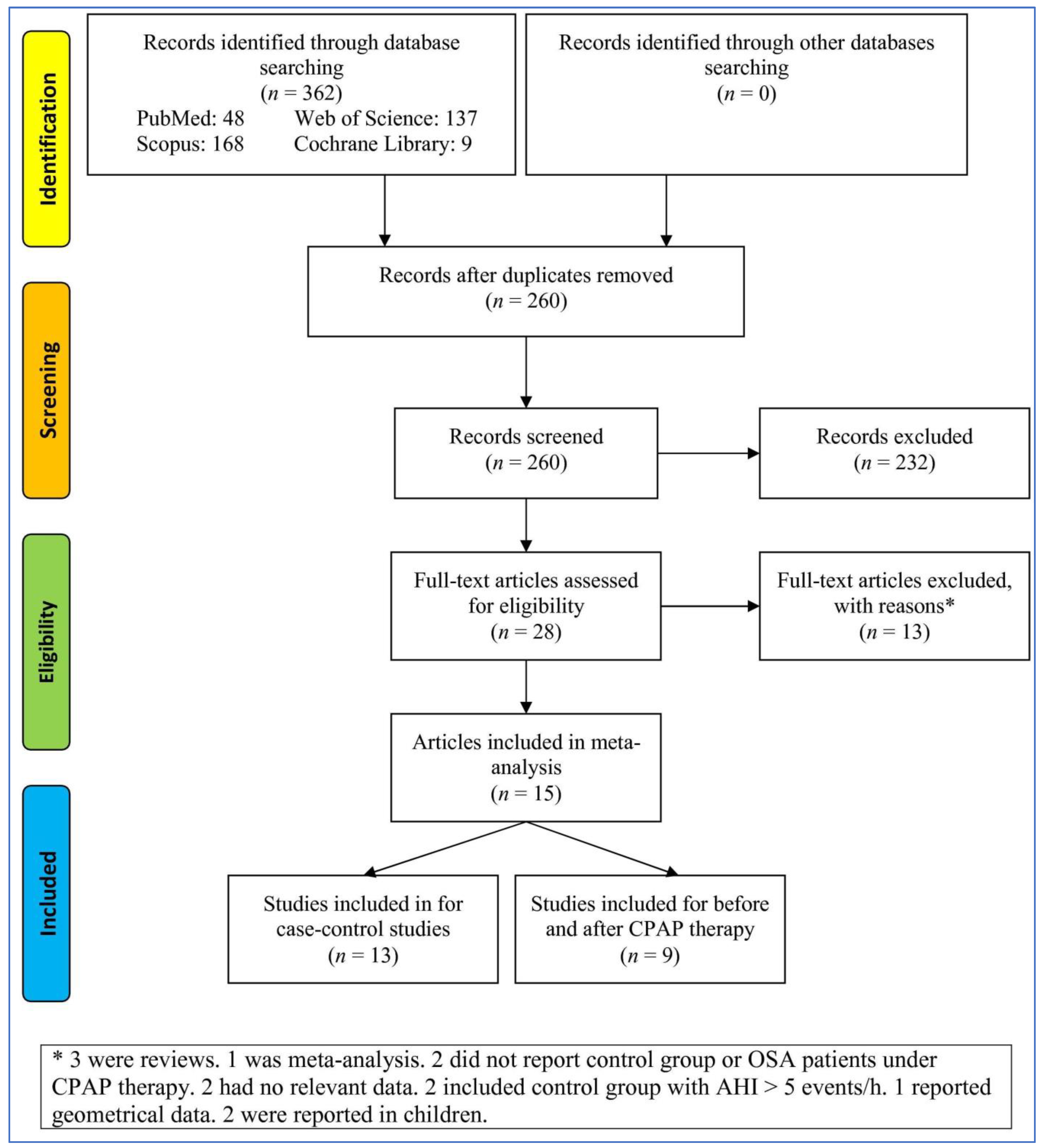
30] related to this subject—searching three databases until 2018—with eight case–control and six before–after studies. Therefore, a new systematic review and meta-analysis in four main databases were conducted with more studies (thirteen case–control and nine before–after studies) and additional analyses than the previous meta-analysis for findings potentially effective factors on heterogeneity and bias (radial plot analysis, meta-regression, and trial sequential analysis (TSA)) to check the changes of serum/plasma levels of ghrelin in adults with OSA compared to controls, as well as before compared after CPAP therapy in adults with OSA with more details. In addition to a few new studies, the previous meta-analysis missed several articles before 2018 that could be due of the choices of database or the searching criteria.
2. Materials and Methods
To design of the present meta-analysis, it was followed the PRISMA-P items [
43]. The PECO question [
44,
45] was: Are blood ghrelin levels different in adults with OSA in comparison to controls? (P: human adults with and without OSA, E: OSA disorder, C: adults with OSA compared to controls; O: and the plasma/serum ghrelin level). The clinical PICO (Population, Intervention, Comparator, and Outcome) question was: What is the impact of CPAP therapy on serum/plasma levels of ghrelin in adults with OSA? (P: human adults with OSA, I: CPAP therapy, C: adults with OSA before and after CPAP therapy; O: and the plasma/serum ghrelin level).
2.1. Search Strategy
Four databases (PubMed, Web of Science, Scopus, and Cochrane Library) were systematically and comprehensively searched until 17 October 2022, without any restrictions by one reviewer (M.S.). The search terms were as: (“obstructive sleep apnea” or “sleep apnea” or “OSA” or “obstructive sleep apnea syndrome” or “OSAS” or “obstructive sleep apnea-hypopnea syndrome” or “OSAHS”) and (“ghrelin”). The citations of all types of articles linked to the subject and “Google Scholar” were checked to ensure no study was missed.
2.2. Eligibility Criteria
Inclusion criteria: (1) studies including both adults with OSA and controls aged ≥18 years without any treatment or adults with OSA under CPAP therapy, (2) studies reporting plasma/serum ghrelin levels in OSA and controls or adults with OSA before and after CPAP therapy, (3) PSG was applied to diagnose OSA, defined as AHI ≥5 events/h for adult, (4) adults with OSA did not have other systemic diseases (diabetes mellitus, cardiovascular diseases, heart, hepatic, and renal failures, and lung diseases, any malignancy, and infectious diseases, other sleep disorders), (5) controls did not have OSA or systemic disease (see the previous criterion), and (6) venous blood was took in the fasting state on the morning to measure ghrelin. Exclusion criteria: (1) meta-analyses, book chapters, conference papers, the letter to the editor, commentary, and reviews, (2) studies without complete data, (3) studies in the absence of a control group or the control group had AHI was more than 5 events/h, (4) studies including participants aged less than 18 years old, and (5) studies including adults with OSA with any another disease.
2.3. Data Collection
The data were extracted for any study involved in the meta-analysis by two independent reviewers (A.G. and M.S.). The differences between reviewers were resolved by third reviewer (S.B.). Extracted data were the country and ethnicity of participants, the first author, the publication year, ghrelin sampling, the sample size of adults with OSA and controls, quality or quality score, means BMI, age, and AHI the groups, follow-up duration of CPAP therapy, mean AHI before and after CPAP therapy, and mean of blood levels of ghrelin in all groups.
2.4. Quality Assessment
For assessing the quality, we used the Joanna Briggs Institute (JBI) critical appraisal checklist adapted for case–control studies including ten questions or ten scores as Low: 1–4 scores, Moderate: 5–7 scores, High: 8–10 scores [
46] and the National Institutes of Health (NIH) quality assessment tool for before–after studies with twelve question or twelve scores as Good: 9–12 scores, Fair: 5–8 scores, Poor: 1–4 scores [
47] (See
Supplementary File S1). The quality score were performed by two independent reviewers (M.M.I. and M.S.). The differences between reviewers were resolved by third reviewer (M.K.C.).
2.5. Statistical Analyses
The Review Manager 5.3 (RevMan 5.3) software was applied to extract the effect sizes (standardized mean difference (SMD) and 95% confidence interval (CI)) of blood levels of ghrelin amongst adults with OSA and controls, as well as before and after CPAP therapy by one reviewer (M.S.). The
p-value (2-sided) of less than 0.05 was considered a significant value. A P
heterogeneity < 0.1(I
2 > 50%) reported a significant heterogeneity that in this state, a random-effects model [
48], otherwise, a fixed-effect model [
49] was used.
The subgroup and random-effect meta-regression analyses were done based on several variables and evaluating the stability of initial pooled SMDs, both “one-study-removed” and “cumulative” analyses as sensitivity analyses were utilized.
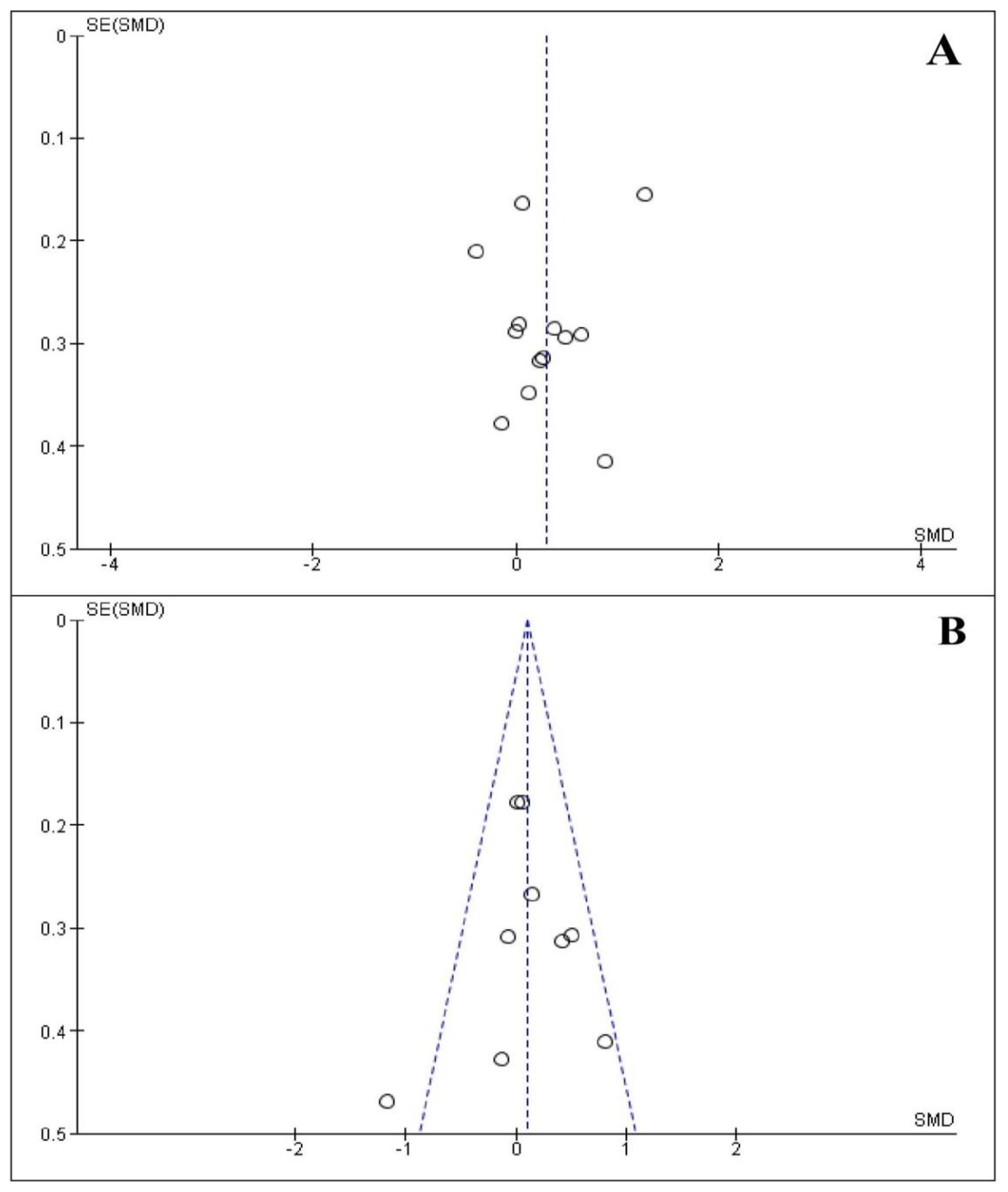
The Begg’s funnel plot by Begg’s test was applied to test potential publication bias [
50] and the Egger’s test to report degree of asymmetry [
51] that the
p-values of both tests and the data for sensitivity analyses were extracted by the Comprehensive Meta-Analysis version 2.0 (CMA 2.0) software and a
p-value (2-sided) less than 0.10 recommended the existence of the publication bias.
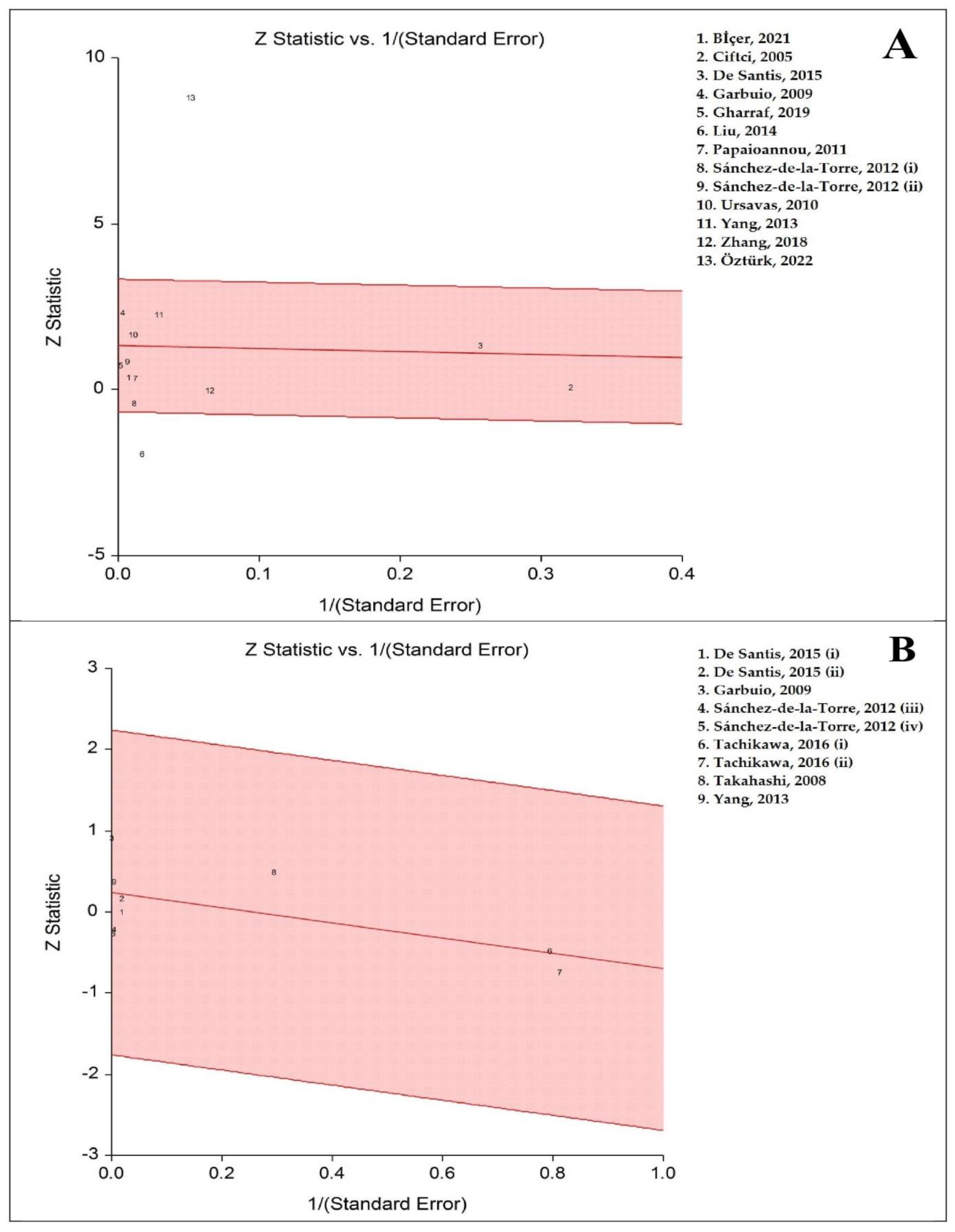
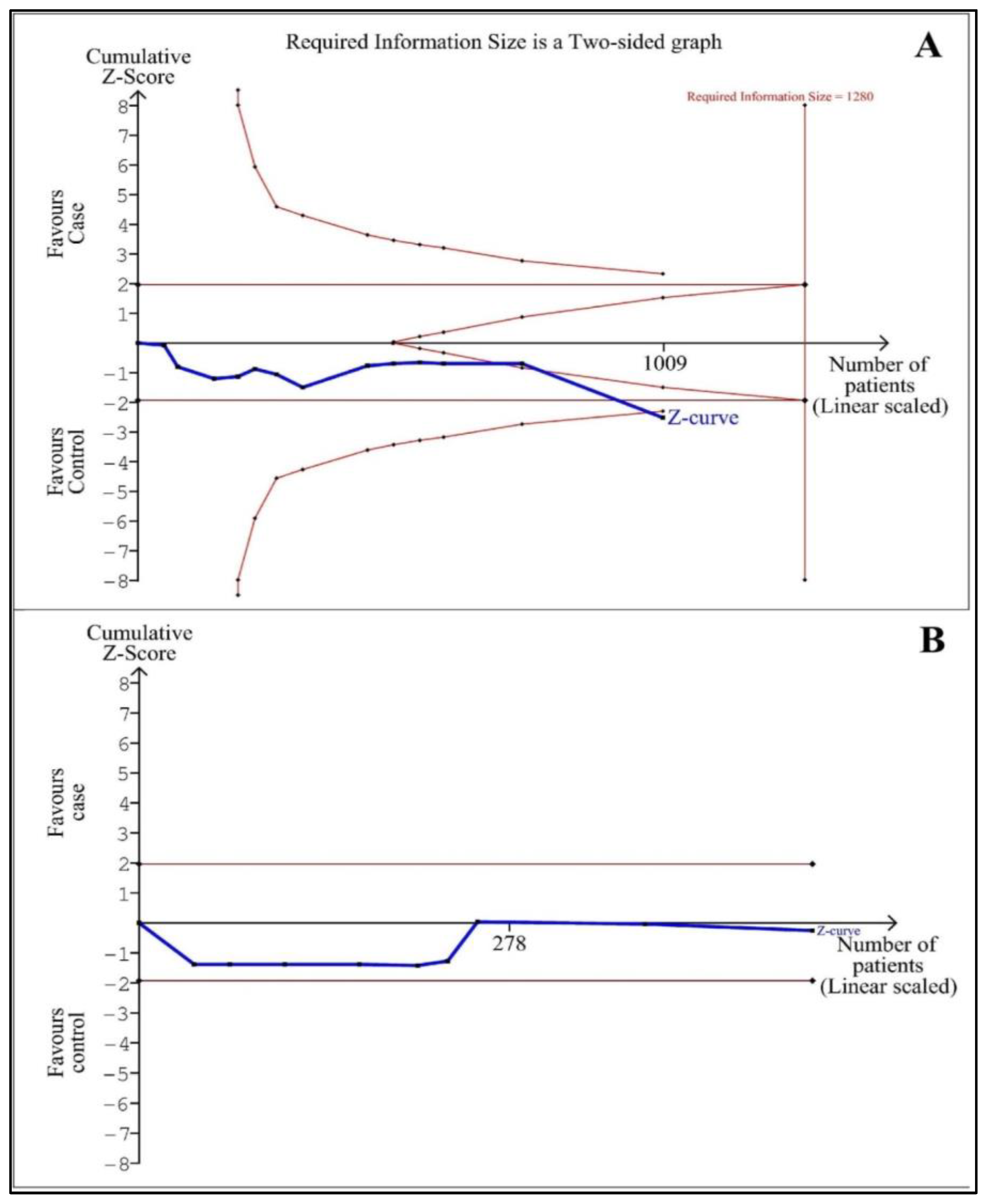
To report the potential random error (false-positive and -negative results) in meta-analysis [
52], trial sequential analysis (TSA) was accomplished using TSA software (version 0.9.5.10 beta) [
53]. The futility threshold can show a no-impact result before attaining the information size. An α-risk of 5%, a β-risk of 20%, and a 2-sided border type reporting the mean difference and variance were based on empirical assumptions created automatically by the software, were used to calculate the required information size (RIS). If the Z-curve reached the RIS line, enough participants were included in the studies and the conclusion was trustworthy or crossed the borderlines the results could be robust. Differently, the volume of information was not large enough and more evidence was needed.
The effect sizes for the studies including the required data just on a graph were extracted from the graph utilizing GetData Graph Digitizer 2.26 software.
4. Discussion
The relationship between OSA and plasma/serum ghrelin levels and the effect of CPAP therapy on ghrelin levels have remained controversial [
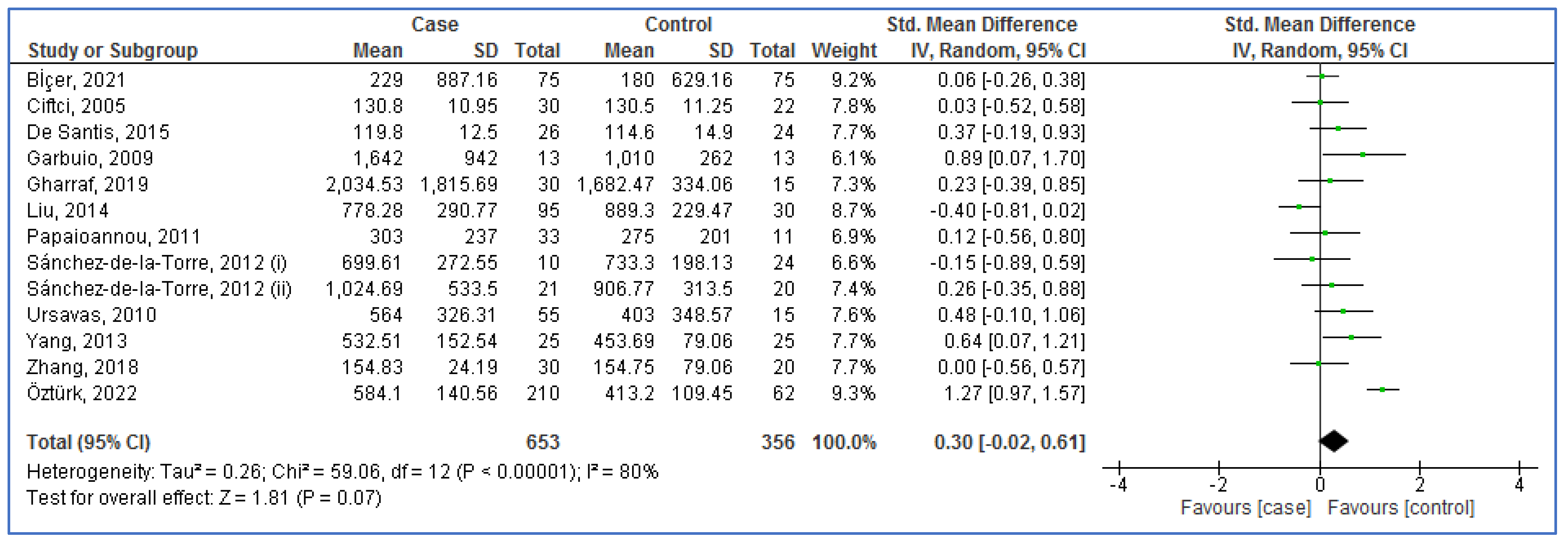
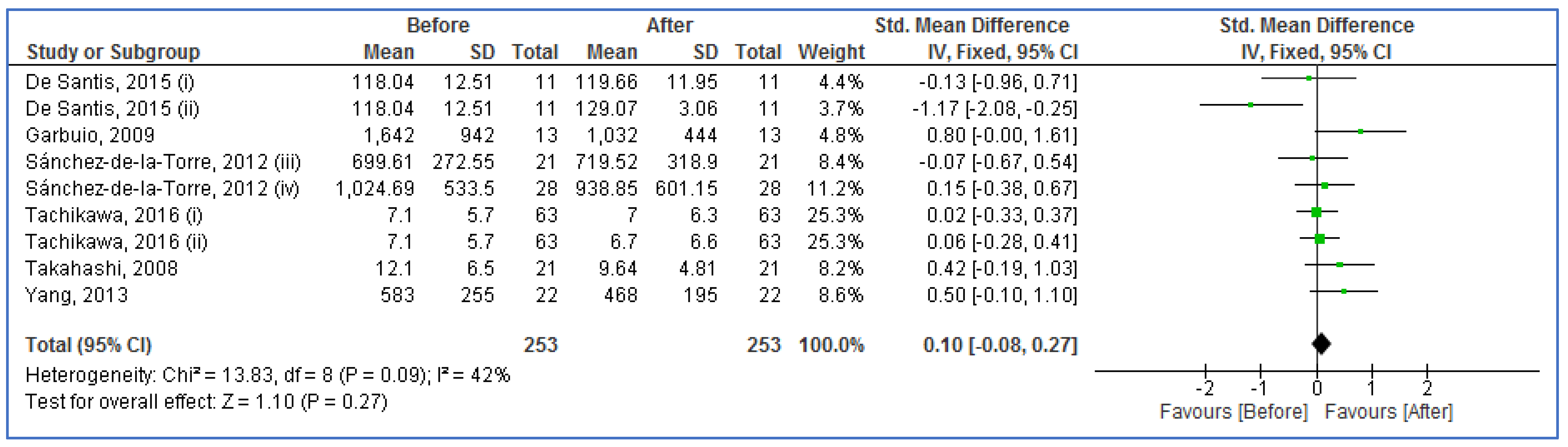
30]. The main results of the present meta-analysis recommended that the serum/plasma levels of ghrelin had no significant difference in the adults with OSA compared to the controls, moreover in adults with OSA before compared to after CPAP therapy. Removing outliers, the serum/plasma levels of ghrelin were significantly higher in the adults with OSA compared to the controls. Two analyses included low sample sizes based on TSA results. Blood sample, sample size, quality scores, means age, and AHI of adults with OSA were effective factors in case–control studies, and the mean AHI of adults with OSA before CPAP therapy in before–after studies. Therefore, the present findings require to be confirmed in additional studies with more cases and higher qualities.
Among thirteen case–control studies, three studies [
28,
41,
61] showed a significantly high level of ghrelin, whereas other studies did not find any significant difference between in adults with OSA versus controls. Among all before–after studies in the present meta-analysis, the CPAP therapy had a significant defect in increasing [
40] and decreasing [
41] the blood levels of ghrelin, but other studies did not find any effect of CPAP on the levels of ghrelin in adults with OSA.
A systematic review recommended the positive impact of older age, male gender, and higher BMI on OSA prevalence [
4]. Research showed that plasma ghrelin decreased in obese people and increased in lean people [
63]. Ciftci et al. [
55] revealed that serum ghrelin level has a positive correlation with BMI and AHI. Other studies confirmed the positive correlation of serum ghrelin levels with BMI [
40] and AHI [
60]. However, a number of studies did not confirm the correlation of serum ghrelin level with BMI [
56] and AHI [
40,
56]. Whatever the present meta-analysis showed the correlation of AHI and age with blood ghrelin levels in adults with OSA, but it did not find any significant correlation between blood levels of ghrelin and BMI.
One study [
28] reported a significant association between serum ghrelin levels and the severity of OSA as serum level of ghrelin was significantly higher in adults with severe OSA vs. moderate OSA and moderate OSA compared to mild OSA. Unfortunately, most studies did not report the blood levels of ghrelin based on OSA severity and therefore we could not analyze the association between the blood ghrelin levels and the severity of OSA. The researchers need to perform this analysis among adults with OSA in their original articles in the future. In addition, results of this current meta-analysis were in line with the previously published meta-analysis [
30].
There were three significant limitations during the meta-analysis design. (1) A low number of participants in the studies and low included studies in each analysis. (2) Less number of studies had high quality. (3) High heterogeneity among case–control studies. In contrast, there were two important strengths. (1) The stability of results. (2) A lack of publication bias across the studies.
5. Conclusions
The present meta-analysis recommended that the blood levels of ghrelin had no significant difference in the adults with OSA vs. the controls, moreover in adults with OSA before vs. after CPAP therapy. Notwithstanding the low number of individuals in the analyses, the study reported that blood sample, sample size, quality scores, mean age, and mean AHI of adults with OSA were effective factors in case–control studies, and mean AHI of adults with OSA before CPAP therapy in before–after studies. Therefore, the present findings require to be accepted in additional studies with more cases and higher qualities.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}